
Molecular Changes Associated with Suicide
by
 , , , and
, , , and
Daniela Navarro
1,2,3 ,
,
Marta Marín-Mayor
4,5,
Ani Gasparyan
1,2,3 ,
,
María Salud García-Gutiérrez
1,2,3,
Gabriel Rubio
2,4,5 and
Jorge Manzanares
1,2,3,* 1
Instituto de Neurociencias, Universidad Miguel Hernández-CSIC, Avda de Ramón y Cajal s/n, San Juan de Alicante, 03550 Alicante, Spain
2
Redes de Investigación Cooperativa Orientada a Resultados en Salud (RICORS), Red de Investigación en Atención Primaria de Adicciones (RIAPAd), Instituto de Salud Carlos III, MICINN and FEDER, 28029 Madrid, Spain
3
Instituto de Investigación Sanitaria y Biomédica de Alicante (ISABIAL), 03010 Alicante, Spain
4
Instituto de Investigación i+12, Hospital Universitario 12 de Octubre, 28041 Madrid, Spain
5
Department of Psychiatry, Complutense University of Madrid, 28040 Madrid, Spain
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2023, 24(23), 16726; https://doi.org/10.3390/ijms242316726
Submission received: 7 November 2023
/
Revised: 20 November 2023
/
Accepted: 21 November 2023
/
Published: 24 November 2023
(This article belongs to the Collection Feature Papers in Molecular Genetics and Genomics)
Abstract
:Suicide is a serious global public health problem, with a worrying recent increase in suicide rates in both adolescent and adult populations. However, it is essential to recognize that suicide is preventable. A myriad of factors contributes to an individual’s vulnerability to suicide. These factors include various potential causes, from psychiatric disorders to genetic and epigenetic alterations. These changes can induce dysfunctions in crucial systems such as the serotonergic, cannabinoid, and hypothalamic–pituitary–adrenal axes. In addition, early life experiences of abuse can profoundly impact an individual’s ability to cope with stress, ultimately leading to changes in the inflammatory system, which is a significant risk factor for suicidal behavior. Thus, it is clear that suicidal behavior may result from a confluence of multiple factors. This review examines the primary risk factors associated with suicidal behavior, including psychiatric disorders, early life adversities, and epigenetic modifications. Our goal is to elucidate the molecular changes at the genetic, epigenetic, and molecular levels in the brains of individuals who have taken their own lives and in the plasma and peripheral mononuclear cells of suicide attempters and how these changes may serve as predisposing factors for suicidal tendencies.
1. Introduction
Suicide is the cause of more than 700,000 deaths each year. Shockingly, in 2019, suicide was the fourth leading cause of death among people aged 15 to 29, according to the World Health Organization (WHO) [1]. Suicide is a severe global problem that is preventable. The need for a comprehensive, multisectoral suicide prevention strategy is paramount. However, it is crucial to recognize that many factors influence an individual’s risk of suicide.
The link between suicide and mental disorders is well established. Psychiatric disorders such as major depression and schizophrenia are among the most critical risk factors for suicide. In addition, early experiences of sexual and psychological abuse are strongly related to suicidal behavior [2]. Both chronic and acute stressful situations can increase suicidal behavior [2]. In addition, many suicides occur impulsively and unexpectedly in times of crisis due to a lack of ability to cope with stressful situations. Suicide victims show several alterations at both the central and peripheral levels. For example, the prefrontal cortex (PFC) of suicide victims shows an increase in the inflammatory interleukins IL-1, IL-6, and tumor necrosis factor alpha (TNF-alpha) and a decrease in brain-derived neurotrophic factor (BDNF) [3]. The abnormal functioning of the cortisol-stress axis and the abnormal interactions of the inflammatory system are significant risk factors for stress-related suicidal behavior [4,5]. The potential markers of suicidal behavior include those related to changes in the inflammatory pathways associated with hypothalamic—pituitary—adrenal (HPA) axis hyperactivity. Several molecular changes in cells associated with neuroinflammation and the immune system have been identified in the brains of suicide victims, including astroglia and microglia [6].
Suicidal behavior is not solely attributed to stressful situations or psychiatric disorders that cause molecular changes; genetic factors also play a role. Seven genes have been identified that are differentially expressed in suicide but not mood disorders [7]. Familial genetic inheritance may be a cause of suicidal behavior. It has been reported that monozygotic twins present a higher concordance for suicidal behavior than dizygotic twins [8,9,10]. In addition, alterations in genes encoding proteins involved in serotonergic neurotransmission have been associated with suicidal behavior [10]. Furthermore, epigenetic changes such as DNA methylation were detected in suicide cases compared to non-psychiatric controls in both the PFC and cerebellum [11].
Therefore, suicidal behavior may be multifactorial, involving a complex interplay of genetic, epigenetic, psychiatric, psychological, and environmental factors [12]. These changes may disrupt stress control, neuroplasticity, and neurotransmission systems [2,3]. However, much remains to be understood about the biological factors underlying the pathophysiology of suicide.
In this review, we have considered the molecular changes in suicide attempters and completers. While we examine the risk factors associated with suicidal behavior in psychiatric disorders and early life adversity, our primary goal is to highlight the most well-studied factors that may predispose individuals to suicide. In addition, we aim to elucidate the molecular changes at the genetic, epigenetic, and system levels observed in the brains of suicide completers, in the plasma and peripheral blood cells of the suicide attempters and how these changes may be a risk factor for suicidal behavior.
2. Mental Disorders as Risk Factors for Suicide
Suicidality can be conceptualized as a continuum from thoughts to actions, with intensity from mild to severe, which includes, in ascendant order, suicidal ideation, suicide planning, suicide attempts, and suicide deaths [13]. It is well established that, compared to individuals without a psychiatric disorder, those with severe mental illness are more likely to commit suicide. This section will review different mental disorders as risk factors for suicide.
2.1. Bipolar Disorder
Multiple psychiatric disorders have been associated with an increased risk of suicidal behaviors. However, bipolar disorder (BD) is the one that confers the highest risk of suicide. Both suicide attempts and completed suicides are significantly more prevalent in patients with BD than in the general population. The risk for suicide among BD patients is about 60 times greater than in the general population. Patients with BD are also the most likely to engage in repeated suicide attempts among all psychiatric disorders. Approximately 25–50% of patients with BD will commit at least one suicide attempt during their lifetime, and 10–20% will complete suicide. It is essential to highlight that suicide attempts in BD patients tend to be associated with greater lethality, as confirmed by the ratio of suicide attempts to completed suicides, which is much lower in BD patients (3:1) compared to the general population (35:1). Therefore, patients with BD die by suicide 20 to 30 times more frequently than their peers in the general population [14,15,16,17,18,19,20,21,22,23,24].
Several sociodemographic, clinical, genetic-neurobiological, and treatment risk factors have been related to suicidality in BD patients. Regarding sociodemographic factors, most studies point out that women with BD are significantly more likely than men with BD to attempt suicide. On the contrary, men with BD are more likely to attempt suicide by violent methods and have significantly higher absolute rates of suicide deaths [16,20,23,24]. Considering age, BD patients who attempt suicide are significantly younger than non-attempters, but older age is associated with a higher suicide lethality [16,17,20]. Finally, other sociodemographic factors proposed for the association of BD and suicidality include divorced or single marital status, inadequate social support, low socioeconomic status, a lower level of education, stressful life events, and a higher mean altitude of residence [16,17,21,22,23,25].
An earlier onset of the disease is associated with an increased risk of suicide attempts in BD patients [14,16,20,21,22,23,26]. Moreover, BD patients who committed more than one suicide attempt showed an even significantly lower age of onset of the disease [26]. Different studies have also reported that BD individuals who attempt suicide have a significantly longer duration of the disorder, independent of gender. Furthermore, a longer duration of the disorder has been positively correlated with a higher lethality of suicide attempts [15]. Rapid cycling (having at least four affective episodes within one year) has also been strongly associated with an increased lifetime risk of suicidal behavior [23,24]. Other clinical variables associated with an increased risk of suicidality in BD patients are a more significant number and severity of affective episodes, especially depressive episodes and symptoms, having treatment-resistant depression, hopelessness, psychotic features, atypical depressive features, agitated depression, and dysthymic or cyclothymic temperaments [15,17,20,22,26].
Comorbidity with other psychiatric disorders and substance use disorders (SUD) increases the likelihood of suicidal behavior in BD individuals. It has also been reported that there are consistent and positive associations between comorbid alcohol and substance use in patients with BD and suicide attempts, regardless of age and gender. Finally, suicide attempters exhibit cognitive difficulties and impaired decision-making, leading to using suicidal behaviors and/or alcohol and drugs as a maladaptive way of managing painful feelings [15,21,23,27]. Other personality traits related to suicidality in BD patients include impulsivity, aggressiveness, difficulties in emotion regulation, a low tolerance to stress, extreme attributional style, lower social skills, and self-directedness [15,28].
Finally, treatment risk factors should also be considered. It has been suggested that antidepressants may increase the risk of suicidality in BD patients, primarily when they associate dysphoric agitation, anger, restlessness, irritability, or insomnia, or, during the mood episode, mixed features are predominant, dysphoric mania or agitated depression. This antidepressant-increased suicide risk has been observed for younger patients, whereas, in older patients, antidepressants could show a protective effect against suicide [20]. On the contrary, lithium treatment has been proposed to show a protective effect over suicidality. Several studies have found a reduced suicide risk in BD patients with lithium [20].
The increased likelihood of suicide among BD patients is related to specific genetic and neurobiological correlates. Suicide attempts among individuals with BD are associated with periventricular white matter and deep white matter hyperintensities [15]; lower grey matter volumes in regions including the ventrolateral prefrontal cortex and the dorsolateral prefrontal cortex (DLPFCx) [29], the right orbitofrontal cortex, the right hippocampus (HIPP) and bilateral cerebellum [15,30]; lower left orbitofrontal cortical thickness and white matter fractional anisotropy [15,25]; and a lower volume in the left ventrolateral prefrontal cortex, right DLPFCx (involved in executive function, particularly voluntary emotional regulation) and bilateral HIPP [31]. In addition, a longitudinal study that included patients with mood disorders (major depressive disorder [MDD] and BD) found lower grey matter volume in prefrontal regions at baseline, including the ventral prefrontal cortex, among youth who went on to make suicide attempts within three years of follow-up [31].
Other biological factors associated with an increased risk for suicidality in BD patients include altered functioning of the HPA-axis with significantly higher levels of corticotropin-releasing hormone (CRH) and bedtime salivary cortisol [15,17], and higher serum testosterone concentrations, lower serum cholesterol, triglyceride, and n-6 arachidonic acid [15]. In a large-scale biomarker discovery study, 16 candidate proteins were identified as being associated with prospective suicide attempts, with three having a robust association: uteroglobin (SCGB1A1), annexin A10 (ANXA10) and centrin 2 (CETN2). These proteins respond to hormonal and steroid activity, immune system processes, cellular growth, and metabolism [32] (Figure 1).
Genetic variations play an essential role in the association between BD and suicidality. Several gene polymorphisms, such as those associated with tryptophan hydroxylase 1 (TPH1) and tryptophan hydroxylase 2 (TPH2), were found to be related to suicide attempts of high lethality and completed suicides, respectively [17]. In addition, serotonin polymorphisms and a low expression of the serotonin receptor 2A (5-HT2A) RNA in the prefrontal cortex have been strongly associated with suicidal behavior in BD patients [15,17]. It has also been suggested that the expression of BDNF is significantly reduced in individuals who commit suicide independently of the psychiatric disorder [17]. Genome-wide association studies (GWAS) on suicide attempts in BD patients have found a trend of association with rs2767403, an intron variant of the Aminopeptidase O (AOPEP) gene, which encodes a metalloprotease linked to the renin-angiotensin system, and strong support for the chromosome 4 locus in LOCI105374524, a non-coding RNA of the glucosylceramidase beta 3 (GBA3) gene [33]. NOTCH and gamma-aminobutyric (GABA)-ergic signaling were also associated with specific related phenotypes [34]. Finally, polygenic scores for externalizing behaviors, smoking, suicide attempts, and MDD have been associated with suicide attempts and ideation in BD patients [35].
2.2. Major Depressive Disorders
Major depressive disorders (MDD) are also strongly associated with suicidality. Mortality from suicide in individuals with MDD is more than 20 times higher compared with the general population. A meta-analysis of observational studies found a pooled lifetime prevalence of suicide attempts of 31% [95% confidence interval (CI) 27–34%], a 1-year prevalence of 8% (95% CI 3–14%) and a 1-month prevalence of 24% (95% CI 15–34%) in individuals with MDD [19]. More recently, another meta-analysis has found that in patients diagnosed with MDD, the prevalence of suicide ideation was 37.7%, whereas the prevalence of suicide plans was 15.1% [36].
Several risk factors have been proposed for the association of MDD and suicidality. These risk factors include male gender, depression severity, age of onset and course of depression, a family history of psychiatric disorders, previously attempted suicide, comorbid psychiatric disorders such as anxiety disorders, and abuse and violence during childhood [37,38,39,40]. In addition, specific symptoms of depression, such as hopelessness, self-blame, irritability, insomnia and bipolar features, have also been associated with an increased risk of suicidality in individuals with MDD [39,40].
The increased risk of suicidality in patients with MDD has been associated with inflammatory changes such as lowered BDNF or increased interleukin 1ß (IL-1ß), interleukin-6 (IL-6), interleukin-13 (IL-13), tumor necrosis factor α (TNF-α), C reactive protein (CRP) and C-C motif chemokine ligand 2 (CCL2), dysfunctions of the HPA-axis, with overproduction of CRH and elevated glucocorticoid production, and structural and functional brain changes [36,41,42] (Figure 1). Recent GWAS analyses have shown that genetic liability for MDD increases the risk for suicide attempts, as suicide-attempters with MDD, BD, and schizophrenia had higher polygenic risk scores for MDD than non-attempters [33].
2.3. Anxiety Disorders
Anxiety disorders (AD) have been associated with suicide behavior in the general population and individuals with other psychiatric comorbidities. Findings regarding the relationship between anxiety disorders and the risk for suicidality have been inconsistent, with some studies concluding that anxiety disorders increase the risk of suicide [43] and others failing to find this significant association [44]. Within those studies with negative results, authors have suggested that specific anxiety symptoms (e.g., hypochondriasis) could be protective against suicide if associated with fear of death or illness [44]. Anxiety sensitivity, defined as the extent to which an individual fears anxiety-related sensations because of their misinterpretation, has also been found to be associated with suicidal ideation and global suicide risk [45].
Several modulators and mediators of the association between anxiety disorders and suicide behavior have been proposed. Some studies conclude that women are at a higher risk of suicide ideation and attempts, while others consider the opposite, although there is a certain consensus about the fact that men are more likely to commit suicide than women [46,47,48]. Furthermore, factors related per se to the disorder, such as the severity of symptoms, age of onset, mean length of the disease, and history of lifetime suicide attempts, are correlated with suicidal behavior [47,49,50].
Post-traumatic stress disorder (PTSD) is more strongly associated with suicide attempts [51], although other anxiety diagnoses have been proposed to predict suicide. In this way, panic disorder, social anxiety disorder, and generalized anxiety disorders have been proposed as significant risk factors for suicide. Finally, several reviews and meta-analyses have confirmed that, contrary to the traditional thought that obsessive compulsive disorders (OCD) are unrelated to elevated suicide risk, individuals with OCD are at an increased risk for suicide ideation and suicide attempts, so at least one patient out of ten with OCD has a lifetime suicide attempt, and nearly half of them suicidal ideation [49,52].
Although the causal role of anxiety in suicidality remains unclear, anxiety disorders and suicidality could share genetic risk and common neurobiological mechanisms (dysregulation of inflammatory responses, alterations in the HPA-axis and the CRH, structural and functional abnormalities in brain regions related to reward and affect) or mutual risk factors (childhood maltreatment has been linked to both, anxiety disorders and suicidality) [47] (Figure 1). Regarding psychological theories of suicide, anxiety is implicated in many suicide theories. It has also been proposed that avoidance strategies associated with anxiety disorders exacerbate psychological distress, which could, in turn, place patients with anxiety in a more vulnerable stage of suicidal behavior, as suicidality has been proposed to be an escape-based response from aversive self-awareness and negative emotions [43].
Genetic studies of anxiety disorders associated with suicidal behavior are scarce. However, a 22-year longitudinal study of 1255 Canadian individuals showed that the N1-acetyltransferase (SAT1) and SAT1, spermine synthase (SMS) polymorphisms are associated with anxiety and suicide attempts [53].
2.4. Psychotic Disorders, and Schizophrenia
Psychotic disorders are one of the psychiatric disorders more frequently associated with suicidality. A recent meta-analysis found that, among psychotic disorders, schizoaffective disorder is associated with the highest risk of suicide attempt and completed suicide, followed by schizophrenia and first psychotic episodes, with the risk of suicide-related to delusional disorders much lower [54]. Focusing on schizophrenia, the relative risk of suicide is 12 times higher in patients diagnosed with schizophrenia than those without this diagnosis. It has been estimated that 10–22% of patients diagnosed with schizophrenia complete suicide with the result of death, 20–40% of patients attempt suicide, and up to 40% of patients with a psychotic first episode experience persistent suicide ideation [55]. Several meta-analyses have been recently conducted, and they conclude that in schizophrenia, the lifetime prevalence of suicide ideation is 19.22% to 34.5%, whereas the lifetime prevalence of suicide attempts and self-harm is 14.6% to 26.8% [55,56,57,58].
Within the subtypes of schizophrenia, the paranoid type has been associated with a higher risk of suicidality [59]. Moreover, comorbid depression, panic attacks, alcohol and/or substance use disorders, suicide ideation and plans and a history of suicide attempts are essential contributors to suicidality. Finally, non-adherence to antipsychotic treatment also increases the risk of suicide in individuals diagnosed with schizophrenia [28,59,60,61].
As in other psychiatric disorders, it has been suggested that suicidal behavior in schizophrenia has a neurobiological basis. The hyperactivity of the HPA-axis would result in glucocorticoid neurotoxicity and subsequently in the tissue damage of different brain regions, and this could be the underlying causal mechanism of suicidality in individuals with schizophrenia. Volumetric abnormalities in the limbic system structures have been shown to discriminate between individuals with schizophrenia who commit suicide and those who do not. Individuals with schizophrenia who commit suicide show significantly lower cerebrospinal fluid concentrations of the serotonin metabolite 5-hydroxy-indol acetic acid (5-HIAA) and a blunted prolactin secretion in response to the D-fenfluramine test (Figure 1).
Genetic variants in the serotonin receptor could play a role in the association between schizophrenia and suicide. The decreased expression levels of 2-glutamate-related genes, glutamate-ammonia ligase and glial high-affinity glutamate transporter member 3 (SLCIA3) have also been found in individuals with schizophrenia who commit suicide. In addition, polymorphisms in adrenoceptor alpha 2B (ADRA2B) are associated with suicidality among patients diagnosed with schizophrenia [59,61].
2.5. Borderline Personality Disorder
A growing body of research has shown that personality disorders, especially borderline personality disorder (BPD), are associated with a high risk of suicidal ideation, suicide attempts and completed suicide [62]. Meta-analytic results confirm a 52-fold increase in suicide rates among BPD individuals compared with the general population. At least 75% of patients with BPD attempt suicide. BPD patients have a mean of three lifetime suicide attempts, primarily by overdose. It has been reported that suicide occurs in up to 10% of BPD patients in retrospective studies and 3–6% in prospectively followed cohorts. In addition, nearly 6% of patients with BPD die due to suicide [63,64].
Emotional dysregulation, identity disturbances, interpersonal difficulties, and a lack of control over impulses make BPD patients more likely to turn to suicidal behaviors, so the frequency of suicide attempts is strongly associated with these traits. In addition, suicide attempts in BPD patients usually occur following stressful life events as a wish to escape [62,63,64].
