
The Human Gastric Juice: A Promising Source for Gastric Cancer Biomarkers

 , , , , and
, , , , and
Abstract
:1. Introduction
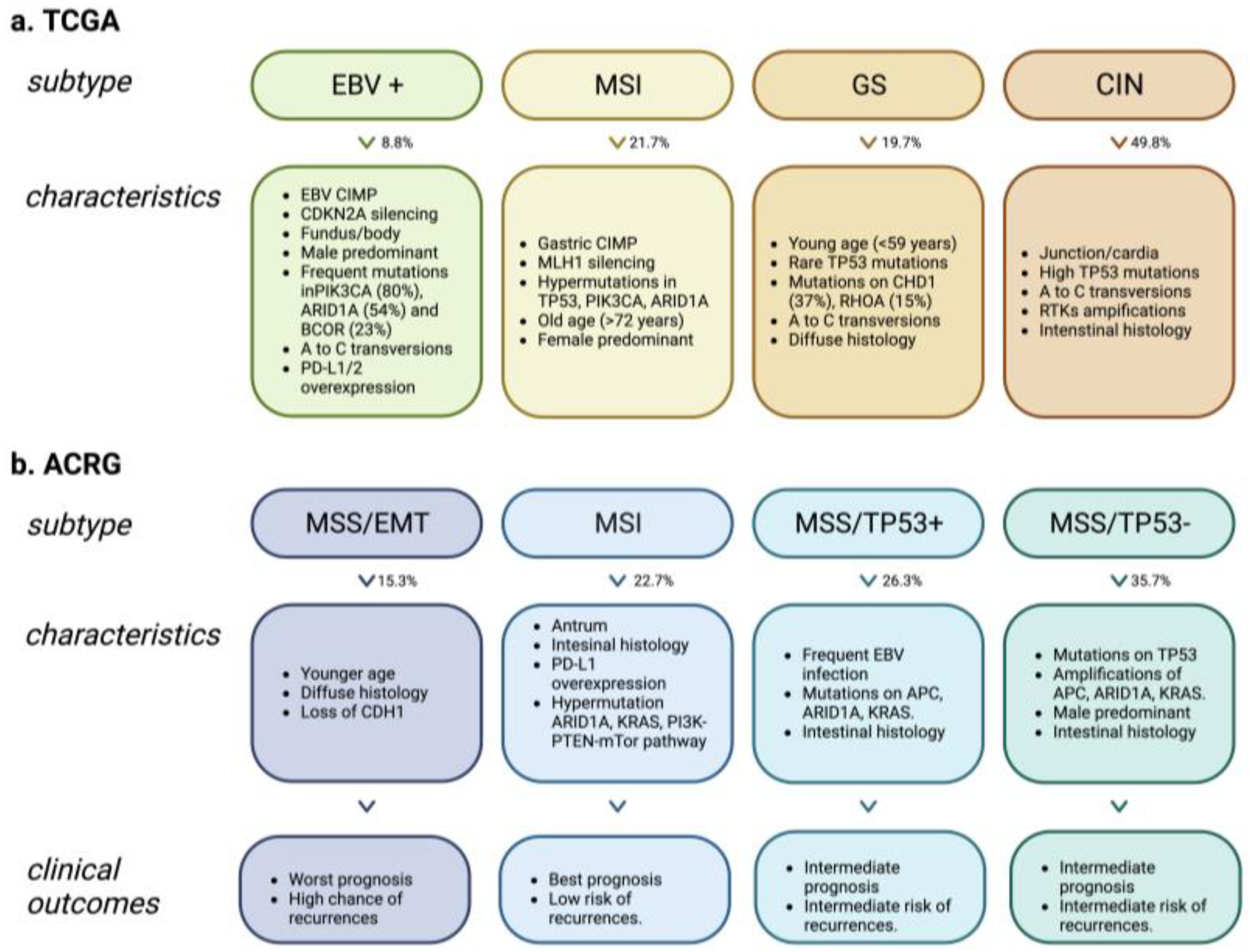
2. Molecular Classification of Gastric Cancer
3. Gastric Fluid Physiopathology: Risk Factors of GC
3.1. Helicobacter Pylori
3.2. Epstein-Barr Virus
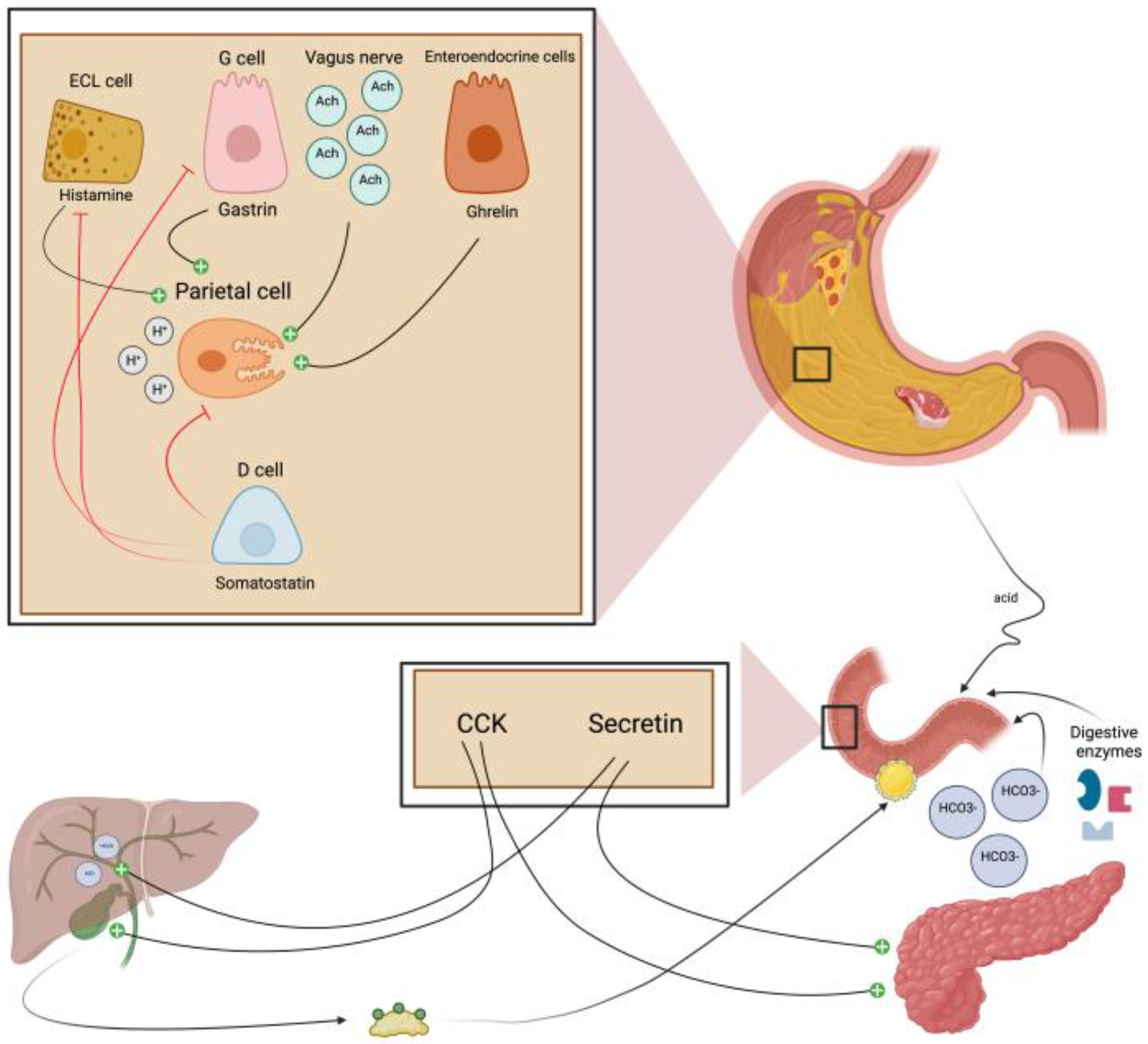
4. The Regulation of the Production of Gastric Juice
5. Gastric Juice Collection and Biomarkers in Gastric Cancer
5.1. Non-Coding RNAs
5.1.1. microRNAs
5.1.2. piRNAs
5.1.3. lncRNAs
5.2. DNA
5.3. Proteins

{kind=link}
{kind=link}
| Ref. No. | Type | Biomarkers | GC/nonGC Patients | Expression Level * | AUC (95% CI) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|
| [39] | miRNA | miR-421 | 42/99 | Downregulated (p < 0.001) | 0.77 (0.68–0.85) | 71.40 | 71.70 |
| [40] | miRNA | miR-129-1-3p and miR-129-2-3p | 42/99 | Downregulated (p < 0.001) | 0.66 (0.56–0.76) | 68.70 | 71.90 |
| [41] | miRNA | miR-106a | 42/99 | Downregulated (p < 0.001) | 0.87 (0.80–0.95) | 73.80 | 89.30 |
| [41,42] | miRNA | miR-21 | 42/99 | Downregulated (p < 0.001) | 0.97 (0.94–1) | 85.70 | 97.80 |
| [42] | miRNA | miR-133a | 62/142 | Downregulated (p < 0.001) | 0.91 (0.86–0.96) | 85.90 | 84.80 |
| [44] | piRNA | piR-1245 | 66/66 | Upregulated (p < 0.0001) | 0.89 (0.83–0.94) | 90.90 | 74.20 |
| [45] | lncRNA | Linc00152 | 17/16 | Upregulated (p = 0.002) | - | - | - |
| [46] | lncRNA | AA174084 | 39/92 | Upregulated (p < 0.01) | 0.85 (0.78–0.92) | 46.00 | 93.00 |
| [47] | lncRNA | RMRP | 39/92 | Upregulated (p < 0.01) | 0.70 (0.59–0.81) | 56.40 | 75.40 |
| [48] | lncRNA | ABHD11-AS1 | 39/92 | Upregulated (p < 0.033) | 0.65 (0.54–0.77) | 41.00 | 93.40 |
| [49] | lncRNA | LINC00982 | 27/27 | Upregulated (p < 0.026) | - | - | - |
| [50] | lncRNA | H19 | 33/23 | Upregulated (p < 0.034) | - | - | - |
| [51] | lncRNA | UCA1 | 26/23 | Upregulated (p < 0.016) | - | - | - |
| [53] | DNA | BARHL2 | 20/10 | - | 0.92 | 90.00 | 100.00 |
| [54] | Protein | α1-Antitrypsin | 31/120 | - | - | - | - |
| [55] | 30/5 | - | - | - | - |
6. Deployment of Proteomics in Gastric Juice
| Ref. No. | Study Subjects | Analytical Platform | Findings |
|---|---|---|---|
| [54] | healthy subjects (n = 120) | 2D-electrophoresis MALDI-TOF MS LC-MS/MS | Alpha-1-antitrypsin precursor as a novel gastric juice biomarker for gastric cancer and ulcer. |
| gastric ulcer (n = 39) | |||
| duodenal ulcer (n = 38) | |||
| gastric cancer (n = 31) | |||
