
Serum Reactive Antibodies against the N-Methyl-D-Aspartate Receptor NR2 Subunit—Could They Act as Potential Biomarkers?

 and
and
Abstract
:1. Introduction
2. Results
2.1. Clinical and Nonclinical Data of Study Participants
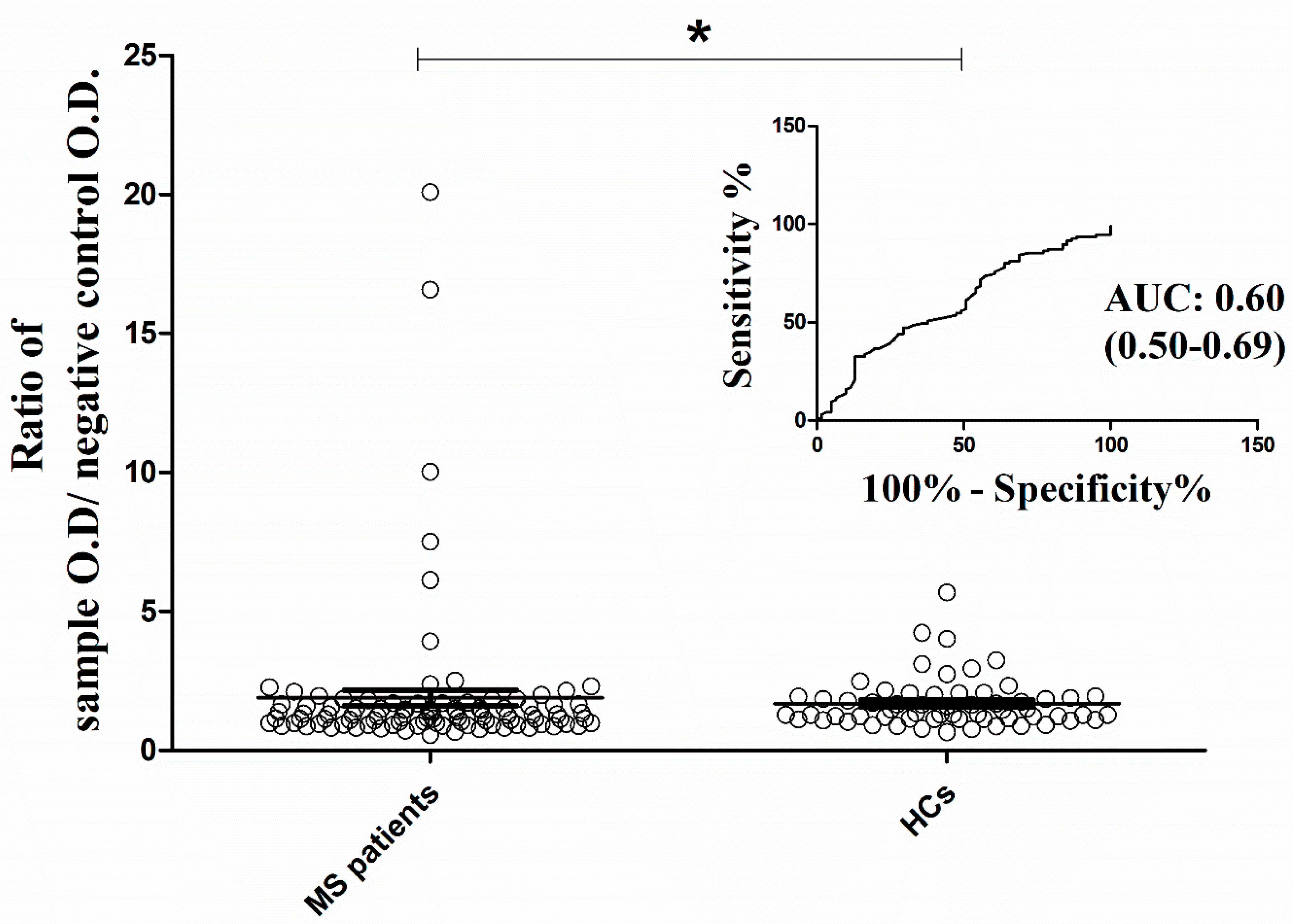
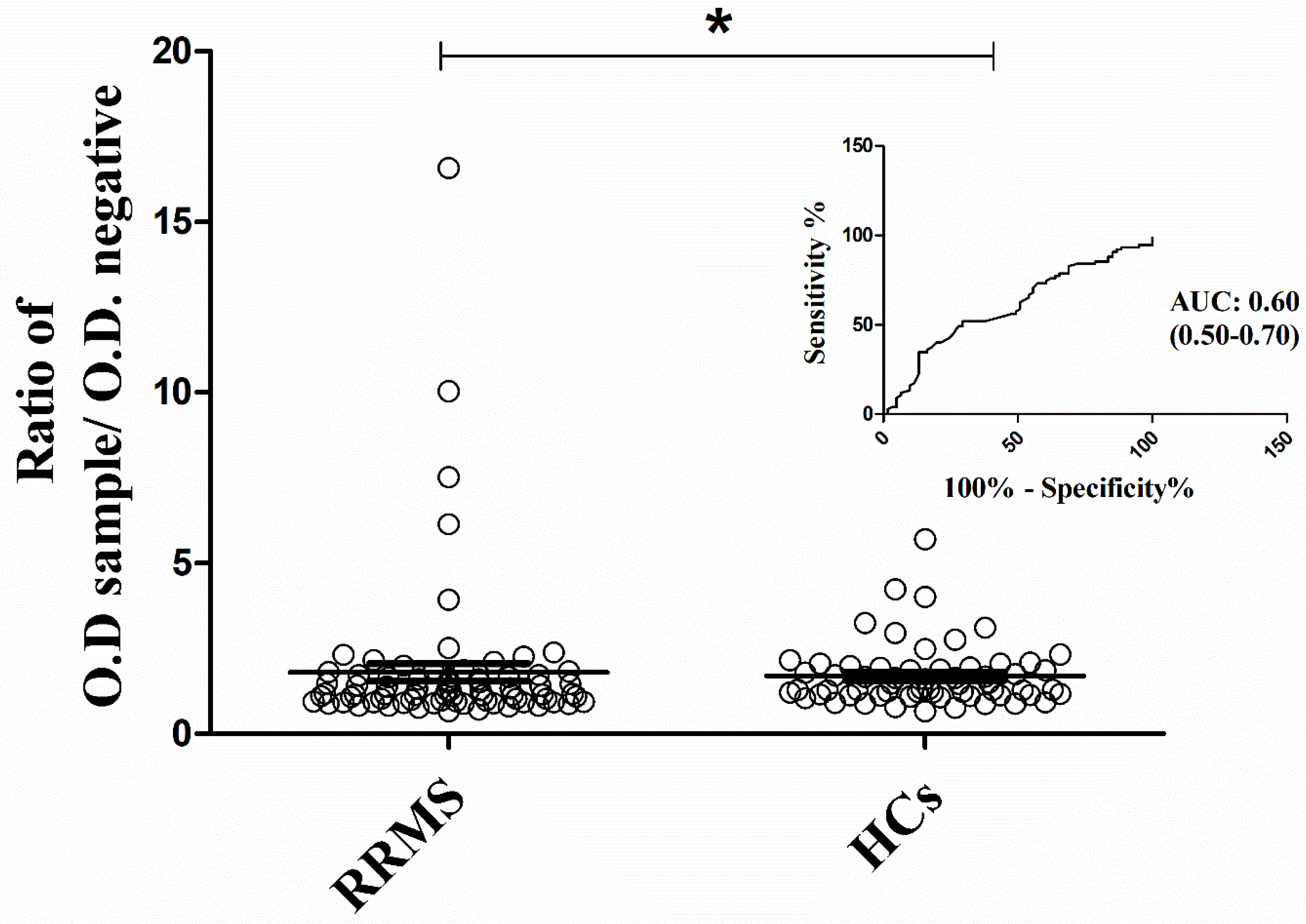
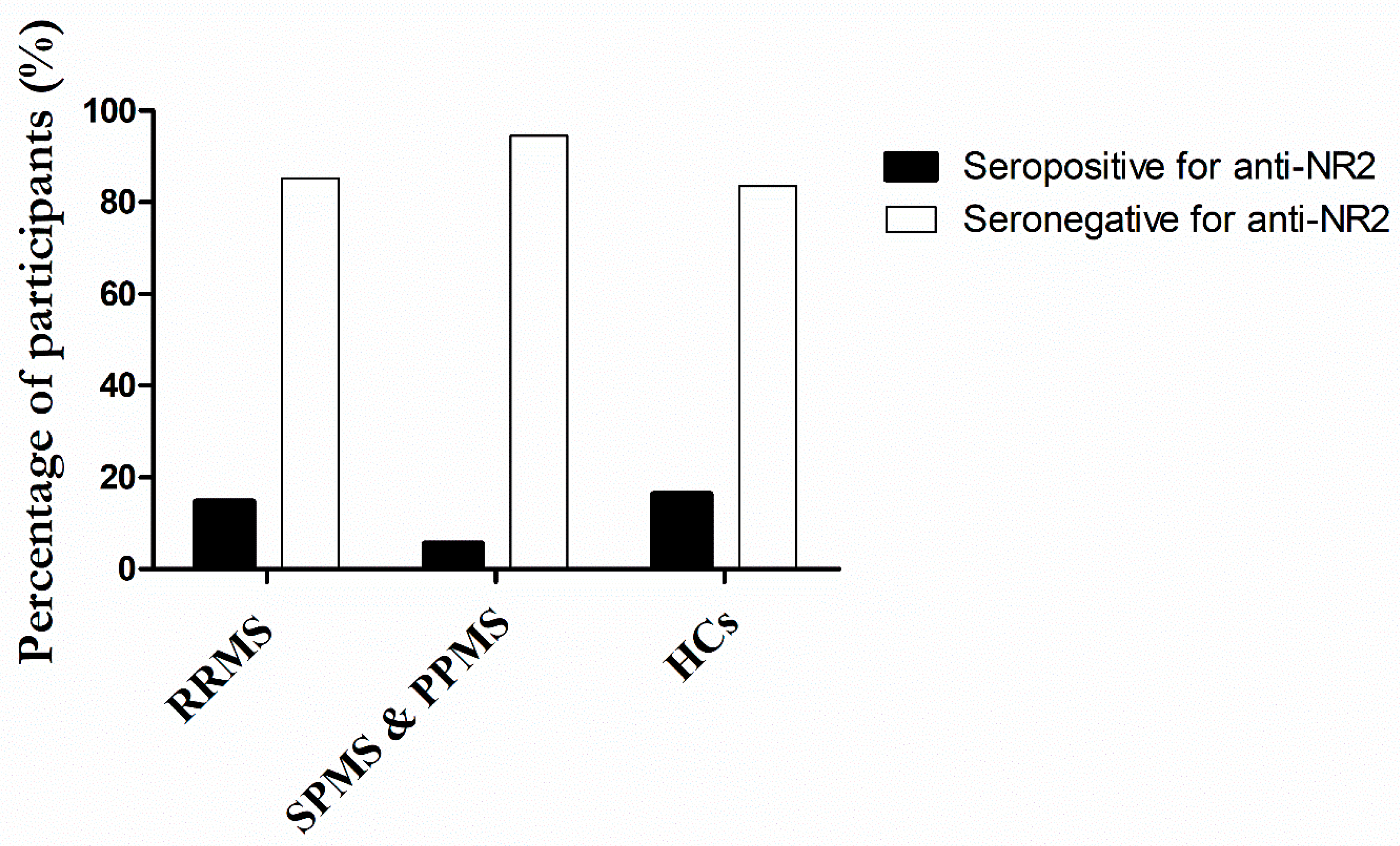
2.2. Qualitative Analysis of Antibody Binding Activity against NR2 Subunit
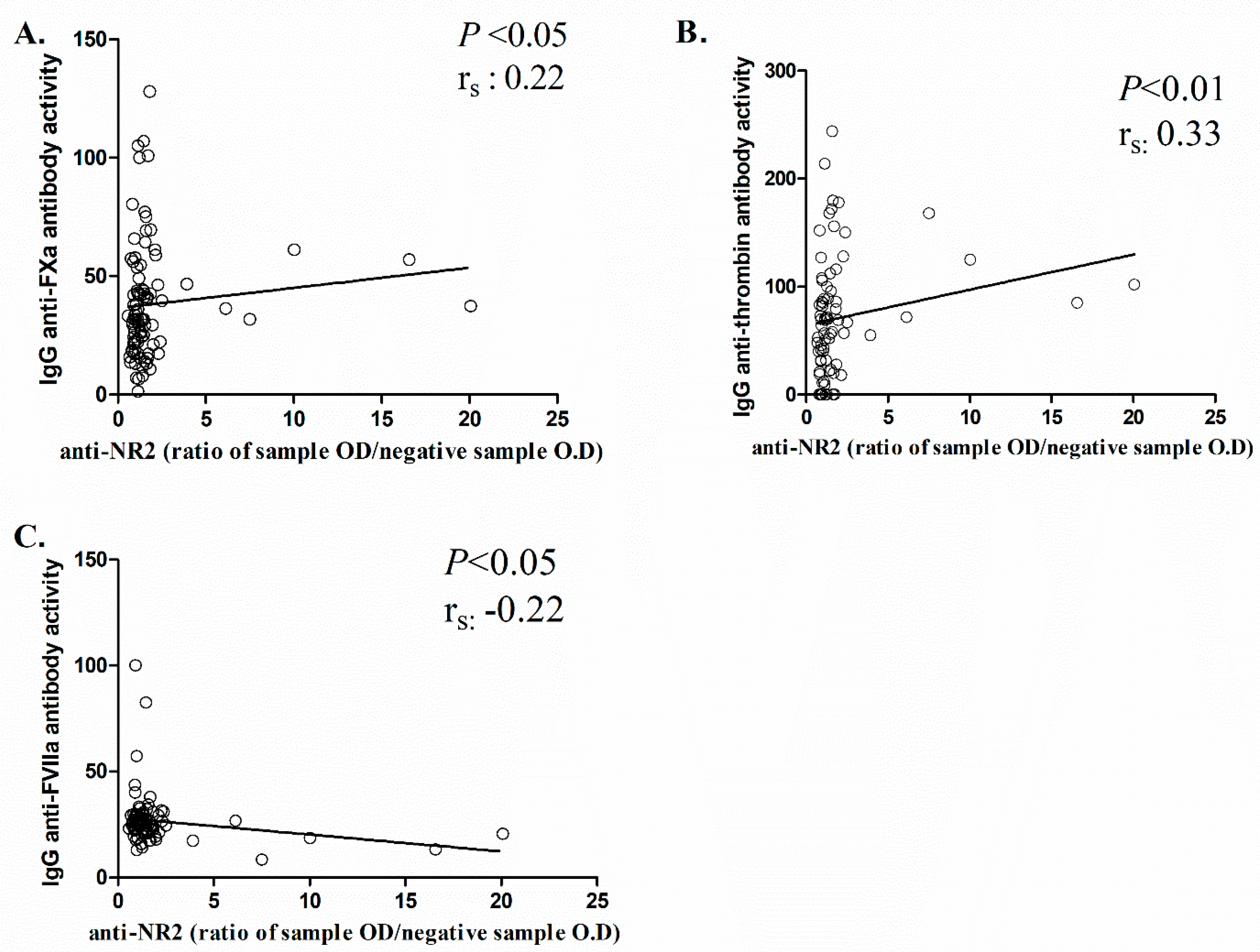
2.3. Correlation between Anti-NR2 Antibody Levels and Clinical/Laboratory Outcomes of MS Patients
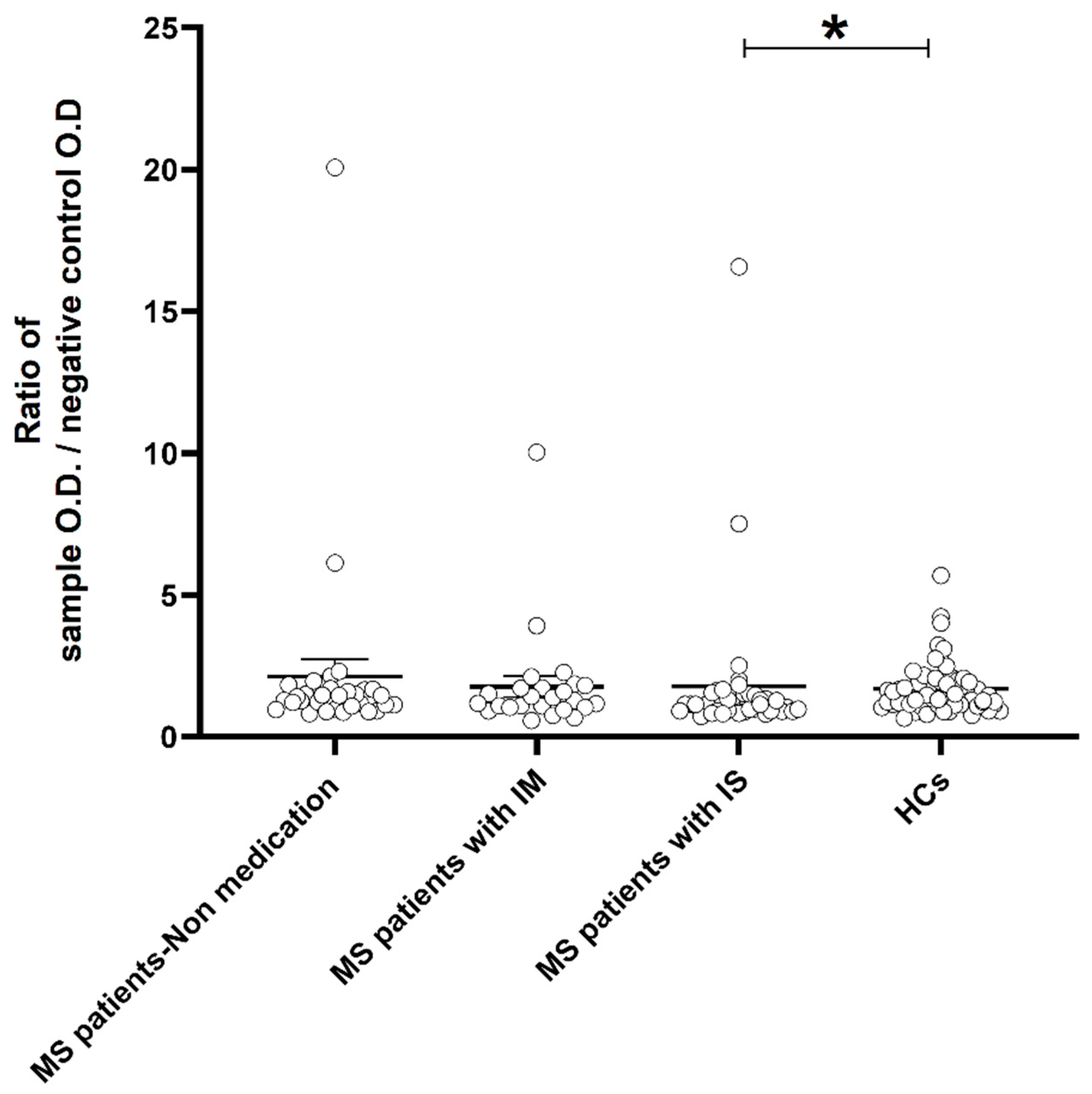
2.4. Analysis between Anti-NR2 Antibody Levels and Receiving Medications for MS Treaatment
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Serum Collection
4.3. Determination of Human Glutamate [NMDA] Receptor Subunit Epsilon-2 (NR2) Antibody
4.4. Qualitative Determination of Activity to Coagulant Serine Proteases
4.4.1. Activity to FVIIa
4.4.2. Activity to Thrombin
4.4.3. Activity to Prothrombin
4.4.4. Activity to FXa
4.4.5. Activity to Plasmin
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oudejans, E.; Luchicchi, A.; Strijbis, E.M.M.; Geurts, J.J.G.; van Dam, A.M. Is MS Affecting the CNS Only? Lessons from Clinic to Myelin Pathophysiology. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e914. [Google Scholar] [CrossRef] [PubMed]
- Bellingacci, L.; Mancini, A.; Gaetani, L.; Tozzi, A.; Parnetti, L.; Di Filippo, M. Synaptic Dysfunction in Multiple Sclerosis: A Red Thread from Inflammation to Network Disconnection. Int. J. Mol. Sci. 2021, 22, 9753. [Google Scholar] [CrossRef] [PubMed]
- Filiano, A.J.; Xu, Y.; Tustison, N.J.; Marsh, R.L.; Baker, W.; Smirnov, I.; Overall, C.C.; Gadani, S.P.; Turner, S.D.; Weng, Z.; et al. Unexpected Role of Interferon-γ 3 in Regulating Neuronal Connectivity and Social Behaviour. Nature 2016, 535, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, I.R.; Kostic, M.; Ljubisavljevic, S. The Role of Glutamate and Its Receptors in Multiple Sclerosis. J. Neural Transm. 2014, 121, 945–955. [Google Scholar] [CrossRef]
- Kostic, M.; Zivkovic, N.; Stojanovic, I. Multiple Sclerosis and Glutamate Excitotoxicity. Rev. Neurosci. 2013, 24, 71–88. [Google Scholar] [CrossRef]
