

Relevance of Biomarkers in Serum vs. Synovial Fluid in Patients with Knee Osteoarthritis

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
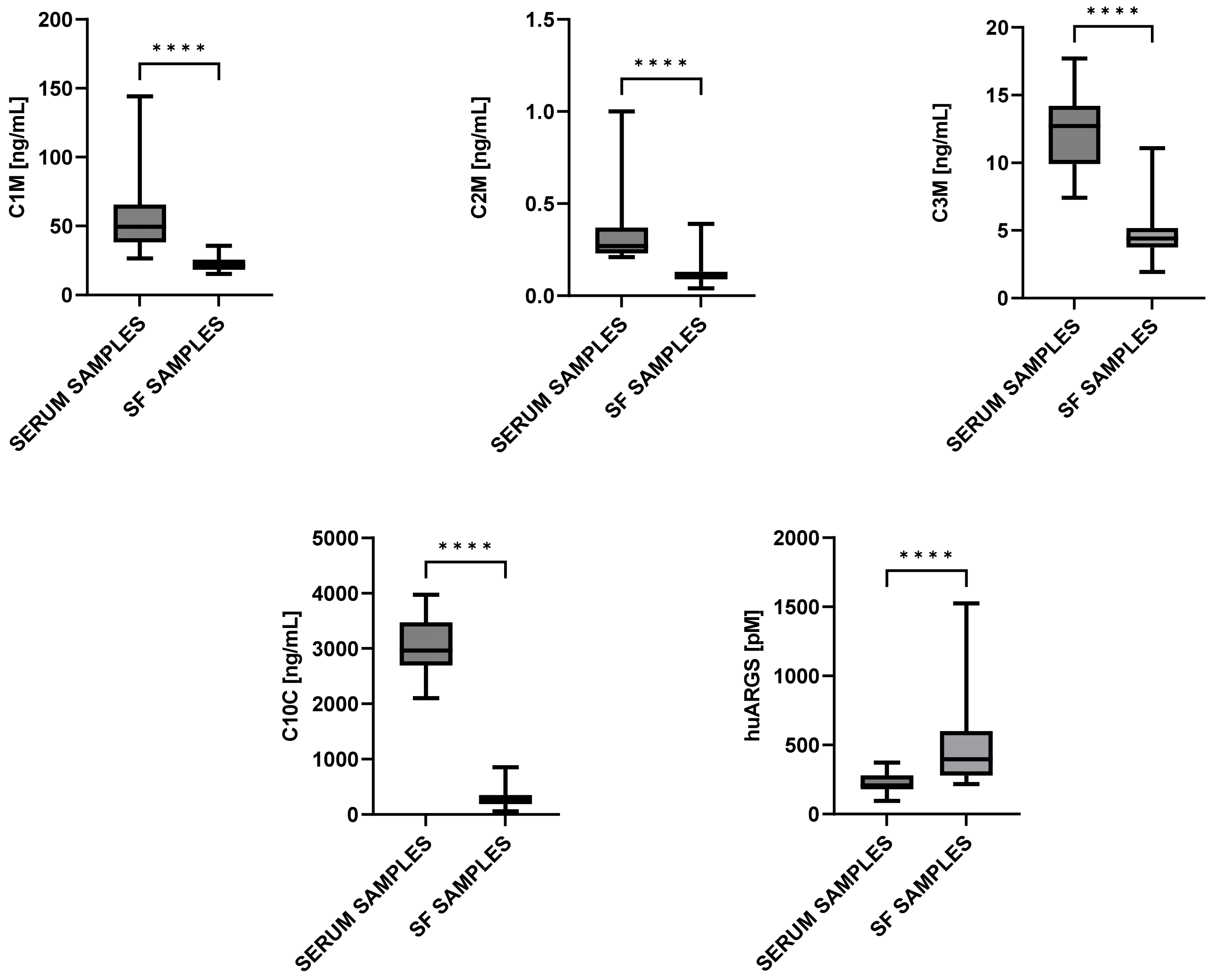
2.2. Biomarkers’ Levels in Serum and SF
2.3. Relationship between Biomarkers’ Levels and Structural Outcomes in Serum and in SF
2.4. Relationship between Biomarkers’ Levels and Pain Outcomes in Serum and in SF
3. Discussion
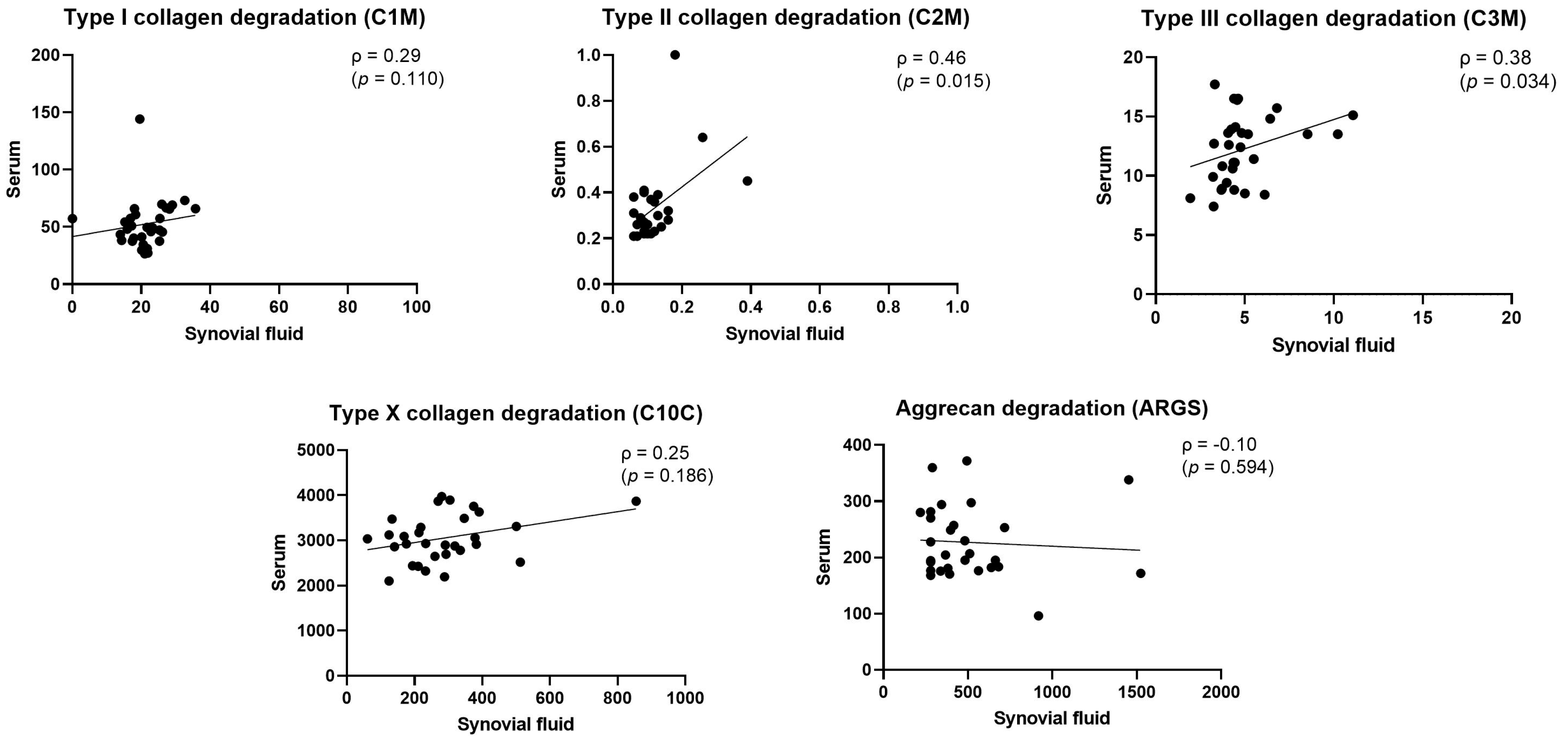
3.1. Correlation between Biomarkers’ Levels in Serum and SF
3.2. Relationship between Biomarkers’ Levels and Structural Outcomes in Both Serum and SF
3.3. Relationship between Biomarkers’ Levels and Pain Outcomes in Both Serum and SF
4. Materials and Methods
4.1. Study Population
4.2. Pain Evaluation
4.3. Structural Evaluation
4.4. Sample Processing
4.4.1. SF Samples
4.4.2. Serum Samples
4.5. Biomarker Assays
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [PubMed]
- Kidd, B.L. Osteoarthritis and joint pain. Pain 2006, 123, 6–9. [Google Scholar] [CrossRef]
- Thudium, C.S.; Löfvall, H.; Karsdal, M.A.; Bay-Jensen, A.C.; Bihlet, A.R. Protein biomarkers associated with pain mechanisms in osteoarthritis. J. Proteom. 2019, 190, 55–66. [Google Scholar] [CrossRef]
- Karsdal, M.A. Biochemistry of Collagens, Laminins and Elastin: Structure, Function and Biomarkers; Academic Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Heinegård, D. Fell-Muir Lecture: Proteoglycans and more—From molecules to biology. Int. J. Exp. Pathol. 2009, 90, 575–586. [Google Scholar] [CrossRef]
- Bay-Jensen, A.C.; Thudium, C.S.; Mobasheri, A. Development and use of biochemical markers in osteoarthritis: Current update. Curr. Opin. Rheumatol. 2018, 30, 121–128. [Google Scholar] [CrossRef]
- Henrotin, Y.; Sanchez, C.; Bay-Jensen, A.C.; Mobasheri, A. Osteoarthritis biomarkers derived from cartilage extracellular matrix: Current status and future perspectives. Ann. Phys. Rehabil. Med. 2016, 59, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Kjelgaard-Petersen, C.; Siebuhr, A.S.; Christiansen, T.; Ladel, C.; Karsdal, M.; Bay-Jensen, A.C. Synovitis biomarkers: Ex vivo characterization of three biomarkers for identification of inflammatory osteoarthritis. Biomarkers 2015, 20, 547–556. [Google Scholar] [CrossRef]