| [55] | 99 individuals | 2D-electrophoresis MALDI-TOF MS LC-MS/MS | Strong association of a high level of alpha-1-antitrypsin in gastric juice with gastric cancer |
| gastric cancer (n = 30) | |||
| gastrititis (n = 56) | |||
| Others (n = 13) | |||
| [61] | benign gastric conditions (n = 170) | 2D-electrophoresis Multidimensional LC-MS/MS | Distinct protein profiles for acidic and neutral samples, highlighting pH effects on protein composition |
| [67] | gastric cancer (n = 19) | SELDI-TOF MS | 60 proteomic features were up-regulated, and 46 were down-regulated in gastric cancer samples. |
| benign gastritis (n = 36) | |||
| [68] | normal (n = 106) | MALDI TOF-TOF ESI-MS/MS | Five peptides for gastric cancer diagnosis with high sensitivity and specificity (derived from pepsinogen, leucine zipper protein, albumin and a-1-antitrypsin fragment) |
| duodenal ulcer (n = 38) | |||
| gastric ulcer (n = 38) | |||
| gastric cancer (n = 34) | |||
| [88] | chronic gastritis (n = 6) | MALDI TOF-TOF | First report of the proteome of human gastric juice with gastritis background (327 proteins) |
| [89] | gastric cancer (n = 70) | iTRAQ and SWATH LC-MS/MS | A biomarker panel scoring matrix for early GC detection (diagnostic sensitivity of 95.7%) |
| benign gastritits (n = 17) |
7. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GC | Gastric Cancer |
| GJ | Gastric Juice |
| NCGC | Non-Cardia Gastric Cancer |
| CGC | Cardia Gastric Cancer |
| DGC | Diffuse Gastric Cancer |
| IGC | Intestinal Gastric Cancer |
| H. pylori | Helicobacter pylori |
| CagA | Cytotoxin-associated gene A |
| VacA | Vacuolating Cytotoxin |
| EBV | Epstein Barr virus |
| HDGC | Hereditary Diffuse Gastric Cancer |
| GAPPS | Gastric Adenocarcinoma and Proximal Polyposis of the Stomach |
| FIGC | Familial Intestinal Gastric Cancer |
| WHO | World Health Organization |
| NGS | Next-generation sequencing |
| TCGA | Cancer Genome Atlas |
| MSI | Microsatellite Instability |
| GS | Genomically Stable |
| CIN | Chromosomal Instability |
| ACRG | Asian Cancer Research Group |
| MSS/EMT | Microsatellite Stability/Epithelial-Mesenchymal Transition |
| MSS/TP53+ | Microsatellite Stable TP53-active |
| MSS/TP53- | Microsatellite Stable TP53-inactive |
| RR | Relative Risk |
| CI | Confidence Interval |
| HRs | Hazard Ratios |
| ROS | Reactive Oxygen Species |
| HCl | Hydrochloric acid |
| Ach | Acetylcholine |
| CCK | Cholecystokinin |