On the other hand, BPD is associated with an increased likelihood of suicidality when it appears comorbid with other psychiatric disorders such as affective and anxiety disorders, eating disorders and SUD [62,65] (Figure 1). BPD features independently predict the risk of clinically significant suicidal ideation and the risk of suicide attempts [65].
Two genetic studies suggest an association between BPD and polymorphisms in the serotonergic system, such as TPH-1 (limiting enzyme for 5-HT biosynthesis) in females and serotonin transporter-linked promoter region (5-HTTLPR) in males [66,67]. Interestingly, one found an association between the catechol-O-methyltransferase COMT Val158 Met single nucleotide polymorphism (SNP), the 5-HTTLPR S/L and BPD [66].
2.6. Substance Use Disorders
Individuals with substance use disorders (SUD) are also at high risk for suicidality. In a meta-analysis conducted by Poorolajal et al., a significant association between SUD and suicidal ideation (OR = 2.04; 95% CI: 1.59, 2.50), suicide attempts (OR = 2.49; 95% CI: 2.00, 2.98) and suicide deaths (OR = 1.49; 95% CI: 0.97, 2.00) was reported [68]. More recently, a meta-analysis of longitudinal studies concluded that heavier alcohol use predicted an increased risk of death by suicide. Specifically, alcohol use was associated with a 94% increase in the risk of death by suicide [69].
SUD and suicidality influence each other in both adolescent and adult populations [70]. Several hypotheses have been developed to explain this bidirectional association: (1) the secondary psychiatric disorder hypothesis supports the idea that SUD leads to suicidality through an increase in psychological distress and impulsivity, depressive-induced symptoms, as well as a decrease in effective coping strategies and problem-solving, the quality of social relationships and/or decreased academic or working performance; (2) the secondary SUD hypothesis postulates that suicidality leads to SUD through increased coping motives for substance use; (3) the bidirectional hypothesis posits SUD and suicidality increases vulnerability each other; and (4) the common factor hypothesis points out that external factors, such as traumatic life events or impulsivity are common to both SUD and suicidality and explain their co-occurrence [70].
Some genetic studies have attempted to correlate gene alterations in patients with SUD who died by suicide. A recent study found that the 5-HTTLPR plays a role in the association between drug use and suicidal behavior in a person with BD [71]. However, in a Slovenian population study, no association was found between polymorphism in the 5HTR gene and transporter gene and alcohol-related suicide [72]. Patients with opioid and cocaine use disorders who attempted suicide were associated with a single nucleotide polymorphism (in the BDNF gene, rs7934165), suggesting a common BDNF-related pathophysiology of suicide attempts and SUD [73]. Brain gene expression patterns of suicide completers and comorbid with SUD were reported a few years ago. The authors conclude that the interaction between suicide and SUD leads to a unique expression profile. In particular, alterations in the expression of genes involved in glial differentiation and glutamatergic neurotransmission were observed in suicide with SUD [74].
3. Childhood Abuse and/or Neglect as a Risk Factor for Suicide
Childhood maltreatment is any sexual, physical, or emotional abuse and/or neglect that results in actual or potential harm that affects the child’s physical or mental health [75]. The prevalence of childhood maltreatment among the general population has been estimated to be up to 30% [75,76].
A growing body of research has found a strong association between childhood maltreatment and suicide behavior during adulthood [75,77,78] (Figure 2).
In the National Epidemiological Survey on Alcohol and Related Conditions (NESARC), childhood physical and sexual abuse was associated with suicide attempts in 2.64% of survey respondents [79]. Furthermore, this study found that childhood maltreatment was significantly associated with an increased risk of suicide at an earlier age. It has also been proposed that childhood maltreatment could additively impact suicidality [80]. In addition, in a study that examined the relationship between childhood maltreatment and prospective suicidal ideation in a cohort of youths, it was concluded that childhood maltreatment predicted suicidal ideation independently of previous suicidal ideation and depression symptoms severity [81].
Multiple meta-analyses [75,78,82,83,84,85,86,87] have studied the relationship between childhood maltreatment and the risk of suicidality in both infant adolescent and adult populations, concluding that childhood abuse and/or neglect is associated with subsequent increased risk for suicide behavior. These studies have found that children, adolescents, and adults exposed to abuse or neglect during childhood have a 2 to 4-fold increased risk for suicidality, including suicide ideation, suicide plans, and suicide attempts. Specifically, early sexual abuse has been suggested to be the type of childhood maltreatment more strongly associated with suicidal behavior, showing an additional direct effect over other forms of maltreatment [79]. Moreover, early sexually abused males would be at a higher risk for suicide attempts than females, although early sexual abuse is more prevalent in the female population [88].
Different mediators and moderators of the association between childhood abuse and/or neglect and suicide behavior have been analyzed. They include age [78,86], gender [83,84], the presence of a psychiatric [89] or substance use [90], comorbidity, the characteristics of the abuser and the maltreatment experience, perceived social support and specific psychopathological symptoms such as impulsivity, dissociation, personality dysfunction, emotional dysregulation, depression, uncontrollable worry, low self-esteem, a sense of hopelessness, and feelings of worthlessness and guilt [90,91,92].
Several biological mechanisms by which childhood maltreatment increases the risk for suicide behavior have been proposed, including inflammation and other dysfunctions of the immune system, alteration in the HPA-axis, structural and functional brain changes, and genetic and epigenetic factors [93].
Early-life abuse causes the persistent hyperactivity of CRF and a markedly sensitized pituitary-adrenal and autonomic response, resulting in heightened stress responses. Individuals with a history of childhood maltreatment and suicide attempters exhibit lower plasmatic cortisol levels [94,95].
Childhood maltreatment has been associated with structural and functional neuroimaging changes that include lower grey matter volumes, decreased thickness, and hypoactivation in the ventral, medial, and dorsal prefrontal cortex, including the orbitofrontal and anterior cingulate cortices, HIPP, insula, and striatum. An association with decreased within and between white matter structural integrity regions has been described [84,85,93,96]. These alterations can lead to cognitive impairments, the disruption of emotional regulation, and an increased risk of suicidality.
Genetic and epigenetic mechanisms, especially related to HPA-axis genes, seem to interact with childhood abuse and/or neglect, increasing the risk of suicide behavior. Specifically, polymorphism of the following genes: corticotropin-releasing hormone receptor 1 (CRH1) and 2 (CRH2), FK506 binding protein 5 (FKBP5), and corticotropin-release hormone binding protein (CRHBP), could constitute specific mediators between childhood maltreatment and suicidality. FKBP5 (rs3800373, rs9296158, and rs306078) interactions with childhood trauma could increase the risk of suicide attempt, whereas variations in CRH1 (rs110402 and rs242924) would moderate the effect of children maltreatment on cortisol responses to Dexamethasone/CRH tests. Adults with a history of childhood maltreatment who carry the short-arm allele of the serotonin transporter promoter polymorphism are at a higher risk for suicidal ideation and attempts than homozygotes with two long-arm alleles. In addition, GWAS analyses have identified 14 independent loci for childhood maltreatment [93,97].
4. Hypothalamic-Pituitary-Adrenal Axis and Suicide
Early life stress has been associated with an aberrant HPA-axis activity in adulthood [98]. Some findings suggest that HPA-axis dysregulation could be related to endogenous forms of depression with greater suicide risk (Figure 2). However, the exact relationship between early life adversities, neuroendocrine changes later in life, and suicide remains to be determined.
Childhood trauma increases the risk of suicidal ideation and has been linked to HPA- axis dysregulation. The dexamethasone suppression test (DMS) has been used to evaluate the HPA-axis activity. Although this test presents low sensitivity and specificity, it has been suggested as a predictive marker of suicide behavior. The correlation between DMS and suicidal ideation has been analyzed in adolescent girls with a history of depression or depression plus self-injury. Interestingly, a reduction in post-DMS cortisol blood concentrations could be related to self-injury in depressed patients, suggesting a critical dysregulation of the HPA-axis negative feedback [99]. Therefore, a blunted cortisol reactivity to stress could be associated with an increased risk of suicidal behavior.
In a study conducted with 160 participants (100 women), a correlation between suicidal attempts or ideation, cortisol levels in saliva, and childhood trauma was evaluated. The authors found that the highest levels of childhood trauma were reported in suicidal attempts in more than 78% of cases. In addition, childhood trauma was a predictor of an impaired cortisol reactivity to stress and lower cortisol concentrations were associated with higher levels of trauma in patients with a suicidal history [100]. These results were analyzed in a general population study, investigating the correlation between childhood trauma, suicidal ideation or behavior later in life and basal cortisol urine levels. A total of 1094 participants were recruited, with a history of early life difficulties (including childhood and adolescence), suicidal ideation and attempt, and 24-h urine for cortisol concentration measurements. The results indicated that early stress exposure, especially during childhood, increases the risk of suicide by around 21%. However, early adversities during childhood and adolescence are equally crucial for suicidal ideation.
Interestingly, no association was found between suicidal ideation/behavior, early stress, and urine cortisol levels [101]. These findings are not consistent with those reported in previous studies on the HPA-axis dysregulation and suicide. These discrepancies could be primarily associated with the different types of samples used to quantify cortisol concentrations (urine, blood, or saliva) or, less importantly, with the moment of sample extraction.
An interesting aspect is that exposure to early life adversities could have a transgenerational impact affecting stress response in offspring. A sample of women with a history of major depressive disorder and childhood physical and sexual abuse has been used to analyze maternal and infant salivary cortisol levels during a laboratory stress paradigm at six months postpartum. Maternal early abuse relates to lower cortisol levels and reduced baseline cortisol in their offspring. A history of maternal abuse increases cortisol levels after laboratory stress exposure, and early abuse with comorbid PTSD in mothers induced a pronounced increase in cortisol levels in infants [102].
To further explore the potential relationship between the HPA-axis, suicide, and early life stress, the protein expression of CRH, FK506-binding protein (FKBP5), brain-derived neurotrophic factor (BDNF), and glucocorticoid receptors (GR) were analyzed in a study conducted using postmortem human prefrontal cortex (BA9) and anterior cingulate cortex (BA24) samples. The authors found a significant interaction between suicide and early life adversity in BA24, related to suicide behavior but not early life adversity. Therefore, this postmortem study revealed that brain alterations on targets closely related to the HPA-axis are not directly associated with suicidal behavior. Still, the BDNF protein levels could disclose a history of early life stress [103]. CRH gene expression levels were also analyzed in other brain regions, such as the frontopolar, dorsomedial, and ventrolateral PFC, from suicide victims (N = 12) and controls (N = 12).
Interestingly, CRH levels were increased in suicide victims versus controls in the frontopolar and dorsomedial PFC but not in the ventrolateral PFC. This increase was accompanied by a statistically significant reduction in CRH1 but not the CRH2 receptor gene expression in the frontopolar region of the PFC. [104]. The DLPFCx and anterior cingulate cortex (ACC) obtained from two different brain banks were evaluated in another study by Zhao and colleagues. The first one included samples from young depressed patients who died by suicide (MDD-S) and depressed patients who died from causes other than suicide (MDD-NS), and the second one included elderly depressed patients who did not commit suicide (DEP). In the ACC region, MMD-S patients presented increased levels of CRH gene expression compared with controls and MDD-NS patients. No differences were observed in the DLPFCx of all groups [105].
The protein and gene levels of some targets related to the HPA-axis activity were also analyzed in another study by Perez-Ortiz and colleagues. Amygdala (AMY) samples were used to analyze changes in the FKBP5 and Nr3c1 in suicide victims compared with controls. Interestingly, the authors found a statistically significant reduction in the targets’ gene and protein expression in this brain region intensely involved in emotional regulation [106]. The gene expression changes in both targets were also analyzed in the PFC of 121 brain samples of victims who died by suicide and 88 non-suicidal victims. In this study, the authors only found a significant reduction in the Nr3c1 transcript, and no differences were found in the case of the FKBP5 [107]. Perhaps because FKBP5 acts as a cochaperone that modulates glucocorticoid receptor activity in response to stressors, a reduction in the gene encoding the receptor means that FKBPA is unchanged.
Despite the interest in exploring central brain markers associated with the stress axis and suicidal behavior after an early life adversity, from a clinical point of view, the peripheral markers are more appropriate because of the facility to access their measurement in patients. Therefore, searching for peripheral changes in different targets should be the first step of the approach to identify suicide-related biomarkers in patients with a previous history of early life stress and set up effective preventive strategies. In this line, the available information is scarce, and more studies are needed to deeply explore this association.
5. Inflammation and Suicide
The relationship between inflammation and suicide has been widely explored, with heterogeneous results. The correlation between inflammation, suicide, and early life stress was evaluated in a study by Su and colleagues. Serum concentrations of inflammatory markers, HPA-axis markers, and metabolism were assessed for their potential association with suicidal behavior. Authors found higher concentrations of chemokine (C-X-C motif) ligand 1 (CXCL-1) in the serum of patients with suicide risk than non-suicidal patients. In these patients, the higher suicidal risk was associated with adulthood adversity and not early life stress [108].
Adverse childhood adversities are also strongly associated with self-harm behaviors. Russell and colleagues found a positive link between early life adversity and self-harm; however, no associations were reported about inflammatory biomarkers (interleukin (IL) 6 and C-reactive protein) [109]. The oxidative status has also been associated with suicidal behavior. Blood samples of patients with affective disorders and controls were analyzed, and alterations in the CMPAase/high-density lipoprotein (HDL) cholesterol levels were found in those exposed to early life stress. However, the direct correlation of these markers with suicide behaviors should be further investigated [110].
To assess the involvement of the immune system in suicide behavior in the early life stage, the gene and protein levels of the tumor necrosis factor-alpha (TNFα), IL-1β, and IL-6 were analyzed in the prefrontal cortex (PFC) of 24 teenage suicide completers and 24 matched controls. The results obtained in this study revealed a significant increase in the gene and protein expression of all three cytokines in the suicide victims, suggesting that these proinflammatory cytokines may have an essential role in suicide behavior [111]. In another study, the levels of different chemokynes and IL10 and IL16 in 16 suicide completers and 23 controls were evaluated in the PFC. The authors found a significant reduction in chemokines and IL10 levels (anti-inflammatory interleukine), whereas IL16 (pro-inflammatory interleukine) levels were increased in this brain region of suicide completers, supporting the critical role of the immune system in suicidal behavior [112].
Relative gene expression changes in different inflammatory markers involved in allergic processes (TNFα, IL-1β, IL-4, IL-5, IL-6, and IL-13) were analyzed in the orbitofrontal cortex of suicide completers with a history of major depressive disorder (MDD) versus controls. The authors reported increases in IL4 and IL13 gene expression in suicide completers compared with controls [113].
In blood samples, the plasma concentrations of different cytokines (IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, TNFα, epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF)) were analyzed using an ELISA assay, in suicide attempters with a history of MDD. In this study, a significant association between lower VEGF levels in the plasma and suicide completion was found, suggesting the involvement of angiogenesis and immune response in suicide behavior [114]. In another study, IL2, IL6, and TNFα concentrations were measured in the plasma of suicide attempters, non-suicidal depressed patients, and healthy controls. Increased concentrations of IL6 and TNF-α and decreased levels of IL2 were found in suicide attempters compared with non-suicidal depressed patients and healthy controls, demonstrating that these markers of the immune system’s activity could act as distinguishing markers between suicide and non-suicide behavior in depressed patients [115].
The concentrations of VEGF and IL8 were also measured in the cerebral spinal fluid (CSF) of suicidal attempters versus controls. The authors found lower concentrations of VEGF, suggesting a lack of trophic neuronal support and reduced neurogenesis in the HIPP of the patients, indicating more severe depressive status. Interestingly, IL6 levels did not differ between all the evaluated groups [116]. However, IL6 concentrations were significantly increased in the CSF of suicide attempters compared with controls. They were even higher in patients with a violent phenotype of suicide attempt compared with non-violent phenotypes [117].
A critical molecular link between inflammation and suicide is the tryptophan metabolism via the kynurenine pathway. This pathway is responsible for 90% of tryptophan degradation. Several proinflammatory cytokines (IL1 beta and IL6, among others) activate this pathway, increasing the synthesis of quinolinic (QA) or kynurenic (KA) acid. This QA can induce excitotoxicity through NMDA glutamatergic receptor activation. This pathway has been analyzed in suicide completers and suicide attempters. In the postmortem anterior cingulate cortex of suicide victims with MDD and controls, the authors found a significant reduction in kynurenic acid levels in MDD suicide victims compared with controls and MDD patients who did not die by suicide [118].
In summary, despite the extensive available information about the inflammation involvement in suicide, the specific association of the changes in the levels of different interleukins in suicidal behavior is not clear because of the heterogeneous results. This heterogeneity could be associated with the type of sample used for the analysis (postmortem brain samples, plasma, and CSF) and psychiatric comorbidities in patients. Therefore, the challenge of finding patients with suicidal behavior without any additional psychiatric comorbidity hampers the search for specific suicide-related biomarkers.
6. Neuropeptides and Suicide
Peptide hormones, such as vasopressin and oxytocin, play a crucial role in the normal and pathological functions of the central nervous system. They are involved in stress response and adaptation; the first studies analyzing the involvement of these neuropeptides in emotional regulation date to the late 90s. In these studies, authors found increased vasopressin concentrations in the plasma and brain postmortem samples of depressed patients. An increased number of vasopressin and oxytocin-positive neurons was also reported in the paraventricular nucleus of the hypothalamus [119,120]. The plasmatic concentrations of vasopressin have been associated with hypercortisolemia and suicide attempts in depressed patients, supporting the available information about the involvement of this neuropeptide in the HPA-axis regulation [121,122]. In a study by Brunner and colleagues, the authors evaluated the plasma and CSF concentrations of neurotransmitters and peptides, including vasopressin. The authors did not find any alteration in these hormones between MDD patients (nine of them being suicide attempters) compared with controls. Only a positive correlation was found between vasopressin and cortisol levels [123].
Similarly, plasma vasopressin levels were assessed in suicide attempters and non-attempters after DMS. No differences were found in the vasopressin concentrations between both groups of patients after the test [124]. However, considering vasopressin-induced regulation of the HPA axis, more studies are required to explore its potential involvement in suicidal behavior further.
Oxytocin is a nonapeptide that is intensely involved in childbirth and lactation, as well as social behavior, memory, and cognition. The peripheral concentrations of this neuropeptide were significantly reduced in suicide attempters compared with healthy subjects [125]. In addition, stress exposure, such as social exclusion, also decreased oxytocin concentrations in young adults with a suicide attempt history [126]. Oxytocin levels were also analyzed in the CSF and plasmatic samples of 28 drug-free suicide attempters and 19 healthy controls. The authors found lower CSF oxytocin levels compared to healthy volunteers, suggesting that this hormone may act as a predictor of suicide attempts [127]. These results indicate that oxytocin could by potentially useful as a biomarker of suicide behavior. However, more studies are needed to confirm this hypothesis.
In a study conducted in the early nineties, brain postmortem samples of suicide victims and age-matched controls were analyzed to evaluate potential changes in the neuropeptide Y concentrations. The authors measured this neuropeptide in the frontal cortex, temporal cortex, caudate nucleus, and cerebellum. The results revealed significantly reduced neuropeptide concentrations in the frontal cortex and caudate nucleus. Interestingly, these reductions were more robust in suicide victims with a history of MDD [128]. In addition, reduced gene expression of neuropeptide Y was found in the prefrontal cortex of suicidal patients with a history of bipolar disorder [129]. Some additional studies were carried out to reveal the involvement of neuropeptide Y in suicide. The expression of this peptide, along with its four receptors, was analyzed at the transcriptional and translational levels in the PFC and HIPP of the postmortem brain of normal healthy and depressed suicide subjects. The authors reported a statistically significant decrease in the neuropeptide Y (NPY) gene expression and an increase in the gene expression of its receptors NPY1R and NPY2R in both brain regions. In addition, a decrease in the protein levels of the peptide in the PFC was also found in depressed suicide victims [130]. Neuropeptide Y has been proposed as a resilience-related peptide, and its involvement in different neuropsychiatric disorders was also evaluated. More studies are necessary to explore its precise role in suicide behavior and its potential usefulness as a biomarker of suicidality.