- Radojčić, M.R.; Thudium, C.S.; Henriksen, K.; Tan, K.; Karlsten, R.; Dudley, A.; Chessell, I.; Karsdal, M.A.; Bay-Jensen, A.-C.; Crema, M.D.; et al. Biomarker of extracellular matrix remodelling C1M and proinflammatory cytokine interleukin 6 are related to synovitis and pain in end-stage knee osteoarthritis patients. Pain 2017, 158, 1254–1263. [Google Scholar] [CrossRef]
- Bay-Jensen, A.C.; Liu, Q.; Byrjalsen, I.; Li, Y.; Wang, J.; Pedersen, C.; Leeming, D.J.; Dam, E.B.; Zheng, Q.; Qvist, P.; et al. Enzyme-linked immunosorbent assay (ELISAs) for metalloproteinase derived type II collagen neoepitope, CIIM-Increased serum CIIM in subjects with severe radiographic osteoarthritis. Clin. Biochem. 2011, 44, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Bay-Jensen, A.C.; Manginelli, A.; Karsdal, M.; Luo, Y.; He, Y.; Michaelis, M.; Guehring, H.; Ladel, C. Low levels of type II collagen formation (PRO-C2) are associated with response to sprifermin: A pre-defined, exploratory biomarker analysis from the FORWARD study. Osteoarthr. Cartil. 2022, 30, 92–99. [Google Scholar] [CrossRef]
- Yang, X.; Thudium, C.S.; Bay-Jensen, A.-C.; Karsdal, M.A.; van Santen, J.; Arden, N.K.; Perry, T.A.; Kluzek, S. Association between Markers of Synovial Inflammation, Matrix Turnover and Symptoms in Knee Osteoarthritis: A Cross-Sectional Study. Cells 2021, 10, 1826. [Google Scholar] [CrossRef] [PubMed]
- Thudium, C.; Kluzek, S.; Newton, J.; Spector, T.; Hart, D.; Karsdal, M.; Bay-Jensen, A.; Arden, N. SAT0504 Predictive ability of biomarkers linked with synovitis for future incidence of painful knee osteoarthritis in a community based cohort of middle-age women. Ann. Rheum. Dis. 2017, 76 (Suppl. 2), 966. [Google Scholar] [CrossRef]
- He, Y.; Siebuhr, A.S.; Brandt-Hansen, N.U.; Wang, J.; Su, D.; Zheng, Q.; Simonsen, O.; Petersen, K.K.; Arendt-Nielsen, L.; Eskehave, T.; et al. Type X collagen levels are elevated in serum from human osteoarthritis patients and associated with biomarkers of cartilage degradation and inflammation. BMC Musculoskelet. Disord. 2014, 15, 309. [Google Scholar] [CrossRef] [PubMed]
- Janusz, M.J.; Little, C.; King, L.; Hookfin, E.; Brown, K.; Heitmeyer, S.; Caterson, B.; Poole, A.; Taiwo, Y. Detection of aggrecanase- and MMP-generated catabolic neoepitopes in the rat iodoacetate model of cartilage degeneration. Osteoarthr. Cartil. 2004, 12, 720–728. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Siebuhr, A.; Karsdal, M.; Larkin, J.; Bay-Jensen, A.-C. Development of a highly sensitive chemiluminescence immunoassay for detection of aggrecanase-generated args aggrecan fragments in serum. Osteoarthr. Cartil. 2020, 28, S65–S66. [Google Scholar] [CrossRef]