| OGD | Oesophageal-Gastro-Duodenoscopy |
| CEA | Carcinoembryonic Antigen |
| RNA | Ribonucleic Acid |
| DNA | Deoxyribonucleic Acid |
| ncRNAs | Non-coding RNAs |
| piRNAs | Piwi-interacting RNAs |
| lncRNA | Long Non-coding RNAs |
| miRNAs | MicroRNAs |
| TMT/iTRAQ | Isobaric Tag Relative Absolute Quantitation and Tandem Mass Tags |
| PCR | Polymerase Chain Reaction |
| PEA | Proximity Extension Assay |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Colquhoun, A.; Arnold, M.; Ferlay, J.; Goodman, K.J.; Forman, D.; Soerjomataram, I. Global Patterns of Cardia and Non-Cardia Gastric Cancer Incidence in 2012. Gut 2015, 64, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Morais, S.; Costa, A.; Albuquerque, G.; Araújo, N.; Tsugane, S.; Hidaka, A.; Hamada, G.S.; Ye, W.; Plymoth, A.; Leja, M.; et al. “True” Helicobacter pylori Infection and Non-cardia Gastric Cancer: A Pooled Analysis within the Stomach Cancer Pooling (StoP) Project. Helicobacter 2022, 27, e12883. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Arnold, M.; Camargo, M.C.; Gini, A.; Kunzmann, A.T.; Matsuda, T.; Meheus, F.; Verhoeven, R.H.A.; Vignat, J.; Laversanne, M.; et al. The Current and Future Incidence and Mortality of Gastric Cancer in 185 Countries, 2020–2040: A Population-Based Modelling Study. EClinicalMedicine 2022, 47, 101404. [Google Scholar] [CrossRef]
- Karimi, P.; Islami, F.; Anandasabapathy, S.; Freedman, N.D.; Kamangar, F. Gastric Cancer: Descriptive Epidemiology, Risk Factors, Screening, and Prevention. Cancer Epidemiol. Biomark. Prev. 2014, 23, 700–713. [Google Scholar] [CrossRef]
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric Cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef]
- Oliveira, C.; Pinheiro, H.; Figueiredo, J.; Seruca, R.; Carneiro, F. Familial Gastric Cancer: Genetic Susceptibility, Pathology, and Implications for Management. Lancet Oncol. 2015, 16, e60–e70. [Google Scholar] [CrossRef]
- Li, Y.; Feng, A.; Zheng, S.; Chen, C.; Lyu, J. Recent Estimates and Predictions of 5-Year Survival in Patients with Gastric Cancer: A Model-Based Period Analysis. Cancer Control 2022, 29, 107327482210992. [Google Scholar] [CrossRef]
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Lopes, C.; Chaves, J.; Ortigão, R.; Dinis-Ribeiro, M.; Pereira, C. Gastric Cancer Detection by Non-blood-based Liquid Biopsies: A Systematic Review Looking into the Last Decade of Research. United Eur. Gastroenterol. J. 2023, 11, 114–130. [Google Scholar] [CrossRef] [PubMed]
