
Ozonated Oil in Liposome Eyedrops Reduces the Formation of Biofilm, Selection of Antibiotic-Resistant Bacteria, and Adhesion of Bacteria to Human Corneal Cells
 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Results
2.1. Antimicrobial Activity
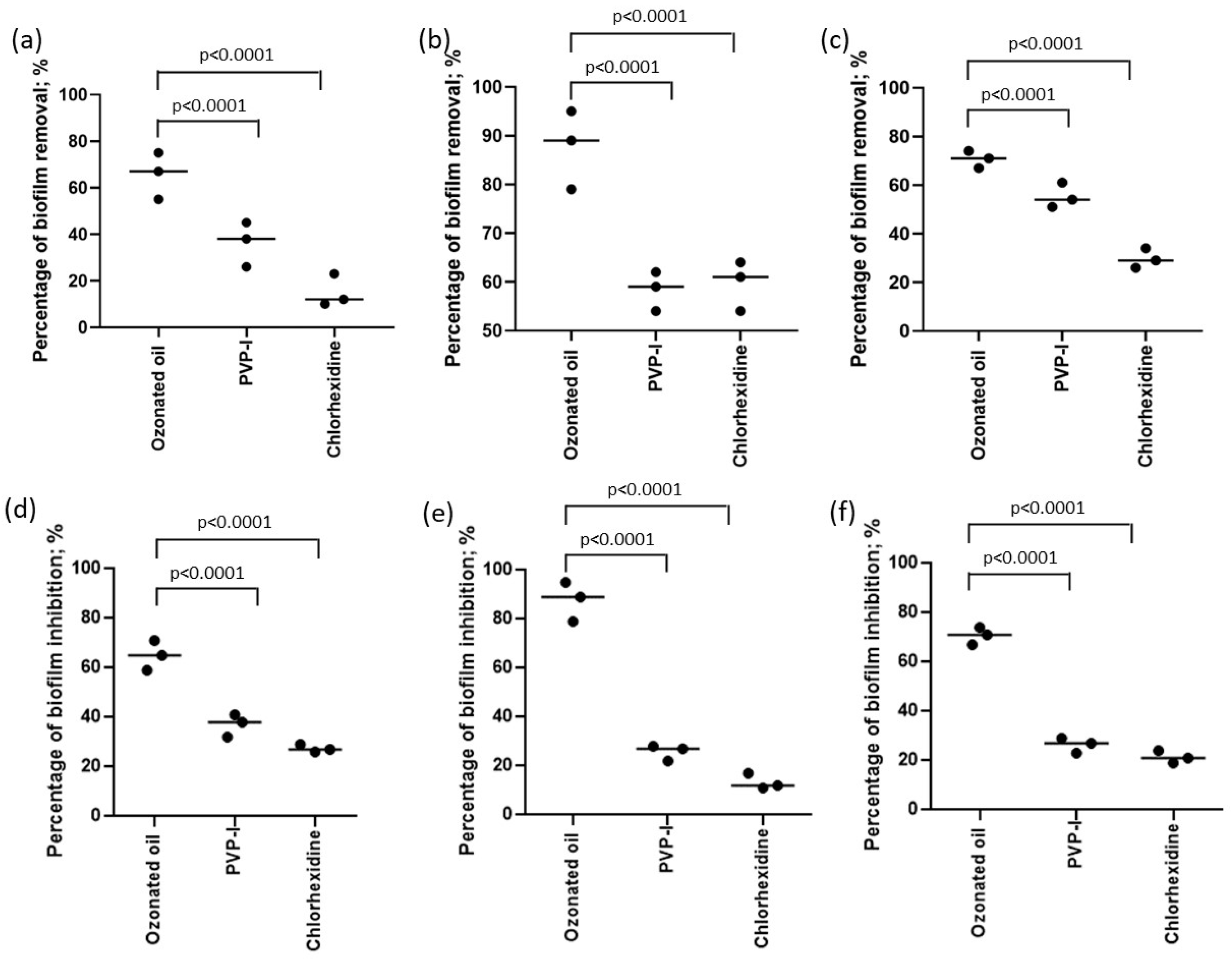
2.2. Antibiofilm Activity
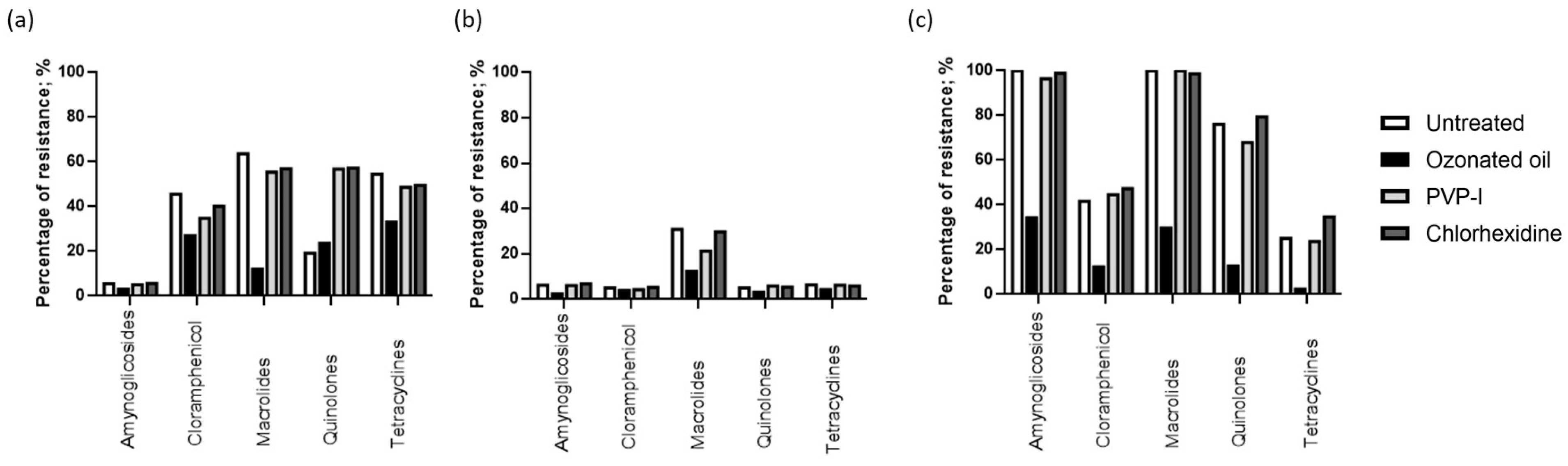
2.3. Antibiotic Resistance Evaluation
2.4. Bacteria Adhesion Test
2.5. Ophthalmologic Solution Resistance Evaluation
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Activity
4.2. Antibiofilm Effect of Using Crystal Violet (CV) Assay
4.2.1. Effect on Biofilm Formation Ability
4.2.2. Effect on Established Biofilms
4.2.3. Assessment of Biofilm Biomass
4.3. Antibiotic Susceptibility Test
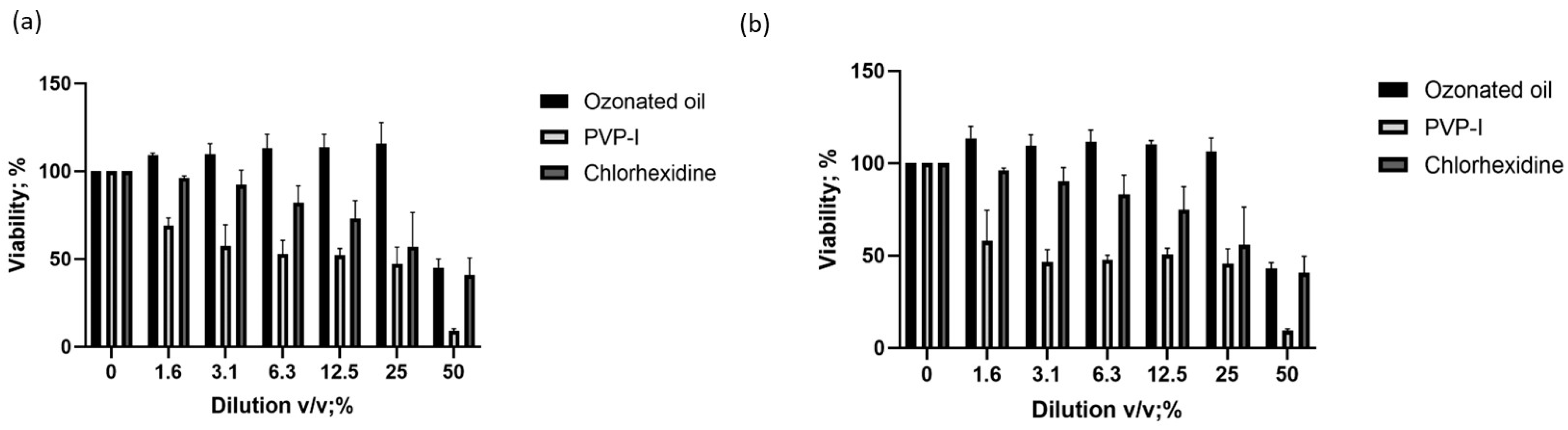
4.4. Cytotoxicity Assay
4.5. Neutral Red Uptake (NRU) Assay
4.6. Bacteria Adhesion Test
4.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, A.E.; Niruttan, K.; Rawson, T.M.; Moore, L.S.P. Antibacterial Resistance in Ophthalmic Infections: A Multi-Centre Analysis Across UK Care Settings. BMC Infect. Dis. 2019, 19, 768. [Google Scholar] [CrossRef]
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial Resistance. JAMA 2016, 316, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Haas, W.; Pillar, C.M.; Torres, M.; Morris, T.W.; Sahm, D.F. Monitoring Antibiotic Resistance in Ocular Microorganisms: Results From the Antibiotic Resistance Monitoring in Ocular micRorganisms (ARMOR) 2009 Surveillance Study. Am. J. Ophthalmol. 2011, 152, 567–574.e3. [Google Scholar] [CrossRef] [PubMed]
