1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is considered a modern pandemic affecting more than 25% of the general population worldwide [
1]. Its prevalence is constantly rising in parallel with the prevalence of οbesity and metabolic syndrome (MetS). NAFLD is considered the hepatic component of the latter. The spectrum of the disease includes non-alcoholic fatty liver (NAFL), which is characterized by steatosis with or without mild inflammation, and the more progressive non-alcoholic steatohepatitis (NASH), which is characterized by the coexistence of steatosis, inflammation, and hepatocellular ballooning [
1,
2] with or without fibrosis.
Regarding the prognosis of the disease, the most important prognostic indicator is the presence of advanced fibrosis. Steatohepatitis seems to be an important driver for the progression of more advanced stages of fibrosis. It has been demonstrated that patients with NAFL progress by one stage of fibrosis on average every 14 years, while patients with NASH show faster disease progression of one fibrosis stage every 7 years. It is evident that the early diagnosis of NASH is clinically important, as it can prompt early interventions in the disease course, leading to a subsequent reduction in morbidity and mortality in a significant part of the general population [
3,
4]. Even though there are reliable non-invasive modalities to assess liver fibrosis, there are currently no non-invasive modalities to assess for the presence and grade of NASH. Transient elastography and several non-invasive serological tests (NITs), such as FIB-4 and NAFLD fibrosis score, can rule out or rule in clinically significant liver fibrosis with high sensitivity and specificity [
5,
6]. On the other hand, the diagnosis of NASH can only be made histologically with a liver biopsy. The limitations of liver biopsy include increased costs (due to the need for hospitalization and follow-up) and a small risk of life-threatening complications. It is evident that there is an increasing need for a reliable non-invasive diagnostic biomarker for NASH.
It has been recently proposed that plasma lipids may have a role in the non-invasive diagnosis of NASH [
7,
8]. Recent studies found notable alterations in lipid composition in liver biopsies of patients with NAFLD (such as phospholipids, fatty acids, and sphingolipids), indicating that disturbances in the metabolism of specific lipid species could be a potential contributor to the pathogenesis of NAFLD/NASH. Puri et al. [
7] assessed hepatic lipid composition in 27 liver biopsies and found that NAFLD is associated with alterations in the hepatic lipid profile. Moreover, changes in the circulating plasma lipid species might also be associated with disease progression. Apostolopoulou et al. [
9] conducted a prospective study including bariatric patients. They analysed liver, serum, and adipose tissue ceramides and found that sphingolipid levels were higher in patients with insulin resistance and NASH, and their levels correlated with the degree of hepatic inflammation and oxidative stress. A small number of further lipidomic studies have been performed in recent years [
10,
11,
12,
13,
14,
15,
16] with important methodological limitations. Most of these studies included morbidly obese/bariatric patients and often heterogeneous populations. The majority of these studies examined only hepatic and not plasma lipids, which potentially could be used for the non-invasive diagnosis of NASH. Finally, the studies that examined both plasma and hepatic lipids showed inconsistency between measured parameters.
The aim of our study was to investigate potential differences in plasma lipids in patients with NASH, NAFL, and healthy controls that may help differentiate NASH from NAFL and non-invasively assess the histological activity of the disease. To achieve this goal, we applied multitargeted analyses by liquid chromatography–mass spectrometry (LC–MS) and gas chromatography–mass spectrometry (GC–MS) for the quantification of plasma fatty acids, acylcarnitines, and ceramides. Moreover, state-of-the-art statistical machine learning methods were used for the analysis of the data.
3. Discussion
The non-invasive diagnosis of NASH remains a clinical challenge, as there is currently no available biomarker that can discriminate NASH from NAFL. The diagnosis of NASH can only be made histologically. However, the large number of NAFLD patients and the invasive nature of liver biopsy render this approach problematic. The aim of this study was to characterize lipid profiles (plasma fatty acids, acylcarnitines, and ceramides) in patients with NASH and NAFL and to investigate potential correlations with histological activity and fibrosis.