- Chia, N.-Y.; Tan, P. Molecular Classification of Gastric Cancer. Ann. Oncol. 2016, 27, 763–769. [Google Scholar] [CrossRef]
- Wang, H.; Ding, Y.; Chen, Y.; Jiang, J.; Chen, Y.; Lu, J.; Kong, M.; Mo, F.; Huang, Y.; Zhao, W.; et al. A Novel Genomic Classification System of Gastric Cancer via Integrating Multidimensional Genomic Characteristics. Gastric Cancer 2021, 24, 1227–1241. [Google Scholar] [CrossRef]
- Comprehensive Molecular Characterization of Gastric Adenocarcinoma. Nature 2014, 513, 202–209. [CrossRef]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular Analysis of Gastric Cancer Identifies Subtypes Associated with Distinct Clinical Outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef]
- Ajani, J.A.; Lee, J.; Sano, T.; Janjigian, Y.Y.; Fan, D.; Song, S. Gastric Adenocarcinoma. Nat. Rev. Dis. Prim. 2017, 3, 17036. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori Infection—The Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Ansari, S.; Yamaoka, Y. Helicobacter pylori Virulence Factors Exploiting Gastric Colonization and Its Pathogenicity. Toxins 2019, 11, 677. [Google Scholar] [CrossRef] [PubMed]
- Khoder, G.; Muhammad, J.; Mahmoud, I.; Soliman, S.; Burucoa, C. Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates. Pathogens 2019, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef]
- Yang, L.; Kartsonaki, C.; Yao, P.; de Martel, C.; Plummer, M.; Chapman, D.; Guo, Y.; Clark, S.; Walters, R.G.; Chen, Y.; et al. The Relative and Attributable Risks of Cardia and Non-Cardia Gastric Cancer Associated with Helicobacter pylori Infection in China: A Case-Cohort Study. Lancet Public Health 2021, 6, e888–e896. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Wang, S.; Xue, L.; Middleton, D.R.S.; Guan, C.; Hao, C.; Wang, J.; Li, B.; Chen, R.; Li, X.; et al. Helicobacter pylori Is Associated with Precancerous and Cancerous Lesions of the Gastric Cardia Mucosa: Results of a Large Population-Based Study in China. Front. Oncol. 2020, 10, 205. [Google Scholar] [CrossRef]
- Cavaleiro-Pinto, M.; Peleteiro, B.; Lunet, N.; Barros, H. Helicobacter pylori Infection and Gastric Cardia Cancer: Systematic Review and Meta-Analysis. Cancer Causes Control 2011, 22, 375–387. [Google Scholar] [CrossRef]
- Graham, D.Y. Helicobacter pylori Update: Gastric Cancer, Reliable Therapy, and Possible Benefits. Gastroenterology 2015, 148, 719–731.e3. [Google Scholar] [CrossRef] [PubMed]