- Asbell, P.A.; Sahm, D.F.; Shaw, M.; Draghi, D.C.; Brown, N.P. Increasing Prevalence of Methicillin Resistance in Serious Ocular Infections Caused by Staphylococcus Aureus in the United States: 2000 to 2005. J. Cataract Refract. Surg. 2008, 34, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Getahun, E.; Gelaw, B.; Assefa, A.; Assefa, Y.; Amsalu, A. Bacterial Pathogens Associated with External Ocular Infections Alongside Eminent Proportion of Multidrug Resistant Isolates at the University of Gondar Hospital, Northwest Ethiopia. BMC Ophthalmol. 2017, 17, 151. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sanfilippo, C.M.; Pillar, C.M.; DeCory, H.H.; Sahm, D.F.; Morris, T.W. Antibiotic Resistance Among Ocular Pathogens in the United States: Five-Year Results From the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) Surveillance Study. JAMA Ophthalmol. 2015, 133, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, R.P.; Dhaliwal, D.K. Ocular Bacterial Infections: Current and Future Treatment Options. Expert Rev. Anti Infect. Ther. 2014, 3, 131–139. [Google Scholar] [CrossRef]
- Marangon, F.B.; Miller, D.; Muallem, M.S.; Romano, A.C.; Alfonso, E.C. Ciprofloxacin and Levofloxacin Resistance Among Methicillin-sensitive Staphylococcus Aureus Isolates From Keratitis and Conjunctivitis. Am. J. Ophthalmol. 2004, 137, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Grzybowski, A.; Kanclerz, P.; Myers, W.G. The Use of Povidone-iodine in Ophthalmology. Curr. Opin. Ophthalmol. 2018, 29, 19–32. [Google Scholar] [CrossRef]
- Merani, R.; McPherson, Z.E.; Luckie, A.P.; Gilhotra, J.S.; Runciman, J.; Durkin, S.; Muecke, J.; Donaldson, M.; Aralar, A.; Rao, A.; et al. Aqueous Chlorhexidine for Intravitreal Injection Antisepsis: A Case Series and Review of the Literature. Ophthalmology 2016, 123, 2588–2594. [Google Scholar] [CrossRef] [PubMed]