- Vandame, D.; Ulmann, L.; Teigell, M.; Prieto-Cappellini, M.; Vignon, J.; Privat, A.; Perez-Polo, R.; Nesic, O.; Hirbec, H. Development of NMDAR Antagonists with Reduced Neurotoxic Side Effects: A Study on GK11. PLoS ONE 2013, 8, e81004. [Google Scholar] [CrossRef]
- Ge, Y.; Chen, W.; Axerio-Cilies, P.; Wang, Y.T. NMDARs in Cell Survival and Death: Implications in Stroke Pathogenesis and Treatment. Trends Mol. Med. 2020, 26, 533–551. [Google Scholar] [CrossRef]
- Guo, F.; Maeda, Y.; Ko, E.M.; Delgado, M.; Horiuchi, M.; Soulika, A.; Miers, L.; Burns, T.; Itoh, T.; Shen, H.; et al. Disruption of NMDA Receptors in Oligodendroglial Lineage Cells Does Not Alter Their Susceptibility to Experimental Autoimmune Encephalomyelitis or Their Normal Development. J. Neurosci. 2012, 32, 639–645. [Google Scholar] [CrossRef]
- Gibson, L.L.; Pollak, T.A.; Hart, M.; Heslegrave, A.; Hye, A.; Church, A.J.; Lakdawala, N.; Nicholson, T.R.; Batzu, L.; Rota, S.; et al. NMDA Receptor Antibodies and Neuropsychiatric Symptoms in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 2023, 35, 236–243. [Google Scholar] [CrossRef]
- Hunter, D.; Jamet, Z.; Groc, L. Autoimmunity and NMDA Receptor in Brain Disorders: Where Do We Stand? Neurobiol. Dis. 2021, 147, 105161. [Google Scholar] [CrossRef]
- Bidari, A.; Vaziri, S.; Moazen Zadeh, E.; Farahmand, S.; Talachian, E. The Value of Serum NR2 Antibody in Prediction of Post-Cardiopulmonary Resuscitation Survival. Emerg. J. 2015, 3, 89–94. [Google Scholar]
- Liu, P.; Yan, H.; Li, H.; Zhang, C.; Li, Y. Overlapping Anti-NMDAR Encephalitis and Multiple Sclerosis: A Case Report and Literature Review. Front. Immunol. 2023, 14, 1088801. [Google Scholar] [CrossRef] [PubMed]
- Lauvsnes, M.B.; Omdal, R. Systemic Lupus Erythematosus, the Brain, and Anti-NR2 Antibodies. J. Neurol. 2012, 259, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Bosch, X.; Ramos-Casals, M.; Khamashta, M.A. The DWEYS Peptide in Systemic Lupus Erythematosus. Trends Mol. Med. 2012, 18, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Levite, M.; Ganor, Y. Autoantibodies to Glutamate Receptors Can Damage the Brain in Epilepsy, Systemic Lupus Erythematosus and Encephalitis. Expert. Rev. Neurother. 2008, 8, 1141–1160. [Google Scholar] [CrossRef] [PubMed]
- Hughes, E.G.; Peng, X.; Gleichman, A.J.; Lai, M.; Zhou, L.; Tsou, R.; Parsons, T.D.; Lynch, D.R.; Dalmau, J.; Balice-Gordon, R.J. Cellular and Synaptic Mechanisms of Anti-NMDA Receptor Encephalitis. J. Neurosci. 2010, 30, 5866–5875. [Google Scholar] [CrossRef]