- Baj, J.; Forma, A.; Sitarz, M.; Portincasa, P.; Garruti, G.; Krasowska, D.; Maciejewski, R. Helicobacter pylori Virulence Factors—Mechanisms of Bacterial Pathogenicity in the Gastric Microenvironment. Cells 2020, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Takahashi-Kanemitsu, A.; Knight, C.T.; Hatakeyama, M. Molecular Anatomy and Pathogenic Actions of Helicobacter pylori CagA That Underpin Gastric Carcinogenesis. Cell. Mol. Immunol. 2020, 17, 50–63. [Google Scholar] [CrossRef]
- Ribeiro, J.; Oliveira, A.; Malta, M.; Oliveira, C.; Silva, F.; Galaghar, A.; Afonso, L.P.; Neves, M.C.; Medeiros, R.; Pimentel-Nunes, P.; et al. Clinical and Pathological Characterization of Epstein-Barr Virus-Associated Gastric Carcinomas in Portugal. World J. Gastroenterol. 2017, 23, 7292–7302. [Google Scholar] [CrossRef]
- Tavakoli, A.; Monavari, S.H.; Solaymani Mohammadi, F.; Kiani, S.J.; Armat, S.; Farahmand, M. Association between Epstein-Barr Virus Infection and Gastric Cancer: A Systematic Review and Meta-Analysis. BMC Cancer 2020, 20, 493. [Google Scholar] [CrossRef] [PubMed]
- Naseem, M.; Barzi, A.; Brezden-Masley, C.; Puccini, A.; Berger, M.D.; Tokunaga, R.; Battaglin, F.; Soni, S.; McSkane, M.; Zhang, W.; et al. Outlooks on Epstein-Barr Virus Associated Gastric Cancer. Cancer Treat. Rev. 2018, 66, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki-Ushiku, A.; Kunita, A.; Fukayama, M. Update on Epstein-Barr Virus and Gastric Cancer (Review). Int. J. Oncol. 2015, 46, 1421–1434. [Google Scholar] [CrossRef]
- Schubert, M.L.; Peura, D.A. Control of Gastric Acid Secretion in Health and Disease. Gastroenterology 2008, 134, 1842–1860. [Google Scholar] [CrossRef]
- Schubert, M.L. Hormonal Regulation of Gastric Acid Secretion. Curr. Gastroenterol. Rep. 2008, 10, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Verbeure, W.; van Goor, H.; Mori, H.; van Beek, A.P.; Tack, J.; van Dijk, P.R. The Role of Gasotransmitters in Gut Peptide Actions. Front. Pharmacol. 2021, 12, 720703. [Google Scholar] [CrossRef]
- Afroze, S.; Meng, F.; Jensen, K.; McDaniel, K.; Rahal, K.; Onori, P.; Gaudio, E.; Alpini, G.; Glaser, S.S. The Physiological Roles of Secretin and Its Receptor. Ann. Transl. Med. 2013, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Pariente, C.; Montori, S.; Llach, J.; Bofill, A.; Albeniz, E.; Moreira, L. Biomarkers for Gastric Cancer Screening and Early Diagnosis. Biomedicines 2021, 9, 1448. [Google Scholar] [CrossRef]