- Lachapelle, J.-M.; Castel, O.; Casado, A.F.; Leroy, B.; Micali, G.; Tennstedt, D.; Lambert, J. Therapeutic Perspective Antiseptics in the Era of Bacterial Resistance: A Focus on Povidone Iodine. Clin. Pract. 2013, 10, 579–592. [Google Scholar] [CrossRef]
- Kunisada, T.; Yamada, K.; Oda, S.; Hara, O. Investigation on the Efficacy of Povidone-iodine Against Antiseptic-resistant Species. Dermatology 1997, 195 (Suppl. S2), 14–18. [Google Scholar] [CrossRef]
- Kawana, R.; Kitamura, T.; Nakagomi, O.; Matsumoto, I.; Arita, M.; Yoshihara, N.; Yanagi, K.; Yamada, A.; Morita, O.; Yoshida, Y.; et al. Inactivation of Human Viruses by Povidone-iodine in Comparison with Other Antiseptics. Dermatology 1997, 195 (Suppl. S2), 29–35. [Google Scholar] [CrossRef]
- Wutzler, P.; Sauerbrei, A.; Klöcking, R.; Brögmann, B.; Reimer, K. Virucidal Activity and Cytotoxicity of The Liposomal Formulation of Povidone-Iodine. Antiviral Res. 2002, 54, 89–97. [Google Scholar] [CrossRef]
- Hoekstra, M.J.; Westgate, S.J.; Mueller, S. Povidone-iodine Ointment Demonstrates In Vitro Efficacy Against Biofilm Formation. Int. Wound J. 2017, 14, 172–179. [Google Scholar] [CrossRef]
- Capriotti, K.; Pelletier, J.; Barone, S.; Capriotti, J. Efficacy of Dilute Povidone-Iodine against Multi- Drug Resistant Bacterial Biofilms, Fungal Biofilms and Fungal Spores. J. Clin. Res. Dermatol. 2018, 5, 1–5. [Google Scholar] [CrossRef]
- Lim, K.S.; Kam, P.C.A. Chlorhexidine--Pharmacology and Clinical Applications. Anaesth. Intensive Care 2008, 36, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Burstein, N.L. Preservative Cytotoxic Threshold for Benzalkonium Chloride and Chlorhexidine Digluconate in Cat and Rabbit Corneas. Investig. Ophthalmol. Vis. Sci. 1980, 19, 308–313. [Google Scholar]