- Kaplan, T.B.; Berkowitz, A.L.; Samuels, M.A. Cardiovascular Dysfunction in Multiple Sclerosis. Neurologist 2015, 10, 364–370. [Google Scholar] [CrossRef]
- Mincu, R.I.; Magda, S.L.; Mihaila, S.; Florescu, M.; Mihalcea, D.J.; Velcea, A.; Chiru, A.; Tiu, C.; Popescu, B.O.; Cinteza, M.; et al. Impaired Cardiac Function in Patients with Multiple Sclerosis by Comparison with Normal Subjects. Sci. Rep. 2018, 8, 3300. [Google Scholar] [CrossRef]
- Liu, Z.Y.; Hu, S.; Zhong, Q.W.; Tian, C.N.; Ma, H.M.; Yu, J.J. N-Methyl-D-Aspartate Receptor-Driven Calcium Influx Potentiates the Adverse Effects of Myocardial Ischemia-Reperfusion Injury Ex Vivo. J. Cardiovasc. Pharmacol. 2017, 70, 329–338. [Google Scholar] [CrossRef]
- Govoruskina, N.; Jakovljevic, V.; Zivkovic, V.; Milosavljevic, I.; Jeremic, J.; Bradic, J.; Bolevich, S.; Omarov, I.A.; Djuric, D.; Radonjic, K.; et al. The Role of Cardiac N-Methyl-D-Aspartate Receptors in Heart Conditioning—Effects on Heart Function and Oxidative Stress. Biomolecules 2020, 10, 1065. [Google Scholar] [CrossRef]
- Hadjiagapiou, M.S.; Krashias, G.; Deeba, E.; Christodoulou, C.; Pantzaris, M.; Lambrianides, A. Antibodies to Blood Coagulation Components Are Implicated in Patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 62, 103775. [Google Scholar] [CrossRef] [PubMed]
- Hadjiagapiou, M.S.; Krashias, G.; Deeba, E.; Christodoulou, C.; Pantzaris, M.; Lambrianides, A. A Preclinical Investigation on the Role of IgG Antibodies against Coagulant Components in Multiple Sclerosis. Biomedicines 2023, 11, 906. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.K.; Petersen, M.A.; Murray, S.G.; Baeten, K.M.; Meyer-Franke, A.; Chan, J.P.; Vagena, E.; Bedard, C.; Machado, M.R.; Coronado, P.E.R.; et al. Blood Coagulation Protein Fibrinogen Promotes Autoimmunity and Demyelination via Chemokine Release and Antigen Presentation. Nat. Commun. 2015, 6, 8164. [Google Scholar] [CrossRef]
- Grover, S.P.; Mackman, N. Tissue Factor: An Essential Mediator of Hemostasis and Trigger of Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 709–725. [Google Scholar] [CrossRef] [PubMed]
- Spronk, H.M.H.; Ten Cate, H.; Van Der Meijden, P.E.J. Differential Roles of Tissue Factor and Phosphatidylserine in Activation of Coagulation. Thromb. Res. 2014, 133, S54–S56. [Google Scholar] [CrossRef]
