
HDL Subclasses and the Distribution of Paraoxonase-1 Activity in Patients with ST-Segment Elevation Acute Myocardial Infarction
 , , ,
, , , 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Methods
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death, Report [Internet]. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 25 March 2021).
- Wang, R.; Mei, B.; Liao, X.; Lu, X.; Yan, L.; Lin, M.; Zhong, Y.; Chen, Y.; You, T. Determination of risk factors affecting the in-hospital prognosis of patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention. BMC Cardiovasc. Disord. 2017, 17, 243. [Google Scholar] [CrossRef]
- Wang, H.H.; Garruti, G.; Liu, M.; Portincasa, P.; Wang, D.Q. Cholesterol and lipoprotein metabolism and atherosclerosis: Recent advances in reverse cholesterol transport. Ann. Hepatol. 2017, 16, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Geovanini, G.R.; Libby, P. Atherosclerosis and inflammation: Overview and updates. Clin. Sci. 2018, 132, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, M.; Poursaleh, A.; Ghasempour, G.; Farhad, S.; Najafi, M. The effects of oxidative stress on the development of atherosclerosis. Biol. Chem. 2019, 400, 711–732. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Bonacina, F.; Norata, G.D.; Catapano, A.L. Interplay of lipids, lipoproteins and immunity in atherosclerosis. Curr. Atheroscler. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Dhindsa, D.S.; Sandesara, P.B.; Shapiro, M.D.; Wong, N.D. The evolving understanding and approach to residual cardiovascular risk management. Front. Cardiovasc. Med. 2020, 7, 88. [Google Scholar] [CrossRef]
- Ikezaki, H.; Lim, E.; Cupples, L.A.; Liu, C.T.; Asztalos, B.F.; Schaefer, E.J. Small dense low-density lipoprotein cholesterol is the most atherogenic lipoprotein parameter in the prospective Framingham Offspring Study. J. Am. Heart Assoc. 2021, 10, e019140. [Google Scholar] [CrossRef]