- Liu, X.; Meltzer, S.J. Gastric Cancer in the Era of Precision Medicine. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 348–358. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Fossmark, R.; Waldum, H.L. The Phylogeny and Biological Function of Gastric Juice-Microbiological Consequences of Removing Gastric Acid. Int. J. Mol. Sci. 2019, 20, 6031. [Google Scholar] [CrossRef]
- Virgilio, E.; Giarnieri, E.; Giovagnoli, M.R.; Montagnini, M.; Proietti, A.; D’Urso, R.; Mercantini, P.; Balducci, G.; Cavallini, M. Gastric Juice MicroRNAs as Potential Biomarkers for Screening Gastric Cancer: A Systematic Review. Anticancer Res. 2018, 38, 613–616. [Google Scholar] [CrossRef]
- Li, P.-F.; Chen, S.-C.; Xia, T.; Jiang, X.-M.; Shao, Y.-F.; Xiao, B.-X.; Guo, J.-M. Non-Coding RNAs and Gastric Cancer. World J. Gastroenterol. 2014, 20, 5411–5419. [Google Scholar] [CrossRef]
- Zhang, X.; Cui, L.; Ye, G.; Zheng, T.; Song, H.; Xia, T.; Yu, X.; Xiao, B.; Le, Y.; Guo, J. Gastric Juice MicroRNA-421 Is a New Biomarker for Screening Gastric Cancer. Tumour Biol. 2012, 33, 2349–2355. [Google Scholar] [CrossRef]
- Yu, X.; Luo, L.; Wu, Y.; Yu, X.; Liu, Y.; Yu, X.; Zhao, X.; Zhang, X.; Cui, L.; Ye, G.; et al. Gastric Juice MiR-129 as a Potential Biomarker for Screening Gastric Cancer. Med. Oncol. 2013, 30, 365. [Google Scholar] [CrossRef]
- Cui, L.; Zhang, X.; Ye, G.; Zheng, T.; Song, H.; Deng, H.; Xiao, B.; Xia, T.; Yu, X.; Le, Y.; et al. Gastric Juice MicroRNAs as Potential Biomarkers for the Screening of Gastric Cancer. Cancer 2013, 119, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Fang, P.-H.; He, B.; Guo, L.-L.; Shi, M.-Y.; Zhu, Y.; Bo, P.; Zhen-Wen, Z.-W. Downregulated MicroRNA-133a in Gastric Juice as a Clinicopathological Biomarker for Gastric Cancer Screening. Asian Pac. J. Cancer Prev. 2016, 17, 2719–2722. [Google Scholar] [PubMed]
- Shi, S.; Yang, Z.-Z.; Liu, S.; Yang, F.; Lin, H. PIWIL1 Promotes Gastric Cancer via a PiRNA-Independent Mechanism. Proc. Natl. Acad. Sci. USA 2020, 117, 22390–22401. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, J.; Meng, A.; Zhang, L.; Wang, M.; Fan, H.; Peng, W.; Lu, J. Gastric Juice PiR-1245: A Promising Prognostic Biomarker for Gastric Cancer. J. Clin. Lab. Anal. 2020, 34, e23131. [Google Scholar] [CrossRef]