- Kamikubo, Y.; Mendolicchio, G.L.; Zampolli, A.; Marchese, P.; Rothmeier, A.S.; Orje, J.N.; Gale, A.J.; Krishnaswamy, S.; Gruber, A.; Østergaard, H.; et al. Selective Factor VIII Activation by the Tissue Factor–Factor VIIa–Factor Xa Complex. Blood 2017, 130, 1661–1670. [Google Scholar] [CrossRef]
- Renné, T.; Schmaier, A.H.; Nickel, K.F.; Blombäck, M.; Maas, C. In Vivo Roles of Factor XII. Blood 2012, 120, 4296–4303. [Google Scholar] [CrossRef]
- Rezaie, A.R. Protease-Activated Receptor Signalling by Coagulation Proteases in Endothelial Cells. Thromb. Haemost. 2014, 112, 876–882. [Google Scholar] [CrossRef]
- Davalos, D.; Kyu Ryu, J.; Merlini, M.; Baeten, K.M.; Le Moan, N.; Petersen, M.A.; Deerinck, T.J.; Smirnoff, D.S.; Bedard, C.; Hakozaki, H.; et al. Fibrinogen-Induced Perivascular Microglial Clustering Is Required for the Development of Axonal Damage in Neuroinflammation. Nat. Commun. 2012, 3, 1227. [Google Scholar] [CrossRef]
- Charalambidou, E.; Pantzaris, M.; Patrikios, I. Multiple Sclerosis in Cyprus: A Fourteen Year (2000–2014) Epidemiological Study. Am. J. Epidemiol. Infect. Dis. 2016, 4, 1–9. [Google Scholar] [CrossRef]
- Möck, E.E.A.; Honkonen, E.; Airas, L. Synaptic Loss in Multiple Sclerosis: A Systematic Review of Human Post-Mortem Studies. Front. Neurol. 2021, 29, 782599. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, M.; Portaccio, E.; Mancini, A.; Calabresi, P. Multiple Sclerosis and Cognition: Synaptic Failure and Network Dysfunction. Nat. Rev. Neurosci. 2018, 19, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Q.; Zeng, S.; Zhang, Y.; Zou, L.; Fu, X.; Xu, Q. Case Report: Overlapping Multiple Sclerosis With Anti-N-Methyl-D-Aspartate Receptor Encephalitis: A Case Report and Review of Literature. Front. Immunol. 2020, 11, 595417. [Google Scholar] [CrossRef] [PubMed]
- Ramberger, M.; Bsteh, G.; Schanda, K.; Hoftberger, R.; Rostasy, K.; Baumann, M.; Djamshidian, F.A.; Lutterotti, A.; Deisenhammer, F.; Berger, T.; et al. NMDA Receptor Antibodies: A Rare Association in Inflammatory Demyelinating Diseases. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e141. [Google Scholar] [CrossRef]