7. Serotonergic System Alteration in Suicide Victims
Psychiatric disorders associated with serotonergic dysfunction include schizophrenia and MDD. Several medications to treat these disorders modulate the serotonergic system [131]. Both diseases have a high incidence of suicide victims, and depression and suicide have been associated with reduced serotonergic transmission. In the dorsal raphe nucleus (DRN), where the primary neurons innervate the prefrontal cortex [132], a decrease in the total number of 5-HT1A receptors was observed in suicide cases compared to controls [133]. In addition, the suicide group had fewer DRN neurons expressing the 5-HT1A gene than the control group [133]. An earlier study by Arango et al. (1995) found an increase in 5-HT1A receptor binding and a decrease in serotonin transporter binding in the ventrolateral prefrontal cortex in suicide cases, suggesting that alterations in the serotonin system occur primarily in these areas [134].
The protein TPH, involved in serotonergic neurotransmission, has been studied extensively. The gene for tryptophan hydroxylase is located at the 11P15.3-P14 locus. In 1994, Nielsen’s work was the first to report an association between suicide attempts and a polymorphism in intron 7 of the TPH gene [135]. Several years later, Turecki et al. (2001) found that one haplotype was more common in suicide completers than in controls, and this haplotype was also more common in patients who committed suicide by violent means [136]. However, further analysis did not reveal differences between controls and victims for the TPH1 gene at the single locus level nor the haplotype level in men of Slavic origin [137]. In a Japanese population, no significant association was found between TPH and 5-HT1A in suicide samples compared to controls [138]. In another study, TPH2 gene expression was significantly increased in the ventral prefrontal cortex of suicide completers compared to controls, but this could not be associated with the polymorphism SNPrs10748185 located in the promoter region of TPH2 and suicide [139].
The serotonin transporter (5-HTT) is responsible for the sodium-dependent serotonin reuptake, and the 5-HTT gene is located at the 17q11.1-q12 locus. Postmortem studies have found a significant frequency of the long allele of the 5-HTT gene in depressed suicide victims [140]. In 2003, an increase in the 5-HTTLPR L allele was found in the suicide group [141]. However, in the Chinese population, no association was found between changes in the 5-HHT genes and suicidal behavior [142]. Given these inconclusive findings, attributing suicidal behavior solely to genetic alterations in this system is overly simplistic. However, the serotonergic system is involved in both the predisposition to suicidal behavior related to decision-making and as a significant stressor [143]. Suicidal behavior is also intricately linked to genetic, environmental, and gender factors.
8. Endocannabinoid System Alteration in Suicide Victims
The endocannabinoid system (ECS) has emerged as a potential target in psychiatric disorders because it regulates emotional responses. The ECS also regulates cognitive processes, inflammation, chronic pain, and epilepsy [144,145]. Studies in rodents have shown that cannabinoid receptors are critical in responding to stress, anxiety, and depression [146,147,148,149,150,151,152,153]. A higher frequency of single nucleotide polymorphisms (SNP) of the CB1r gene (CNR1) was found in patients with MDD [154,155] and schizophrenia [156].
Based on previous animal studies, the CB2r in the central nervous system has a role as a possible anxiolytic and antidepressive target [157,158,159]. G protein-coupled receptor 55 (GPR55) is another target of endocannabinoids [160], with preliminary results suggesting that early life stress induces changes in GPR55 gene expression in mice [161]. Postmortem studies have shown that CB2r and GPR55 gene expression was significantly lower in the DLPCx of suicide victims, although CB2r protein expression was higher in said suicide victims. The presence of CB2-GPR55 receptor heteromers was also found in both neurons and astrocytes [162].
Curiously, an alteration in CB1r was also found in the DLPCx of suicide victims, with a higher CB1r density in alcoholics who died by suicide than in the control group, as confirmed by Western blot analysis. In addition, higher levels of anandamide (AEA) and 2-arachidonoylglycerol (2-AG) were found in the DLPCx of AS [163] (Figure 1). The same group has investigated changes in CB1r in the ventral striatum in alcohol-dependent suicides and found an upregulation of CB1r and an alteration of the FAAH enzyme in the ventral striatum [164]. Furthermore, CB1r gene expression was increased in the DLPCx of depressed suicide victims compared to controls [165]. A cross-sectional study conducted in 2020 found elevated levels of AEA and N-palmitoylethanolamine (PEA) in the serum of suicide attempters compared to controls [166]. Therefore, some evidence suggests that endocannabinoid system dysfunction (ECS) plays a relevant role in the pathophysiological aspects of suicidal behavior [167,168].
9. Excitatory and Inhibitory Balance Alteration in Suicide
Gamma-aminobutyric acid (GABA) and glutamate (Glu) are the mammalian central nervous system’s primary inhibitory and excitatory neurotransmitters and have been found to be involved in suicidal behavior. Alterations in excitatory and inhibitory neurotransmission have been extensively studied in patients with MDD who have or have not committed suicide. Notably, in 2004, Merali et al. showed that the gene expression of CRH and GABAA in the PFC were altered in depressed suicides, consistent with changes in the regulation of the HPA-axis in suicide cases [104]. Other studies have also demonstrated disturbances in the balance between excitatory and inhibitory processes in suicide. In 2005, Jones’ group identified the significant downregulation of SLC1A2 and SLC1A3, critical members of the glutamate-neutral amino acid transporter protein family, as well as L-glutamate ammonia ligase, an enzyme responsible for converting glutamate to nontoxic glutamine [169]. These alterations could significantly increase extracellular glutamate levels, potentially leading to neurotoxicity and reduced signaling efficiency. In 2023, our research group showed a decrease in vesicular GABA transporter (VGAT) immunoreactivity and an increase in vesicular glutamatergic transporter-1 (VGluT1) immunoreactivity in the HIPP of individuals who died by suicide [170].
Using microarray analysis and RT-PCR, Turecki’s group showed in 2009 that glutamatergic and GABAergic-related genes were globally altered in prefrontal cortical areas and the HIPP in suicide cases [171]. A protein-coding transcript (ENST00000414552) of the GABA-A receptor, gamma 2 (GABRG2), presented lower brain expression in postmortem suicides and was significantly decreased in the ACC in mood disorders [172,173]. Consistent with these results, a recent RT-PCR analysis of 32 genes encoding proteins directly involving glutamatergic or GABAergic synaptic transmission revealed the significantly increased expression of genes associated with these processes in the ACC in individuals with MDD who died by suicide (MDD-S). Conversely, in the DLPFCx, the expression of these genes was decreased in MDD-S cases [174].
In conclusion, several factors and systems are altered in individuals who die by suicide (Table 1). Further research is needed to identify biomarkers that can serve as early warning signs for healthcare professionals and help prevent suicidal behavior.
10. Epigenetic Changes in Suicidal Behavior
Epigenetic studies examine the interaction between the environmental and genetic risk factors of suicide. Epigenetic alterations include DNA methylation, histone acetylation and non-coding RNAs, which control gene expression without affecting the DNA sequence. DNA methylation is one of the most studied epigenetic modifications. It is regulated by DNA methyltransferases (DNMTs), involving the addition of a methyl (-CH3) group to the fifth carbon of a cytosine–guanine (CpG) dinucleotide. This epigenetic modification is associated with the repression of gene expression [175].
The evidence achieved to date identified DNA methylation alterations in genes involved in stress response and neuronal plasticity in the peripheral blood and brain regions of psychiatric patients who died by suicide, with previous suicide attempts or suicidal ideation (Figure 3).
10.1. DNA Methylation Alterations in Peripheral Blood Tissues
DNA methylation changes have been found in the peripheral blood tissues of patients with suicidal ideations and behaviors. One of the most well-studied genes in the epigenetics of suicide is the NR3C1 gene, which encodes the glucocorticoid receptor (GCr) [176]. This receptor is involved in cortisol signaling, stress, and inflammatory responses [177,178]. Abnormalities in the methylation status of NR3C1 impact the regulation of the negative feedback loop of the HPA-axis, inducing a poorer adaptation to stress [179]. In lymphocytes from women with bulimia nervosa and comorbid bipolar disorder (BPD) or a history of suicidality, higher methylation was found in specific GR exon 1C promoter sites [180]. In addition, the hypermethylation of promoters of NR3C1, FK506 binding protein 5 (FKBP5), and CRHBP genes, additional critical elements of the HPA axis, were found in major depressive MDD patients with and without suicidal ideation. Interestingly, these genes’ methylation degree was positively correlated with severe suicidal ideation [181]. Moreover, epigenetic changes in the CRH gene (hypomethylation of two CpG CRH cg19035496 and cg234090749) were found in adult suicide attempters. Curiously, the hypermethylation of cg19035496 was linked with a high general psychiatric risk score in adolescents [182].
SKA2 is another gene that regulates GCr nuclear transactivation [183,184]. Epigenetic SKA2 gene variations have been proposed to impact the modulation of HPA-axis function [183], and the increased methylation of SKA2 was identified in the blood of suicide victims [185].
DNA methylation alterations, which are involved in neuroplasticity, have also been found in the BDNF. Higher methylation levels of the BDNF promoter were identified in MDD patients with suicidal ideation compared to those without [186]. Similarly, higher BDNF promoter methylation levels were significantly associated with a previous history of suicide attempts, suicide ideation during treatment, higher Beck Scale for Suicide Ideation (BSS) scores, and poor treatment outcomes for suicidal ideation [187]. In addition, the hypermethylation of BDNF promoters was found in MDD patients with and without suicidal ideation. The degree of methylation was positively correlated with severe suicidal ideation [181]. In agreement with these findings, a recent study contributes to establishing a connection between the increased methylation of BDNF and severe suicidal behavior in women [188].
Similarly, increased BDNF methylation was associated with suicidal ideation and depression one year after breast surgery in women with breast cancer [189]. However, hypomethylation of the BDNF region upstream of exon I has been found in blood samples of suicide victims. In contrast, no differences in DNA methylation were observed in the hippocampus or the DLPFCx [190].
Some studies revealed epigenetic alterations in genes coding for the critical elements of the monoaminergic system. In the case of serotonin receptor 1A (HTR1A), hypomethylation was found in the blood of suicide victims. For amplicon monoamine oxidase A (MAOA) gene exon I (MAOA_1), the results showed increased blood methylation in suicide victims [185]. In female affective disorder patients with a history of violent suicide attempters, the decreased methylation of the MAOA gene exon I promoter region was identified in DNA samples of peripheral blood cells [191]. The blood methylation status of the SCL6A4 gene, which encodes the serotonin transporter, has been associated with suicidal ideation in stroke patients [192]. Zhang and colleagues evaluated the Tryptophan Hydroxylase TPH2 methylation, an enzyme involved in serotonin synthesis [193], in peripheral blood samples in patients diagnosed with MDD who had attempted suicide and control patients with MDD. The results revealed that TPH2 was hypermethylated in MDD with suicide. This epigenetic change was also associated with reduced TPH2 mRNA levels [194]. However, in the study by Kouter and colleagues, hypomethylation of TPH2 was found in the blood of suicide victims [185].
Recently, differences in the methylation of the Cyclin-Dependent Kinase 5 (CDK5) gene have been found in the PMBCs of US military veterans with suicide attempts [195]. CDK5 is highly expressed in the adult brain and is relevant in regulating neuronal growth, survival, learning, and memory [196]. Interestingly, significant differences in the expression of CDK5 were identified in the PFC of individuals who died by suicide [197].
GWASs provide relevant information regarding a different blood methylation profile in suicide. Such is the case of the study by Jeremian and colleagues, who found a different blood methylation profile between BPD patients with and without suicidal behaviors. More specifically, there is less methylation in the 5′ untranslated region of Membrane palmitoylated protein 4 (MMP4) and intron 3 of TRE2/BUB2/CDC16 domain family member 16 (TBC1D16) and less methylation in exon 1 of nucleoporin 133 (NUP133) in BPD patients with a history of suicidal behaviors [198].
In addition, hypomethylation in the CpG site cg19647197 within the CCDC53 gene was found in the white blood cells of schizophrenic suicide attempters [199], which is a core subunit of the WASH complex involved in endosomal fission [200].
Finally, DNA methylation in regulatory regions of the Elovl5 gene (elongation of very long-chain fatty acids protein 5) was associated with the diagnosis of MDD and suicide attempts. This epigenetic change explains the connection between plasma polyunsaturated fatty acid (PUFA) levels and suicide risk [201].
10.2. DNA Methylation Alterations in the Brain from Postmortem Studies
Postmortem studies have identified DNA methylation alterations in different brain regions of individuals who died by suicide. As described in blood peripheral cells, hypermethylation of the NR3C1 gene was detected in the HIP of individuals who died by suicide with a history of childhood abuse [202]. Moreover, decreased levels of mRNA, mRNA transcripts bearing the glucocorticoid receptor 1F splice variant, and increased cytosine methylation of the NR3C1 promoter have been identified in the same samples [203]. Recently, lower methylation levels of the 1B promoter have been determined in the HIP of suicide victims, where methylation levels were higher in the insula and blood. On the other hand, mixed methylation patterns were found in the amygdala and Broadman area 46 [185]. Complementarily, Rizavi and colleagues found a strong correlation between the DNA methylation status and gene expression changes in specific NR3C1 exon-1 variants in the PFC of teenage suicide completers. Moreover, in the HIP and PFC, the aberrant expression of DNA methylating and demethylating enzymes was also identified [204].
An additional gene evaluated was SKA2 due to its connection with GCr. The opposite methylation status was found in suicide victims, depending on the brain region analyzed. Decreased SKA2 methylation was found In the HIP, whereas increased methylation was identified in the insula [185]. A complementary study on individuals with high interpersonal violence and psychosocial stress rates showed that SKA2 DNA methylation variations mediate vulnerability to suicidal behaviors and PTSD through the dysregulation of the HPA axis in response to stress [205]. Furthermore, an altered methylation status at SKA2 and three additional CpGs (ATP8A1, LOC153328, and KCNAB2) were found in the frontal cortex of suicide victims [206]. Curiously, a strong correlation has been observed with the NR3C1 and SKAAK2, since suicide victims often have increased DNA methylation of one or the other [207].
Analysis of the methylation status of the BDNF promoter received particular interest due to its role in neuroplasticity. Higher levels of methylation in the BDNF promoter were identified in the Wernicke area of suicide victims compared to controls. Interestingly, this methylation status was associated with lower mRNA expression [208]. The same authors carried out one study analyzing the methylation status and gene expression of the tropomyosin-related kinase B (NTRK2), one of the receptors of BDNF, without detecting differences [209]. Curiously, the methylation state of the promoter region of the truncated variant of the TrkB receptor (TrkB.T1) was associated with its expression in the frontal areas of individuals who died by suicide [210]. In addition, hypermethylation of the TrKB-T1 3’UTR region was found in the frontal cortex (BA8/9) of suicide completers, showing an association with reduced TrKB-T1 expression [211]. These epigenetic alterations could be underlying the plasticity changes observed in suicide completers.
Recently, another study evaluated potential epigenetic alterations in genes coding critical elements of the serotoninergic system, the SLC6A4 and the HTR1A. Hypomethylation of the SLC6A4 gene has been identified in the BA46 of suicide victims. On the contrary, the methylation pattern was mixed in the other measured tissues (HIP, amygdala, and insula). In the case of HTR1A, the study revealed hypermethylation in the insula and mixed methylation in the HIP, AMY, and BA46 [185]. In the same study, epigenetic alterations were analyzed in the TPH2, observing hypomethylation in the BA46 and hypermethylation in the HIP. Moreover, differences in the methylation of MAOA, an enzyme involved in serotonin degradation [212], were found in the HIP, insula, AMY, and Brodmann area 46 of suicide victims [185]. Altogether, these results revealed epigenetic alterations in critical elements of the monoaminergic system.
Furthermore, DNA methylation alterations have also been analyzed in GABA receptors. Alterations in the functioning of the inhibitory GABAergic signaling have been proposed as one of the etiopathogenic mechanisms underlying different neuropsychiatric disorders, including suicide. Hypermethylation of the GABAA receptor alpha 1 subunit promoter region was found in the frontopolar cortex of individuals who committed suicide and were diagnosed with MDD [213]. In line with this finding, a recent study found differences in the methylation status for the amplicons GABRA1_1 and GABRA1_2 [185].
Finally, GWAS methylation studies provide relevant information about altered methylation patterns in different brain regions of suicidal samples. In the HIP, Labonte and colleagues found differences in the methylation patterns of male suicide victims, the majority of them hypermethylated and closely related to cognitive processes, such as NR2E1, which encodes a brain-specific orphan nuclear receptor acting as a transcriptional repressor [214]; GRM7, which codes for the G-protein coupled metabotropic glutamate receptor subunit 7 [215]; CHRNB2, encoding a brain-specific subunit (β2) of the ligand-gated ionotropic nicotinic acetylcholine receptor family [216,217]; and DBH, coding for a catecholamine-synthetic membrane-bound enzyme responsible for the synthesis of norepinephrine [218]. Interestingly, promoter methylation differences were inversely correlated with gene expression differences [202].
In the PFC of male death by suicide and controls, Schneider and colleagues identified differences in methylation patterns between groups studying single CpGs over the genome. The study highlights the enrichment of the genes APLP2 (encodes the amyloid precursor-like protein 2), BDNF, HTR1A (encodes the serotonin receptor 1A), NUAK1 (encodes the enzyme AMPK-related protein kinase 5), PHACTR3 (encodes a member of the phosphatase and actin regulator protein family), MSMP (encodes the prostate-associated microsemiprotein), SLC6A4, SYN2 (synapsin 2), and SYNE2 (codes the Spectrin Repeat Containing Nuclear Envelope Protein 2) and supports a role for epigenetics in the pathophysiology of suicide [219]. Gaine and cols. found that 55% of the differentially methylated regions (DMRs) were hypermethylated in the PFC of suicidal samples. The genes found to be altered and methylated belonged to several pathways, including axonal guidance signaling, calcium signaling, β-adrenergic signaling, and opioid signaling [220]. Similarly, altered DNA methylation patterns (affecting 4430 genomic regions) were found in the PFC of males who died by suicide, identifying 10 genes with potential relevance to suicide and psychiatric disorders involved in synaptic plasticity, HPA-axis, and additional pathways [221]. Complementary studies found different methylation levels in the PFC of suicide victims [222,223]. Interestingly, Cabrera-Mendoza and colleagues found a significant correlation between 22CpGs and gene expression in suicide victims [224].
Kouter and colleagues examined alterations in the pattern of DNA methylation in the HIP and PFC of suicide victims, finding differences in the methylation levels of approximately 3000 CpGs. The gene analyses provide information about enrichment for genes associated with cell structural integrity and nervous system regulation [225].
In an additional GWAS study, hypomethylation in the intronic region of the ELAVL4 gene was found in the PFC of individuals who died by suicide. This gene plays a role in the translation and stabilization of mRNA, modulating neuronal development and maintenance. In the cerebellum, the altered methylation status of six genes related to long-term synaptic depression has been found between suicide completers and controls [11].
In summary, several studies on DNA methylation have been conducted in recent years, contributing to a better understanding of the epigenetic mechanisms underlying suicide. These studies revealed DNA methylation alterations in the serotoninergic system, HPA and neuroplasticity markers. However, it is hard to achieve conclusive results, mainly due to the differences in the methodology employed by each study and the sample analyzed.