- Germaschewski, F.M.; Matheny, C.; Larkin, J.; Liu, F.; Thomas, L.; Saunders, J.; Sully, K.; Whittall, C.; Boyle, Y.; Peters, G.; et al. Quantitation OF ARGS aggrecan fragments in synovial fluid, serum and urine from osteoarthritis patients. Osteoarthr. Cartil. 2014, 22, 690–697. [Google Scholar] [CrossRef]
- Boffa, A.; Merli, G.; Andriolo, L.; Lattermann, C.; Salzmann, G.M.; Filardo, G. Synovial Fluid Biomarkers in Knee Osteoarthritis: A Systematic Review and Quantitative Evaluation Using BIPEDs Criteria. Cartilage 2021, 13 (Suppl. 1), 82S–103S. [Google Scholar] [CrossRef]
- Zhang, W.; Likhodii, S.; Aref-Eshghi, E.; Zhang, Y.; Harper, P.E.; Randell, E.; Green, R.; Martin, G.; Furey, A.; Sun, G.; et al. Relationship between blood plasma and synovial fluid metabolite concentrations in patients with osteoarthritis. J. Rheumatol. 2015, 42, 859–865. [Google Scholar] [CrossRef]
- Gibson, D.S.; Blelock, S.; Curry, J.; Finnegan, S.; Healy, A.; Scaife, C.; McAllister, C.; Pennington, S.; Dunn, M.; Rooney, M. Comparative analysis of synovial fluid and plasma proteomes in juvenile arthritis—Proteomic patterns of joint inflammation in early stage disease. J. Proteom. 2009, 72, 656–676. [Google Scholar] [CrossRef]
- Beattie, K.A.; Duryea, J.; Pui, M.; O’Neill, J.; Boulos, P.; Webber, C.E.; Eckstein, F.; Adachi, J.D. Minimum joint space width and tibial cartilage morphology in the knees of healthy individuals: A cross-sectional study. BMC Musculoskelet. Disord. 2008, 9, 119. [Google Scholar] [CrossRef]
- Beattie, K.; Duryea, J.; Pui, M.; Boulos, P.; Webber, C.; Eckstein, F.; Adachi, J.; Oneill, J. The contribution of medial femoral and tibial cartilage thickness to minimum joint space width in osteoarthritic knees. Osteoarthr. Cartil. 2007, 18, S13. [Google Scholar] [CrossRef]
- Jansen, M.P.; Roemer, F.W.; Marijnissen, A.K.C.A.; Kloppenburg, M.; Blanco, F.J.; Haugen, I.K.; Berenbaum, F.; Lafeber, F.P.J.G.; Welsing, P.M.J.; Mastbergen, S.C.; et al. Exploring the differences between radiographic joint space width and MRI cartilage thickness changes using data from the IMI-APPROACH cohort. Skelet. Radiol. 2023, 52, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Reijman, M.; Hazes, J.M.W.; Bierma-Zeinstra, S.M.A.; Koes, B.W.; Christgau, S.; Christiansen, C.; Uitterlinden, A.G.; Pols, H.A.P. A new marker for osteoarthritis: Cross-sectional and longitudinal approach. Arthritis Rheum. 2004, 50, 2471–2478. [Google Scholar] [CrossRef] [PubMed]