- Hirohata, S.; Arinuma, Y.; Yanagida, T.; Yoshio, T. Blood-Brain Barrier Damages and Intrathecal Synthesis of Anti-N-Methyl-D-Aspartate Receptor NR2 Antibodies in Diffuse Psychiatric/Neuropsychological Syndromes in Systemic Lupus Erythematosus. Arthritis Res. Ther. 2014, 16, R77. [Google Scholar] [CrossRef] [PubMed]
- Degiorgio, L.A.; Konstantinov, K.N.; Lee, S.C.; Hardin, J.A.; Volpe, B.T.; Diamond, B. A Subset of Lupus Anti-DNA Antibodies Cross-Reacts with the NR2 Glutamate Receptor in Systemic Lupus Erythematosus. Nat. Med. 2001, 7, 1189–1193. [Google Scholar] [CrossRef]
- Kowal, C.; DeGiorgio, L.A.; Nakaoka, T.; Hetherington, H.; Huerta, P.T.; Diamond, B.; Volpe, B.T. Cognition and Immunity: Antibody Impairs Memory. Immunity 2004, 21, 179–188. [Google Scholar] [CrossRef]
- González-García, S.; González-Quevedo, A.; Hernandez-Diaz, Z.; Alvarez Camino, L.; Peña-Sanchez, M.; Cordero-Eiriz, A.; Brown, M.; Gaya, J.A.; Betancourt-Losa, M.; Fernandez-Almirall, I.; et al. Circulating Autoantibodies against the NR2 Peptide of the NMDA Receptor Are Associated with Subclinical Brain Damage in Hypertensive Patients with Other Pre-Existing Conditions for Vascular Risk. J. Neurol. Sci. 2017, 375, 324–330. [Google Scholar] [CrossRef]
- Dobrynina, L.A.; Alexandrova, E.V.; Zabitova, M.R.; Kalashnikova, L.A.; Krotenkova, M.V.; Akhmetzyanov, B.M. Anti-NR2 Glutamate Receptor Antibodies as an Early Biomarker of Cerebral Small Vessel Disease. Clin. Biochem. 2021, 96, 26–32. [Google Scholar] [CrossRef]
- Tran, P.; Thoprakarn, U.; Gourieux, E.; dos Santos, C.L.; Cavedo, E.; Guizard, N.; Cotton, F.; Krolak-Salmon, P.; Delmaire, C.; Heidelberg, D.; et al. Automatic Segmentation of White Matter Hyperintensities: Validation and Comparison with State-of-the-Art Methods on Both Multiple Sclerosis and Elderly Subjects. Neuroimage Clin. 2022, 33, 102940. [Google Scholar] [CrossRef]
- Bidot, C.J.; Jy, W.; Horstman, L.L.; Huisheng, H.; Jimenez, J.J.; Yaniz, M.; Ahn, Y.S. Factor VII/VIIa: A New Antigen in the Anti-Phospholipid Antibody Syndrome. Br. J. Haematol. 2003, 120, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, M.S.; Birktoft, J.J.; Steer, S.A.; Bajaj, S.P. Structure and Biology of Tissue Factor Pathway Inhibitor. Thromb. Haemost. 2001, 86, 959–972. [Google Scholar] [PubMed]
- Lenoir, S.; Varangot, A.; Lebouvier, L.; Galli, T.; Hommet, Y.; Vivien, D. Post-Synaptic Release of the Neuronal Tissue-Type Plasminogen Activator (TPA). Front. Cell Neurosci. 2019, 13, 164. [Google Scholar] [CrossRef]