- Teng, B.; Thompson, G.R.; Sniderman, A.D.; Forte, T.M.; Krauss, R.M.; Kwiterovich, P.O., Jr. Composition and distribution of low density lipoprotein fractions in hyperapobetalipoproteinemia, normolipidemia, and familial hypercholesterolemia. Proc. Natl. Acad. Sci. USA 1983, 80, 6662–6666. [Google Scholar] [CrossRef]
- Maiolino, G.; Rossitto, G.; Caielli, P.; Bisogni, V.; Rossi, G.P.; Calò, L.A. The role of oxidized low-density lipoproteins in atherosclerosis: The myths and the facts. Mediat. Inflamm. 2013, 2013, 714653. [Google Scholar] [CrossRef]
- Camont, L.; Chapman, M.J.; Kontush, A. Biological activities of HDL subpopulations and their relevance to cardiovascular disease. Trends Mol. Med. 2011, 17, 594–603. [Google Scholar] [CrossRef]
- Rached, F.H.; Chapman, M.J.; Kontush, A. HDL particle subpopulations: Focus on biological function. Biofactors 2015, 41, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Rye, K.A.; Barter, P.J. Cardioprotective functions of HDLs. J. Lipid Res. 2014, 55, 168–179. [Google Scholar] [CrossRef]
- Kontush, A.; Chantepie, S.; Chapman, M.J. Small, dense HDL particles exert potent protection of atherogenic LDL against oxidative stress. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Navab, M.; Reddy, S.T.; Van Lenten, B.J.; Anantharamaiah, G.M.; Fogelman, A.M. Role of dysfunctional HDL in atherosclerosis. J. Lipid Res. 2009, 50, 145–149. [Google Scholar] [CrossRef]
- Otocka-Kmiecik, A.; Mikhailidis, D.P.; Nicholls, S.J.; Davidson, M.; Rysz, J.; Banach, M. Dysfunctional HDL: A novel important diagnostic and therapeutic target in cardiovascular disease? Prog. Lipid Res. 2012, 51, 314–324. [Google Scholar] [CrossRef]
- Chistiakov, D.A.; Melnichenko, A.A.; Orekhov, A.N.; Bobryshev, Y.V. Paraoxonase and atherosclerosis-related cardiovascular diseases. Biochimie 2017, 132, 19–27. [Google Scholar] [CrossRef]
- Samouilidou, E.; Kostopoulos, V.; Liaouri, A.; Kioussi, E.; Vassiliou, K.; Bountou, E.; Grapsa, E. Association of lipid profile with serum PON1 concentration in patients with chronic kidney disease. Ren. Fail. 2016, 38, 1601–1606. [Google Scholar] [CrossRef]
