

Molecular Analysis of Dihydropteroate Synthase Gene Mutations in Pneumocystis jirovecii Isolates among Bulgarian Patients with Pneumocystis Pneumonia
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Ethical Considerations
4.3. Patients and Samples
4.4. DNA Extraction and Real-Time PCR for Detection of P. jirovecii
4.5. Amplification of P. jirovecii DHPS Gene
4.6. Sequencing of DHPS Gene and Phylogenetic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fujii, T.; Nakamura, T.; Iwamoto, A. Pneumocystis pneumonia in patients with HIV infection: Clinical manifestations, laboratory findings, and radiological features. J. Infect. Chemother. 2007, 13, 1–7. [Google Scholar] [CrossRef]
- Martin, S.I.; Fishman, J.A. Pneumocystis Pneumonia in Solid Organ Transplantation. Am. J. Transplant. 2013, 13, 272–279. [Google Scholar] [CrossRef]
- Kovacs, J.A.; Masur, H. Evolving health effects of Pneumocystis: One hundred years of progress in diagnosis and treatment. JAMA 2009, 301, 2578–2585. [Google Scholar] [CrossRef] [PubMed]
- Tabarsi, P.; Mirsaeidi, M.; Amiri, M.; Karimi, S.; Masjedi, M.R.; Mansouri, D. Inappropriate use of steroid and Pneumocystis jiroveci pneumonia: Report of two cases. East. Mediterr. Health J. 2008, 14, 1217–1221. [Google Scholar] [PubMed]
- El Halabieh, N.A.; Petrillo, E.; Laviano, A.; Delfino, M.; Fanelli, F.R. A Case of Pneumocystis jirovecii Pneumonia in a Severely Malnourished, HIV-Negative Patient: A Role for Malnutrition in Opportunistic Infections? J. Parenter. Enter. Nutr. 2016, 40, 722–724. [Google Scholar] [CrossRef] [PubMed]
- Hanachi, M.; Bohem, V.; Bemer, P.; Kayser, N.; de Truchis, P.; Melchior, J.-C. Negative role of malnutrition in cell-mediated immune response: Pneumocystis jirovecii pneumonia (PCP) in a severely malnourished, HIV-negative patient with anorexia nervosa. Clin. Nutr. ESPEN 2018, 25, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.Y.L.; Mattke, A.C.; Clark, J.E.; Pinzon-Charry, A.; Alphonso, N.; Kapur, N. Acquired Immunodeficiency from Maternal Chemotherapy and Severe Primary Pneumocystis Infection in an Infant. Case Rep. Pediatr. 2020, 2020, 5740304. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhu, H.; Zheng, Y. Detection of Pneumocystis jirovecii Pneumonia in Infants with Non-Human Immunodeficiency Virus Admitted to Pediatric Intensive Care Using Metagenomics Next-Generation Sequencing. Infect. Drug Resist. 2022, 15, 1889–1902. [Google Scholar] [CrossRef] [PubMed]
- Pyrgos, V.; Shoham, S.; Roilides, E.; Walsh, T.J. Pneumocystis pneumonia in children. Paediatr. Respir. Rev. 2009, 10, 192–198. [Google Scholar] [CrossRef]
- Morrow, B.M.; Samuel, C.M.; Zampoli, M.; Whitelaw, A.; Zar, H.J. Pneumocystis pneumonia in South African children diagnosed by molecular methods. BMC Res. Notes 2014, 7, 26. [Google Scholar] [CrossRef]
- Mantadakis, E. Pneumocystis jirovecii Pneumonia in Children with Hematological Malignancies: Diagnosis and Approaches to Management. J. Fungi 2020, 6, 331. [Google Scholar] [CrossRef]
- Kovacs, J.A.; Hiemenz, J.W.; Macher, A.M.; Stover, D.; Murray, H.W.; Shelhamer, J.; Lane, H.C.; Urmacher, C.; Honig, C.; Longo, D.L.; et al. Pneumocystis carinii pneumonia: A comparison between patients with the acquired immunodeficiency syndrome and patients with other immunodeficiencies. Ann. Intern. Med. 1984, 100, 663–671. [Google Scholar] [CrossRef]
- Huang, L.; Cattamanchi, A.; Davis, J.L.; den Boon, S.; Kovacs, J.; Meshnick, S.; Miller, R.F.; Walzer, P.D.; Worodria, W.; Masur, H. HIV-associated Pneumocystis pneumonia. Proc. Am. Thorac. Soc. 2011, 8, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Zolopa, A.R.; Andersen, J.; Komarow, L.; Sanne, I.; Sanchez, A.; Hogg, E.; Suckow, C.; Powderly, W.; ACTG A5164 Study Team. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: A multicenter randomized strategy trial. PLoS ONE 2009, 4, e5575. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, A.