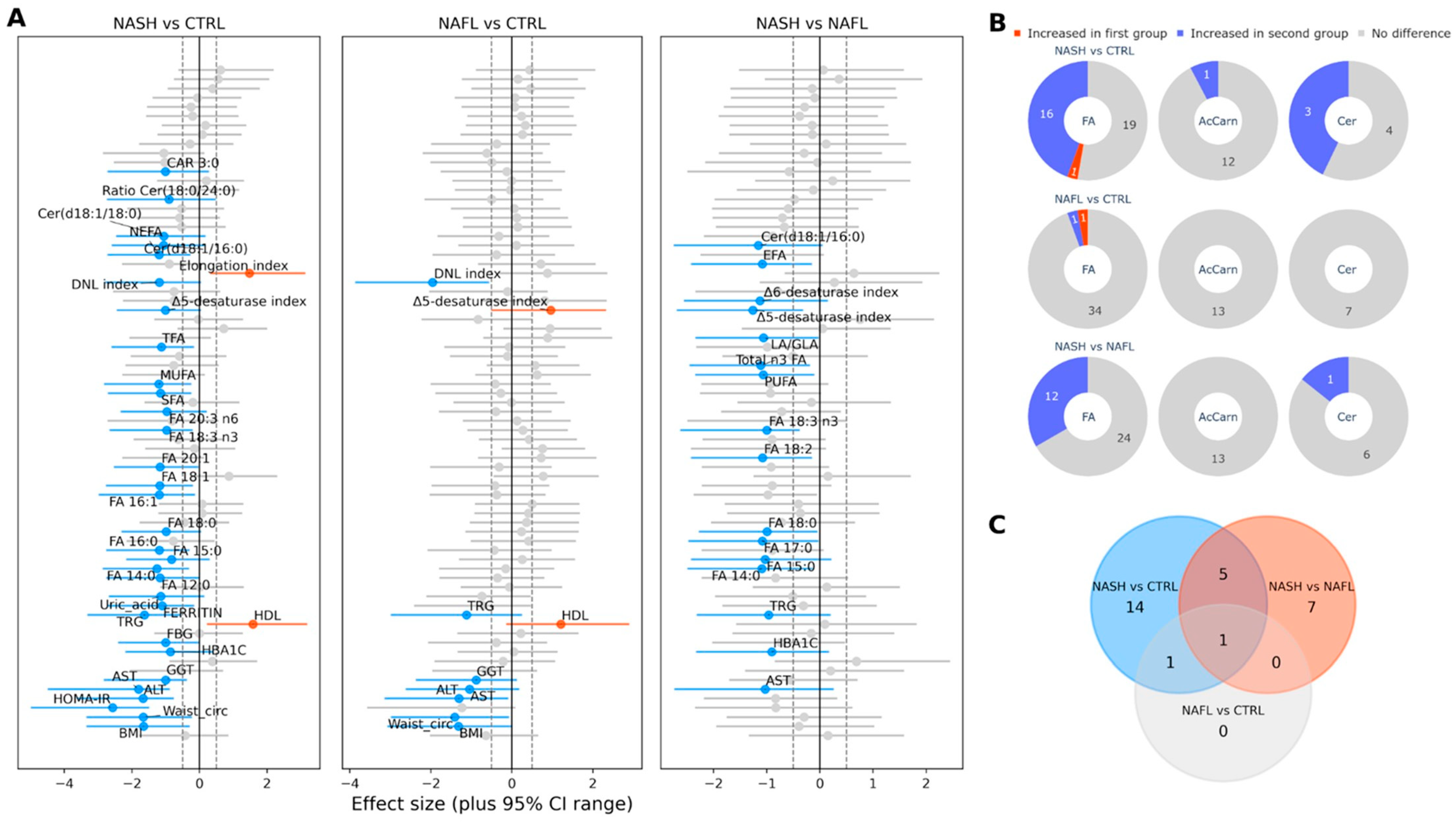
Patients were classified as having NASH or NAFL based on liver histology. Patients with NAFL and NASH had similar metabolic profiles, but had more metabolic risk factors compared to controls, as expected. A major finding of our study is that patients with NASH had a distinctive plasma lipid profile from patients with NAFL, although the two groups did not differ in terms of established metabolic risk factors. In addition, patients with NAFL and healthy controls had similar plasma lipid profiles, even though the former had significantly more metabolic risk factors.