- Gugliucci, A. Activation of paraoxonase 1 is associated with HDL remodelling ex vivo. Clin. Chim. Acta 2014, 429, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Gugliucci, A.; Menini, T. Paraoxonase 1 and HDL maturation. Clin. Chim. Acta 2015, 439, 5–13. [Google Scholar] [CrossRef]
- Rosenson, R.S. Myocardial injury: The acute phase response and lipoprotein metabolism. J. Am. Coll. Cardiol. 1993, 22, 933–940. [Google Scholar] [CrossRef]
- Carnuta, M.G.; Stancu, C.S.; Toma, L.; Sanda, G.M.; Niculescu, L.S.; Deleanu, M.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; et al. Dysfunctional high-density lipoproteins have distinct composition, diminished antiinflammatory potential and discriminate acute coronary syndrome from stable coronary artery disease patients. Sci. Rep. 2017, 7, 72–95. [Google Scholar] [CrossRef] [PubMed]
- Brites, F.; Martin, M.; Guillas, I.; Kontush, A. Antioxidative activity of high-density lipoprotein (HDL): Mechanistic insights into potential clinical benefit. BBA Clin. 2017, 8, 66–77. [Google Scholar] [CrossRef]
- Miljkovic, M.; Stefanovic, A.; Vekic, J.; Zeljkovic, A.; Gojkovic, T.; Simic-Ogrizovic, S.; Bogavac-Stanojevic, N.; Cerne, D.; Ilic, J.; Stefanovic, I.; et al. Activity of paraoxonase 1 (PON1) on HDL 2 and HDL 3 subclasses in renal disease. Clin. Biochem. 2018, 60, 52–58. [Google Scholar] [CrossRef]
- Nobecourt, E.; Jacqueminet, S.; Hansel, B.; Chantepie, S.; Grimaldi, A.; Chapman, M.J.; Kontush, A. Defective antioxidative activity of small dense HDL3 particles in type 2 diabetes: Relationship to elevated oxidative stress and hyperglycaemia. Diabetologia 2005, 48, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Bains, Y.; Caccavello, R.; Kotani, K.; Gugliucci, A. Paraoxonase 1, HDL subclasses and post surgery acute inflammation: A pilot study. Antioxidants 2019, 8, 192. [Google Scholar] [CrossRef]
- Meisinger, C.; Freuer, D.; Bub, A.; Linseisen, J. Association between inflammatory markers and serum paraoxonase and arylesterase activities in the general population: A cross-sectional study. Lipids Health Dis. 2021, 20, 81. [Google Scholar] [CrossRef]