- Lin, H.; Xu, L.; Yu, S.; Hong, W.; Huang, M.; Xu, P. Therapeutics Targeting the Fibrinolytic System. Exp. Mol. Med. 2020, 52, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Fredriksson, L.; Lawrence, D.A.; Medcalf, R.L. TPA Modulation of the Blood-Brain Barrier: A Unifying Explanation for the Pleiotropic Effects of TPA in the CNS. Semin. Thromb. Hemost. 2017, 43, 154–168. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic Criteria for Multiple Sclerosis: 2010 Revisions to the McDonald Criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Artim-Esen, B.; Pericleous, C.; Mackie, I.; Ripoll, V.M.; Latchman, D.; Isenberg, D.; Rahman, A.; Ioannou, Y.; Giles, I. Anti-Factor Xa Antibodies in Patients with Antiphospholipid Syndrome and Their Effects upon Coagulation Assays. Arthritis Res. Ther. 2015, 17, 47. [Google Scholar] [CrossRef]
- Matsuda, J.; Sanaka, T.; Nishizawa, A.; Gotoh, M.; Gohchi, K. Two Antiprothrombin Antibodies against Prothrombin and Prothrombin-Phosphatidyl Serine Show Partial but Not Total Identity. Blood Coagul. Fibrinolysis 2002, 13, 697–702. [Google Scholar] [CrossRef]
- Yang, Y.-H.; Hwang, K.-K.; FitzGerald, J.; Grossman, J.M.; Taylor, M.; Hahn, B.H.; Chen, P.P. Antibodies against the Activated Coagulation Factor X (FXa) in the Antiphospholipid Syndrome That Interfere with the FXa Inactivation by Antithrombin. J. Immunol. 2006, 177, 8219–8225. [Google Scholar] [CrossRef]
- Lambrianides, A.; Turner-Stokes, T.; Pericleous, C.; Ehsanullah, J.; Papadimitraki, E.; Poulton, K.; Ioannou, Y.; Lawrie, A.; MacKie, I.; Chen, P.; et al. Interactions of Human Monoclonal and Polyclonal Antiphospholipid Antibodies with Serine Proteases Involved in Hemostasis. Arthritis Rheum. 2011, 63, 3512–3521. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | MS Patients (n = 95) | HCs (n = 61) | p Value | RRMS (n = 75) | p Value |
|---|---|---|---|---|---|
| Gender | |||||
| Female/Male | 60/35 | 33/28 | 0.31 | 47/28 | 0.38 |
| Age in years | |||||
| Mean ± SD | 48 ± 14 | 43.5 ± 12 | 0.06 | 45.4 ± 13 | |
| Min–Max | 21–80 | 23–66 | 21–80 | 0.53 | |
| Disease course (CIS/RRMS/SPMS/PPMS) | |||||
| 1/75/16/3 | N/A | ||||
| Disease Duration (years) | 15.16 ± 9.6 | ||||
| Mean ± SD | 16.23 ± 9.4 | N/A | 15 (9–21) | ||