- Lotz, M.; Martel-Pelletier, J.; Christiansen, C.; Brandi, M.-L.; Bruyère, O.; Chapurlat, R.; Collette, J.; Cooper, C.; Giacovelli, G.; Kanis, J.A.; et al. Value of biomarkers in osteoarthritis: Current status and perspectives. Ann. Rheum. Dis. 2013, 72, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Van der Kraan, M.; Van den Berg, W.B. Chondrocyte hypertrophy and osteoarthritis: Role in initiation and progression of cartilage degeneration? Osteoarthr. Cartil. 2012, 20, 223–232. [Google Scholar] [CrossRef]
- Boegård, T.; Rudling, O.; Petersson, I.F.; Jonsson, K. Correlation between radiographically diagnosed osteophytes and magnetic resonance detected cartilage defects in the patellofemoral joint. Ann. Rheum. Dis. 1998, 57, 395–400. [Google Scholar] [CrossRef]
- He, Y.; Manon-Jensen, T.; Arendt-Nielsen, L.; Petersen, K.K.; Christiansen, T.; Samuels, J.; Abramson, S.; Karsdal, M.A.; Attur, M.; Bay-Jensen, A.C. Potential diagnostic value of a type X collagen neo-epitope biomarker for knee osteoarthritis. Osteoarthr. Cartil. 2019, 27, 611–620. [Google Scholar] [CrossRef]
- van de Stadt, L.A.; Kroon, F.B.; Thudium, C.F.; Bay-Jensen, A.C.; Kloppenburg, M. Serum biomarkers in prednisolone-treated hand osteoarthritis patients. Rheumatology 2022, 62, 1350–1355. [Google Scholar] [CrossRef]
- Siebuhr, A.S.; Petersen, K.; Arendt-Nielsen, L.; Egsgaard, L.; Eskehave, T.; Christiansen, C.; Simonsen, O.; Hoeck, H.; Karsdal, M.; Bay-Jensen, A. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthr. Cartil. 2014, 22, 44–50. [Google Scholar] [CrossRef]
- Hawker, G.A.; Davis, A.; French, M.; Cibere, J.; Jordan, J.; March, L.; Suarez-Almazor, M.; Katz, J.; Dieppe, P. Development and preliminary psychometric testing of a new OA pain measure—An OARSI/OMERACT initiative. Osteoarthr. Cartil. 2008, 16, 409–414. [Google Scholar] [CrossRef]