11. Conclusions
This article reviews the molecular changes occurring in individuals with psychiatric disorders or those undergoing epigenetic modifications due to adversity, precipitating suicidal behavior.
Individuals struggling with a psychiatric disorder such as MDD, BP, or schizophrenia are more likely to manifest suicidal behavior. Alterations in the serotonergic system, HPA-axis, GABAergic/glutamatergic system and BDNF reduction were reported in BP, MDD and schizophrenic patients. Increased proinflammatory cytokines and changes in the HPA-axis were also detected in patients with AD. In the case of BPD, the inclination towards suicidal behavior is often intertwined with comorbidities. Nevertheless, impulsive and unforeseen suicide cases may arise from an inadequate ability to cope with stressful situations. Indeed, early-life adversity may induce heightened stress and anxiety, ultimately leading to the modification of the HPA-axis, potentially escalating susceptibility to suicidal tendencies (Figure 2).
Suicide victims exhibit diverse central and peripheral alterations, irrespective of a prior psychiatric diagnosis. Notably, DNA methylation changes have been documented in the peripheral blood tissues of individuals with suicidal ideation and behavior. For instance, epigenetic alteration in the methylation status of the NR3C1 gene, which encodes the GCr [176], which is involved in cortisol signaling, stress, and inflammatory responses [177,178], was found in individuals with childhood abuse or exposure to a highly stressful situation that may trigger PTSD later [205]. Also, genetic alterations in this serotonergic system have been found in suicide victims.
Other systems are also affected by suicidal behavior. The study of the ECS has been of great importance in recent years. Postmortem studies have shown that CB2r and GPR55 gene expression was significantly lower in the DLPCx of suicide victims, although CB2r protein expression was higher in suicide victims. In addition, several alterations in the GABAergic and glutamatergic balance, as well as an increase in the inflammatory interleukins IL-1, IL-6, and TNF-alpha and a decrease in BDNF, were found in the PFC of suicide victims.
In summary, suicidal behavior may result from a confluence of factors. It is imperative to develop a comprehensive, multifaceted suicide prevention strategy highlighting the severity of suicide as a global and preventable issue.
12. Methods
The literature review consisted of an exhaustive search for scientific information in the Medline database (PubMed). To identify molecular alterations and risk factors of suicide, the following keywords and their combinations were used: “major depression disorder” AND “molecular alteration” AND “suicide”, “bipolar disorder” AND “molecular alteration” AND “suicide”, “borderline personality disorder” AND “molecular alteration” AND “suicide”,” anxiety disorder” AND “molecular alteration” AND “suicide”, “schizophrenia” AND “molecular alteration” AND “suicide”, “substance use disorder” AND “molecular alteration” AND “suicide”, “early life adversity” AND “suicide”, “inflammation factor alteration” AND suicide”, “neuroendocrine system alteration” AND “suicide”, “serotonergic system” AND “suicide”, “endocannabinoid system alteration” AND “suicide”, “GABAergic system alteration” AND “suicide” “Glutamatergic system alteration” AND “suicide” “Epigenetic changes” AND “suicide”. To search gene alteration the following keywords and their combinations were used: “major depression disorder” AND “gene alteration” AND “suicide”, “bipolar disorder” AND “gene alteration” AND “suicide”, “borderline personality disorder” AND “gene alteration” AND “suicide”,” anxiety disorder” AND “gene alteration” AND “suicide”, “schizophrenia” AND “gene alteration” AND “suicide”, “substance use disorder” AND “gene alteration” AND “suicide”. AND “screening tools” were combined with terms related to the technical approach using the Boolean operator “AND”; “molecular changes”, “gene alteration” AND “suicide”. References of identified publications were included in the additional searches. Articles published in predatory journals were excluded from the screening process.
Author Contributions
J.M. designed, coordinated, and reviewed the sections and contents of the review manuscript. D.N. reviewed the sections and contents of the review manuscript. J.M. oversaw the organization to distribute the writing tasks among the authors. D.N., M.M.-M., A.G., M.S.G.-G. and G.R. performed the literature searches. D.N., M.M.-M., A.G., M.S.G.-G. and G.R. participated in the manuscript writing. All authors have read and agreed to the published version of the manuscript.
Funding
The preparation of the manuscript was supported by “Red de Investigación en Atención Primaria de Adicciones” RD21/0009/0008.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Suicide Worldwide in 2019; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Wislowska-Stanek, A.; Kolosowska, K.; Maciejak, P. Neurobiological Basis of Increased Risk for Suicidal Behaviour. Cells 2021, 10, 2519. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Parisi, V.M.; Aguglia, A.; Amerio, A.; Sampogna, G.; Fiorillo, A.; Pompili, M.; Amore, M. A Specific Inflammatory Profile Underlying Suicide Risk? Systematic Review of the Main Literature Findings. Int. J. Environ. Res. Public Health 2020, 17, 2393. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J. Neurobiology of suicidal behaviour. Nat. Rev. Neurosci. 2003, 4, 819–828. [Google Scholar] [CrossRef]
- Thomas, N.; Armstrong, C.W.; Hudaib, A.R.; Kulkarni, J.; Gurvich, C. A network meta-analysis of stress mediators in suicide behaviour. Front. Neuroendocrinol. 2021, 63, 100946. [Google Scholar] [CrossRef]
- Piras, I.S.; Huentelman, M.J.; Pinna, F.; Paribello, P.; Solmi, M.; Murru, A.; Carpiniello, B.; Manchia, M.; Zai, C.C. A review and meta-analysis of gene expression profiles in suicide. Eur. Neuropsychopharmacol. 2022, 56, 39–49. [Google Scholar] [CrossRef]
- Galfalvy, H.; Zalsman, G.; Huang, Y.Y.; Murphy, L.; Rosoklija, G.; Dwork, A.J.; Haghighi, F.; Arango, V.; Mann, J.J. A pilot genome wide association and gene expression array study of suicide with and without major depression. World J. Biol. Psychiatry 2013, 14, 574–582. [Google Scholar] [CrossRef]
- Tidemalm, D.; Runeson, B.; Waern, M.; Frisell, T.; Carlstrom, E.; Lichtenstein, P.; Langstrom, N. Familial clustering of suicide risk: A total population study of 11.4 million individuals. Psychol. Med. 2011, 41, 2527–2534. [Google Scholar] [CrossRef]
- Baldessarini, R.J.; Hennen, J. Genetics of suicide: An overview. Harv. Rev. Psychiatry 2004, 12, 1–13. [Google Scholar] [CrossRef]
- Roy, A.; Rylander, G.; Sarchiapone, M. Genetics of suicides. Family studies and molecular genetics. Ann. N. Y. Acad. Sci. 1997, 836, 135–157. [Google Scholar] [CrossRef] [PubMed]
- Policicchio, S.; Washer, S.; Viana, J.; Iatrou, A.; Burrage, J.; Hannon, E.; Turecki, G.; Kaminsky, Z.; Mill, J.; Dempster, E.L.; et al. Genome-wide DNA methylation meta-analysis in the brains of suicide completers. Transl. Psychiatry 2020, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Statham, D.J.; Heath, A.C.; Madden, P.A.; Bucholz, K.K.; Bierut, L.; Dinwiddie, S.H.; Slutske, W.S.; Dunne, M.P.; Martin, N.G. Suicidal behaviour: An epidemiological and genetic study. Psychol. Med. 1998, 28, 839–855. [Google Scholar] [CrossRef]
- Sveticic, J.; De Leo, D. The hypothesis of a continuum in suicidality: A discussion on its validity and practical implications. Ment. Illn. 2012, 4, e15. [Google Scholar] [CrossRef]
- Tondo, L.; Pompili, M.; Forte, A.; Baldessarini, R.J. Suicide attempts in bipolar disorders: Comprehensive review of 101 reports. Acta Psychiatr. Scand. 2016, 133, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.; Isometsa, E.T.; Azorin, J.M.; Cassidy, F.; Goldstein, T.; Rihmer, Z.; Sinyor, M.; Tondo, L.; Moreno, D.H.; Turecki, G.; et al. A review of factors associated with greater likelihood of suicide attempts and suicide deaths in bipolar disorder: Part II of a report of the International Society for Bipolar Disorders Task Force on Suicide in Bipolar Disorder. Aust. N. Z. J. Psychiatry 2015, 49, 1006–1020. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.; Isometsa, E.T.; Tondo, L.; Moreno, D.H.; Sinyor, M.; Kessing, L.V.; Turecki, G.; Weizman, A.; Azorin, J.M.; Ha, K.; et al. Epidemiology, neurobiology and pharmacological interventions related to suicide deaths and suicide attempts in bipolar disorder: Part I of a report of the International Society for Bipolar Disorders Task Force on Suicide in Bipolar Disorder. Aust. N. Z. J. Psychiatry 2015, 49, 785–802. [Google Scholar] [CrossRef]
- Da Silva Costa, L.; Alencar, A.P.; Nascimento Neto, P.J.; dos Santos Mdo, S.; da Silva, C.G.; Pinheiro, S.d.F.L.; Silveira, R.T.; Bianco, B.A.; Pinheiro, R.F., Jr.; de Lima, M.A.; et al. Risk factors for suicide in bipolar disorder: A systematic review. J. Affect. Disord. 2015, 170, 237–254. [Google Scholar] [CrossRef]
- Plans, L.; Barrot, C.; Nieto, E.; Rios, J.; Schulze, T.G.; Papiol, S.; Mitjans, M.; Vieta, E.; Benabarre, A. Association between completed suicide and bipolar disorder: A systematic review of the literature. J. Affect. Disord. 2019, 242, 111–122. [Google Scholar] [CrossRef]
- Dong, M.; Zeng, L.N.; Lu, L.; Li, X.H.; Ungvari, G.S.; Ng, C.H.; Chow, I.H.I.; Zhang, L.; Zhou, Y.; Xiang, Y.T. Prevalence of suicide attempt in individuals with major depressive disorder: A meta-analysis of observational surveys. Psychol. Med. 2019, 49, 1691–1704. [Google Scholar] [CrossRef] [PubMed]
- Tondo, L.; Vazquez, G.H.; Baldessarini, R.J. Prevention of suicidal behavior in bipolar disorder. Bipolar Disord. 2021, 23, 14–23. [Google Scholar] [CrossRef]
- Goldstein, T.R.; Merranko, J.; Hafeman, D.; Gill, M.K.; Liao, F.; Sewall, C.; Hower, H.; Weinstock, L.; Yen, S.; Goldstein, B.; et al. A risk calculator to predict suicide attempts among individuals with early-onset bipolar disorder. Bipolar Disord. 2022, 24, 749–757. [Google Scholar] [CrossRef]
- Buoli, M.; Cesana, B.M.; Bolognesi, S.; Fagiolini, A.; Albert, U.; Di Salvo, G.; Maina, G.; de Bartolomeis, A.; Pompili, M.; Palumbo, C.; et al. Factors associated with lifetime suicide attempts in bipolar disorder: Results from an Italian nationwide study. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 359–370. [Google Scholar] [CrossRef]
- Miola, A.; Fountoulakis, K.N.; Baldessarini, R.J.; Veldic, M.; Solmi, M.; Rasgon, N.; Ozerdem, A.; Perugi, G.; Frye, M.A.; Preti, A. Prevalence and outcomes of rapid cycling bipolar disorder: Mixed method systematic meta-review. J. Psychiatr. Res. 2023, 164, 404–415. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Lu, L.; Zhang, L.; Zhang, Q.; Ungvari, G.S.; Ng, C.H.; Yuan, Z.; Xiang, Y.; Wang, G.; Xiang, Y.T. Prevalence of suicide attempts in bipolar disorder: A systematic review and meta-analysis of observational studies. Epidemiol. Psychiatr. Sci. 2019, 29, e63. [Google Scholar] [CrossRef] [PubMed]
- Huber, R.S.; Coon, H.; Kim, N.; Renshaw, P.F.; Kondo, D.G. Altitude is a risk factor for completed suicide in bipolar disorder. Med. Hypotheses 2014, 82, 377–381. [Google Scholar] [CrossRef]
- Engstrom, C.; Brandstrom, S.; Sigvardsson, S.; Cloninger, C.R.; Nylander, P.O. Bipolar disorder. III: Harm avoidance a risk factor for suicide attempts. Bipolar Disord. 2004, 6, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Carra, G.; Bartoli, F.; Crocamo, C.; Brady, K.T.; Clerici, M. Attempted suicide in people with co-occurring bipolar and substance use disorders: Systematic review and meta-analysis. J. Affect. Disord. 2014, 167, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Buyuksandalyaci Tunc, E.; Gul, O. Difficulties in Emotion Regulation: Are They the Preventable Cause of Suicide, Impulsivity, and Aggression in Schizophrenia and Bipolar Disorder? Psychiatr. Danub. 2023, 35, 38–46. [Google Scholar] [CrossRef]
- Benedetti, F.; Radaelli, D.; Poletti, S.; Locatelli, C.; Falini, A.; Colombo, C.; Smeraldi, E. Opposite effects of suicidality and lithium on gray matter volumes in bipolar depression. J. Affect. Disord. 2011, 135, 139–147. [Google Scholar] [CrossRef]
- Johnston, J.A.Y.; Wang, F.; Liu, J.; Blond, B.N.; Wallace, A.; Liu, J.; Spencer, L.; Cox Lippard, E.T.; Purves, K.L.; Landeros-Weisenberger, A.; et al. Multimodal Neuroimaging of Frontolimbic Structure and Function Associated With Suicide Attempts in Adolescents and Young Adults With Bipolar Disorder. Am. J. Psychiatry 2017, 174, 667–675. [Google Scholar] [CrossRef]
- Fan, S.; Lippard, E.T.C.; Sankar, A.; Wallace, A.; Johnston, J.A.Y.; Wang, F.; Pittman, B.; Spencer, L.; Oquendo, M.A.; Blumberg, H.P. Gray and white matter differences in adolescents and young adults with prior suicide attempts across bipolar and major depressive disorders. J. Affect. Disord. 2019, 245, 1089–1097. [Google Scholar] [CrossRef]
- Sandberg, J.V.; Hansson, C.; Goteson, A.; Joas, E.; Jakobsson, J.; Palsson, E.; Landen, M. Proteins associated with future suicide attempts in bipolar disorder: A large-scale biomarker discovery study. Mol. Psychiatry 2022, 27, 3857–3863. [Google Scholar] [CrossRef] [PubMed]
- Mullins, N.; Bigdeli, T.B.; Borglum, A.D.; Coleman, J.R.I.; Demontis, D.; Mehta, D.; Power, R.A.; Ripke, S.; Stahl, E.A.; Starnawska, A.; et al. GWAS of Suicide Attempt in Psychiatric Disorders and Association With Major Depression Polygenic Risk Scores. Am. J. Psychiatry 2019, 176, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Lybech, L.K.M.; Calabro, M.; Briuglia, S.; Drago, A.; Crisafulli, C. Suicide Related Phenotypes in a Bipolar Sample: Genetic Underpinnings. Genes 2021, 12, 1482. [Google Scholar] [CrossRef] [PubMed]
- Bigdeli, T.B.; Barr, P.B.; Rajeevan, N.; Graham, D.P.; Li, Y.; Meyers, J.L.; Gorman, B.R.; Peterson, R.E.; Sayward, F.; Radhakrishnan, K.; et al. Correlates of suicidal behaviors and genetic risk among United States veterans with schizophrenia or bipolar I disorder. medRxiv 2023, preprint. [Google Scholar] [CrossRef]
- Cai, H.; Jin, Y.; Liu, S.; Zhang, Q.; Zhang, L.; Cheung, T.; Balbuena, L.; Xiang, Y.T. Prevalence of suicidal ideation and planning in patients with major depressive disorder: A meta-analysis of observation studies. J. Affect. Disord. 2021, 293, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Casanas, I.C.C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Sanches, M.; Nguyen, L.K.; Chung, T.H.; Nestadt, P.; Wilcox, H.C.; Coryell, W.H.; Soares, J.C.; Selvaraj, S. Anxiety symptoms and suicidal thoughts and behaviors among patients with mood disorders. J. Affect. Disord. 2022, 307, 171–177. [Google Scholar] [CrossRef]
- Olgiati, P.; Serretti, A. Persistence of suicidal ideation within acute phase treatment of major depressive disorder: Analysis of clinical predictors. Int. Clin. Psychopharmacol. 2022, 37, 193–200. [Google Scholar] [CrossRef]
- Olgiati, P.; Fanelli, G.; Serretti, A. Clinical correlates and prognostic implications of severe suicidal ideation in major depressive disorder. Int. Clin. Psychopharmacol. 2023, 38, 201–208. [Google Scholar] [CrossRef]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Kim, K.Y.; Shin, K.Y.; Chang, K.A. Potential Inflammatory Biomarkers for Major Depressive Disorder Related to Suicidal Behaviors: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 13907. [Google Scholar] [CrossRef]
- Kanwar, A.; Malik, S.; Prokop, L.J.; Sim, L.A.; Feldstein, D.; Wang, Z.; Murad, M.H. The association between anxiety disorders and suicidal behaviors: A systematic review and meta-analysis. Depress. Anxiety 2013, 30, 917–929. [Google Scholar] [CrossRef]
- Abreu, L.N.; Oquendo, M.A.; Galfavy, H.; Burke, A.; Grunebaum, M.F.; Sher, L.; Sullivan, G.M.; Sublette, M.E.; Mann, J.; Lafer, B. Are comorbid anxiety disorders a risk factor for suicide attempts in patients with mood disorders? A two-year prospective study. Eur. Psychiatry 2018, 47, 19–24. [Google Scholar] [CrossRef]
- Stanley, I.H.; Boffa, J.W.; Rogers, M.L.; Hom, M.A.; Albanese, B.J.; Chu, C.; Capron, D.W.; Schmidt, N.B.; Joiner, T.E. Anxiety sensitivity and suicidal ideation/suicide risk: A meta-analysis. J. Consult. Clin. Psychol. 2018, 86, 946–960. [Google Scholar] [CrossRef]
- Gilmour, H. Threshold and subthreshold Generalized Anxiety Disorder (GAD) and suicide ideation. Health Rep. 2016, 27, 13–21. [Google Scholar]