- Blagojevic, I.M.P.; Vekic, J.Z.; Macut, D.P.; Ignjatovic, S.D.; Miljkovic-Trailovic, M.M.; Zeljkovic, A.R.; Spasojevic-Kalimanovska, V.V.; Bozic-Antic, I.B.; Bjekic-Macut, J.D.; Kastratovic-Kotlica, B.A.; et al. Overweight and obesity in polycystic ovary syndrome: Association with inflammation, oxidative stress and dyslipidaemia. Br. J. Nutr. 2021, 128, 604–612. [Google Scholar] [CrossRef]
- Djekic, S.; Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Kafedzic, S.; Zdravkovic, M.; Ilic, I.; Hinic, S.; Cerovic, M.; Stefanovic, M.; et al. Investigation of IgG anti-oxLDL antibody levels and HDL and LDL subclasses in patients with ST-segment elevation acute myocardial infarction. Arch. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Van de Werf, F.; Ardissino, D.; Betriu, A.; Cokkinos, D.V.; Falk, E.; Fox, K.A.; Julian, D.; Lengyel, M.; Neumann, F.J.; Ruzyllo, W.; et al. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur. Heart J. 2003, 24, 28–66. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef]
- Fukuyama, N.; Homma, K.; Wakana, N.; Kudo, K.; Suyama, A.; Ohazama, H.; Tsuji, C.; Ishiwata, K.; Eguchi, Y.; Nakazawa, H.; et al. Validation of the Friedewald equation for evaluation of plasma LDL-cholesterol. J. Clin. Biochem. Nutr. 2008, 43, 1–5. [Google Scholar] [CrossRef]
- Girotti, M.J.; Khan, N.; McLellan, B.A. Early measurements of systemic lipid peroxidation products in plasma of major blunt trauma patients. J. Trauma 1991, 31, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Rainwater, D.L.; Moore, P.H.; Gamboa, I.O. Improved method for making non-denaturing composite gradient gels for the electrophoretic separation of lipoproteins. J. Lipid Res. 2004, 45, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Vekic, J.; Topic, A.; Zeljkovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V. LDL and HDL subclasses and their relationship with Framingham risk score in middle-aged Serbian population. Clin. Biochem. 2007, 40, 310–316. [Google Scholar] [CrossRef]