- Loeser, R.F.; Beavers, D.; Bay-Jensen, A.; Karsdal, M.; Nicklas, B.; Guermazi, A.; Hunter, D.; Messier, S. Effects of dietary weight loss with and without exercise on interstitial matrix turnover and tissue inflammation biomarkers in adults with knee osteoarthritis: The Intensive Diet and Exercise for Arthritis trial (IDEA). Osteoarthr. Cartil. 2017, 25, 1822–1828. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.K.; Siebuhr, A.S.M.; Graven-Nielsen, T.P.; Simonsen, O.P.; Boesen, M.; Gudbergsen, H.; Karsdal, M.M.; Bay-Jensen, A.C.M.; Arendt-Nielsen, L.P. Sensitization and Serological Biomarkers in Knee Osteoarthritis Patients with Different Degrees of Synovitis. Clin. J. Pain 2016, 32, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Eskehave, T.N.; Egsgaard, L.L.; Petersen, K.K.; Graven-Nielsen, T.; Hoeck, H.C.; Simonsen, O.; Siebuhr, A.S.; Karsdal, M.; Bay-Jensen, A.C. Association between experimental pain biomarkers and serologic markers in patients with different degrees of painful knee osteoarthritis. Arthritis Rheumatol. 2014, 66, 3317–3326. [Google Scholar] [CrossRef] [PubMed]
- Dieppe, A.; Lohmander, L.S. Pathogenesis and management of pain in osteoarthritis. Lancet 2005, 365, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Guermazi, A.; Roemer, F.; Zhang, Y.; Neogi, T. Structural correlates of pain in joints with osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1170–1178. [Google Scholar] [CrossRef]
- van Helvoort, E.M.; van Spil, W.E.; Jansen, M.P.; Welsing, P.M.J.; Kloppenburg, M.; Loef, M.; Blanco, F.J.; Haugen, I.K.; Berenbaum, F.; Bacardit, J.; et al. Cohort profile: Cohort profile: The Applied Public-Private Research enabling OsteoArthritis Clinical Headway (IMI-APPROACH) study: A 2-year, European, cohort study to describe, validate and predict phenotypes of osteoarthritis using clinical, imaging and biochemical markers. BMJ Open 2020, 10, e035101. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Downie, W.W.; Leatham, A.; Rhind, V.M.; Wright, V.; Branco, J.A.; Anderson, J.A. Studies with pain rating scales. Ann. Rheum. Dis. 1978, 37, 378–381. [Google Scholar] [CrossRef]
- Marijnissen, A.C.A.; Vincken, K.; Vos, P.; Saris, D.; Viergever, M.; Bijlsma, J.; Bartels, L.; Lafeber, F. Knee Images Digital Analysis (KIDA): A novel method to quantify individual radiographic features of knee osteoarthritis in detail. Osteoarthr. Cartil. 2008, 16, 234–243. [Google Scholar] [CrossRef]