- Wiebenga, J.X.M.; Dickhoff, J.; Merelle, S.Y.M.; Eikelenboom, M.; Heering, H.D.; Gilissen, R.; van Oppen, P.; Penninx, B. Prevalence, course, and determinants of suicide ideation and attempts in patients with a depressive and/or anxiety disorder: A review of NESDA findings. J. Affect. Disord. 2021, 283, 267–277. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, J.; Xiong, X.; Jian, Q.; Zhang, L.; Xiang, M.; Zhou, B.; Zou, Z. Suicidality in patients with primary diagnosis of panic disorder: A single-rate meta-analysis and systematic review. J. Affect. Disord. 2022, 300, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Albert, U.; De Ronchi, D.; Maina, G.; Pompili, M. Suicide Risk in Obsessive-Compulsive Disorder and Exploration of Risk Factors: A Systematic Review. Curr. Neuropharmacol. 2019, 17, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Tietbohl-Santos, B.; Chiamenti, P.; Librenza-Garcia, D.; Cassidy, R.; Zimerman, A.; Manfro, G.G.; Kapczinski, F.; Passos, I.C. Risk factors for suicidality in patients with panic disorder: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 105, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Bentley, K.H.; Franklin, J.C.; Ribeiro, J.D.; Kleiman, E.M.; Fox, K.R.; Nock, M.K. Anxiety and its disorders as risk factors for suicidal thoughts and behaviors: A meta-analytic review. Clin. Psychol. Rev. 2016, 43, 30–46. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, L.; Maietti, E.; Rucci, P.; Casadei, G.; Maina, G.; Fineberg, N.A.; Albert, U. Suicide attempts and suicidal ideation in patients with obsessive-compulsive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 276, 1001–1021. [Google Scholar] [CrossRef]
- Fiori, L.M.; Wanner, B.; Jomphe, V.; Croteau, J.; Vitaro, F.; Tremblay, R.E.; Bureau, A.; Turecki, G. Association of polyaminergic loci with anxiety, mood disorders, and attempted suicide. PLoS ONE 2010, 5, e15146. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, A.; Guardia, A.; Gonzalez-Rodriguez, A.; Betriu, M.; Palao, D.; Monreal, J.A.; Soria, V.; Labad, J. A systematic review and meta-analysis of suicidality in psychotic disorders: Stratified analyses by psychotic subtypes, clinical setting and geographical region. Neurosci. Biobehav. Rev. 2022, 143, 104964. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Wu, M.; Zou, Y.; Wan, X.; Liu, Y.; Liu, X. Prevalence of suicide ideation, self-harm, and suicide among Chinese patients with schizophrenia: A systematic review and meta-analysis. Front. Public. Health 2023, 11, 1097098. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Dong, M.; Zhang, L.; Zhu, X.M.; Ungvari, G.S.; Ng, C.H.; Wang, G.; Xiang, Y.T. Prevalence of suicide attempts in individuals with schizophrenia: A meta-analysis of observational studies. Epidemiol. Psychiatr. Sci. 2019, 29, e39. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Wang, S.B.; Wang, F.; Zhang, L.; Ungvari, G.S.; Ng, C.H.; Meng, X.; Yuan, Z.; Wang, G.; Xiang, Y.T. Suicide-related behaviours in schizophrenia in China: A comprehensive meta-analysis. Epidemiol. Psychiatr. Sci. 2019, 28, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Liu, Z.H.; Jiang, Y.Y.; Zhang, Q.E.; Rao, W.W.; Cheung, T.; Hall, B.J.; Xiang, Y.T. Worldwide prevalence of suicidal ideation and suicide plan among people with schizophrenia: A meta-analysis and systematic review of epidemiological surveys. Transl. Psychiatry 2021, 11, 552. [Google Scholar] [CrossRef] [PubMed]
- Balhara, Y.P.; Verma, R. Schizophrenia and suicide. East. Asian Arch. Psychiatry 2012, 22, 126–133. [Google Scholar]
- Hubers, A.A.M.; Moaddine, S.; Peersmann, S.H.M.; Stijnen, T.; van Duijn, E.; van der Mast, R.C.; Dekkers, O.M.; Giltay, E.J. Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations: A meta-analysis. Epidemiol. Psychiatr. Sci. 2018, 27, 186–198. [Google Scholar] [CrossRef]
- Sher, L.; Kahn, R.S. Suicide in Schizophrenia: An Educational Overview. Medicina 2019, 55, 361. [Google Scholar] [CrossRef]
- Krysinska, K.; Heller, T.S.; De Leo, D. Suicide and deliberate self-harm in personality disorders. Curr. Opin. Psychiatry 2006, 19, 95–101. [Google Scholar] [CrossRef]
- Paris, J. Suicidality in Borderline Personality Disorder. Medicina 2019, 55, 223. [Google Scholar] [CrossRef]
- Reichl, C.; Kaess, M. Self-harm in the context of borderline personality disorder. Curr. Opin. Psychol. 2021, 37, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Soderholm, J.J.; Socada, J.L.; Rosenstrom, T.H.; Ekelund, J.; Isometsa, E. Borderline personality disorder and depression severity predict suicidal outcomes: A six-month prospective cohort study of depression, bipolar depression, and borderline personality disorder. Acta Psychiatr. Scand. 2023, 148, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Tadic, A.; Victor, A.; Baskaya, O.; von Cube, R.; Hoch, J.; Kouti, I.; Anicker, N.J.; Hoppner, W.; Lieb, K.; Dahmen, N. Interaction between gene variants of the serotonin transporter promoter region (5-HTTLPR) and catechol O-methyltransferase (COMT) in borderline personality disorder. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2009, 150B, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Zaboli, G.; Gizatullin, R.; Nilsonne, A.; Wilczek, A.; Jonsson, E.G.; Ahnemark, E.; Asberg, M.; Leopardi, R. Tryptophan hydroxylase-1 gene variants associate with a group of suicidal borderline women. Neuropsychopharmacology 2006, 31, 1982–1990. [Google Scholar] [CrossRef]
- Poorolajal, J.; Haghtalab, T.; Farhadi, M.; Darvishi, N. Substance use disorder and risk of suicidal ideation, suicide attempt and suicide death: A meta-analysis. J Public Health 2016, 38, e282–e291. [Google Scholar] [CrossRef]
- Isaacs, J.Y.; Smith, M.M.; Sherry, S.B.; Seno, M.; Moore, M.L.; Stewart, S.H. Alcohol use and death by suicide: A meta-analysis of 33 studies. Suicide Life Threat. Behav. 2022, 52, 600–614. [Google Scholar] [CrossRef]
- Rioux, C.; Huet, A.S.; Castellanos-Ryan, N.; Fortier, L.; Le Blanc, M.; Hamaoui, S.; Geoffroy, M.C.; Renaud, J.; Seguin, J.R. Substance use disorders and suicidality in youth: A systematic review and meta-analysis with a focus on the direction of the association. PLoS ONE 2021, 16, e0255799. [Google Scholar] [CrossRef]
- Roane, S.J.; Kapoor, S.; Sun, S.; Cramer, R.J.; Lamis, D.A. The interactive effect of the serotonin transporter genotype and drug use on suicidal behaviors in patients diagnosed with bipolar disorder. J. Affect. Disord. 2020, 262, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Zupanc, T.; Pregelj, P.; Tomori, M.; Komel, R.; Paska, A.V. No association between polymorphisms in four serotonin receptor genes, serotonin transporter gene and alcohol-related suicide. Psychiatr. Danub. 2010, 22, 522–527. [Google Scholar] [PubMed]
- Icick, R.; Bloch, V.; Prince, N.; Karsinti, E.; Lepine, J.P.; Laplanche, J.L.; Mouly, S.; Marie-Claire, C.; Brousse, G.; Bellivier, F.; et al. Clustering suicidal phenotypes and genetic associations with brain-derived neurotrophic factor in patients with substance use disorders. Transl. Psychiatry 2021, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, B.; Monroy-Jaramillo, N.; Fries, G.R.; Mendoza-Morales, R.C.; Garcia-Dolores, F.; Mendoza-Larios, A.; Diaz-Otanez, C.; Walss-Bass, C.; Glahn, D.C.; Ostrosky-Wegman, P.; et al. Brain Gene Expression Pattern of Subjects with Completed Suicide and Comorbid Substance Use Disorder. Mol. Neuropsychiatry 2019, 5, 60–73. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, I.; Austin, J.L.; Gooding, P. Childhood maltreatment and suicide attempts in prisoners: A systematic meta-analytic review. Psychol. Med. 2020, 50, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hussey, J.M.; Chang, J.J.; Kotch, J.B. Child maltreatment in the United States: Prevalence, risk factors, and adolescent health consequences. Pediatrics 2006, 118, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Esposito-Smythers, C.; Weismoore, J.T.; Renshaw, K.D. The relation between child maltreatment and adolescent suicidal behavior: A systematic review and critical examination of the literature. Clin. Child. Fam. Psychol. Rev. 2013, 16, 146–172. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, I.; Gillespie, E.L.; Panagioti, M. Childhood maltreatment and adult suicidality: A comprehensive systematic review with meta-analysis. Psychol. Med. 2019, 49, 1057–1078. [Google Scholar] [CrossRef]
- Hoertel, N.; Franco, S.; Wall, M.M.; Oquendo, M.A.; Wang, S.; Limosin, F.; Blanco, C. Childhood maltreatment and risk of suicide attempt: A nationally representative study. J. Clin. Psychiatry 2015, 76, 916–923, quiz 923. [Google Scholar] [CrossRef]
- Anderson, P.L.; Tiro, J.A.; Price, A.W.; Bender, M.A.; Kaslow, N.J. Additive impact of childhood emotional, physical, and sexual abuse on suicide attempts among low-income African American women. Suicide Life Threat. Behav. 2002, 32, 131–138. [Google Scholar] [CrossRef]
- Miller, A.B.; Jenness, J.L.; Oppenheimer, C.W.; Gottleib, A.L.; Young, J.F.; Hankin, B.L. Childhood Emotional Maltreatment as a Robust Predictor of Suicidal Ideation: A 3-Year Multi-Wave, Prospective Investigation. J. Abnorm. Child. Psychol. 2017, 45, 105–116. [Google Scholar] [CrossRef]
- Castellvi, P.; Miranda-Mendizabal, A.; Pares-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebria, A.; Gabilondo, A.; Gili, M.; Lagares, C.; et al. Exposure to violence, a risk for suicide in youths and young adults. A meta-analysis of longitudinal studies. Acta Psychiatr. Scand. 2017, 135, 195–211. [Google Scholar] [CrossRef]
- Zatti, C.; Rosa, V.; Barros, A.; Valdivia, L.; Calegaro, V.C.; Freitas, L.H.; Cereser, K.M.M.; Rocha, N.S.D.; Bastos, A.G.; Schuch, F.B. Childhood trauma and suicide attempt: A meta-analysis of longitudinal studies from the last decade. Psychiatry Res. 2017, 256, 353–358. [Google Scholar] [CrossRef]
- Liu, J.; Fang, Y.; Gong, J.; Cui, X.; Meng, T.; Xiao, B.; He, Y.; Shen, Y.; Luo, X. Associations between suicidal behavior and childhood abuse and neglect: A meta-analysis. J. Affect. Disord. 2017, 220, 147–155. [Google Scholar] [CrossRef]
- Ng, Q.X.; Yong, B.Z.J.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W.S. Early life sexual abuse is associated with increased suicide attempts: An update meta-analysis. J. Psychiatr. Res. 2018, 99, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, I.; Austin, J.L.; Gooding, P. Association of Childhood Maltreatment With Suicide Behaviors Among Young People: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2012563. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Murat Baldwin, M.; Wong, S.C.; Obsuth, I.; Meinck, F.; Murray, A.L. The Impact of Childhood Psychological Maltreatment on Mental Health Outcomes in Adulthood: A Systematic Review and Meta-Analysis. Trauma. Violence Abuse 2023, 24, 3049–3064. [Google Scholar] [CrossRef]
- Rhodes, A.E.; Boyle, M.H.; Tonmyr, L.; Wekerle, C.; Goodman, D.; Leslie, B.; Mironova, P.; Bethell, J.; Manion, I. Sex differences in childhood sexual abuse and suicide-related behaviors. Suicide Life Threat. Behav. 2011, 41, 235–254. [Google Scholar] [CrossRef] [PubMed]
- Koola, M.M.; Ahmed, A.O.; Sebastian, J.; Duncan, E.J. Childhood Physical and Sexual Abuse Predicts Suicide Risk in a Large Cohort of Veterans. Prim. Care Companion CNS Disord. 2018, 20, 18m02317. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gonzalez, A.; Pereda, N. Systematic review of the prevalence of suicidal ideation and behavior in minors who have been sexually abused. Actas Esp. Psiquiatr. 2015, 43, 149–158. [Google Scholar]
- Perez-Balaguer, A.; Penuelas-Calvo, I.; Alacreu-Crespo, A.; Baca-Garcia, E.; Porras-Segovia, A. Impulsivity as a mediator between childhood maltreatment and suicidal behavior: A systematic review and meta-analysis. J. Psychiatr. Res. 2022, 151, 95–107. [Google Scholar] [CrossRef]
- Li, J.; Jin, Y.; Xu, S.; Luo, X.; Wilson, A.; Li, H.; Wang, X.; Sun, X.; Wang, Y. Anxiety and Depression Symptoms among Youth Survivors of Childhood Sexual Abuse: A Network Analysis. BMC Psychol. 2023, 11, 278. [Google Scholar] [CrossRef]
- Lippard, E.T.C.; Nemeroff, C.B. The Devastating Clinical Consequences of Child Abuse and Neglect: Increased Disease Vulnerability and Poor Treatment Response in Mood Disorders. Am. J. Psychiatry 2023, 180, 548–564. [Google Scholar] [CrossRef]
- Heim, C.; Newport, D.J.; Bonsall, R.; Miller, A.H.; Nemeroff, C.B. Altered pituitary-adrenal axis responses to provocative challenge tests in adult survivors of childhood abuse. Am. J. Psychiatry 2001, 158, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Melhem, N.M.; Keilp, J.G.; Porta, G.; Oquendo, M.A.; Burke, A.; Stanley, B.; Cooper, T.B.; Mann, J.J.; Brent, D.A. Blunted HPA Axis Activity in Suicide Attempters Compared to those at High Risk for Suicidal Behavior. Neuropsychopharmacology 2016, 41, 1447–1456. [Google Scholar] [CrossRef]
- Van Harmelen, A.L.; van Tol, M.J.; van der Wee, N.J.; Veltman, D.J.; Aleman, A.; Spinhoven, P.; van Buchem, M.A.; Zitman, F.G.; Penninx, B.W.; Elzinga, B.M. Reduced medial prefrontal cortex volume in adults reporting childhood emotional maltreatment. Biol. Psychiatry 2010, 68, 832–838. [Google Scholar] [CrossRef]
- Gonzalez-Castro, T.B.; Juarez-Rojop, I.E.; Tovilla-Zarate, C.A.; Ovando-Ricardez, J.A.; Hernandez-Diaz, Y.; Lopez-Narvaez, M.L.; Genis-Mendoza, A.D.; Rodriguez-Perez, C. Gene-environment interaction between HPA-axis genes and trauma exposure in the suicide behavior: A systematic review. J. Psychiatr. Res. 2023, 164, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Berardelli, I.; Serafini, G.; Cortese, N.; Fiasche, F.; O’Connor, R.C.; Pompili, M. The Involvement of Hypothalamus-Pituitary-Adrenal (HPA) Axis in Suicide Risk. Brain Sci. 2020, 10, 653. [Google Scholar] [CrossRef] [PubMed]
- Beauchaine, T.P.; Crowell, S.E.; Hsiao, R.C. Post-dexamethasone cortisol, self-inflicted injury, and suicidal ideation among depressed adolescent girls. J. Abnorm. Child. Psychol. 2015, 43, 619–632. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Green, J.A.; Ferguson, E.; O’Carroll, R.E.; O’Connor, R.C. Effects of childhood trauma on cortisol levels in suicide attempters and ideators. Psychoneuroendocrinology 2018, 88, 9–16. [Google Scholar] [CrossRef]
- Gartland, N.; Rosmalen, J.G.M.; O’Connor, D.B. Effects of childhood adversity and cortisol levels on suicidal ideation and behaviour: Results from a general population study. Psychoneuroendocrinology 2022, 138, 105664. [Google Scholar] [CrossRef]
- Brand, S.R.; Brennan, P.A.; Newport, D.J.; Smith, A.K.; Weiss, T.; Stowe, Z.N. The impact of maternal childhood abuse on maternal and infant HPA axis function in the postpartum period. Psychoneuroendocrinology 2010, 35, 686–693. [Google Scholar] [CrossRef]
- Underwood, M.D.; Galfalvy, H.; Hsiung, S.C.; Liu, Y.; Simpson, N.R.; Bakalian, M.J.; Rosoklija, G.B.; Dwork, A.J.; Arango, V.; Mann, J.J. A Stress Protein-Based Suicide Prediction Score and Relationship to Reported Early-Life Adversity and Recent Life Stress. Int. J. Neuropsychopharmacol. 2023, 26, 501–512. [Google Scholar] [CrossRef]
- Merali, Z.; Du, L.; Hrdina, P.; Palkovits, M.; Faludi, G.; Poulter, M.O.; Anisman, H. Dysregulation in the suicide brain: mRNA expression of corticotropin-releasing hormone receptors and GABA(A) receptor subunits in frontal cortical brain region. J. Neurosci. 2004, 24, 1478–1485. [Google Scholar] [CrossRef]
- Zhao, J.; Qi, X.R.; Gao, S.F.; Lu, J.; van Wamelen, D.J.; Kamphuis, W.; Bao, A.M.; Swaab, D.F. Different stress-related gene expression in depression and suicide. J. Psychiatr. Res. 2015, 68, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ortiz, J.M.; Garcia-Gutierrez, M.S.; Navarrete, F.; Giner, S.; Manzanares, J. Gene and protein alterations of FKBP5 and glucocorticoid receptor in the amygdala of suicide victims. Psychoneuroendocrinology 2013, 38, 1251–1258. [Google Scholar] [CrossRef]
- Yin, H.; Galfalvy, H.; Pantazatos, S.P.; Huang, Y.Y.; Rosoklija, G.B.; Dwork, A.J.; Burke, A.; Arango, V.; Oquendo, M.A.; Mann, J.J. Glucocorticoid Receptor-Related Genes: Genotype and Brain Gene Expression Relationships to Suicide and Major Depressive Disorder. Depress. Anxiety 2016, 33, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.A.; Lin, J.Y.; Liu, Q.; Lv, X.Z.; Wang, G.; Wei, J.; Zhu, G.; Chen, Q.L.; Tian, H.J.; Zhang, K.R.; et al. Associations among serum markers of inflammation, life stress and suicide risk in patients with major depressive disorder. J. Psychiatr. Res. 2020, 129, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.E.; Heron, J.; Gunnell, D.; Ford, T.; Hemani, G.; Joinson, C.; Moran, P.; Relton, C.; Suderman, M.; Mars, B. Pathways between early-life adversity and adolescent self-harm: The mediating role of inflammation in the Avon Longitudinal Study of Parents and Children. J. Child. Psychol. Psychiatry 2019, 60, 1094–1103. [Google Scholar] [CrossRef]
- Maes, M.; Congio, A.; Moraes, J.B.; Bonifacio, K.L.; Barbosa, D.S.; Vargas, H.O.; Morris, G.; Puri, B.K.; Michelin, A.P.; Nunes, S.O.V. Early Life Trauma Predicts Affective Phenomenology and the Effects are Partly Mediated by Staging Coupled with Lowered Lipid-Associated Antioxidant Defences. Biomol. Concepts 2018, 9, 115–130. [Google Scholar] [CrossRef]
- Pandey, G.N.; Rizavi, H.S.; Ren, X.; Fareed, J.; Hoppensteadt, D.A.; Roberts, R.C.; Conley, R.R.; Dwivedi, Y. Proinflammatory cytokines in the prefrontal cortex of teenage suicide victims. J. Psychiatr. Res. 2012, 46, 57–63. [Google Scholar] [CrossRef]