- Gugliucci, A.; Caccavello, R.; Kotani, K.; Sakane, N.; Kimura, S. Enzymatic assessment paraoxonase 1 activity on HDL subclasses: A practical zymogram method to assess HDL function. Clin. Chim. Acta 2013, 415, 162–168. [Google Scholar] [CrossRef]
- Zeljkovic, A.; Vekic, J.; Spasojevic-Kalimanovska, V.; Jelic-Ivanovic, Z.; Bogavac-Stanojevic, N.; Gulan, B.; Spasic, S. LDL and HDL subclasses in acute ischemic stroke: Prediction of risk and short-term mortality. Atherosclerosis 2010, 210, 548–554. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable. | Control Group | STEMI Group | p Value |
|---|---|---|---|
| N | 67 | 69 | |
| Age, years | 55 ± 9 | 61 ± 12 | 0.005 |
| Prevalence of males, % | 73.1 | 79.7 | 0.37 |
| BMI, kg/m2 | 26.28 (24.18–29.50) | 25.25 (23.37–27.70) | 0.04 |
| Smokers, % | 19.4 | 58 | <0.001 |
| HT, % | 38.8 | 61.8 | 0.001 |
| TC, mmol/L | 5.70 ± 1.09 | 5.54 ± 1.30 | 0.44 |
| TG, mmol/L | 1.40 (0.98–1.74) | 1.70 (1.22–2.33) | 0.007 |
| HDL-C, mmol/L | 1.34 (1.10–1.55) | 0.95 (0.80–1.21) | <0.001 |
| LDL-C, mmol/L | 3.65 ± 1.06 | 3.67 ± 1.12 | 0.92 |
| sdLDL, % | 53.3 (43.0–58.5) | 54.5 (48.1–58.7) | 0.15 |
| MDA, µmol/L | 3.74 (3.26–4.28) | 3.26 (2.44–6.11) | 0.40 |
| hsCRP, mg/L | 0.7 (0.3–1.9) | 3.7 (2.1–7.2) | <0.001 |
| Variable | Control Group | STEMI Group | p Value |
|---|---|---|---|
| N | 67 | 69 | |
| HDL2, % | 62.1 (60.1–64.2) | 56.6 (545–58.7) | <0.001 |
| HDL2b, % | 39.4 (37.5–41.3) | 37.0 (35.0–38.9) | 0.10 |
| HDL2a, % | 22.7 (21.7–23.7) | 19.6 (18.7–20.6) | <0.001 |
| HDL3, % | 37.9 (35.8–39.9) | 43.1 (41.1–45.1) | <0.001 |
| HDL3a, % | 18.6 (17.7–19.5) | 17.0 (16.1–17.9) | <0.03 |
| HDL3b, % | 9.5 (8.9–10.2) | 11.6 (10.8–12.3) | 0.001 |
| HDL3c, % | 9.8 (9.5–11.0) | 14.6 (13.3–15.8) | <0.001 |
| pPON1 within HDL2, % | 65.4 (63.4–67.3) | 11.3 (9.8–12.9) | 0.09 |
| pPON1 within HDL2b, % | 43.6 (41.7–44.4) | 46.4 (44.4–48.4) | 0.06 |
| pPON1 within HDL2a, % | 21.8 (20.5–23.1) | 21.7 (20.3–23.0) | 0.87 |
| pPON1 within HDL3, % | 34.6 (32.7–36.6) | 31.8 (29.9–34.1) | 0.09 |
| pPON1 within HDL3a, % | 13.6 (13.0–14.1) | 12.7 (12.1–13.3) | 0.07 |