- Leeming, D.J.; He, Y.; Veidal, S.; Nguyen, Q.; Larsen, D.; Koizumi, M.; Segovia-Silvestre, T.; Zhang, C.; Zheng, Q.; Sun, S.; et al. A novel marker for assessment of liver matrix remodeling: An enzyme-linked immunosorbent assay (ELISA) detecting a MMP generated type I collagen neo-epitope (C1M). Biomarkers 2011, 16, 616–628. [Google Scholar] [CrossRef] [PubMed]
- Barascuk, N.; Veidal, S.S.; Larsen, L.; Larsen, D.V.; Larsen, M.R.; Wang, J.; Zheng, Q.; Xing, R.; Cao, Y.; Rasmussen, L.M.; et al. A novel assay for extracellular matrix remodeling associated with liver fibrosis: An enzyme-linked immunosorbent assay (ELISA) for a MMP-9 proteolytically revealed neoepitope of type III collagen. Clin. Biochem. 2010, 43, 899–904. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Full Dataset (n = 247) | Subset (n = 31) | p-Value | |
|---|---|---|---|
| Age (SD) | 66.5 (7.1) | 68.4 (6.7) | 0.090 |
| Female, n (%) | 176 (71.2) | 19 (61.3) | 0.082 |
| BMI (SD) | 28.3 (5.3) | 27.2 (4.5) | 0.506 |
| KOOS Pain | 63.4 (20.6) | 76.2 (18.9) | <0.001 |
| NRS Pain | 4.4 (2.8) | 3.4 (2.8) | 0.016 |
| ICOAP Pain | 26.3 (21.0) | 16.6 (17.5) | 0.009 |
| minJSW (mm) | 2.4 (1.2) | 2.3 (1.5) | 0.924 |
| Osteophyte Area (mm2) | 26.9 (25.7) | 34.8 (29.62) | 0.158 |
| Subchondral Bone Density (mm) | 30.1 (4.9) | 15.3 (7.8) | 0.096 |
| KL Grade (%) | |||
| 0 | 38 (15.4) | 6 (19.4) | 0.537 |
| 1 | 63 (25.5) | 7 (22.6) | |
| 2 | 47 (19.0) | 5 (16.1) | |
| 3 | 73 (29.6) | 9 (29.0) | |
| 4 | 10 (4.0) | 4 (12.9) |
| Biomarkers/ Clinical Variables | KL Grade | MinJSW | Osteophyte Area | Subchondral Bone Density | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Relative Difference | 95% CI | p | Relative Difference | 95% CI | p | Relative Difference | 95% CI | p | Relative Difference | 95% CI | p | |
| C1M_Serum | 0.955 | 0.864–1.056 | 0.378 | 1.026 | 0.936–1.124 | 0.595 | 0.988 | 0.975–1.001 | 0.155 | 0.938 | 0.908–0.970 | 0.001 |
| C2M_Serum | 0.903 | 0.819–0.995 | 0.049 | 1.131 | 1.041–1.228 | 0.007 | 0.998 | 0.994–1.003 | 0.486 | 1.014 | 0.972–1.057 | 0.532 |
| C3M_Serum | 1.011 | 0.944–1.083 | 0.756 | 1.010 | 0.949–1.075 | 0.760 | 1.001 | 0.998–1.004 | 0.630 | 0.994 | 0.967–1.022 | 0.671 |
| C10C_Serum | 1.030 | 0.982–1.081 | 0.231 | 0.974 | 0.932–1.017 | 0.247 | 1.001 | 0.999–1.003 | 0.464 | 1.011 | 0.991–1.031 | 0.287 |
| ARGS_Serum | 1.077 | 0.999–1.161 | 0.063 | 0.957 | 0.891–1.027 | 0.233 | 1.003 | 1.000–1.007 | 0.055 | 0.996 | 0.964–1.028 | 0.789 |