-L.; Traore, K.; Plekhanova, I.; Bouchrik, M.; Bossard, C.; Picot, S. Pneumocystis pneumonia suspected cases in 604 non-HIV and HIV patients. Int. J. Infect. Dis. 2016, 46, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, X.; Sun, T.; Fan, G.; Zhan, Q.; Weng, L. Non-HIV-infected patients with Pneumocystis pneumonia in the intensive care unit: A bicentric, retrospective study focused on predictive factors of in-hospital mortality. Clin. Respir. J. 2022, 16, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Chio, L.C.; Bolyard, L.A.; Nasr, M.; Queener, S.F. Identification of a class of sulfonamides highly active against dihydropteroate synthase from Toxoplasma gondii, Pneumocystis carinii, and Mycobacterium avium. Antimicrob. Agents Chemother. 1996, 40, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, M.; Ushiki, A.; Ikuyama, Y.; Hirai, K.; Matsuo, A.; Hachiya, T.; Hanaoka, M. A four-center retrospective study of the efficacy and toxicity of low-dose trimethoprim-sulfamethoxazole for the treatment of Pneumocystis pneumonia in patients without HIV infection. Antimicrob. Agents Chemother. 2017, 61, e01173-17. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Price, J.S.; Backx, M. Therapy and Management of Pneumocystis jirovecii Infection. J. Fungi 2018, 4, 127. [Google Scholar] [CrossRef]
- Lu, Y.-W.; Chen, T.-C. Use of Trimethoprim-Sulfamethoxazole in Patient with G6PD Deficiency for Treating Pneumocystis jirovecii Pneumonia. Clin. Case Rep. Int. 2019, 3, 1119. [Google Scholar] [CrossRef]
- Centers for Disease Control. Guidelines for prophylaxis against Pneumocystis carinii pneumonia for persons infected with human immunodeficiency virus. JAMA 1989, 262, 335–339. [Google Scholar] [CrossRef]
- Kaplan, J.E.; Hanson, D.; Dworkin, M.S.; Frederick, T.; Bertolli, J.; Lindegren, M.L.; Holmberg, S.; Jones, J.L. Epidemiology of human immunodeficiency virus-associated opportunistic infections in the United States in the era of highly active antiretroviral therapy icon. Clin. Infect. Dis. 2000, 30 (Suppl. S1), S5–S14. [Google Scholar] [CrossRef]
- Shiota, T.; Disraely, M.N.; McCann, M.P. The Enzymatic Synthesis of Folate-like Compounds from Hydroxymethyldihydropteridine Pyrophosphate. J. Biol. Chem. 1964, 239, 2259–2266. [Google Scholar] [CrossRef] [PubMed]
- Vinnicombe, H.G.; Derrick, J.P. Dihydropteroate synthase from Streptococcus pneumoniae: Characterization of substrate binding order and sulfonamide inhibition. Biochem. Biophys. Res. Commun. 1999, 258, 752–757. [Google Scholar] [CrossRef]
- Brown, G.M.; Weisman, R.A.; Molnar, D.A. The Biosynthesis of Folic Acid: I. Substrate and cofactor requirements for enzymatic synthesis by cell-free extracts of Escherichia coli. J. Biol. Chem. 1961, 236, 2534–2543. [Google Scholar] [CrossRef]
- Tibbetts, A.S.; Appling, D.R. Compartmentalization of mammalian folate-mediated one-carbon metabolism. Annu. Rev. Nutr. 2010, 30, 57–81. [Google Scholar] [CrossRef] [PubMed]
- Revuelta, J.L.; Serrano-Amatriain, C.; Ledesma-Amaro, R.; Jiménez, A. Formation of folates by microorganisms: Towards the biotechnological production of this vitamin. Appl. Microbiol. Biotechnol. 2018, 102, 8613–8620. [Google Scholar] [CrossRef]
- Voeller, D.; Kovacs, J.; Andrawis, V.; Chu, E.; Masur, H.; Allegra, C. Interaction of Pneumocystis carinii dihydropteroate synthase with sulfonamides and diaminodiphenyl sulfone (dapsone). J. Infect. Dis. 1994, 169, 456–459. [Google Scholar] [CrossRef]
- Hong, Y.L.; Hossler, P.A.; Calhoun, D.H.; Meshnick, S.R. Inhibition of recombinant Pneumocystis carinii dihydropteroate synthetase by sulfa drugs. Antimicrob. Agents Chemother. 1995, 39, 1756–1763. [Google Scholar] [CrossRef]
- Ovung, A.; Bhattacharyya, J. Sulfonamide drugs: Structure, antibacterial property, toxicity, and biophysical interactions. Biophys. Rev. 2021, 13, 259–272. [Google Scholar] [CrossRef]
- Lopez, P.; Espinosa, M.; Greenberg, B.; Lacks, S.A. Sulfonamide resistance in Streptococcus pneumoniae: DNA sequence of the gene encoding dihydropteroate synthase and characterization of the enzyme. J. Bacteriol. 1987, 169, 4320–4326. [Google Scholar] [CrossRef]