- Shinko, Y.; Otsuka, I.; Okazaki, S.; Horai, T.; Boku, S.; Takahashi, M.; Ueno, Y.; Sora, I.; Hishimoto, A. Chemokine alterations in the postmortem brains of suicide completers. J. Psychiatr. Res. 2020, 120, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, L.H.; Stiller, J.; Rujescu, D.; Giegling, I.; Schneider, B.; Maurer, K.; Schnabel, A.; Moller, H.J.; Chen, H.H.; Postolache, T.T. Elevated cytokine expression in the orbitofrontal cortex of victims of suicide. Acta Psychiatr. Scand. 2008, 117, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Isung, J.; Mobarrez, F.; Nordstrom, P.; Asberg, M.; Jokinen, J. Low plasma vascular endothelial growth factor (VEGF) associated with completed suicide. World J. Biol. Psychiatry 2012, 13, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Janelidze, S.; Mattei, D.; Westrin, A.; Traskman-Bendz, L.; Brundin, L. Cytokine levels in the blood may distinguish suicide attempters from depressed patients. Brain Behav. Immun. 2011, 25, 335–339. [Google Scholar] [CrossRef]
- Isung, J.; Aeinehband, S.; Mobarrez, F.; Martensson, B.; Nordstrom, P.; Asberg, M.; Piehl, F.; Jokinen, J. Low vascular endothelial growth factor and interleukin-8 in cerebrospinal fluid of suicide attempters. Transl. Psychiatry 2012, 2, e196. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Janelidze, S.; Hagell, P.; Erhardt, S.; Samuelsson, M.; Minthon, L.; Hansson, O.; Bjorkqvist, M.; Traskman-Bendz, L.; Brundin, L. Interleukin-6 is elevated in the cerebrospinal fluid of suicide attempters and related to symptom severity. Biol. Psychiatry 2009, 66, 287–292. [Google Scholar] [CrossRef]
- Brown, S.J.; Christofides, K.; Weissleder, C.; Huang, X.F.; Shannon Weickert, C.; Lim, C.K.; Newell, K.A. Sex- and suicide-specific alterations in the kynurenine pathway in the anterior cingulate cortex in major depression. Neuropsychopharmacology 2023. [Google Scholar] [CrossRef]
- Purba, J.S.; Hoogendijk, W.J.; Hofman, M.A.; Swaab, D.F. Increased number of vasopressin- and oxytocin-expressing neurons in the paraventricular nucleus of the hypothalamus in depression. Arch. Gen. Psychiatry 1996, 53, 137–143. [Google Scholar] [CrossRef]
- Van Londen, L.; Goekoop, J.G.; van Kempen, G.M.; Frankhuijzen-Sierevogel, A.C.; Wiegant, V.M.; van der Velde, E.A.; De Wied, D. Plasma levels of arginine vasopressin elevated in patients with major depression. Neuropsychopharmacology 1997, 17, 284–292. [Google Scholar] [CrossRef]
- Inder, W.J.; Donald, R.A.; Prickett, T.C.; Frampton, C.M.; Sullivan, P.F.; Mulder, R.T.; Joyce, P.R. Arginine vasopressin is associated with hypercortisolemia and suicide attempts in depression. Biol. Psychiatry 1997, 42, 744–747. [Google Scholar] [CrossRef]
- Aguilera, G.; Rabadan-Diehl, C. Vasopressinergic regulation of the hypothalamic-pituitary-adrenal axis: Implications for stress adaptation. Regul. Pept. 2000, 96, 23–29. [Google Scholar] [CrossRef]
- Brunner, J.; Keck, M.E.; Landgraf, R.; Uhr, M.; Namendorf, C.; Bronisch, T. Vasopressin in CSF and plasma in depressed suicide attempters: Preliminary results. Eur. Neuropsychopharmacol. 2002, 12, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Pitchot, W.; Scantamburlo, G.; Pinto, E.; Hansenne, M.; Reggers, J.; Ansseau, M.; Legros, J.J. Vasopressin-neurophysin and DST in major depression: Relationship with suicidal behavior. J. Psychiatr. Res. 2008, 42, 684–688. [Google Scholar] [CrossRef]
- Jahangard, L.; Shayganfard, M.; Ghiasi, F.; Salehi, I.; Haghighi, M.; Ahmadpanah, M.; Sadeghi Bahmani, D.; Brand, S. Serum oxytocin concentrations in current and recent suicide survivors are lower than in healthy controls. J. Psychiatr. Res. 2020, 128, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.; Hammock, E.A.D.; Joiner, T.E. Unextracted plasma oxytocin levels decrease following in-laboratory social exclusion in young adults with a suicide attempt history. J. Psychiatr. Res. 2020, 121, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Jokinen, J.; Chatzittofis, A.; Hellstrom, C.; Nordstrom, P.; Uvnas-Moberg, K.; Asberg, M. Low CSF oxytocin reflects high intent in suicide attempters. Psychoneuroendocrinology 2012, 37, 482–490. [Google Scholar] [CrossRef]
- Widdowson, P.S.; Ordway, G.A.; Halaris, A.E. Reduced neuropeptide Y concentrations in suicide brain. J. Neurochem. 1992, 59, 73–80. [Google Scholar] [CrossRef]
- Caberlotto, L.; Hurd, Y.L. Reduced neuropeptide Y mRNA expression in the prefrontal cortex of subjects with bipolar disorder. Neuroreport 1999, 10, 1747–1750. [Google Scholar] [CrossRef]
- Sharma, A.; Ren, X.; Zhang, H.; Pandey, G.N. Effect of depression and suicidal behavior on neuropeptide Y (NPY) and its receptors in the adult human brain: A postmortem study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 112, 110428. [Google Scholar] [CrossRef]
- Jones, B.J.; Blackburn, T.P. The medical benefit of 5-HT research. Pharmacol. Biochem. Behav. 2002, 71, 555–568. [Google Scholar] [CrossRef]
- Hensler, J.G. Serotonergic modulation of the limbic system. Neurosci. Biobehav. Rev. 2006, 30, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Arango, V.; Underwood, M.D.; Boldrini, M.; Tamir, H.; Kassir, S.A.; Hsiung, S.; Chen, J.J.; Mann, J.J. Serotonin 1A receptors, serotonin transporter binding and serotonin transporter mRNA expression in the brainstem of depressed suicide victims. Neuropsychopharmacology 2001, 25, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Arango, V.; Underwood, M.D.; Gubbi, A.V.; Mann, J.J. Localized alterations in pre- and postsynaptic serotonin binding sites in the ventrolateral prefrontal cortex of suicide victims. Brain Res. 1995, 688, 121–133. [Google Scholar] [CrossRef]
- Nielsen, D.A.; Virkkunen, M.; Lappalainen, J.; Eggert, M.; Brown, G.L.; Long, J.C.; Goldman, D.; Linnoila, M. A tryptophan hydroxylase gene marker for suicidality and alcoholism. Arch. Gen. Psychiatry 1998, 55, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G. Suicidal behavior: Is there a genetic predisposition? Bipolar Disord. 2001, 3, 335–349. [Google Scholar] [CrossRef]
- Stefulj, J.; Kubat, M.; Balija, M.; Skavic, J.; Jernej, B. Variability of the tryptophan hydroxylase gene: Study in victims of violent suicide. Psychiatry Res. 2005, 134, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Ohtani, M.; Shindo, S.; Yoshioka, N. Polymorphisms of the tryptophan hydroxylase gene and serotonin 1A receptor gene in suicide victims among Japanese. Tohoku J. Exp. Med. 2004, 202, 123–133. [Google Scholar] [CrossRef]
- Perroud, N.; Neidhart, E.; Petit, B.; Vessaz, M.; Laforge, T.; Relecom, C.; La Harpe, R.; Malafosse, A.; Guipponi, M. Simultaneous analysis of serotonin transporter, tryptophan hydroxylase 1 and 2 gene expression in the ventral prefrontal cortex of suicide victims. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2010, 153B, 909–918. [Google Scholar] [CrossRef]
- Du, L.; Faludi, G.; Palkovits, M.; Demeter, E.; Bakish, D.; Lapierre, Y.D.; Sotonyi, P.; Hrdina, P.D. Frequency of long allele in serotonin transporter gene is increased in depressed suicide victims. Biol. Psychiatry 1999, 46, 196–201. [Google Scholar] [CrossRef]
- Hranilovic, D.; Stefulj, J.; Furac, I.; Kubat, M.; Balija, M.; Jernej, B. Serotonin transporter gene promoter (5-HTTLPR) and intron 2 (VNTR) polymorphisms in Croatian suicide victims. Biol. Psychiatry 2003, 54, 884–889. [Google Scholar] [CrossRef]
- Zhang, J.; Shen, Y.; He, G.; Li, X.; Meng, J.; Guo, S.; Li, H.; Gu, N.; Feng, G.; He, L. Lack of association between three serotonin genes and suicidal behavior in Chinese psychiatric patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J. The serotonergic system in mood disorders and suicidal behaviour. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120537. [Google Scholar] [CrossRef]
- Marco, E.M.; Garcia-Gutierrez, M.S.; Bermudez-Silva, F.J.; Moreira, F.A.; Guimaraes, F.; Manzanares, J.; Viveros, M.P. Endocannabinoid system and psychiatry: In search of a neurobiological basis for detrimental and potential therapeutic effects. Front. Behav. Neurosci. 2011, 5, 63. [Google Scholar] [CrossRef]
- Marsicano, G.; Wotjak, C.T.; Azad, S.C.; Bisogno, T.; Rammes, G.; Cascio, M.G.; Hermann, H.; Tang, J.; Hofmann, C.; Zieglgansberger, W.; et al. The endogenous cannabinoid system controls extinction of aversive memories. Nature 2002, 418, 530–534. [Google Scholar] [CrossRef]
- Steiner, M.A.; Wanisch, K.; Monory, K.; Marsicano, G.; Borroni, E.; Bachli, H.; Holsboer, F.; Lutz, B.; Wotjak, C.T. Impaired cannabinoid receptor type 1 signaling interferes with stress-coping behavior in mice. Pharmacogenomics J. 2008, 8, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Uriguen, L.; Perez-Rial, S.; Ledent, C.; Palomo, T.; Manzanares, J. Impaired action of anxiolytic drugs in mice deficient in cannabinoid CB1 receptors. Neuropharmacology 2004, 46, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Cota, D.; Steiner, M.A.; Marsicano, G.; Cervino, C.; Herman, J.P.; Grubler, Y.; Stalla, J.; Pasquali, R.; Lutz, B.; Stalla, G.K.; et al. Requirement of cannabinoid receptor type 1 for the basal modulation of hypothalamic-pituitary-adrenal axis function. Endocrinology 2007, 148, 1574–1581. [Google Scholar] [CrossRef]
- Zarruk, J.G.; Fernandez-Lopez, D.; Garcia-Yebenes, I.; Garcia-Gutierrez, M.S.; Vivancos, J.; Nombela, F.; Torres, M.; Burguete, M.C.; Manzanares, J.; Lizasoain, I.; et al. Cannabinoid type 2 receptor activation downregulates stroke-induced classic and alternative brain macrophage/microglial activation concomitant to neuroprotection. Stroke 2012, 43, 211–219. [Google Scholar] [CrossRef]
- Aso, E.; Ozaita, A.; Valdizan, E.M.; Ledent, C.; Pazos, A.; Maldonado, R.; Valverde, O. BDNF impairment in the hippocampus is related to enhanced despair behavior in CB1 knockout mice. J. Neurochem. 2008, 105, 565–572. [Google Scholar] [CrossRef]
- Shearman, L.P.; Rosko, K.M.; Fleischer, R.; Wang, J.; Xu, S.; Tong, X.S.; Rocha, B.A. Antidepressant-like and anorectic effects of the cannabinoid CB1 receptor inverse agonist AM251 in mice. Behav. Pharmacol. 2003, 14, 573–582. [Google Scholar] [CrossRef]
- Tzavara, E.T.; Davis, R.J.; Perry, K.W.; Li, X.; Salhoff, C.; Bymaster, F.P.; Witkin, J.M.; Nomikos, G.G. The CB1 receptor antagonist SR141716A selectively increases monoaminergic neurotransmission in the medial prefrontal cortex: Implications for therapeutic actions. Br. J. Pharmacol. 2003, 138, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Witkin, J.M.; Tzavara, E.T.; Davis, R.J.; Li, X.; Nomikos, G.G. A therapeutic role for cannabinoid CB1 receptor antagonists in major depressive disorders. Trends Pharmacol. Sci. 2005, 26, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, P.; Bifulco, M.; Maina, G.; Tortorella, A.; Gazzerro, P.; Proto, M.C.; Di Filippo, C.; Monteleone, F.; Canestrelli, B.; Buonerba, G.; et al. Investigation of CNR1 and FAAH endocannabinoid gene polymorphisms in bipolar disorder and major depression. Pharmacol. Res. 2010, 61, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Mitjans, M.; Serretti, A.; Fabbri, C.; Gasto, C.; Catalan, R.; Fananas, L.; Arias, B. Screening genetic variability at the CNR1 gene in both major depression etiology and clinical response to citalopram treatment. Psychopharmacology 2013, 227, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.S.; Kim, J.Y.; Park, B.L.; Kim, J.H.; Kim, B.; Park, C.S.; Kim, B.J.; Lee, C.S.; Lee, M.; Choi, W.H.; et al. Genetic association analysis of CNR1 and CNR2 polymorphisms with schizophrenia in a Korean population. Psychiatr. Genet. 2014, 24, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Gutierrez, M.S.; Perez-Ortiz, J.M.; Gutierrez-Adan, A.; Manzanares, J. Depression-resistant endophenotype in mice overexpressing cannabinoid CB(2) receptors. Br. J. Pharmacol. 2010, 160, 1773–1784. [Google Scholar] [CrossRef]
- Garcia-Gutierrez, M.S.; Manzanares, J. Overexpression of CB2 cannabinoid receptors decreased vulnerability to anxiety and impaired anxiolytic action of alprazolam in mice. J. Psychopharmacol. 2011, 25, 111–120. [Google Scholar] [CrossRef]
- Garcia-Gutierrez, M.S.; Garcia-Bueno, B.; Zoppi, S.; Leza, J.C.; Manzanares, J. Chronic blockade of cannabinoid CB2 receptors induces anxiolytic-like actions associated with alterations in GABA(A) receptors. Br. J. Pharmacol. 2012, 165, 951–964. [Google Scholar] [CrossRef]
- Ryberg, E.; Larsson, N.; Sjogren, S.; Hjorth, S.; Hermansson, N.O.; Leonova, J.; Elebring, T.; Nilsson, K.; Drmota, T.; Greasley, P.J. The orphan receptor GPR55 is a novel cannabinoid receptor. Br. J. Pharmacol. 2007, 152, 1092–1101. [Google Scholar] [CrossRef]
- Marco, E.M.; Echeverry-Alzate, V.; Lopez-Moreno, J.A.; Gine, E.; Penasco, S.; Viveros, M.P. Consequences of early life stress on the expression of endocannabinoid-related genes in the rat brain. Behav. Pharmacol. 2014, 25, 547–556. [Google Scholar] [CrossRef]
- Garcia-Gutierrez, M.S.; Navarrete, F.; Navarro, G.; Reyes-Resina, I.; Franco, R.; Lanciego, J.L.; Giner, S.; Manzanares, J. Alterations in Gene and Protein Expression of Cannabinoid CB(2) and GPR55 Receptors in the Dorsolateral Prefrontal Cortex of Suicide Victims. Neurotherapeutics 2018, 15, 796–806. [Google Scholar] [CrossRef]
- Vinod, K.Y.; Arango, V.; Xie, S.; Kassir, S.A.; Mann, J.J.; Cooper, T.B.; Hungund, B.L. Elevated levels of endocannabinoids and CB1 receptor-mediated G-protein signaling in the prefrontal cortex of alcoholic suicide victims. Biol. Psychiatry 2005, 57, 480–486. [Google Scholar] [CrossRef]
- Vinod, K.Y.; Kassir, S.A.; Hungund, B.L.; Cooper, T.B.; Mann, J.J.; Arango, V. Selective alterations of the CB1 receptors and the fatty acid amide hydrolase in the ventral striatum of alcoholics and suicides. J. Psychiatr. Res. 2010, 44, 591–597. [Google Scholar] [CrossRef]
- Hungund, B.L.; Vinod, K.Y.; Kassir, S.A.; Basavarajappa, B.S.; Yalamanchili, R.; Cooper, T.B.; Mann, J.J.; Arango, V. Upregulation of CB1 receptors and agonist-stimulated [35S]GTPgammaS binding in the prefrontal cortex of depressed suicide victims. Mol. Psychiatry 2004, 9, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Herranz-Herrer, J.; Gil-Benito, E.; Ponte-Lopez, T.; Ortega-Gutierrez, S.; Macicior, J.; Rosado-Garcia, S.; Sanchez-Lopez, A.J.; Blasco-Fontecilla, H. Serum endocannabinoid levels in suicide attempters: A pilot study. Eur. Neuropsychopharmacol. 2020, 40, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Vinod, K.Y.; Hungund, B.L. Role of the endocannabinoid system in depression and suicide. Trends Pharmacol. Sci. 2006, 27, 539–545. [Google Scholar] [CrossRef]
- Pinna, G. Endocannabinoids and Precision Medicine for Mood Disorders and Suicide. Front. Psychiatry 2021, 12, 658433. [Google Scholar] [CrossRef] [PubMed]
- Choudary, P.V.; Molnar, M.; Evans, S.J.; Tomita, H.; Li, J.Z.; Vawter, M.P.; Myers, R.M.; Bunney, W.E., Jr.; Akil, H.; Watson, S.J.; et al. Altered cortical glutamatergic and GABAergic signal transmission with glial involvement in depression. Proc. Natl. Acad. Sci. USA 2005, 102, 15653–15658. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Gutierrez, M.S.; Navarro, D.; Torregrosa, A.B.; Viudez-Martinez, A.; Giner, S.; Manzanares, J. Alterations of BDNF, mGluR5, Homer1a, p11 and excitatory/inhibitory balance in corticolimbic brain regions of suicide decedents. J. Affect. Disord. 2023, 339, 366–376. [Google Scholar] [CrossRef]
- Sequeira, A.; Mamdani, F.; Ernst, C.; Vawter, M.P.; Bunney, W.E.; Lebel, V.; Rehal, S.; Klempan, T.; Gratton, A.; Benkelfat, C.; et al. Global brain gene expression analysis links glutamatergic and GABAergic alterations to suicide and major depression. PLoS ONE 2009, 4, e6585. [Google Scholar] [CrossRef]
- Zhao, J.; Bao, A.M.; Qi, X.R.; Kamphuis, W.; Luchetti, S.; Lou, J.S.; Swaab, D.F. Gene expression of GABA and glutamate pathway markers in the prefrontal cortex of non-suicidal elderly depressed patients. J. Affect. Disord. 2012, 138, 494–502. [Google Scholar] [CrossRef]
- Yin, H.; Pantazatos, S.P.; Galfalvy, H.; Huang, Y.Y.; Rosoklija, G.B.; Dwork, A.J.; Burke, A.; Arango, V.; Oquendo, M.A.; Mann, J.J. A pilot integrative genomics study of GABA and glutamate neurotransmitter systems in suicide, suicidal behavior, and major depressive disorder. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2016, 171B, 414–426. [Google Scholar] [CrossRef]
- Zhao, J.; Verwer, R.W.H.; Gao, S.F.; Qi, X.R.; Lucassen, P.J.; Kessels, H.W.; Swaab, D.F. Prefrontal alterations in GABAergic and glutamatergic gene expression in relation to depression and suicide. J. Psychiatr. Res. 2018, 102, 261–274. [Google Scholar] [CrossRef]
- Moore, L.D.; Le, T.; Fan, G. DNA methylation and its basic function. Neuropsychopharmacology 2013, 38, 23–38. [Google Scholar] [CrossRef]
- Smart, C.; Strathdee, G.; Watson, S.; Murgatroyd, C.; McAllister-Williams, R.H. Early life trauma, depression and the glucocorticoid receptor gene--an epigenetic perspective. Psychol. Med. 2015, 45, 3393–3410. [Google Scholar] [CrossRef] [PubMed]