- Oakley, C.; Allen, P.; Hooshmand, J.; Vote, B.J.T. Pain and Antisepsis After Ocular Administration of Povidone-iodine versus Chlorhexidine. Retina 2018, 38, 2064–2066. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Yu, J.M.; Ko, J.H. Analysis of Ethanol Effects on Corneal Epithelium. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3852–3856. [Google Scholar] [CrossRef] [PubMed]
- Naor, J.; Savion, N.; Blumenthal, M.; Assia, E.I. Corneal Endothelial Cytotoxicity of Diluted Povidone--iodine. J. Cataract Refract. Surg. 2001, 27, 941–947. [Google Scholar] [CrossRef]
- Artasensi, A.; Mazzotta, S.; Fumagalli, L. Back to Basics: Choosing the Appropriate Surface Disinfectant. Antibiotics 2021, 10, 613. [Google Scholar] [CrossRef] [PubMed]
- Celenza, G.; Iorio, R.; Cracchiolo, S.; Petricca, S.; Costagliola, C.; Cinque, B.; Segatore, B.; Amicosante, G.; Bellio, P. Antimycotic Activity of Ozonized Oil in Liposome Eye Drops against Candida spp. Transl. Vis. Sci. Technol. 2020, 9, 4. [Google Scholar] [CrossRef]
- Kalinowski, J.; Heinonen, P.; Kilpeläinen, I.; Räsänen, M.; Gerber, R.B. Stability of criegee intermediates formed by ozonolysis of different double bonds. J. Phys. Chem. A 2015, 119, 2318–2325. [Google Scholar] [CrossRef] [PubMed]
- Ugazio, E.; Tullio, V.; Binello, A.; Tagliapietra, S.; Dosio, F. Ozonated Oils as Antimicrobial Systems in Topical Applications. Their Characterization, Current Applications, and Advances in Improved Delivery Techniques. Molecules 2020, 25, 334. [Google Scholar] [CrossRef]
- Zeng, J.; Lu, J. Mechanisms of Action Involved in Ozone-Therapy in Skin Diseases. Int. Immunopharmacol. 2018, 56, 235–241. [Google Scholar] [CrossRef]