- Triglia, T.; Menting, J.G.; Wilson, C.; Cowman, A.F. Mutations in dihydropteroate synthase are responsible for sulfone and sulfonamide resistance in Plasmodium falciparum. Proc. Natl. Acad. Sci. USA 1997, 94, 13944–13949. [Google Scholar] [CrossRef]
- Huang, L.; Crothers, K.; Atzori, C.; Benfield, T.; Miller, R.; Rabodonirina, M.; Helweg-Larsen, J. Dihydropteroate Synthase Gene Mutations in Pneumocystis and Sulfa Resistance. Emerg. Infect. Dis. 2004, 10, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- De la Horra, C.; Friaza, V.; Morilla, R.; Delgado, J.; Medrano, F.J.; Miller, R.F.; de Armas, Y.; Calderón, E.J. Update on Dihydropteroate Synthase (DHPS) Mutations in Pneumocystis jirovecii. J. Fungi 2021, 7, 856. [Google Scholar] [CrossRef] [PubMed]
- Mirdha, B.R. Dihydropteroate Synthase (DHPS) Gene Mutations in Human Pneumocystosis. J. AIDS HIV Treat. 2021, 3, 17–20. [Google Scholar] [CrossRef]
- Calderón, E.; de la Horra, C.; Medrano, F.J.; López-Suárez, A.; Montes-Cano, M.A.; Respaldiza, N.; Elvira-González, J.; Martín-Juan, J.; Bascuñana, A.; Varela, J.M. Pneumocystis jiroveci isolates with dihydropteroate synthase mutations in patients with chronic bronchitis. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 545–549. [Google Scholar] [CrossRef]
- OECD; European Observatory on Health Systems and Policies. Bulgaria: Country Health Profile 2021; State of Health in the EU; OECD Publishing: Paris, France, 2021; pp. 1–24. [Google Scholar] [CrossRef]
- OECD. EU Country Cancer Profile: Bulgaria, EU Country Cancer Profiles; OECD Publishing: Paris, France, 2023; pp. 1–20. [Google Scholar] [CrossRef]
- Naumova, E.; Lesichkova, S.; Milenova, V.; Yankova, P.; Murdjeva, M.; Mihailova, S. Primary immunodeficiencies in Bulgaria—Achievements and challenges of the PID National Expert Center. Front. Immunol. 2022, 22, 922752. [Google Scholar] [CrossRef] [PubMed]
- Gamcheva, C.S. Study on Pneumocystosis in Infancy. Ph.D. Thesis, National Center of Infectious and Parasitic Diseases, Sofia, Bulgaria, 1980. (In Bulgarian). [Google Scholar]
- Kurdova-Mincheva, R.; Tsvetanov, J.; Dikov, I. Pneumocystosis in a patient who died of AIDS—Electron microscopy. Epidemic Microbiol. Infect. Dis. 1990, 27, 31–38. (In Bulgarian) [Google Scholar]
- Kurdova, R.; Marinova, T.; Jordanova, D.; Ivanova, M.; Tzvetkova, N.; Rainova, I. Opportunistic parasitic diseases associated with HIV infection in Bulgaria. In Proceedings of the IX European Multicolloquium of Parasitology, Valencia, Spain, 18–23 July 2004; pp. 435–440. [Google Scholar]
- Georgieva, V.; Vatev, N.; Petrov, A.; Stoycheva, M. Opportunistic and Coinfections in HIV Positive Patients at the Clinic of Infectious Diseases, “St. George” University Hospital, Plovdiv. Int. J. Pharm. Sci. Inv. 2012, 1, 8–10. [Google Scholar]
- Ivanova, A.; Tsvetkova, N.; Harizanov, R.; Borisova, R. Study of the distribution of pneumocystosis in Bulgaria between September 2017 and April 2019 by using real-time PCR. PROBLEMS Infect. Parasit. Dis. 2019, 47, 24–27. [Google Scholar] [CrossRef]
- Iliades, P.; Walker, D.J.; Castelli, L.; Satchell, J.; Meshnick, S.R.; Macreadie, I.G. Cloning of the Pneumocystis jirovecii trifunctional FAS gene and complementation of its DHPS activity in Escherichia coli. Fungal Genet. Biol. 2004, 41, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Borio, L.; Masur, H.; Kovacs, J.A. Pneumocystis carinii dihydropteroate synthase but not dihydrofolate reductase gene mutations correlate with prior trimethoprim-sulfamethoxazole or dapsone use. J. Infect. Dis. 1999, 180, 1969–1978. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.R.; Ast, J.C.; Hossler, P.A.; Mindell, D.P.; Bartlett, M.S.; Smith, J.W.; Meshnick, S.R. Dihydropteroate Synthase Polymorphisms in Pneumocystis carinii. J. Infect. Dis. 1997, 175, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Riebold, D.; Reisinger, E.C. Pneumocystis jiroveci Dihydropteroate Synthase (DHPS) Gene Mutants in Germany—Are There Sulfamethoxazole Resistant Pneumocystis? Available online: https://www.ncbi.nlm.nih.gov/nuccore/AJ586567 (accessed on 3 November 2023).