Patients with NASH had significant differences in the values of several species of fatty acids, such as FA 12:0, FA 14:0, FA 15:0, FA 16:1, FA 17:0, FA 18:0, FA 18:3n3, FA 18:2, the LA/GLA ratio, EFA, TFA, SFA, total n3-FAs, and others, compared to NAFL patients and healthy controls. These results indicate that specific lipotoxic fatty acids, mainly saturated fatty acids, may play a role in the pathogenesis of NASH. The intrahepatic accumulation of saturated fatty acids probably induces oxidative stress and activates the inflammasome in the liver, resulting in hepatocyte injury and apoptosis [
18]. Given the fact that the samples in our study were taken after an overnight fasting, it is unlikely that this finding is an effect of dietary intake, but it probably is a result of increased DNL and increased peripheral lipolysis (due to insulin resistance). The fact that the products of DNL are exclusively saturated fatty acids further supports this rationale. This trend was also demonstrated in a previous study carried out by Puri et al. [
19], although this study had important methodological limitations, such as differences between the study groups. Similar findings were also observed in a study conducted by Walle et al. [
16], which found increased serum concentrations of saturated fatty acids, mainly FA 14:0, FA16:0, and FA 18:0, in patients with NASH compared to patients with NAFL. Another study that was conducted by Luukonen et al. [
12] showed increased levels of saturated fatty acids in the livers of adults with NASH. Similar results have also been found in recent animal studies [
20]. The existence of a genetic predisposition probably contributes to these findings. This was seen in a previous study conducted by our group, which concluded that the
rs738409 polymorphism of the
PNPLA3 gene affects the composition of the blood fatty acids [
21]. This polymorphism resulted in increased concentrations of blood saturated fatty acids such as palmitic, stearic, oleic, and linoleic acids, the values of which were found to be significantly elevated in NASH patients in our study. In contrast to previous lipidomic studies, the levels of PUFA in our study were increased [
8,
19].
Regarding ceramides, in our study, Cer(d18:1/16:0) levels were significantly increased in NASH patients compared to NAFL patients and healthy controls, and Cer(d18:1/18:0) levels and the Cer(d18:1/18:0)/Cer(d18:1/24:0) ratio were significantly higher in NASH patients compared to healthy controls. Increased concentrations of C 16:0 ceramide were also observed both in recent animal studies [
22,
23], which found that this specific ceramide’s concentrations were increased in obesity-related insulin resistance, and in a human study carried out by Luukonen et al. [
12] in patients with NASH and insulin resistance. These findings indicate that the “de novo” ceramide synthesis pathway is probably upregulated in NASH. Ceramides are bioactive molecules that play an important role in many cellular functions and have been associated with insulin resistance, altered insulin signaling, as well as inflammatory and apoptotic processes [
24]. These lipotoxic intermediates are considered important mediators in hepatocellular injury in NASH.