| Median (interquartile range) | 17 (11–22) | ||||
| EDSS | |||||
| Median (interquartile range) | 3.5 (2.25–4.80) | N/A | 3.0 (2.0–4.0) | ||
| Mild: 0–3.0 [n (%)] | 45 (47.4) | 42 (56.0) | |||
| Moderate: 3.5–5.5 [n (%)] | 34 (35.8) | 26 (34.7) | |||
| Severe: 6.0–9.5 [n (%)] | 16 (16.8) | 7 (9.3) | |||
| MSSS | |||||
| Median (interquartile range) | 3.4 (2.4–5.5) | N/A | 3.05 (2.1–4.3) | ||
| Benign MS: 1–2 [n (%)] | 17 (17.9) | 15 (20.0) | |||
| Severe MS: 7–10 [n (%)] | 10 (10.5) | 5 (6.7) | |||
| Medication [n (%)] | N/A | ||||
| Interferon beta-1a or -1b | 20 (21.0) | 20 (26.7) | |||
| Natalizumab | 12 (12.7) | 12 (16.0) | |||
| Fingolimod | 17 (17.9) | 16 (21.3) | |||
| Other * | 20 (21.0) | 10 (13.3) | |||
| None | 26 (27.4) | 17 (22.7) |
| Antibodies | Mean Index (SEM) | Kruskal–Wallis Test p Value | Dunn’s Multiple Comparisons Test | ||||
|---|---|---|---|---|---|---|---|
| RRMS | Progressive Types of MS (SPMS and PPMS) | HCs | RRMS-HCs | Progressive Types of MS-HCs | RRMS-Progressive Types of MS | ||
| p Value | |||||||
| anti-NR2 | 1.80 (0.26) | 2.26 (0.99) | 1.69 (0.11) | =0.10 | ns | ns | ns |
| Anti-FVIIa | Anti-FXa | Anti-PT | Anti-Thrombin | Anti-Plasmin | |
|---|---|---|---|---|---|
| Mean Index (SEM) | |||||
| MS patients | 26.70 (1.20) | 38.18 (2.50) | 9.70 (1.60) | 71.17 (6.30) | 39.54 (2.40) |
| RRMS patients | 26.46 (1.27) | 38.28 (2.76) | 9.48 (1.71) | 72.15 (7.10) | 38.22 (2.56) |
| SPMS and PPMS patients | 28.08 (3.28) | 38.19 (6.11) | 9.04 (1.71) | 66.70 (15.22) | 43.62 (6.10) |
| Laboratory Finding | Demographic and Clinical Findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Anti-FVIIa | Anti-FXa | Anti-PT | Anti-Thrombin | Anti-Plasmin | Age | Disease Duration | EDSS | MSSS | |
| Spearman Correlation Coefficient (95% Confident Interval) p Value | |||||||||
| Anti-NR2 | −0.22 (−0.41–0.01) p = 0.03 | 0.22 (0.02–0.41) p = 0.03 | −0.06 (−0.27–0.14) p = 0.54 | 0.33 (0.11–0.52) p = 0.003 | 0 (−0.20–0.21) p = 0.95 | 0.20 (−0.01–0.39) p = 0.06 | 0.12 (−0.09–0.32) p = 0.24 | 0.30 (0.10–0.48) p = 0.0028 | 0.24 (0.03–0.43) p = 0.02 |
| Gender (ref. M) | Age | EDSS | MSSS | Anti-FVIIa | Anti-FXa | Anti-PT | Anti-Thrombin | Anti-Plasmin | RRMS | Progressive Types (SPMS and PPMS) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anti-NR2 | Odds Ratio (95% CI) | ||||||||||