- Tsvetkova, N.D.; Harizanov, R.N.; Ivanova, A.I.; Strashimirov, D.T.; Grozdeva, R.S.; Yancheva-Petrova, N.S. Recurrent Pneumocystis jirovecii pneumonia in an HIV-infected patient: A case report. GSC Adv. Res. Rev. 2021, 7, 083–086. [Google Scholar] [CrossRef]
- Phair, J.; Muñoz, A.; Detels, R.; Kaslow, R.; Rinaldo, C.; Saah, A. The risk of Pneumocystis carinii pneumonia among men infected with human immunodeficiency virus type 1. Multicenter AIDS Cohort Study Group. N. Engl. J. Med. 1990, 322, 161–165. [Google Scholar] [CrossRef]
- Lundberg, B.E.; Davidson, A.J.; Burman, W.J. Epidemiology of Pneumocystis carinii pneumonia in an era of effective prophylaxis: The relative contribution of non-adherence and drug failure. AIDS 2000, 14, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.S.; Schroff, R.; Schanker, H.M.; Weisman, J.D.; Fan, P.T.; Wolf, R.A.; Saxon, A. Pneumocystis carinii pneumonia and mucosal candidiasis in previously healthy homosexual men: Evidence of a new acquired cellular immunodeficiency. N. Engl. J. Med. 1981, 305, 1425–1431. [Google Scholar] [CrossRef]
- Masur, H.; Michelis, M.A.; Greene, J.B.; Onorato, I.; Stouwe, R.A.; Holzman, R.S.; Wormser, G.; Brettman, L.; Lange, M.; Murray, H.W.; et al. An outbreak of community acquired Pneumocystis carinii pneumonia: Initial manifestation of cellular immune dysfunction. N. Engl. J. Med. 1981, 305, 1431–1438. [Google Scholar] [CrossRef]
- Mocroft, A.; Reiss, P.; Kirk, O.; Mussini, C.; Girardi, E.; Morlat, P.; Stephan, C.; De Wit, S.; Doerholt, K.; Ghosn, J.; et al. Is it safe to discontinue primary Pneumocystis jiroveci pneumonia prophylaxis in patients with virologically suppressed HIV infection and a CD4 cell count <200 cells/microL? Clin. Infect. Dis. 2010, 51, 611–619. [Google Scholar] [CrossRef]
- Buchacz, K.; Lau, B.; Jing, Y.; Bosch, R.; Abraham, A.G.; Gill, M.J.; Silverberg, M.J.; Goedert, J.J.; Sterling, T.R.; Althoff, K.N.; et al. Incidence of AIDS-defining opportunistic infections in a multicohort analysis of HIV-infected persons in the United States and Canada, 2000–2010. J. Infect. Dis. 2016, 214, 862–872. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control; WHO Regional Office for Europe. HIV/AIDS Surveillance in Europe 2020–2019 Data; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control; WHO Regional Office for Europe. HIV/AIDS Surveillance in Europe 2021–2020 Data; ECDC: Stockholm, Sweden, 2021. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe; European Centre for Disease Prevention and Control. HIV/AIDS Surveillance in Europe 2022–2021 Data; WHO Regional Office for Europe: Copenhagen, Denmark, 2022. [Google Scholar] [CrossRef]
- Tyufekchieva, M.; Yaneva, A.; Varleva, T. Spread of HIV in the country. Modern epidemiological trends. In Proceedings of the Sixth National Scientific Conference on HIV and Coinfections, Sofia, Bulgaria, 2–3 December 2022; pp. 6–7. [Google Scholar]