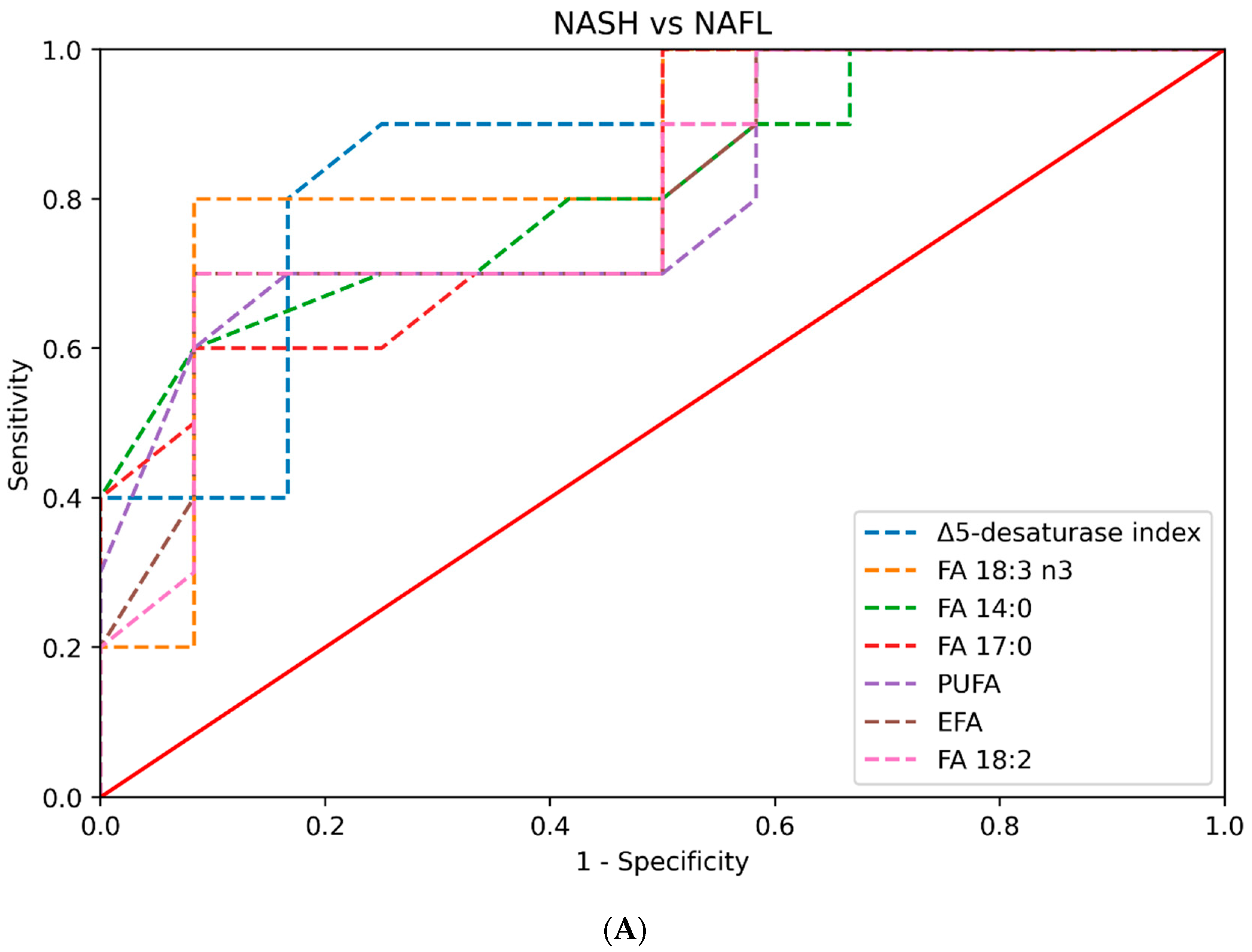
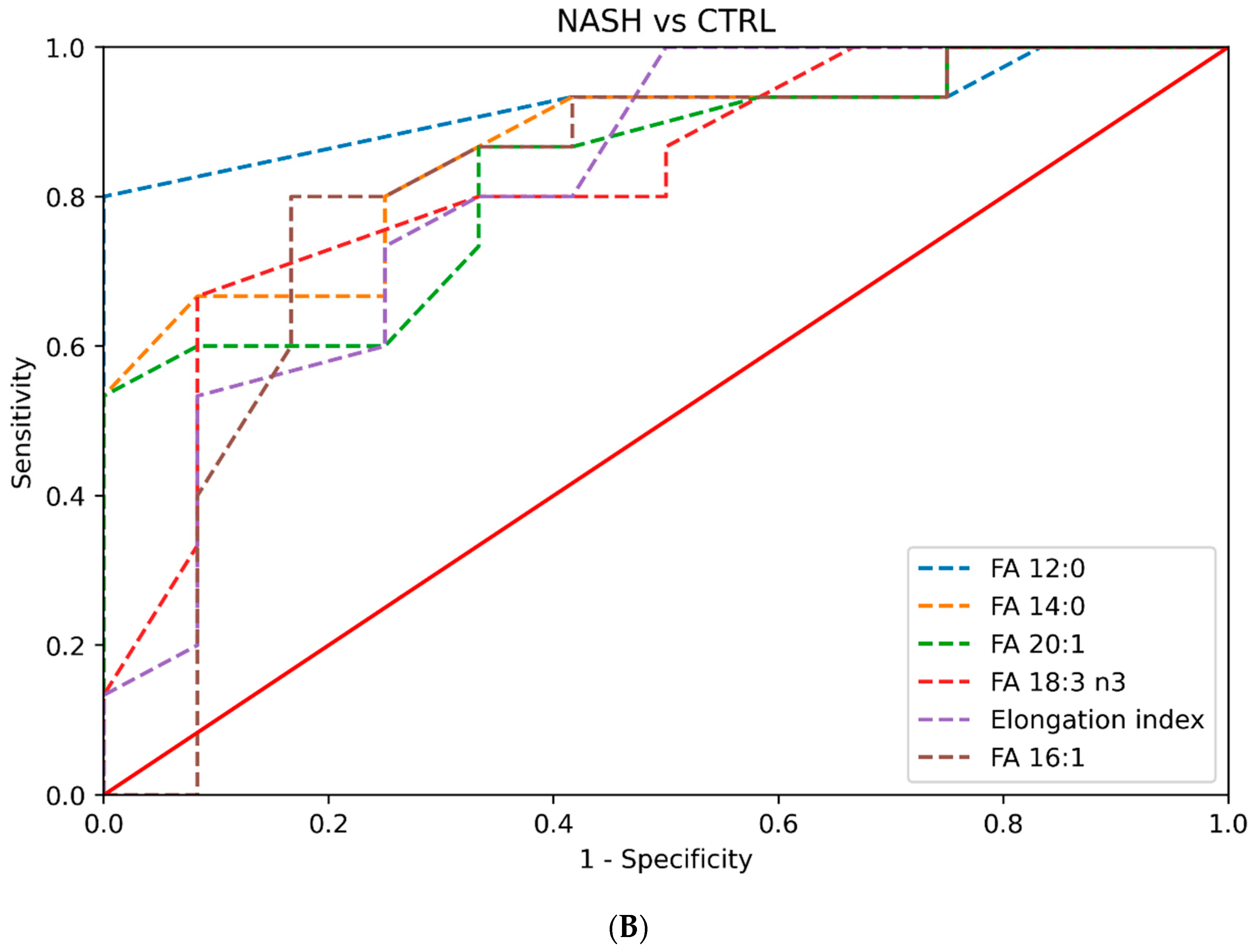
Another important finding of our study is the association between several fatty acid levels and histological activity, as assessed using the NAS score. In addition, several lipids, such as Δ5-desaturase index, FA 14:0, FA 17:0, FA 18:2, FA 18:3 n3, and PUFA, exhibit high accuracy in discriminating NASH from NAFL. This suggests that the plasma lipid profile might prove a useful tool in the non-invasive diagnosis of NASH. In contrast, the plasma lipid profile did not correlate with the fibrosis stage, except for fatty acid FA 12:0. However, safe conclusions could not be drawn due to the relatively small sample size of our study.