| C1M_SF | 0.984 | 0.919–1.052 | 0.637 | 1.003 | 0.942–1.068 | 0.921 | 1.000 | 0.996–1.012 | 0.917 | 1.004 | 0.977–1.032 | 0.778 |
| C2M_SF | 0.994 | 0.86–1.150 | 0.941 | 1.048 | 0.923–1.191 | 0.475 | 1.004 | 1.005–1.043 | 0.195 | 1.021 | 0.966–1.080 | 0.465 |
| C3M_SF | 1.014 | 0.931–1.104 | 0.753 | 0.940 | 0.873–1.013 | 0.115 | 1.000 | 0.982–1.007 | 0.869 | 0.988 | 0.955–1.023 | 0.503 |
| C10C_SF | 1.256 | 1.092–1.445 | 0.004 | 0.837 | 0.737–0.950 | 0.011 | 1.011 | 0.976–1.018 | 0.001 | 1.044 | 0.982–1.109 | 0.180 |
| ARGS_SF | 0.889 | 0.768–1.029 | 0.129 | 1.123 | 0.989–1.274 | 0.086 | 0.095 | 0.986–1.033 | 0.148 | 0.990 | 0.934–1.050 | 0.752 |
| Biomarkers/ Clinical Variables | KOOS Pain | NRS Pain | ICOAP Pain | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Relative Difference | 95% CI | p | Relative Difference | 95% CI | p | Relative Difference | 95% CI | p | |||
| C1M_Serum | 1.002 | 0.994–1.009 | 0.671 | 0.990 | 0.937–1.046 | 0.718 | Constant | 0.997 | 0.988–1.007 | 0.584 | |
| Intermittent | 1.002 | 0.994–1.010 | 0.609 | ||||||||
| Total | 1.000 | 0.991–1.009 | 0.949 | ||||||||
| C2M_Serum | 1.007 | 1.000–1.015 | 0.049 | 0.961 | 0.910–1.016 | 0.173 | Constant | 0.991 | 0.982–1.000 | 0.059 | |
| Intermittent | 0.993 | 0.985–1.001 | 0.112 | ||||||||
| Total | 0.992 | 0.983–1.000 | 0.071 | ||||||||
| C3M_Serum | 1.004 | 0.999–1.009 | 0.130 | 0.966 | 0.932–1.000 | 0.064 | Constant | 0.993 | 0.987–0.999 | 0.020 | |
| Intermittent | 0.997 | 0.992–1.002 | 0.268 | ||||||||
| Total | 0.091 | 0.989–1.001 | 0.995 | ||||||||
| C10C_Serum | 0.999 | 0.995–1.002 | 0.497 | 1.012 | 0.985–1.039 | 0.396 | Constant | 1.000 | 0.996–1.005 | 0.978 | |
| Intermittent | 1.001 | 0.998–1.005 | 0.482 | ||||||||
| Total | 1.001 | 0.997–1.005 | 0.664 | ||||||||
| ARGS_Serum | 0.999 | 0.993–1.005 | 0.793 | 1.009 | 0.966–1.054 | 0.685 | Constant | 0.999 | 0.992–1.007 | 0.867 | |
| Intermittent | 1.003 | 0.997–1.010 | 0.310 | ||||||||
| Total | 1.002 | 0.995–1.009 | 0.594 | ||||||||
| C1M_SF | 1.000 | 0.995–1.003 | 0.996 | 1.002 | 0.965–1.039 | 0.929 | Constant | 1.000 | 0.993–1.008 | 0.941 | |
| Intermittent | 0.999 | 0.993–1.004 | 0.667 | ||||||||
| Total | 1.000 | 0.991–1.001 | 0.949 | ||||||||
| C2M_SF | 1.004 | 0.988–1.009 | 0.396 | 0.953 | 0.887–1.025 | 0.209 | Constant | 0.993 | 0.980–1.006 | 0.292 | |
| Intermittent | 0.991 | 0.981–1.002 | 0.130 | ||||||||