- Alexiev, I.; Grigorova, L.; Partsuneva, A.; Dimitrova, R.; Gancheva, A.; Kostadinova, A.; Elenkov, I.; Yancheva, N.; Grozdeva, R.; Stoycheva, M.; et al. Virological monitoring of persons with HIV/AIDS in Bulgaria. In Proceedings of the Fifth National Scientific Conference on HIV and Coinfections, Sofia, Bulgaria, 26–27 November 2021; Abstract Book. pp. 8–10. [Google Scholar]
- Roux, A.; Canet, E.; Valade, S.; Gangneux-Robert, F.; Hamane, S.; Lafabrie, A.; Maubon, D.; Debourgogne, A.; Le Gal, S.; Dalle, F.; et al. Pneumocystis jirovecii pneumonia in patients with or without AIDS, France. Emerg. Infect. Dis. 2014, 20, 1490–1497. [Google Scholar] [CrossRef]
- Kolbrink, B.; Scheikholeslami-Sabzewari, J.; Borzikowsky, C.; von Samson-Himmelstjerna, F.A.; Ullmann, A.J.; Kunzendorf, U.; Schulte, K. Evolving epidemiology of Pneumocystis pneumonia: Findings from a longitudinal population-based study and a retrospective multi-center study in Germany. Lancet Reg. Health Eur. 2022, 18, 100400. [Google Scholar] [CrossRef]
- Yale, S.H.; Limper, A.H. Pneumocystis carinii pneumonia in patients without acquired immunodeficiency syndrome: Associated illness and prior corticosteroid therapy. Mayo Clin. Proc. 1996, 71, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Chen, Y.; Yang, S.-L.; Xia, H.; Li, X.-W.; Tong, Z.-H. Pneumocystis Pneumonia in HIV-Infected and Immunocompromised Non-HIV Infected Patients: A Retrospective Study of Two Centers in China. PLoS ONE 2014, 9, e101943. [Google Scholar] [CrossRef]
- Roblot, F.; Godet, C.; Le Moal, G.; Garo, B.; Faouzi Souala, M.; Dary, M.; De Gentile, L.; Gandji, J.A.; Guimard, Y.; Lacroix, C.; et al. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Hao, J.; Li, A.; Tong, Z. Nomograms for Death from Pneumocystis jirovecii Pneumonia in HIV-Uninfected and HIV-Infected Patients. Int. J. Gen. Med. 2022, 15, 3055–3067. [Google Scholar] [CrossRef] [PubMed]
- Quick, C.A.; Wagner, D. Trimethoprim-Sulfamethoxazole in the Treatment of Infections of the Ears, Nose, and Throat. J. Infect. Dis. 1973, 128, S696–S700. [Google Scholar] [CrossRef]
- Schwartz, R.H.; Rodriguez, W.J.; Khan, W.N.; Mann, R.; Barsanti, R.G.; Ross, S. Trimethoprim-sulfamethoxazole in the treatment of otitis media caused by ampicillin-resistant strains of Haemophilus influenzae. Rev. Infect. Dis. 1982, 4, 514–516. [Google Scholar] [CrossRef]
- Huovinen, P. Resistance to trimethoprim-sulfamethoxazole. Clin. Infect. Dis. 2001, 32, 1608–1614. [Google Scholar] [CrossRef]
- Olson, R.P.; Harrell, L.J.; Kaye, K.S. Antibiotic Resistance in Urinary Isolates of Escherichia coli from College Women with Urinary Tract Infections. Antimicrob. Agents Chemother. 2008, 53, 1285–1286. [Google Scholar] [CrossRef]
- Huang, L.; Beard, C.B.; Creasman, J.; Levy, D.; Duchin, J.S.; Lee, S.; Pieniazek, N.; Carter, J.L.; del Rio, C.; Rimland, D.; et al. Sulfa or Sulfone Prophylaxis and Geographic Region Predict Mutations in the Pneumocystis carinii Dihydropteroate Synthase Gene. J. Infect. Dis. 2000, 182, 1192–1198. [Google Scholar] [CrossRef]