- Menéndez, S.; Falcón, L.; Maqueira, Y. Therapeutic Efficacy of Topical OLEOZON® in Patients Suffering from Onychomycosis. Mycoses 2011, 54, e272–e277. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, S.; Falcón, L.; Simón, D.R.; Landa, N. Efficacy of Ozonized Sunflower Oil in The Treatment of Tinea Pedis. Mycoses 2002, 45, 329–332. [Google Scholar] [CrossRef]
- Guerra-Blanco, P.; Poznyak, T.; Pérez, A.; Gómez y Gómez, Y.M.; Bautista-Ramírez, M.E.; Chairez, I. Ozonation Degree of Vegetable Oils as the Factor of Their Anti-Inflammatory and Wound-Healing Effectiveness. Ozone Sci. Eng. 2017, 39, 374–384. [Google Scholar] [CrossRef]
- Zerillo, L.; Polvere, I.; Varricchio, R.; Madera, J.R.; D’Andrea, S.; Voccola, S.; Franchini, I.; Stilo, R.; Vito, P.; Zotti, T. Antibiofilm and repair activity of ozonated oil in liposome. Microb. Biotechnol. 2022, 15, 1422–1433. [Google Scholar] [CrossRef]
- Cutarelli, A.; Carlini, G.; Sarno, F.; Nebbioso, A.; Garofalo, F.; Altucci, L.; Corrado, F.; Cutarelli, A.; Carlini, G.; Sarno, F.; et al. The Role of Ozone Carried by Liposomes in the Therapy of Infectious and Skin-Regenerating Ocular Surface. J. Biomed. Sci. Eng. 2019, 12, 347–353. [Google Scholar] [CrossRef]
- Pérez-Santonja, J.J.; Güell, J.L.; Gris, O.; Dorrego, X.M.V.; Pellicer, E.; Benítez-Del-castillo, J.M. Liposomal Ozonated Oil in Ocular Infections: A Review of Preclinical and Clinical Studies, Focusing on Its Antiseptic and Regenerative Properties. Clin. Ophthalmol. 2022, 16, 1953–1962. [Google Scholar] [CrossRef] [PubMed]
- EUCAST. MIC Determination of Non-fastidious and Fastidious Organisms. Available online: https://www.eucast.org/ast_of_bacteria/mic_determination (accessed on 22 July 2023).