| pPON1 within HDL3b, % | 9.0 (8.5–9.6) | 7.9 ± 2.1 | 0.006 |
| pPON1 within HDL3c, % | 12.5 ± 5.9 | 10.9 ± 3.7 | 0.12 |
| Variable | sdLDL Proportion | Control Group | STEMI Group | p (sdLDL Groups) | p (STEMI vs. Control) | p (Interaction) |
|---|---|---|---|---|---|---|
| HDL2, % | sdLDL ≤ 50% | 63.4 ± 7.4 | 59.4 ± 9.0 | 0.04 | 0.15 | 0.24 |
| sdLDL > 50% | 58.5 ± 9.7 | 58.0 ± 6.8 | ||||
| HDL2b, % | sdLDL ≤ 50% | 40.6 ± 5.9 | 38.3 ± 8.7 | 0.15 | 0.85 | 0.15 |
| sdLDL > 50% | 36.6 ± 9.3 | 38.3 ± 5.8 | ||||
| HDL2a, % | sdLDL ≤ 50% | 22.8 ± 3.9 | 21.1 ± 3.0 | 0.08 | 0.004 | 0.76 |
| sdLDL > 50% | 31.8 ± 3.4 | 19.7 ± 3.9 | ||||
| HDL3, % | sdLDL ≤ 50% | 36.4 ± 6.9 | 40.6 ± 9.0 | 0.04 | 0.15 | 0.14 |
| sdLDL > 50% | 41.5 ± 9.7 | 41.6 ± 6.5 | ||||
| HDL3a, % | sdLDL ≤ 50% | 17.8 ± 3.3 | 16.0 ± 2.8 | 0.03 | <0.001 | 0.30 |
| sdLDL > 50% | 19.8 ± 4.1 | 16.7 ± 2.9 | ||||
| HDL3b, % | sdLDL ≤ 50% | 9.0 ± 2.6 | 10.8 ± 2.8 | 0.06 | 0.01 | 0.36 |
| sdLDL > 50% | 10.5 ± 3.2 | 11.3 ± 2.2 | ||||
| HDL3c, % | sdLDL ≤ 50% | 9.5 ± 6.0 | 13.8 ± 5.3 | 0.37 | <0.001 | 0.29 |
| sdLDL > 50% | 11.3 ± 4.4 | 13.7 ± 4.5 |
| Variable | sdLDL Proportion | Control Group | STEMI Group | p (sdLDL Groups) | p (STEMI vs. Control) | p (Interaction) |
|---|---|---|---|---|---|---|
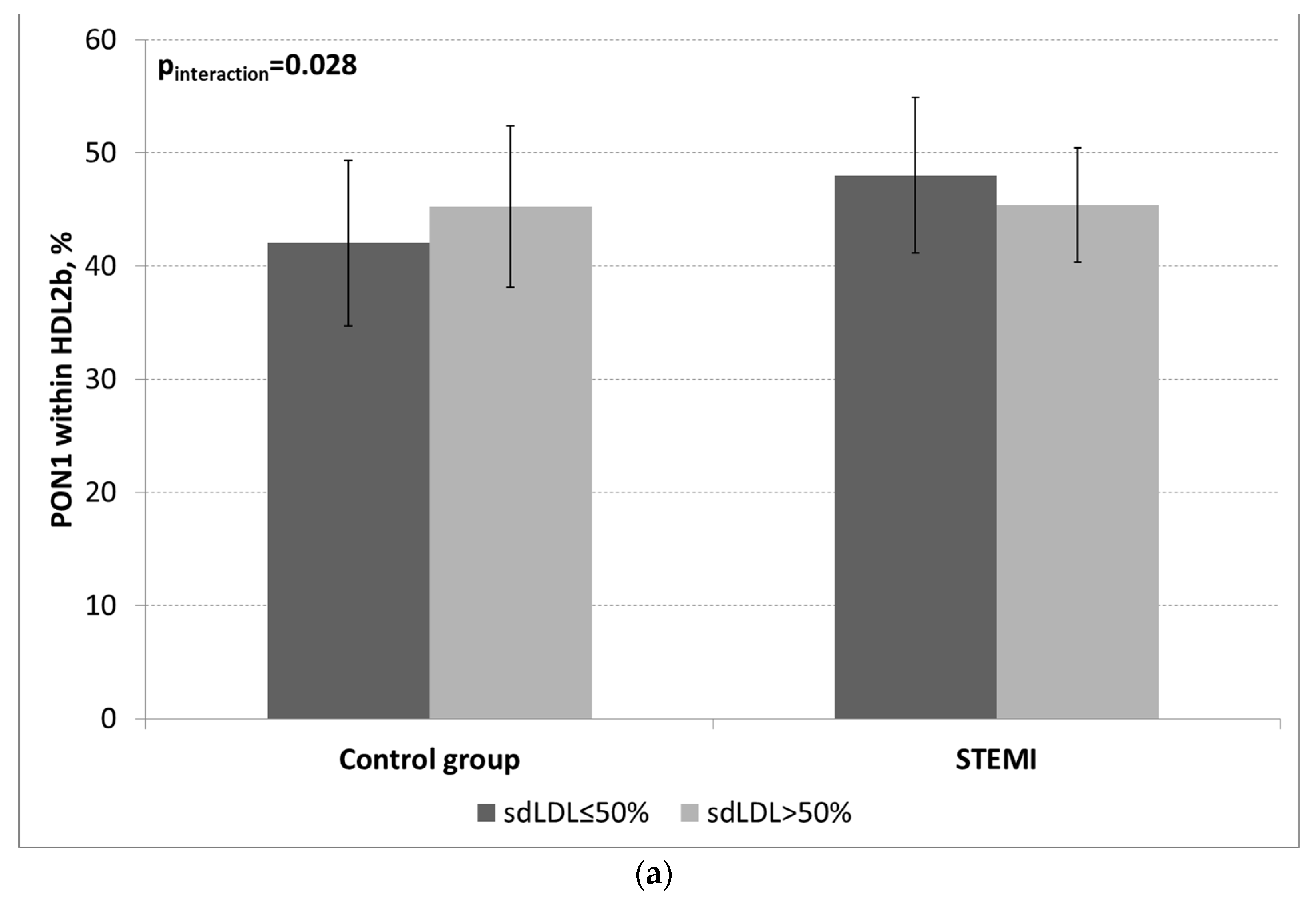
| pPON1 within HDL2b, % | sdLDL ≤ 50% | 42.0 ± 7.3 | 48.0 ± 6.8 | 0.82 | 0.09 | 0.03 |
| sdLDL > 50% | 45.3 ± 7.1 | 45.4 ± 5.0 | ||||
| pPON1 within HDL2a, % | sdLDL ≤ 50% | 22.9 ± 5.5 | 22.7 ± 3.9 | 0.04 | 0.45 | 0.30 |
| sdLDL > 50% | 20-2 ± 3.1 | 21.8 ± 4.9 | ||||
| pPON1 within HDL3, % | sdLDL ≤ 50% | 35.1 ± 7.0 | 29.3 ± 6.7 | 0.28 | 0.02 | 0.14 |
| sdLDL > 50% | 34.5 ± 7.8 | 32.8 ± 5.5 | ||||
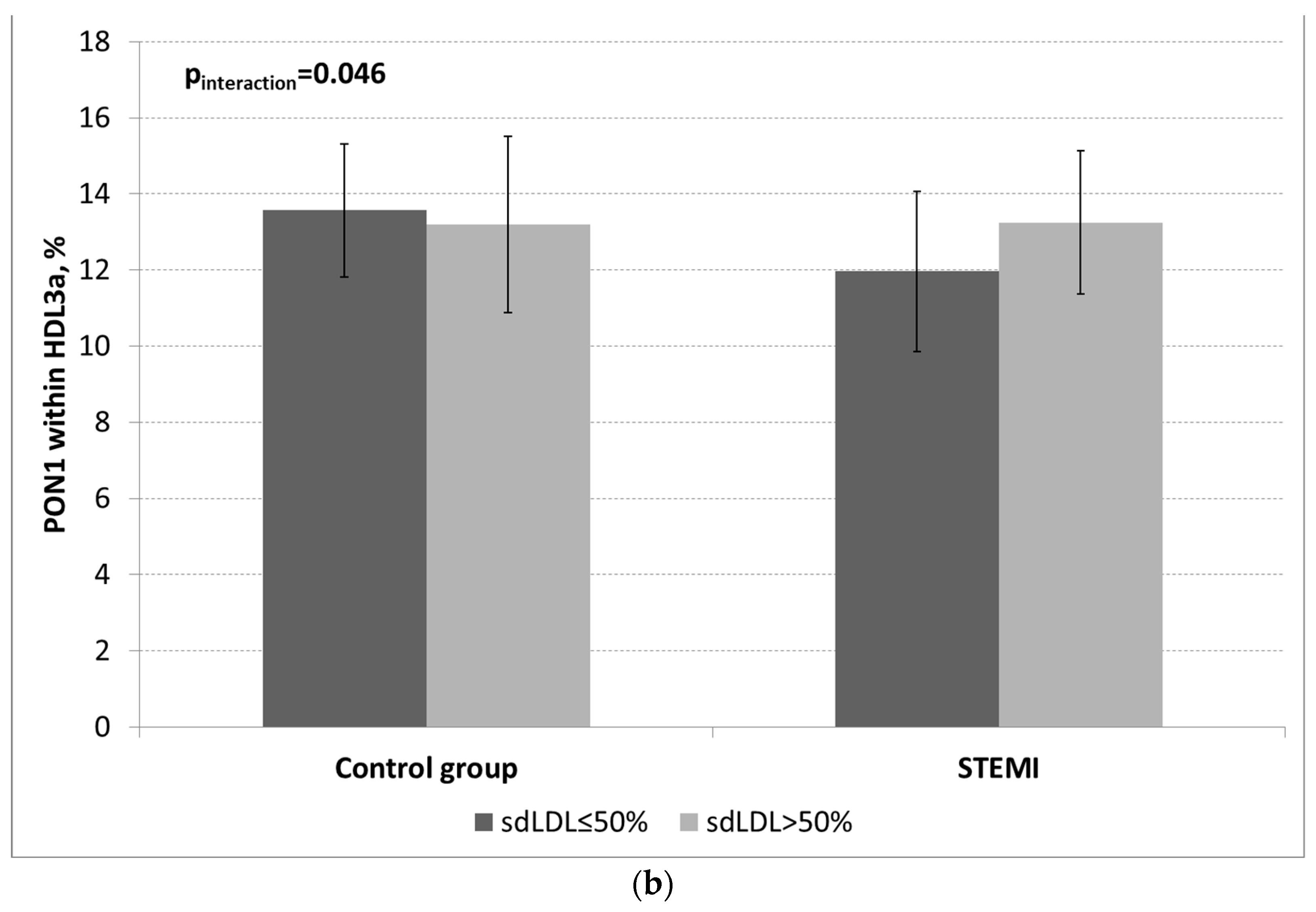
| pPON1 within HDL3a, % | sdLDL ≤ 50% | 13.6 ± 1.7 | 11.9 ± 2.1 | 0.27 | 0.06 | 0.046 |
| sdLDL > 50% | 13.2 ± 2.3 | 13.2 ± 1.9 | ||||
| pPON1within HDL3b, % | sdLDL ≤ 50% | 9.3 ± 1.9 | 7.6 ± 1.9 | 0.89 | 0.003 | 0.15 |
| sdLDL > 50% | 8.7 ± 1.8 | 8.1 ± 2.1 | ||||
| pPON1 within HDL3c, % | sdLDL ≤ 50% | 12.2 ± 4.3 | 9.8 ± 3.4 | 0.29 | 0.08 | 0.53 |