- Walzer, P.D.; Kim, C.K.; Foy, J.M.; Linke, M.J.; Cushion, M.T. Inhibitors of folic acid synthesis in the treatment of experimental Pneumocystis carinii pneumonia. Antimicrob. Agents Chemother. 1988, 32, 96–103. [Google Scholar] [CrossRef]
- Walzer, P.D.; Foy, J.; Steele, P.; Kim, C.K.; White, M.; Klein, R.S.; Otter, B.A.; Allegra, C. Activities of antifolate, antiviral, and other drugs in an immunosuppressed rat model of Pneumocystis carinii pneumonia. Antimicrob. Agents Chemother. 1992, 36, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- Hughes, W.T.; Killmar, J.T.; Oz, H.S. Relative potency of 10 drugs with anti-Pneumocystis carinii activity in an animal model. J. Infect. Dis. 1994, 170, 906–911. [Google Scholar] [CrossRef]
- Vedantam, G.; Guay, G.G.; Austria, N.E.; Doktor, S.Z.; Nichols, B.P. Characterization of mutations contributing to sulfathiazole resistance in Escherichia coli. Antimicrob. Agents Chemother. 1998, 42, 88–93. [Google Scholar] [CrossRef]
- Kazanjian, P.; Locke, A.B.; Hossler, P.A.; Lane, B.R.; Bartlett, M.S.; Smith, J.W.; Cannon, M.; Meshnick, S.R. Pneumocystis carinii mutations associated with sulfa and sulfone prophylaxis failures in AIDS patients. AIDS 1998, 12, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Gurunathan, S.; Masur, H.; Kovacs, J.A. Failure of co-trimoxazole in Pneumocystis carinii infection and mutations in dihydropteroate synthase gene. Lancet 1998, 351, 1631–1632. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, J.A.; Gill, V.J.; Meshnick, S.; Masur, H. New insights into transmission, diagnosis, and drug treatment of Pneumocystis carinii pneumonia. JAMA 2001, 286, 2450–2460. [Google Scholar] [CrossRef] [PubMed]
- Helweg-Larsen, J.; Benfield, T.L.; Eugen-Olsen, J.; Lundgren, J.D.; Lundgren, B. Effects of mutations in Pneumocystis carinii dihydropteroate synthase gene on outcome of AIDS-associated P. carinii pneumonia. Lancet 1999, 354, 1347–1351. [Google Scholar] [CrossRef] [PubMed]
- Ponce, C.A.; Chabé, M.; George, C.; Cárdenas, A.; Durán, L.; Guerrero, J.; Bustamante, R.; Matos, O.; Huang, L.; Miller, R.F.; et al. High Prevalence of Pneumocystis jirovecii Dihydropteroate Synthase Gene Mutations in Patients with a First Episode of Pneumocystis Pneumonia in Santiago, Chile, and Clinical Response to Trimethoprim-Sulfamethoxazole Therapy. Antimicrob. Agents Chemother. 2017, 61, e01290-16. [Google Scholar] [CrossRef]
- Le Gal, S.; Robert-Gangneux, F.; Perrot, M.; Rouillé, A.; Virmaux, M.; Damiani, C.; Totet, A.; Gangneux, J.-P.; Nevez, G. Absence of Pneumocystis dihydropteroate synthase mutants in Brittany, France. Diagn. Microbiol. Infect. Dis. 2013, 76, 113–115. [Google Scholar] [CrossRef]
- Mane, A.; Gujar, P.; Chandra, J.; Lokhande, R.; Dhamgaye, T.; Ghorpade, S.; Risbud, A. Pneumocystis jirovecii Infection and the Associated Dihydropteroate Synthase (DHPS) and Dihydrofolate Reductase (DHFR) Mutations in HIV-Positive Individuals from Pune, India. Mycopathologia 2015, 179, 141–145. [Google Scholar] [CrossRef]