Several previous lipidomic/metabolomic studies attempted to further investigate the complex pathophysiology of NAFLD [
7,
8,
9,
10,
11,
12,
13,
14,
15]. These studies yielded encouraging results regarding the different qualitative and quantitative hepatic lipid compositions in NAFLD patients in comparison to healthy subjects. However, most of these studies had several limitations. Most of these studies included morbidly obese patients undergoing bariatric surgery, which raises concerns as to the effect that extreme BMI levels might have on the circulating plasma lipidomic footprint [
7,
9,
12,
13,
14,
15]. Moreover, the absence of steatosis was confirmed histologically in some of the studies, whereas others relied on the combination of normal liver ultrasound scans and normal liver biochemistry. Ultrasonography has the limitation that it can detect hepatic steatosis when at least 20–30% of the liver parenchyma is affected [
25]. In addition, performing a liver biopsy in a patient with a normal liver raises bioethical issues when there is an equivalent, safe, and accurate non-invasive way to assess for hepatic steatosis, such as MRI-PDFF, which was used in our study [
26,
27]. Moreover, most of the studies focused on hepatic lipid composition, which might reflect more precisely the alterations in lipid metabolism that occur in NAFLD/NASH, but liver tissue is a biological material that is not easily accessible in daily clinical practice. In the studies that examined both plasma and hepatic lipids, the results were inconsistent in plasma and liver tissue. Finally, discrepancies were found in the results between the different studies that examined plasma lipids, possibly because of the different methods used, the heterogeneity in the populations examined, and the study designs.
Our study had substantial strengths. Firstly, we included three well-characterized groups. NAFL and NASH were confirmed histologically, and the absence of steatosis was confirmed by means of MRI-PDFF. Participants were common NAFLD patients seen in hepatology clinics and not patients at extreme ends of the MetS, such as morbidly obese patients (median BMI of NAFL and NASH patients were 31.1 and 31.6 kg/m
2, respectively, and 25.3 kg/m
2 in the control group). Moreover, a subgroup analysis was performed according to the HOMA-IR, which added further to our understanding of the role of lipids in NAFLD [
28]. State-of-the-art statistical methods were also used. Regarding the methodology followed in our study for the plasma lipid profiles, it should be noted that it was specifically developed in our lab with the aim to assess dysregulated lipid profiles in clinical samples and to ensure the accurate determination of the certain lipid species.
Our study has some limitations. The relatively small number of participants is the main limitation. Another limitation is that a targeted lipidomic analysis was conducted that included lipid species that are thought to contribute to NASH pathogenesis according to currently available data. An untargeted lipidomic analysis that could identify more (all detectable) lipid species that potentially contribute to the pathogenesis of the disease could provide a more comprehensive pattern. This is the next study to be performed in these samples, and results will be soon published to build on the present data.
In summary, the results of our study indicate that NASH patients exhibit a distinct plasma lipid profile that is distinctive from NAFL patients and non-NAFLD controls. This profile seems to correlate with histological activity. Based on these results, plasma lipids may provide a useful biomarker for the diagnosis of NASH. Our findings might have significant implications, facilitating earlier diagnosis and the personalized management of NASH, leading to improved patient outcomes and reduced disease burden. The results of our study require validation in larger cohorts.
4. Materials and Methods
4.1. Study Design
The current study was a case-control study that included three well characterized groups: patients with biopsy-proven NAFL, patients with biopsy-proven NASH, and healthy controls. All participants were enrolled in our study between June 2021 and June 2023 after providing written informed consent. The study was performed according to the principles of the Declaration of Helsinki. The study was approved by the Institutional Review Board and the Bioethics Board of Medical School of Aristotle University of Thessaloniki (protocol number 4.399/26/01/2021).