| Total | 0.991 | 0.979–1.003 | 0.161 | ||||||||
| C3M_SF | 1.000 | 0.993–1.006 | 0.926 | 0.993 | 0.947–1.040 | 0.761 | Constant | 1.000 | 0.993–1.008 | 0.941 | |
| Intermittent | 1.001 | 0.994–1.008 | 0.847 | ||||||||
| Total | 1.001 | 0.003–1.008 | 0.882 | ||||||||
| C10C_SF | 0.998 | 1.000–1020 | 0.718 | 0.996 | 0.914–1.084 | 0.919 | Constant | 1.005 | 0.992–1.018 | 0.497 | |
| Intermittent | 1.002 | 0.989–1.015 | 0.760 | ||||||||
| Total | 1.002 | 0.989–1.016 | 0.738 | ||||||||
| ARGS_SF | 0.997 | 0.983–1.006 | 0.548 | 1.054 | 0.977–1.137 | 0.188 | Constant | 1.005 | 0.992–1.018 | 0.497 | |
| Intermittent | 1.006 | 0.994–1.017 | 0.347 | ||||||||
| Total | 1.006 | 0.993–1.018 | 0.384 | ||||||||
| Protein | Biomarker Description | Reflective of | Ref. |
|---|---|---|---|
| Type I collagen | C1M: Neo-epitope of MMP-2-, -9-, and -13-mediated degradation of type I collagen | Bone and synovial tissue degradation | [42] |
| Type II collagen | C2M: Neo-epitope of MMP (multiple)-mediated degradation of type II collagen | Cartilage degradation | [10] |
| Type III collagen | C3M: Neo-epitope of MMP-9-mediated degradation of type III collagen | Synovial tissue degradation | [43] |
| Type X collagen | C10C: Cathepsin-K-mediated degradation of type X collagen | Chondrocyte activity | [14] |
| Aggrecan | ARGS: ADAMTS4/5-mediated degradation of aggrecan | Cartilage degradation | [16] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalogera, S.; Jansen, M.P.; Bay-Jensen, A.-C.; Frederiksen, P.; Karsdal, M.A.; Thudium, C.S.; Mastbergen, S.C. Relevance of Biomarkers in Serum vs. Synovial Fluid in Patients with Knee Osteoarthritis. Int. J. Mol. Sci. 2023, 24, 9483. https://doi.org/10.3390/ijms24119483
Kalogera S, Jansen MP, Bay-Jensen A-C, Frederiksen P, Karsdal MA, Thudium CS, Mastbergen SC. Relevance of Biomarkers in Serum vs. Synovial Fluid in Patients with Knee Osteoarthritis. International Journal of Molecular Sciences. 2023; 24(11):9483. https://doi.org/10.3390/ijms24119483
Chicago/Turabian StyleKalogera, Stefania, Mylène P. Jansen, Anne-Christine Bay-Jensen, Peder Frederiksen, Morten A. Karsdal, Christian S. Thudium, and Simon C. Mastbergen. 2023. "Relevance of Biomarkers in Serum vs. Synovial Fluid in Patients with Knee Osteoarthritis" International Journal of Molecular Sciences 24, no. 11: 9483. https://doi.org/10.3390/ijms24119483