- Suárez, I.; Roderus, L.; van Gumpel, E.; Jung, N.; Lehmann, C.; Fätkenheuer, G.; Hartmann, P.; Plum, G.; Rybniker, J. Low prevalence of DHFR and DHPS mutations in Pneumocystis jirovecii strains obtained from a German cohort. Infection 2017, 45, 341–347. [Google Scholar] [CrossRef]
- Ma, L.; Kovacs, J.A.; Cargnel, A.; Valerio, A.; Fantoni, G.; Atzori, C. Mutations in the Dihydropteroate Synthase Gene of Human-Derived Pneumocystis carinii Isolates from Italy Are Infrequent but Correlate with Prior Sulfa Prophylaxis. J. Infect. Dis. 2002, 185, 1530–1532. [Google Scholar] [CrossRef]
- Singh, Y.; Mirdha, B.R.; Guleria, R.; Kabra, S.K.; Mohan, A.; Chaudhry, R.; Kumar, L.; Dwivedi, S.N.; Agarwal, S.K. Genetic polymorphisms associated with treatment failure and mortality in pediatric Pneumocystosis. Sci. Rep. 2019, 9, 1192. [Google Scholar] [CrossRef]
- Singh, Y.; Mirdha, B.R.; Guleria, R.; Kabra, S.K.; Mohan, A.; Chaudhry, R.; Kumar, L.; Dwivedi, S.N.; Agarwal, S.K. Novel dihydropteroate synthase gene mutation in Pneumocystis jirovecii among HIV-infected patients in India: Putative association with drug resistance and mortality. J. Glob. Antimicrob. Resist. 2019, 17, 236–239. [Google Scholar] [CrossRef] [PubMed]
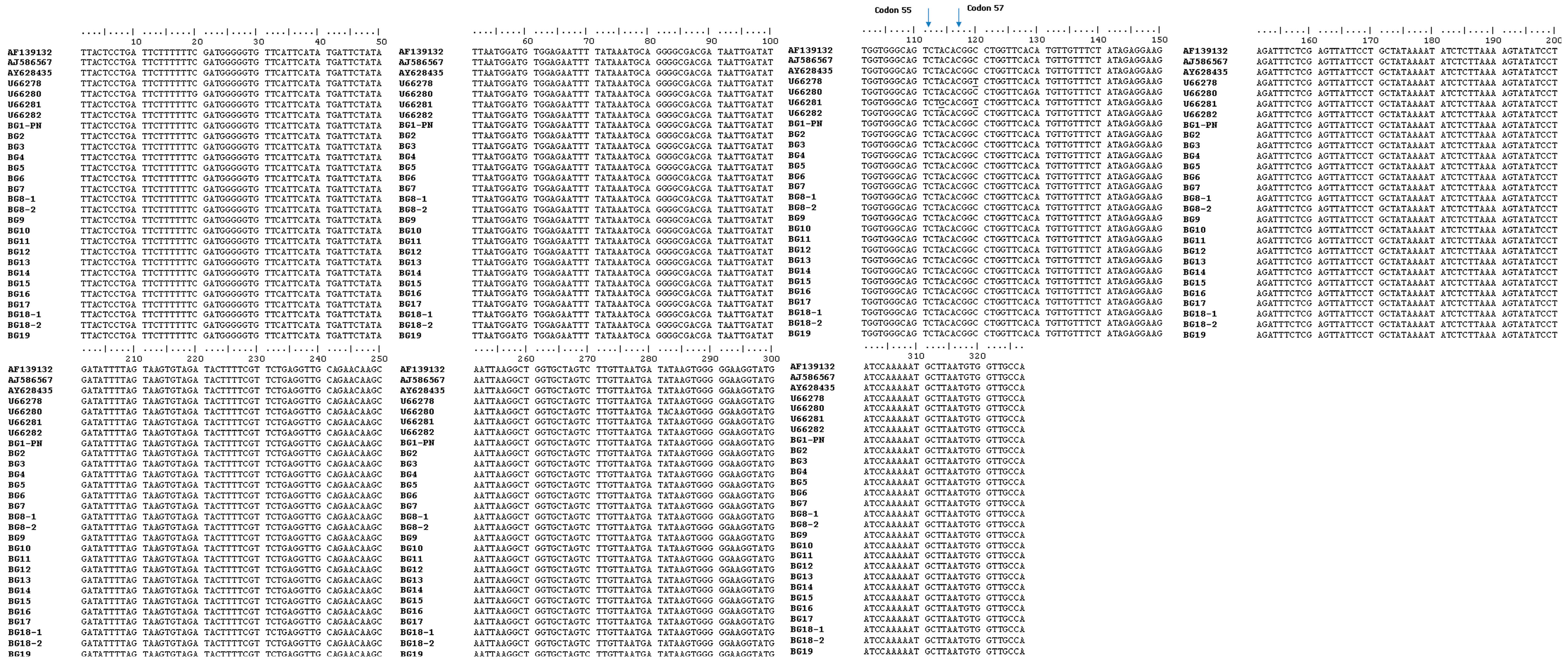
- Riebold, D.; Fritzsche, C.; Lademann, M.; Bier, A.; Reisinger, E.C. Pneumocystis jiroveci Dihydropteroate Synthase Gene Mutations at Codon 171 but Not at Codons 55 or 57 Detected in Germany. Clin. Infect. Dis. 2006, 42, 582–583. [Google Scholar] [CrossRef]
- Dumaidi, K.; Qaraqe, H.; Al-Jawabreh, A.; Abu-Helu, R.; Samarah, F.; Al-Jawabreh, H. Genetic diversity, haplotype analysis, and risk factor assessment of hepatitis A virus isolates from the West Bank, Palestine during the period between 2014 and 2016. PLoS ONE 2020, 15, e0240339. [Google Scholar] [CrossRef] [PubMed]
- Helweg-Larsen, J.; Eugen-Olsen, J.; Lundgren, B. Rapid detection of dihydropteroate polymorphism in AIDS-related Pneumocystis carinii pneumonia by restriction fragment length polymorphism. Scand. J. Infect. Dis. 2000, 32, 481–483. [Google Scholar] [CrossRef] [PubMed]
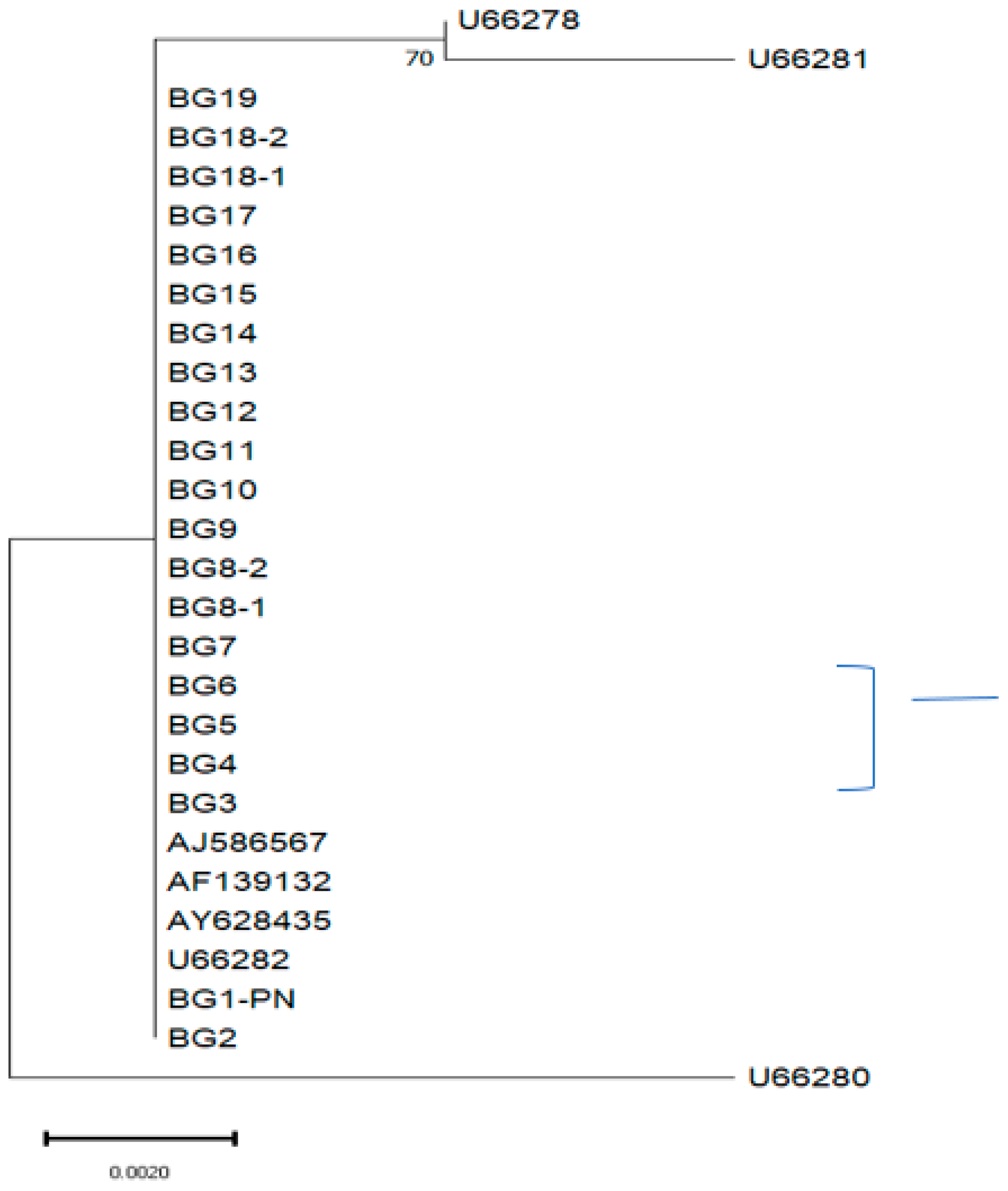
- Saitou, N.; Nei, M. The neighbor-joining method: A new method for reconstructing phylogenetic trees. Mol. Biol. Evol. 1987, 4, 406–425. [Google Scholar] [CrossRef]
- Tamura, K.; Stecher, G.; Kumar, S. MEGA 11: Molecular Evolutionary Genetics Analysis Version 11. Mol. Biol. Evol. 2021, 38, 3022–3027. [Google Scholar] [CrossRef] [PubMed]
- Felsenstein, J. Confidence limits on phylogenies: An approach using the bootstrap. Evolution 1985, 39, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M. A simple method for estimating evolutionary rate of base substitutions through comparative studies of nucleotide sequences. J. Mol. Evol. 1980, 16, 111–120. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Immunocompromised (n = 42) | Immunocompetent (n = 8) | Total = (n = 50) | ||