4.2. Study Cohort
Consecutive adult subjects with a recent (or suspected) diagnosis of NAFLD (within 6 months) that attended the hepatology outpatient clinic at AHEPA University Hospital (Thessaloniki, Greece) during the study period were screened for eligibility after providing written informed consent. Inclusion criteria were age > 18 years and a probable diagnosis of NAFLD based on the presence of hepatic steatosis on imaging studies (ultrasound scan, CT, or MRI scan), the presence of metabolic risk factors, and the exclusion of other causes for hepatic steatosis. Exclusion criteria were alcohol consumption > 20 gr/d in women and >30 gr/day in men. Patients with concomitant liver diseases (chronic viral hepatitis, autoimmune and cholestatic liver diseases, Wilson’s disease, hemochromatosis, a-1-antitrypsin deficiency, and drug-induced liver disease) were also excluded. Finally, subjects with underlying severe systemic diseases (such as cancer and end-stage liver, kidney, and heart disease) were excluded from our study.
Healthy controls were recruited from June 2021 to June 2023. In this group, the absence of hepatic steatosis was determined by normal liver biochemistry and a liver fat fraction < 5% on MRI-PDFF [
26,
27]. All healthy controls had a complete liver screen that was negative for chronic liver diseases.
Participants had clinical assessment, physical examination, and blood tests at baseline. The anthropometric and demographic parameters that were recorded were age, gender, weigh, height, body mass index (BMI), and waist circumference (WC). Baseline biochemistry parameters included: alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGt), alkaline phosphatase (ALP), billrubin, serum albumin, total cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides, fasting blood glucose (FBG), insulin, HbA1c, and ferritin.
Patients with NAFLD, who had indications according to current clinical practice guidelines [
1,
2], underwent ultrasound-guided percutaneous liver biopsy [
1,
2]. Liver biopsies were examined by an expert liver pathologist, who was blinded to patient characteristics. The definitive diagnosis of NAFLD was established by the presence of steatosis in at least 5% of the hepatocytes. The NAFLD activity score (NAS) and fibrosis score by the NASH Clinical Research Network (CRN) were used to grade inflammatory activity and stage fibrosis, respectively [
29]. The NAS score consists of three components: steatosis (0–3), lobular inflammation (0–3), and hepatocellular ballooning (0–2), and it ranges from 0 to 8. The fibrosis score ranges from 0 (absence of fibrosis) to 4 (cirrhosis). Subjects with NAFLD were further divided into NAFL and NASH based on histological findings. Subjects with steatosis with no or mild inflammation were classified as NAFL. Subjects with at least 1 grade of each component of the NAS score were classified as NASH [
30].
Blood samples were taken from all participants for plasma lipid analysis by three different methods (in subjects with NAFLD on the morning of the liver biopsy) after overnight fasting and a low-fat diet in the past 24 h. Blood samples were centrifugated, and plasma was separated and immediately stored at −80 °C.
4.3. Acylcarnitines, Ceramides and Fatty Acids Analyses
For the analysis of acylcarnitines and ceramides, two LC-MS methods developed in our lab were applied. For acylcarnitines, an hydrophilic interaction liquid chromatography tandem mass spectrometry (HILIC–MS/MS) method was applied quantifying 13 acylcarnitine analogues, namely Acetyl-L-Carnitine (CAR 2:0); Propionyl-L-Carnitine (CAR 3:0); Butyryl-L-Carnitine (CAR 4:0); Valeryl-L-Carnitine (CAR 5:0); Hexanoyl-L-Carnitine (CAR 6:); Octanoyl-L-Carnitine (CAR 8:0); Decanoyl-L-Carnitine (CAR 10:0); Lauroyl-L-Carnitine (CAR 12:0); Myristoyl-L-Carnitine (CAR 14:0); Palmitoyl-L-Carnitine (CAR 16:0); Stearoyl-L-Carnitine (CAR 18:0); Oleoyl-L-carnitine (CAR 18:1); and Linoleoyl-L-Carnitine (CAR 18:2) [
31,
32].