- Khatoon, Z.; McTiernan, C.D.; Suuronen, E.J.; Mah, T.F.; Alarcon, E.I. Bacterial biofilm formation on implantable devices and approaches to its treatment and prevention. Heliyon 2018, 4, e01067. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.P.; Perez, N.; Lozano, C.M.S.; Altube, M.J.; de Farias, M.A.; Portugal, R.V.; Buzzola, F.; Morilla, M.J.; Romero, E.L. The anti MRSA biofilm activity of Thymus vulgaris essential oil in nanovesicles. Phytomedicine 2019, 57, 339–351. [Google Scholar] [CrossRef]
- Bispo, P.J.M.; Sahm, D.F.; Asbell, P.A. A Systematic Review of Multi-decade Antibiotic Resistance Data for Ocular Bacterial Pathogens in the United States. Ophthalmol. Ther. 2022, 11, 503. [Google Scholar] [CrossRef]
- Kline, K.A.; Fälker, S.; Dahlberg, S.; Normark, S.; Henriques-Normark, B. Bacterial Adhesins in Host-Microbe Interactions. Cell Host Microbe 2009, 5, 580–592. [Google Scholar] [CrossRef]
- Tognetto, D.; Pastore, M.R.; Guerin, G.M.; Decorti, G.; Franzin, M.; Lagatolla, C.; Cirigliano, G. Bactericidal Activity of Three Different Antiseptic Ophthalmic Preparations as Surgical Prophylaxis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 289–293. [Google Scholar] [CrossRef]
- Wang, Y. Liposome as a delivery system for the treatment of biofilm-mediated infections. J. Appl. Microbiol. 2021, 131, 2626–2639. [Google Scholar] [CrossRef]
- Marchegiani, A.; Magagnini, M.; Cerquetella, M.; Troiano, P.; Franchini, I.; Franchini, A.; Scapagnini, G.; Spaterna, A. Preoperative topical liposomal ozone dispersion to reduce bacterial colonization in conjunctival sac and periocular skin: Preliminary study in dogs. Exp. Eye Res. 2019, 189, 107848. [Google Scholar] [CrossRef] [PubMed]
- Spadea, L.; Tonti, E.; Spaterna, A.; Marchegiani, A. Use of Ozone-Based Eye Drops: A Series of Cases in Veterinary and Human Spontaneous Ocular Pathologies. Case Rep. Ophthalmol. 2018, 9, 287–298. [Google Scholar] [CrossRef]
- Díaz, M.F.; Hernández, R.; Martínez, G.; Vidal, G.; Gómez, M.; Fernández, H.; Garcés, R. Comparative study of ozonized olive oil and ozonized sunflower oil. J. Braz. Chem. Soc. 2006, 17, 403–407. [Google Scholar] [CrossRef]
- Silva, V.; Peirone, C.; Amaral, J.S.; Capita, R.; Alonso-Calleja, C.; Marques-Magallanes, J.A.; Martins, Â.; Carvalho, Á.; Maltez, L.; Pereira, J.E.; et al. High Efficacy of Ozonated Oils on the Removal of Biofilms Produced by Methicillin-Resistant Staphylococcus aureus (MRSA) from Infected Diabetic Foot Ulcers. Molecules 2020, 25, 3601. [Google Scholar] [CrossRef] [PubMed]
- Letourneau, J.; Levesque, C.; Berthiaume, F.; Jacques, M.; Mourez, M. In Vitro Assay of Bacterial Adhesion onto Mammalian Epithelial Cells. J. Vis. Exp. 2011, 51, e2783. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Bacterial Strain | Ozonated Oil Ophthalmic Solution | PVP-I Ophthalmic Solution | Chlorhexidine Ophthalmic Solution |