|---|---|---|---|---|
| HIV-Infected | HIV-Negative | |||
| Gender | ||||
| Male (%) | 30 (71.4) | 3 (7.14) | 8 (100) | 41 (82) |
| Female (%) | 6 (14.3) | 3 (7.14) | 0 | 9 (18) |
| Age in years | ||||
| Median (range) | 36 (6–54) | 35.5 (8–61) | 30 (0.4–54) | 35 (0.4–61) |
| Specimens * | 50 | |||
| LRT | 47 | |||
| BAL | 1 | 2 | 3 | |
| SP | 36 | 5 | 3 | 44 |
| URT | 3 | |||
| TA | 3 | 3 | ||
| Underlying conditions ** (No. of patients) | ||||
| HIV | 36 | 36 | ||
| HM | 3 | 3 | ||
| IPF | 2 | 2 | ||
| NS | 1 | 1 | ||
| Pneumonia | 7 | 7 | ||
| Dyspnoea | 1 | 1 | ||
| Specimen ID | Patient ID | Age in Years | Sex * | Type of Respirator Specimen # | Underlying Conditions ** | Clinical Information | |
|---|---|---|---|---|---|---|---|
| F/M | New HIV Diagnosis | PCP Prophylaxis | |||||
| BG1 | P1 | 0.6 | M | TA | pneumonia | No | |
| BG2 | P2 | 15 | M | Sputum | pneumonia | No | |
| BG3 | P3 | 14 | M | Sputum | HM | No | |
| BG4 | P4 | 8 | F | Sputum | NS | No | |
| BG5 | P5 | 60 | M | BALF | IPF | No | |
| BG6 | P6 | 44 | F | Sputum | HIV/P | Yes | No |
| BG7 | P7 | 35 | M | Sputum | HIV/P | Yes | No |
| BG8-1 BG8-2 | P8 | 46 | M | Sputum | HIV/P | Yes | No |
| BG09 | P09 ϯ | 34 | M | Sputum | HIV/P | Yes | No |
| BG10 | P10 ϯ | 6 | M | Sputum | HIV/P | No | Yes |
| BG11 | P11 ϯ | 32 | F | Sputum | HIV/P | No | Yes |
| BG12 | P12 ϯ | 28 | M | Sputum | HIV/P | No | Yes |
| BG13 | P13 ϯ | 44 | M | Sputum | HIV/P | Yes | No |
| BG14 | P14 | 25 | M | Sputum | HIV/P | Yes | No |
| BG15 | P15 ϯ | 42 | M | Sputum | HIV/P | Yes | No |
| BG16 | P16 | 35 | M | Sputum | HIV/P | Yes | No |
| BG17 | P17 | 54 | M | BLAF | HIV/P | No | Yes |
| BG18-1 BG18-2 | P18 | 45 | M | Sputum | HIV/P | Yes | No |
| BG19 | P19 | 51 | M | Sputum | bronchiectasis | No | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsvetkova, N.; Harizanov, R.; Rainova, I.; Ivanova, A.; Yancheva-Petrova, N. Molecular Analysis of Dihydropteroate Synthase Gene Mutations in Pneumocystis jirovecii Isolates among Bulgarian Patients with Pneumocystis Pneumonia. Int. J. Mol. Sci. 2023, 24, 16927. https://doi.org/10.3390/ijms242316927
Tsvetkova N, Harizanov R, Rainova I, Ivanova A, Yancheva-Petrova N. Molecular Analysis of Dihydropteroate Synthase Gene Mutations in Pneumocystis jirovecii Isolates among Bulgarian Patients with Pneumocystis Pneumonia. International Journal of Molecular Sciences. 2023; 24(23):16927. https://doi.org/10.3390/ijms242316927
Chicago/Turabian StyleTsvetkova, Nina, Rumen Harizanov, Iskra Rainova, Aleksandra Ivanova, and Nina Yancheva-Petrova. 2023. "Molecular Analysis of Dihydropteroate Synthase Gene Mutations in Pneumocystis jirovecii Isolates among Bulgarian Patients with Pneumocystis Pneumonia" International Journal of Molecular Sciences 24, no. 23: 16927. https://doi.org/10.3390/ijms242316927