- Kadmiel, M.; Cidlowski, J.A. Glucocorticoid receptor signaling in health and disease. Trends Pharmacol. Sci. 2013, 34, 518–530. [Google Scholar] [CrossRef]
- Petta, I.; Dejager, L.; Ballegeer, M.; Lievens, S.; Tavernier, J.; De Bosscher, K.; Libert, C. The Interactome of the Glucocorticoid Receptor and Its Influence on the Actions of Glucocorticoids in Combatting Inflammatory and Infectious Diseases. Microbiol. Mol. Biol. Rev. 2016, 80, 495–522. [Google Scholar] [CrossRef]
- Weaver, I.C.; Cervoni, N.; Champagne, F.A.; D’Alessio, A.C.; Sharma, S.; Seckl, J.R.; Dymov, S.; Szyf, M.; Meaney, M.J. Epigenetic programming by maternal behavior. Nat. Neurosci. 2004, 7, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Steiger, H.; Labonte, B.; Groleau, P.; Turecki, G.; Israel, M. Methylation of the glucocorticoid receptor gene promoter in bulimic women: Associations with borderline personality disorder, suicidality, and exposure to childhood abuse. Int. J. Eat. Disord. 2013, 46, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Roy, B.; Shelton, R.C.; Dwivedi, Y. DNA methylation and expression of stress related genes in PBMC of MDD patients with and without serious suicidal ideation. J. Psychiatr. Res. 2017, 89, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Jokinen, J.; Bostrom, A.E.; Dadfar, A.; Ciuculete, D.M.; Chatzittofis, A.; Asberg, M.; Schioth, H.B. Epigenetic Changes in the CRH Gene are Related to Severity of Suicide Attempt and a General Psychiatric Risk Score in Adolescents. EBioMedicine 2018, 27, 123–133. [Google Scholar] [CrossRef]
- Rice, L.; Waters, C.E.; Eccles, J.; Garside, H.; Sommer, P.; Kay, P.; Blackhall, F.H.; Zeef, L.; Telfer, B.; Stratford, I.; et al. Identification and functional analysis of SKA2 interaction with the glucocorticoid receptor. J. Endocrinol. 2008, 198, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Bu, Y. SKA2/FAM33A: A novel gene implicated in cell cycle, tumorigenesis, and psychiatric disorders. Genes Dis. 2019, 6, 25–30. [Google Scholar] [CrossRef]
- Kouter, K.; Zupanc, T.; Videtic Paska, A. Targeted sequencing approach: Comprehensive analysis of DNA methylation and gene expression across blood and brain regions in suicide victims. World J. Biol. Psychiatry 2023, 24, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kang, H.J.; Bae, K.Y.; Kim, S.W.; Shin, I.S.; Kim, H.R.; Shin, M.G.; Yoon, J.S. Association of BDNF promoter methylation and genotype with suicidal ideation in elderly Koreans. Am. J. Geriatr. Psychiatry 2014, 22, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.J.; Kim, J.M.; Lee, J.Y.; Kim, S.Y.; Bae, K.Y.; Kim, S.W.; Shin, I.S.; Kim, H.R.; Shin, M.G.; Yoon, J.S. BDNF promoter methylation and suicidal behavior in depressive patients. J. Affect. Disord. 2013, 151, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, E.; Bostrom, A.E.D.; Wilczek, A.; Nilsonne, A.; Asberg, M.; Jokinen, J. Increased Methylation of Brain-Derived Neurotrophic Factor (BDNF) Is Related to Emotionally Unstable Personality Disorder and Severity of Suicide Attempt in Women. Cells 2023, 12, 350. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kang, H.J.; Kim, S.Y.; Kim, S.W.; Shin, I.S.; Kim, H.R.; Park, M.H.; Shin, M.G.; Yoon, J.H.; Yoon, J.S. BDNF promoter methylation associated with suicidal ideation in patients with breast cancer. Int. J. Psychiatry Med. 2015, 49, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Ropret, S.; Kouter, K.; Zupanc, T.; Videtic Paska, A. BDNF methylation and mRNA expression in brain and blood of completed suicides in Slovenia. World J. Psychiatry 2021, 11, 1301–1313. [Google Scholar] [CrossRef]
- Ludwig, B.; Carlberg, L.; Kienesberger, K.; Swoboda, P.; Mitschek, M.M.M.; Bernegger, A.; Koller, R.; Inaner, M.; Senft, B.; Meisner, L.; et al. Monoamino Oxidase A Gene Single-Nucleotide Polymorphisms and Methylation Status and the Risk of Violent Suicide Attempts in Affective Disorder Patients. Front. Psychiatry 2021, 12, 667191. [Google Scholar] [CrossRef]
- Kang, H.J.; Lee, E.H.; Kim, J.W.; Kim, S.W.; Shin, I.S.; Kim, J.T.; Park, M.S.; Cho, K.H.; Han, J.S.; Lyoo, I.K.; et al. Association of SLC6A4 methylation with long-term outcomes after stroke: Focus on the interaction with suicidal ideation. Sci. Rep. 2021, 11, 2710. [Google Scholar] [CrossRef]
- Walther, D.J.; Peter, J.U.; Bashammakh, S.; Hortnagl, H.; Voits, M.; Fink, H.; Bader, M. Synthesis of serotonin by a second tryptophan hydroxylase isoform. Science 2003, 299, 76. [Google Scholar] [CrossRef]
- Zhang, Y.; Chang, Z.; Chen, J.; Ling, Y.; Liu, X.; Feng, Z.; Chen, C.; Xia, M.; Zhao, X.; Ying, W.; et al. Methylation of the tryptophan hydroxylase-2 gene is associated with mRNA expression in patients with major depression with suicide attempts. Mol. Med. Rep. 2015, 12, 3184–3190. [Google Scholar] [CrossRef]
- Kimbrel, N.A.; Garrett, M.E.; Evans, M.K.; Mellows, C.; Dennis, M.F.; Hair, L.P.; Hauser, M.A.; Workgroup, V.A.M.-A.M.; Ashley-Koch, A.E.; Beckham, J.C. Large epigenome-wide association study identifies multiple novel differentially methylated CpG sites associated with suicidal thoughts and behaviors in veterans. Front. Psychiatry 2023, 14, 1145375. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Lahiri, D.K. Cdk5 activity in the brain—Multiple paths of regulation. J. Cell Sci. 2014, 127, 2391–2400. [Google Scholar] [CrossRef]
- Choi, K.; Le, T.; Xing, G.; Johnson, L.R.; Ursano, R.J. Analysis of kinase gene expression in the frontal cortex of suicide victims: Implications of fear and stress. Front. Behav. Neurosci. 2011, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Jeremian, R.; Chen, Y.A.; De Luca, V.; Vincent, J.B.; Kennedy, J.L.; Zai, C.C.; Strauss, J. Investigation of correlations between DNA methylation, suicidal behavior and aging. Bipolar Disord. 2017, 19, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Bani-Fatemi, A.; Jeremian, R.; Wang, K.Z.; Silveira, J.; Zai, C.; Kolla, N.J.; Graff, A.; Gerretsen, P.; Strauss, J.; De Luca, V. Epigenome-wide association study of suicide attempt in schizophrenia. J. Psychiatr. Res. 2018, 104, 192–197. [Google Scholar] [CrossRef]
- Derivery, E.; Gautreau, A. Evolutionary conservation of the WASH complex, an actin polymerization machine involved in endosomal fission. Commun. Integr. Biol. 2010, 3, 227–230. [Google Scholar] [CrossRef]
- Haghighi, F.; Galfalvy, H.; Chen, S.; Huang, Y.Y.; Cooper, T.B.; Burke, A.K.; Oquendo, M.A.; Mann, J.J.; Sublette, M.E. DNA methylation perturbations in genes involved in polyunsaturated Fatty Acid biosynthesis associated with depression and suicide risk. Front. Neurol. 2015, 6, 92. [Google Scholar] [CrossRef]
- Labonte, B.; Yerko, V.; Gross, J.; Mechawar, N.; Meaney, M.J.; Szyf, M.; Turecki, G. Differential glucocorticoid receptor exon 1(B), 1(C), and 1(H) expression and methylation in suicide completers with a history of childhood abuse. Biol. Psychiatry 2012, 72, 41–48. [Google Scholar] [CrossRef] [PubMed]
- McGowan, P.O.; Sasaki, A.; D’Alessio, A.C.; Dymov, S.; Labonte, B.; Szyf, M.; Turecki, G.; Meaney, M.J. Epigenetic regulation of the glucocorticoid receptor in human brain associates with childhood abuse. Nat. Neurosci. 2009, 12, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Rizavi, H.S.; Khan, O.S.; Zhang, H.; Bhaumik, R.; Grayson, D.R.; Pandey, G.N. Methylation and expression of glucocorticoid receptor exon-1 variants and FKBP5 in teenage suicide-completers. Transl. Psychiatry 2023, 13, 53. [Google Scholar] [CrossRef] [PubMed]
- Kaminsky, Z.; Wilcox, H.C.; Eaton, W.W.; Van Eck, K.; Kilaru, V.; Jovanovic, T.; Klengel, T.; Bradley, B.; Binder, E.B.; Ressler, K.J.; et al. Epigenetic and genetic variation at SKA2 predict suicidal behavior and post-traumatic stress disorder. Transl. Psychiatry 2015, 5, e627. [Google Scholar] [CrossRef] [PubMed]
- Guintivano, J.; Brown, T.; Newcomer, A.; Jones, M.; Cox, O.; Maher, B.S.; Eaton, W.W.; Payne, J.L.; Wilcox, H.C.; Kaminsky, Z.A. Identification and replication of a combined epigenetic and genetic biomarker predicting suicide and suicidal behaviors. Am. J. Psychiatry 2014, 171, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Meaney, M.J. Effects of the Social Environment and Stress on Glucocorticoid Receptor Gene Methylation: A Systematic Review. Biol. Psychiatry 2016, 79, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.; Sarchiapone, M.; Zarrilli, F.; Videtic, A.; Ferraro, A.; Carli, V.; Sacchetti, S.; Lembo, F.; Angiolillo, A.; Jovanovic, N.; et al. Increased BDNF promoter methylation in the Wernicke area of suicide subjects. Arch. Gen. Psychiatry 2010, 67, 258–267. [Google Scholar] [CrossRef]
- Keller, S.; Sarchiapone, M.; Zarrilli, F.; Tomaiuolo, R.; Carli, V.; Angrisano, T.; Videtic, A.; Amato, F.; Pero, R.; di Giannantonio, M.; et al. TrkB gene expression and DNA methylation state in Wernicke area does not associate with suicidal behavior. J. Affect. Disord. 2011, 135, 400–404. [Google Scholar] [CrossRef]
- Ernst, C.; Deleva, V.; Deng, X.; Sequeira, A.; Pomarenski, A.; Klempan, T.; Ernst, N.; Quirion, R.; Gratton, A.; Szyf, M.; et al. Alternative splicing, methylation state, and expression profile of tropomyosin-related kinase B in the frontal cortex of suicide completers. Arch. Gen. Psychiatry 2009, 66, 22–32. [Google Scholar] [CrossRef]
- Maussion, G.; Yang, J.; Suderman, M.; Diallo, A.; Nagy, C.; Arnovitz, M.; Mechawar, N.; Turecki, G. Functional DNA methylation in a transcript specific 3’UTR region of TrkB associates with suicide. Epigenetics 2014, 9, 1061–1070. [Google Scholar] [CrossRef]
- Hotamisligil, G.S.; Breakefield, X.O. Human monoamine oxidase A gene determines levels of enzyme activity. Am. J. Hum. Genet. 1991, 49, 383–392. [Google Scholar] [PubMed]
- Poulter, M.O.; Du, L.; Weaver, I.C.G.; Palkovits, M.; Faludi, G.; Merali, Z.; Szyf, M.; Anisman, H. GABAA receptor promoter hypermethylation in suicide brain: Implications for the involvement of epigenetic processes. Biol. Psychiatry 2008, 64, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Shi, Y. Nuclear receptors in stem cells and their therapeutic potential. Adv. Drug Deliv. Rev. 2010, 62, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Swanson, C.J.; Bures, M.; Johnson, M.P.; Linden, A.M.; Monn, J.A.; Schoepp, D.D. Metabotropic glutamate receptors as novel targets for anxiety and stress disorders. Nat. Rev. Drug Discov. 2005, 4, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Nai, Q.; McIntosh, J.M.; Margiotta, J.F. Relating neuronal nicotinic acetylcholine receptor subtypes defined by subunit composition and channel function. Mol. Pharmacol. 2003, 63, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, A.; Fujiyoshi, Y.; Unwin, N. Structure and gating mechanism of the acetylcholine receptor pore. Nature 2003, 423, 949–955. [Google Scholar] [CrossRef]
- Stewart, L.C.; Klinman, J.P. Dopamine beta-hydroxylase of adrenal chromaffin granules: Structure and function. Annu. Rev. Biochem. 1988, 57, 551–592. [Google Scholar] [CrossRef] [PubMed]
- Schneider, E.; El Hajj, N.; Muller, F.; Navarro, B.; Haaf, T. Epigenetic Dysregulation in the Prefrontal Cortex of Suicide Completers. Cytogenet. Genome Res. 2015, 146, 19–27. [Google Scholar] [CrossRef]
- Gaine, M.E.; Seifuddin, F.; Sabunciyan, S.; Lee, R.S.; Benke, K.S.; Monson, E.T.; Zandi, P.P.; Potash, J.B.; Willour, V.L. Differentially methylated regions in bipolar disorder and suicide. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2019, 180, 496–507. [Google Scholar] [CrossRef]
- Romero-Pimentel, A.L.; Almeida, D.; Munoz-Montero, S.; Rangel, C.; Mendoza-Morales, R.; Gonzalez-Saenz, E.E.; Nagy, C.; Chen, G.; Aouabed, Z.; Theroux, J.F.; et al. Integrative DNA Methylation and Gene Expression Analysis in the Prefrontal Cortex of Mexicans Who Died by Suicide. Int. J. Neuropsychopharmacol. 2021, 24, 935–947. [Google Scholar] [CrossRef]
- Kozlenkov, A.; Jaffe, A.E.; Timashpolsky, A.; Apontes, P.; Rudchenko, S.; Barbu, M.; Byne, W.; Hurd, Y.L.; Horvath, S.; Dracheva, S. DNA Methylation Profiling of Human Prefrontal Cortex Neurons in Heroin Users Shows Significant Difference between Genomic Contexts of Hyper- and Hypomethylation and a Younger Epigenetic Age. Genes 2017, 8, 152. [Google Scholar] [CrossRef]
- Nagy, C.; Suderman, M.; Yang, J.; Szyf, M.; Mechawar, N.; Ernst, C.; Turecki, G. Astrocytic abnormalities and global DNA methylation patterns in depression and suicide. Mol. Psychiatry 2015, 20, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Mendoza, B.; Martinez-Magana, J.J.; Genis-Mendoza, A.D.; Monroy-Jaramillo, N.; Walss-Bass, C.; Fries, G.R.; Garcia-Dolores, F.; Lopez-Armenta, M.; Flores, G.; Vazquez-Roque, R.A.; et al. Brain Gene Expression-DNA Methylation Correlation in Suicide Completers: Preliminary Results. Rev. Investig. Clin. 2020, 73, 283–292. [Google Scholar] [CrossRef]
- Kouter, K.; Zupanc, T.; Videtic Paska, A. Genome-wide DNA methylation in suicide victims revealing impact on gene expression. J. Affect. Disord. 2019, 253, 419–425. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Molecular changes found in the brains of suicide victims with psychiatric disorders. In BP, alterations in the serotonergic system, the HPA-axis in the GABAergic system, and BDNF reduction have been found. In MDD, alterations in the HPA-axis, GABAergic-Glutamatergic system, BDNF reduction, and increased proinflammatory cytokines were detected. Increased proinflammatory cytokines and changes in the HPA-axis were found in AD. In schizophrenia, alterations in the serotonergic system, the HPA- axis, and the glutamatergic system were reported. In BPD, the changes found are associated with comorbidity with other disorders. Finally, alterations in the ECS have been found in the brains of alcoholics who committed suicide. AD: anxiety disorder, BD: bipolar disorder, BDNF: brain-derived neurotrophic factor, BPD: borderline personality disorder, ECS: endocannabinoid system, MDD: major depression disorders, SUD: substance use disorder.
Figure 1.
Molecular changes found in the brains of suicide victims with psychiatric disorders. In BP, alterations in the serotonergic system, the HPA-axis in the GABAergic system, and BDNF reduction have been found. In MDD, alterations in the HPA-axis, GABAergic-Glutamatergic system, BDNF reduction, and increased proinflammatory cytokines were detected. Increased proinflammatory cytokines and changes in the HPA-axis were found in AD. In schizophrenia, alterations in the serotonergic system, the HPA- axis, and the glutamatergic system were reported. In BPD, the changes found are associated with comorbidity with other disorders. Finally, alterations in the ECS have been found in the brains of alcoholics who committed suicide. AD: anxiety disorder, BD: bipolar disorder, BDNF: brain-derived neurotrophic factor, BPD: borderline personality disorder, ECS: endocannabinoid system, MDD: major depression disorders, SUD: substance use disorder.

Figure 2.
Flowchart linking early life adversity and suicidal behavior. up arrow: increase; down arrow: decrease.
Figure 2.
Flowchart linking early life adversity and suicidal behavior. up arrow: increase; down arrow: decrease.

Figure 3.
Main epigenetic changes in suicide behavior. The figure represents the main DNA methylation changes observed in peripheral blood cells and brain areas of patients with suicide behavior and in those who died by suicide, respectively. HPA axis: hypothalamus–pituitary–adrenal axis, NR3C1: gene encoding glucocorticoid receptor, FKBP5: the gene encoding the FK506-binding protein 5, CRHBP: the gene encoding the corticotropin-releasing hormone binding protein, SKA2: gene encoding spindle and kinetochore associated complex subunit 2, BDNF: the gene encoding the brain-derived neurotrophic factor, HTR1A: the gene encoding serotonin receptor 1 A, MAOA: the gene encoding monoamine oxidase A, SCL6A4: serotonin transporter gene, TPH2: gene encoding tryptophan hydroxylase 2, NRTK2: the gene encoding neurotrophic receptor tyrosine kinase 2; GABRA1: the gene encoding the alpha-1 subunit of the GABAA receptor protein.
Figure 3.
Main epigenetic changes in suicide behavior. The figure represents the main DNA methylation changes observed in peripheral blood cells and brain areas of patients with suicide behavior and in those who died by suicide, respectively. HPA axis: hypothalamus–pituitary–adrenal axis, NR3C1: gene encoding glucocorticoid receptor, FKBP5: the gene encoding the FK506-binding protein 5, CRHBP: the gene encoding the corticotropin-releasing hormone binding protein, SKA2: gene encoding spindle and kinetochore associated complex subunit 2, BDNF: the gene encoding the brain-derived neurotrophic factor, HTR1A: the gene encoding serotonin receptor 1 A, MAOA: the gene encoding monoamine oxidase A, SCL6A4: serotonin transporter gene, TPH2: gene encoding tryptophan hydroxylase 2, NRTK2: the gene encoding neurotrophic receptor tyrosine kinase 2; GABRA1: the gene encoding the alpha-1 subunit of the GABAA receptor protein.