| sdLDL > 50% | 12.6 ± 6.7 | 11.5 ± 3.8 |
| Controls r | |||||
| PON1 within HDL2b | PON1 within HDL2a | PON1 within HDL3a | PON1 within HDL3b | PON1 within HDL3c | |
| HDL | 0.054 | 0.121 | −0.098 | −0.027 | −0.113 |
| logTG | −0.017 | −0.199 | 0.050 | 0.110 | 0.115 |
| logsdLDL | 0.070 | −0.375 ** | −0.038 | 0.054 | 0.187 |
| logCRP | 0.204 | −0.044 | −0.109 | −0.0117 | −0.132 |
| logMDA | 0.086 | −0.132 | 0.089 | 0.069 | −0.063 |
| STEMI Patients r | |||||
| PON1 within HDL2b | PON1 within HDL2a | PON1 within HDL3a | PON1 within HDL3b | PON1 within HDL3c | |
| HDL | 0.021 | 0.002 | 0.117 | −0.129 | 0.035 |
| logTG | 0.066 | −0.208 | −0.013 | 0.046 | 0.153 |
| logsdLDL | 0.029 | −0.129 | 0.177 | −0.053 | 0.059 |
| logCRP | −0.199 | 0.039 | 0.248 | 0.096 | 0.053 |
| logMDA | 0.342 * | −0.133 | −0.125 | −0.106 | −0.196 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djekic, S.; Vekic, J.; Zeljkovic, A.; Kotur-Stevuljevic, J.; Kafedzic, S.; Zdravkovic, M.; Ilic, I.; Hinic, S.; Cerovic, M.; Stefanovic, M.; et al. HDL Subclasses and the Distribution of Paraoxonase-1 Activity in Patients with ST-Segment Elevation Acute Myocardial Infarction. Int. J. Mol. Sci. 2023, 24, 9384. https://doi.org/10.3390/ijms24119384
Djekic S, Vekic J, Zeljkovic A, Kotur-Stevuljevic J, Kafedzic S, Zdravkovic M, Ilic I, Hinic S, Cerovic M, Stefanovic M, et al. HDL Subclasses and the Distribution of Paraoxonase-1 Activity in Patients with ST-Segment Elevation Acute Myocardial Infarction. International Journal of Molecular Sciences. 2023; 24(11):9384. https://doi.org/10.3390/ijms24119384
Chicago/Turabian StyleDjekic, Saska, Jelena Vekic, Aleksandra Zeljkovic, Jelena Kotur-Stevuljevic, Srdjan Kafedzic, Marija Zdravkovic, Ivan Ilic, Sasa Hinic, Milivoje Cerovic, Milica Stefanovic, and et al. 2023. "HDL Subclasses and the Distribution of Paraoxonase-1 Activity in Patients with ST-Segment Elevation Acute Myocardial Infarction" International Journal of Molecular Sciences 24, no. 11: 9384. https://doi.org/10.3390/ijms24119384