| 0.79 (0.23–2.88) | 1.00 (0.96–1.05) | 0.95 (0.66–1.34) | 0.93 (0.66–1.26) | 0.90 (0.81–1.0) | 1.0 (0.98–1.03) | 0.98 (0.92–1.02) | 1.00 (0.99–1.02) | 0.96 (0.92–0.99) p = 0.03 | 3.27 (0.57–61.59) | 0.33 (0.02–1.86) | |
| Gender (ref. M) | Age | EDSS | MSSS | Anti-FVIIa | Anti-FXa | Anti-PT | Anti-Thrombin | Anti-Plasmin | |
|---|---|---|---|---|---|---|---|---|---|
| Anti-NR2 | Odds Ratio (95% CI) | ||||||||
| 0.67 (0.18–2.56) | 1.00 (0.96–1.06) | 0.95 (0.60–1.41) | 0.87 (0.58–1.21) | 0.91 (0.80–1.0) | 1.01 (0.98–1.03) | 0.98 (0.92–1.03) | 1.0 (0.99–1.02) | 0.97 (0.93–1.00) | |
| Antibodies | Mean Index (SEM) | Kruskal–Wallis Test p Value | Dunn’s Multiple Comparisons Test | ||||
|---|---|---|---|---|---|---|---|
| Non-Medication | Medication | HCs | Non-Medication-HCs | Non-Medication-Medication | Medication-HCs | ||
| p Value | |||||||
| anti-NR2 | 2.12 (0.62) | 1.78 (0.29) | 1.68 (0.11) | =0.07 | ns | ns | ns |
| Antibodies | Mean Index (SEM) | Kruskal–Wallis Test p Value | Dunn’s Multiple Comparisons Test | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-Medication | IM Medication | IS Medication | HCs | Non-Medication-IM | Non-Medication-IS | IM-IS Medication | IM-HCs | IS-HCs | ||
| p Value | ||||||||||
| anti-NR2 | 2.12 (0.62) | 1.76 (0.37) | 1.77 (0.44) | 1.68 (0.11) | =0.06 | ns | ns | ns | ns | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hadjiagapiou, M.S.; Krashias, G.; Christodoulou, C.; Pantzaris, M.; Lambrianides, A. Serum Reactive Antibodies against the N-Methyl-D-Aspartate Receptor NR2 Subunit—Could They Act as Potential Biomarkers? Int. J. Mol. Sci. 2023, 24, 16170. https://doi.org/10.3390/ijms242216170
Hadjiagapiou MS, Krashias G, Christodoulou C, Pantzaris M, Lambrianides A. Serum Reactive Antibodies against the N-Methyl-D-Aspartate Receptor NR2 Subunit—Could They Act as Potential Biomarkers? International Journal of Molecular Sciences. 2023; 24(22):16170. https://doi.org/10.3390/ijms242216170
Chicago/Turabian StyleHadjiagapiou, Maria S., George Krashias, Christina Christodoulou, Marios Pantzaris, and Anastasia Lambrianides. 2023. "Serum Reactive Antibodies against the N-Methyl-D-Aspartate Receptor NR2 Subunit—Could They Act as Potential Biomarkers?" International Journal of Molecular Sciences 24, no. 22: 16170. https://doi.org/10.3390/ijms242216170