For ceramides, the reverse phase LC–MS/MS method, quantifying four species, namely N-Palmitoyl-D-erythro-sphingosine (Cer d18:1/16:0); N-stearoyl-D-erythro-sphingosine (Cer d18:1/18:0); N-lignoceroyl-D-erythro-sphingosine (Cer d18:1/24:0); and N-nervonoyl-D-erythro-sphingosine (Cer d18:1/24:1), was applied [
33]. Analysis was performed on an Acquity UPLC System (Waters Corporation, Milford, CT, USA) coupled on a XEVO TQD Mass Spectrometer (Waters Corporation, Milford, CT, USA). Data acquisition and analysis were performed by Waters MassLynx version 4.1 and TargetLynx (Waters, Milford, MA 01757, USA).
Total fatty acid analysis was performed on an Agilent Technologies 8860 GC, combined with a 5977 MSD (Agilent Technologies, Santa Clara, CA, USA). Fatty acid methyl esters were separated on an Agilent 100 m HP-88 column (0.25 μm, i.d. of 0.25 μm). Data were processed by MassHunter Workstation (Version 10.0) software. Fatty acids were extracted from serum samples using a modified Folch protocol followed by methanolysis/methylation under acidic conditions, as described in our previous study [
21]. In total, 20 fatty acid methyl esters were quantified, namely Lauric (FA 12:0), Myristic (FA 14:0), Pentadecanoic (FA 15:0), Palmitic (FA 16:0), Heptadecanoic (FA 17:0), Stearic (FA 18:0), Arachidic (FA 20:0), Behenic (FA 22:0), Lignoceric (FA 24:0), Palmitoleic (FA 16:1),
cis-9-Oleic (FA 18:1),
cis-11-Eicosenoic (FA 20:1), Nervonic (FA 24:1), Linoleic (FA 18:2), Gamma Linolenic (FA 18:3n6), Alpha Linolenic (FA 18:3n3), Dihomogamma Linolenic (FA 20:3n6), Arachidonic (FA 20:4n6),
cis-5,8,11,14,17 Eicosapentaenoic (FA 20:5n3),
cis-4,7,10,13,16,19 Docosahexaenoic (FA 22:6n3) acids.
4.4. Data and Statistical Analysis
The Python (v. 3.10.6) programming language was used for statistical computations and the visualization of the results on a Linux OS based PC. The continuous variables are expressed as medians with interquartile range (IQR, 25th–75th percentile), while the categorical variables are expressed as counts and percentages for each variable’s category. The differences between the variables’ categories were examined using the Mann–Whitney U test for the continuous variables and the Chi-square (χ
2) test for the categorical variables. Receiver operating characteristic (ROC) curves were plotted, and the area under the ROC (AUROC) and the corresponding
p value were calculated to determine the diagnostic accuracy of the lipids to differentiate NASH from NAFL and CTRL. The sensitivity and the specificity for cutoffs were also calculated for specific lipids. Two-tailed
p values < 0.05 were considered to indicate statistically significant differences in variables between groups. In addition, the effect size offering valuable information about the practical significance of a finding, independent of sample size, was calculated, along with its 95% confidence interval range, as a metric to quantify the magnitude of the observed differences in the study [
34]. Cohen’s d was used as an effect size measure, which calculated the standardized mean difference between two groups by dividing the difference in means by the pooled standard deviation. Effect size values greater than 0.5 and 0.8 indicated medium and large effects, respectively. Confidence intervals were calculated using the bootstrapping method, which involves the repeated random resampling of the original dataset with the replacement [
35]. Correlations between lipids and histological features were assessed by Pearson’s correlation.
4.5. Predetermined Subgroup Analysis
A subgroup analysis was performed based on the values of the homeostasis model assessment of insulin resistance (HOMA-IR) to examine patients that were insulin-resistant and, therefore, at a higher risk of suffering from NASH. Due to the lack of a globally accepted cut-off value of HOMA-IR that can differentiate insulin-resistant from insulin-sensitive subjects, a cut-off value of 3 was used. The total study population was divided into two groups: individuals with HOMA-IR values > 3 were classified into the “High HOMA-IR” group, while individuals with HOMA-IR values < 3 were classified into the “Low HOMA-IR” group.


 ,
, 




{kind=link}
{kind=link}
{kind=link}