|---|---|---|---|
| E. coli (ATCC 8739) | 25% | 100% | 100% |
| P. aeruginosa (ATCC 9027) | 50% | 100% | 100% |
| S. aureus (ATCC 6538) | 12.5% | 50% | 12.5% |
| MRSA (ATCC 33591) | 25% | 50% | 25% |
| S. epidermidis (ATCC 12228) | 12.5% | 50% | 12.5% |
| Antibiotics | P. aeruginosa (ATCC 9027) | S. aureus (ATCC 6538) | MRSA (ATCC 33591) |
|---|---|---|---|
| Aminoglycosides (gentamycin, tobramycin, neomycin) | 5.5% | 6.2% | 100.0% |
| Chloramphenicol | 45.5% | 5.0% | 41.7% |
| Macrolides (azithromycin, erythromycin) | 63.6% | 30.8% | 100.0% |
| Quinolones (ciprofloxacin, moxifloxacin, besifloxacin, gatifloxacin, levofloxacin, ofloxacin) | 19.2% | 5.0% | 76.0% |
| Tetracyclines | 54.5% | 6.4% | 25.0% |
| Ophthalmic Solution | P. aeruginosa (ATCC 9027) (CFU) | S. aureus (ATCC 6538) (CFU) | MRSA (ATCC 33591) (CFU) |
|---|---|---|---|
| Ozonated sunflower oil | 1.7 × 103 | 2.1 × 103 | 1.9 × 103 |
| PVP-I | 5.5 × 104 | 4.6 × 104 | 5.1 × 104 |
| Chlorhexidine | 3.2 × 104 | 2.2 × 104 | 5.2 × 104 |
| Bacterial Strain | Ozonated Oil Ophthalmic Solution | PVP-I Ophthalmic Solution | Chlorhexidine Ophthalmic Solution |
|---|---|---|---|
| E. coli (ATCC 8739) | 25% | 100% | 100% |
| P. aeruginosa (ATCC 9027) | 50% | 100% | 100% |
| S. aureus (ATCC 6538) | 12.5% | 50% | 12.5% |
| MRSA (ATCC 33591) | 25% | 50% | 25% |
| S. epidermidis (ATCC 12228) | 12.5% | 50% | 12.5% |
| Solutions | P. aeruginosa (ATCC 9027) | S. aureus (ATCC 6538) |
|---|---|---|
| LB | 5.7 × 104 | 5.5 × 104 |
| LB + 1% Triton X-100 | 5.8 × 104 | 5.6 × 104 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gentili, V.; Strazzabosco, G.; Salgari, N.; Mancini, A.; Rizzo, S.; Beltrami, S.; Schiuma, G.; Casciano, F.; Alogna, A.; Passarella, D.; et al. Ozonated Oil in Liposome Eyedrops Reduces the Formation of Biofilm, Selection of Antibiotic-Resistant Bacteria, and Adhesion of Bacteria to Human Corneal Cells. Int. J. Mol. Sci. 2023, 24, 14078. https://doi.org/10.3390/ijms241814078
Gentili V, Strazzabosco G, Salgari N, Mancini A, Rizzo S, Beltrami S, Schiuma G, Casciano F, Alogna A, Passarella D, et al. Ozonated Oil in Liposome Eyedrops Reduces the Formation of Biofilm, Selection of Antibiotic-Resistant Bacteria, and Adhesion of Bacteria to Human Corneal Cells. International Journal of Molecular Sciences. 2023; 24(18):14078. https://doi.org/10.3390/ijms241814078
Chicago/Turabian StyleGentili, Valentina, Giovanni Strazzabosco, Niccolò Salgari, Alessandra Mancini, Sabrina Rizzo, Silvia Beltrami, Giovanna Schiuma, Fabio Casciano, Andrea Alogna, Daniela Passarella, and et al. 2023. "Ozonated Oil in Liposome Eyedrops Reduces the Formation of Biofilm, Selection of Antibiotic-Resistant Bacteria, and Adhesion of Bacteria to Human Corneal Cells" International Journal of Molecular Sciences 24, no. 18: 14078. https://doi.org/10.3390/ijms241814078