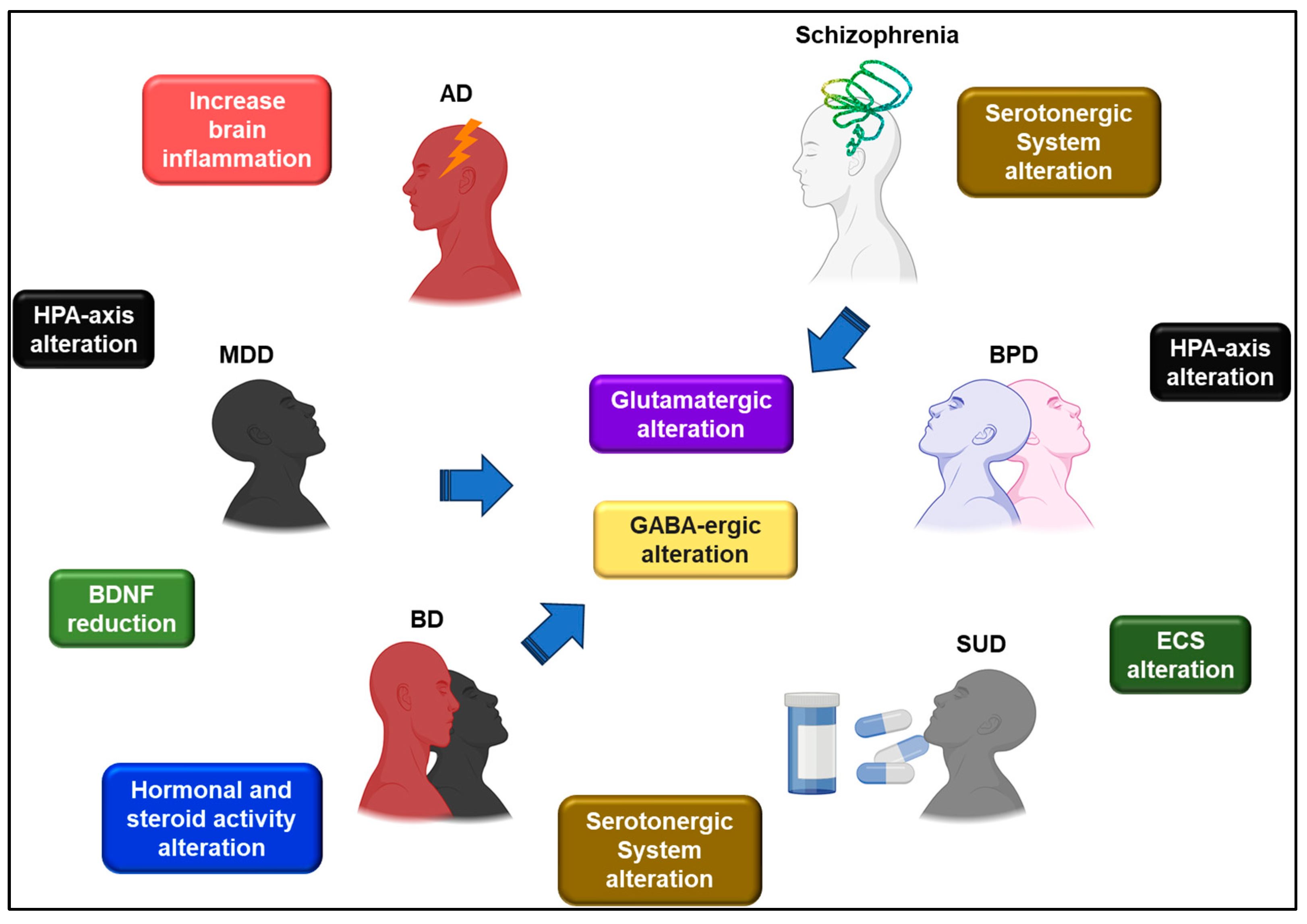{kind=link}
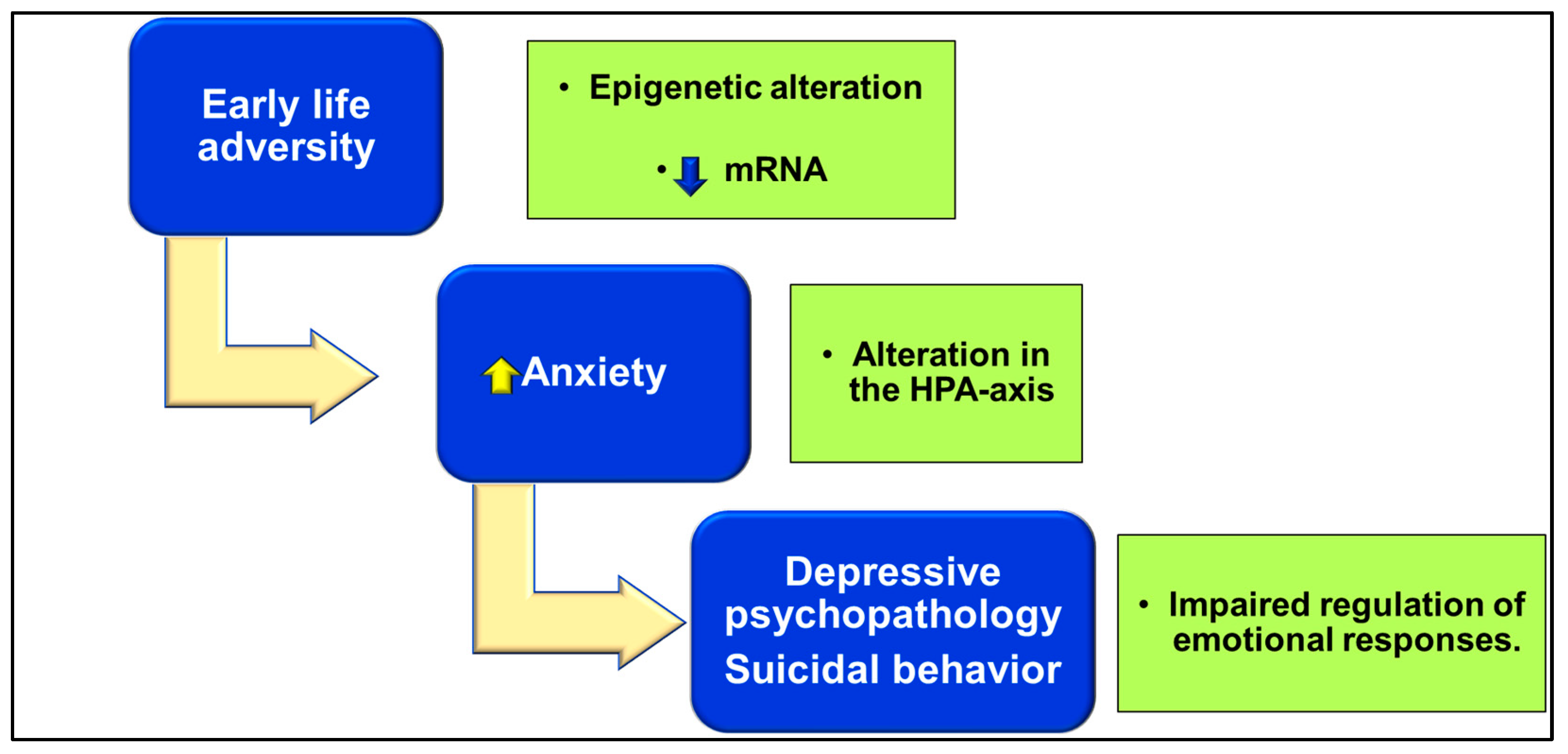{kind=link}
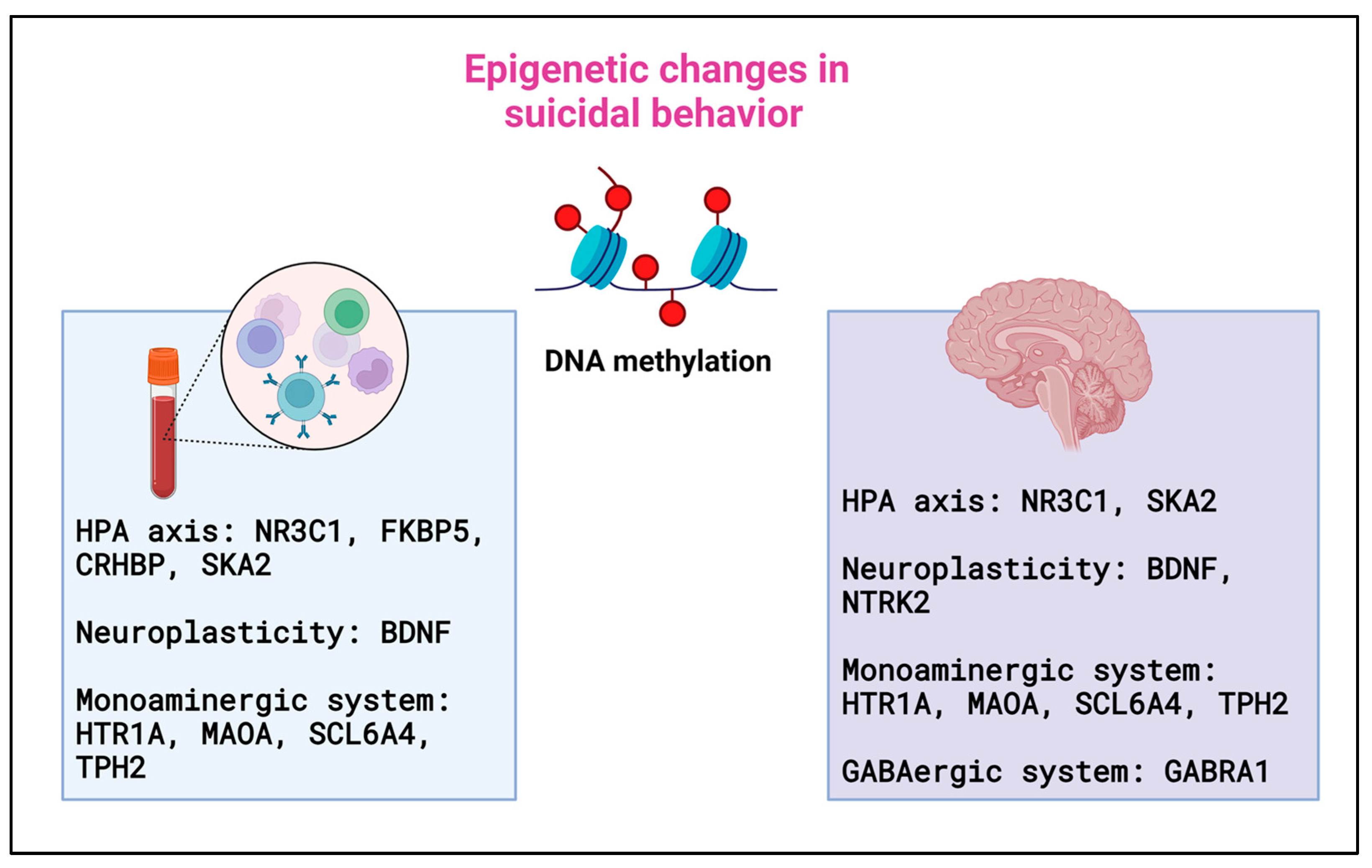{kind=link}
Table 1.
Main system alteration found in human samples of suicide attempters and completers.
| System Affected | Change | Sample (Males:Females) (M:F) | References |
|---|---|---|---|
| HPA axis | ↓ Plasma cortisol post-DST | MDD (28F) and MDD plus self-harm (29F) | [99] |
| ↓ Plasma cortisol post-stress levels | Suicide attempt (47, 17M:30F), suicidal ideation without attempt (53, 24M:29F) | [100] | |
| No correlation with 24-h urinary cortisol levels | General population 588F, 506M | [101] | |
| ↓ Baseline plasma cortisol levels and ↑ after stress exposure | MDD (126F) | [102] | |
| ↓ BDNF in ACC of suicide victims ↓ BDNF in ACC of ELA patients | ELA (13M), RLS (13M) | [103] | |
| ↑ CRH in FPC and DMPFC ↓ CRH1 gene expression in FPC | Suicide completers with MDD (11M:1F) | [104] | |
| ↑ CRH and NIDD in ACC | Suicide with MDD (17, 10M:7F) | [105] | |
| ↓ FKBP5 and GR gene and protein expression in AMY | Suicide completers (13M) | [106] | |
| ↓ GR transcript expression | Suicide completers (121M:F) | [107] | |
| Inflammatory markers | ↑ CXCL-1 in serum | Suicide risk and MDD (50, 15M:35F) | [108] |
| No changes in inflammatory markers | The general population with ELA and self-harm (4308F) | [109] | |
| No changes in oxidative status | Affective disorders (118, M:F) | [110] | |
| ↑ TNFα, IL-1β and IL6 gene and protein levels in PFC | Suicide completers (24, 14M:10F) | [111] | |
| ↓ Chemokines and IL10 and ↑ IL16 in PFC | Suicide completers (16, 10M:6F) | [112] | |
| ↑ IL4 and IL13 gene expression in OFC | Suicide completers (34, 20M:14F) | [113] | |
| ↓ VEGF in plasma | Suicide attempts (58, 23M:25F) | [114] | |
| ↑ IL6 and TNFα and ↓ IL2 in plasma | Suicide attempts (47, 21M:26F) | [115] | |
| ↓ VEGF in CSF | Suicide attempts (43: 15M:28F) | [116] | |
| ↑ IL6 in CSF | Suicide attempts (63, M:F) | [117] | |
| ↓ KA in ACC | Suicide completers with MDD (44) | [118] | |
| Neuropeptides | ↑ Plasma vasopressin and hypercortisolism | Suicide attempts (45, 18M:27F) | [121] |
| ↑ Plasma vasopressin and cortisol | MDD (19, 7M:12F) being 9 suicide attempts | [123] | |
| No changes were observed in the vasopressin levels | Suicide attempts and MDD (13, 9M:4F), non-attempts and MDD (15, 10M:5F) | [124] | |
| ↓ Serum oxytocin levels | Suicide attempts (48, 18M:30F) | [125] | |
| ↓ Plasma oxytocin levels after stress exposure | Suicide attempts (100, 30M:70F) | [126] | |
| ↓ CSF oxytocin levels | Suicide attempts (28, 18M:10F) | [127] | |
| ↓ Neuropeptide Y in frontal cortex and caudate nucleus | Suicide completers (26, 21M:5F) | [128] | |
| ↓ Neuropeptide Y gene expression in the PFC in BD | Suicide completers (SZP 15, 9M:6F; BD 15, 9M:6F; MDD 15, 9M:6F) | [129] | |
| ↓ Neuropeptide Y and ↑ NPY1R and NPY2R gene expression in PFC and HIPP | Suicide completers with MDD (24, 14M:10F) | [130] | |
| Serotonergic system | ↓ 5-HT1A binding and total number in the DRN ↓ 5-HT1A gene expression in the DRN | Depressed suicide victims (6M:4F) | [133] |
| ↑ 5-HT1A binding in the PFC ↓ 5-HT1A binding in the PFC | Suicide completers (14M:8F) | [134] | |
| ↑ TPH I7779C (L) allele frequency | Alcoholic violent offenders (185M) | [135] | |
| No association of the promoter (-7065CT) and intron 7 (218AC) polymorphisms of TPH1 gene | Violent suicide (160M) | [137] | |
| No association between A779C and A218C in the intron of TPH gene No association of Pro 16Leu in the coding region of 5-HT1A | Suicide victims in the Japanese population (95M:39F) | [138] | |
| No changes in SLC6A4 and TPH1 mRNA levels in VPFC ↑ TPH2 gene expression in VPFC No association of SNPs10748185 in the promoter region of TPH2 | Suicide victims (27M:13F) | [139] | |
| ↑ Frequency long allele of 5-HT1A | Depressed suicide victims (34M) Suicide victims (102M:33F) | [140] [141] | |
| No association of SNPs in 5-HT2A, 5-HT2C, 5-HTT | Suicide attempters (127M:126F) | [142] | |
| Endocannabinoid System | ↓ CB2r and GPR55 gene expressions in the DLPFCx ↑ CB2r protein in the DLPFCx ↑CB2r-GPR55 heteromers in the DLPFC | Suicide completers (18M) | [162] |
| ↑ CB1r protein in DLPFCx ↑ AEA and 2-AG in DLPFCx | Alcohol-dependents who died by suicide (7M:11F) | [163] | |
| ↑ CB1r protein and binding, and FAAH activity in the ventral striatum | Alcohol-dependents who died by suicide (9M) | [164] | |
| ↑ CB1r density and binding in DLPFCx | MDD who died by suicide. (24M) | [165] | |
| ↑ AEA and PEA in serum | Suicide attempters (8M:22F) | [166] | |
| GABAergic System | GABAA gene expression (alpha1, alpha3, alpha4, and delta receptor subunits) in PFC | Suicide completers (11M:1F) | [104] |
| ↓ VGAT-ir in HIPP | Suicide completers (28M) | [170] | |
| Alterations in GABAergic-related genes in PFC and HIP | Suicide completers with and without MDD (16:10) | [171] | |
| ↓GABRG2 in DLPFCx | Suicide completers with MDD (13M:8F) | [173] | |
| ↑ GABAergic-related genes in ACC ↓ GABAergic-related genes in DLPFCx | MDD suicide completers (10M:7F) | [174] | |
| Glutamatergic System | mGluR5 gene expression in the AMY and HIPP ↑ VGluT1-ir in HIPP | Suicide completers (28M) | [170] |
| Alterations in glutamatergic-related genes in PFC and HIP | Suicide completers with and without MDD (16:10) | [171] | |
| ↑ Glutamatergic-related genes in ACC ↓ Glutamatergic-related genes in DLPFCx | MDD suicide completers (10M:7F) | [174] |
↑: increase; ↓: decrease; 2-AG: 2-arachidonoylglycerol; ACC: anterior cingulate cortex; AEA: anandamide; AMY: amygdala; BD: bipolar disorder; CB1r: cannabinoid receptor 1; CB2r: cannabinoid receptor 2; CRH: corticotropin-releasing hormone;CRH1: corticotropin-releasing hormone receptor 1; CSF: cerebrospinal fluid; CXCL-1: chemokine ligand 1; DLPFCx: dorsolateral prefrontal cortex; DMPFC: dorsomedial prefrontal cortex; DRN: dorsal raphe nucleus; DST: dexamethasone suppression test; ELA: early life stress; FAAH: fatty acid amide hydrolase; FKBP5: FK506-binding protein 5; FPC: frontopolar cortex; GABAA: gamma aminobutyric type A receptor; GABRG2: gamma-aminobutyric acid type A receptor subunit gamma 2; GPR55: G protein-coupled receptor 55; GR: glucocorticoid receptor; HIPP: hippocampus; 5-HT1A: serotonin receptor 1A; 5-HT2A: serotonin receptor 2A; 5-HT2C: serotonin receptor 2C; 5-HTT: serotonin transporter; IL-1β: interleukine 1-beta; IL-2: interleukine 2; IL-6: interleukine 6; KA: kynurenic acid; MDD: major depressive disorders; mGluR5: metabotropic glutamate receptor subtype 5; NIDD: NOS1-interacting DHHC domain-containing protein with dendritic mRNA; NPY1R: neuropeptide Y receptor 1; NPY2R: neuropeptide Y receptor 2; OFC: orbitofrontal cortex; PEA: palmitoylethanolamide; PFC: prefrontal cortex; RLS: recent life stress; SNPs: single nucleotide polymorphisms; SLC6A4: gene that codifies serotonin transporter; SZP: schizophrenia; TNFα: tumor necrosis factor-alpha; TPH: tryptophan hydroxylase; TPH2: tryptophan hydroxylase 2; TPH1: tryptophan hydroxylase 1; VEGF: vascular endothelial growth factor; VGAT-ir: vesicular GABA transporter immunoreactivity; VGluT1-ir: vesicular glutamate transporter 1 immunoreactivity; VPFC: ventromedial prefrontal cortex.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Navarro, D.; Marín-Mayor, M.; Gasparyan, A.; García-Gutiérrez, M.S.; Rubio, G.; Manzanares, J. Molecular Changes Associated with Suicide. Int. J. Mol. Sci. 2023, 24, 16726. https://doi.org/10.3390/ijms242316726
AMA Style
Navarro D, Marín-Mayor M, Gasparyan A, García-Gutiérrez MS, Rubio G, Manzanares J. Molecular Changes Associated with Suicide. International Journal of Molecular Sciences. 2023; 24(23):16726. https://doi.org/10.3390/ijms242316726
Chicago/Turabian StyleNavarro, Daniela, Marta Marín-Mayor, Ani Gasparyan, María Salud García-Gutiérrez, Gabriel Rubio, and Jorge Manzanares. 2023. "Molecular Changes Associated with Suicide" International Journal of Molecular Sciences 24, no. 23: 16726. https://doi.org/10.3390/ijms242316726
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.