- Pang, Q.; Ge, J.; Shao, Y.; Sun, W.; Song, H.; Xia, T.; Xiao, B.; Guo, J. Increased Expression of Long Intergenic Non-Coding RNA LINC00152 in Gastric Cancer and Its Clinical Significance. Tumour Biol. 2014, 35, 5441–5447. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Ye, M.; Jiang, X.; Sun, W.; Ding, X.; Liu, Z.; Ye, G.; Zhang, X.; Xiao, B.; Guo, J. Gastric Juice Long Noncoding RNA Used as a Tumor Marker for Screening Gastric Cancer. Cancer 2014, 120, 3320–3328. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Ye, M.; Li, Q.; Sun, W.; Ye, G.; Zhang, X.; Yang, Y.; Xiao, B.; Guo, J. LncRNA-RMRP Promotes Carcinogenesis by Acting as a MiR-206 Sponge and Is Used as a Novel Biomarker for Gastric Cancer. Oncotarget 2016, 7, 37812–37824. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shao, Y.; Zhu, M.; Li, Q.; Yang, F.; Lu, X.; Xu, C.; Xiao, B.; Sun, Y.; Guo, J. Using Gastric Juice LncRNA-ABHD11-AS1 as a Novel Type of Biomarker in the Screening of Gastric Cancer. Tumour Biol. 2016, 37, 1183–1188. [Google Scholar] [CrossRef]
- Fei, Z.-H.; Yu, X.-J.; Zhou, M.; Su, H.-F.; Zheng, Z.; Xie, C.-Y. Upregulated Expression of Long Non-Coding RNA LINC00982 Regulates Cell Proliferation and Its Clinical Relevance in Patients with Gastric Cancer. Tumour Biol. 2016, 37, 1983–1993. [Google Scholar] [CrossRef]
- Chen, J.S.; Wang, Y.F.; Zhang, X.Q.; Lv, J.M.; Li, Y.; Liu, X.X.; Xu, T.P. H19 Serves as a Diagnostic Biomarker and Up-Regulation of H19 Expression Contributes to Poor Prognosis in Patients with Gastric Cancer. Neoplasma 2016, 63, 223–230. [Google Scholar] [CrossRef]
- Zheng, Q.; Wu, F.; Dai, W.-Y.; Zheng, D.-C.; Zheng, C.; Ye, H.; Zhou, B.; Chen, J.-J.; Chen, P. Aberrant Expression of UCA1 in Gastric Cancer and Its Clinical Significance. Clin. Transl. Oncol. 2015, 17, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Watanabe, Y.; Sato, Y.; Maehata, T.; Itoh, F. Non-Invasive Early Molecular Detection of Gastric Cancers. Cancers 2020, 12, 2880. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Watanabe, Y.; Oikawa, R.; Morita, R.; Yoshida, Y.; Maehata, T.; Yasuda, H.; Itoh, F. BARHL2 Methylation Using Gastric Wash DNA or Gastric Juice Exosomal DNA Is a Useful Marker for Early Detection of Gastric Cancer in an H. Pylori-Independent Manner. Clin. Transl. Gastroenterol. 2016, 7, e184. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-I.; Chen, C.-H.; Hsieh, C.-S.; Chang, W.-C.; Lai, K.-H.; Lo, G.-H.; Hsu, P.-N.; Tsay, F.-W.; Chen, Y.-S.; Hsiao, M.; et al. Alpha1-Antitrypsin Precursor in Gastric Juice Is a Novel Biomarker for Gastric Cancer and Ulcer. Clin. Cancer Res. 2007, 13, 876–883. [Google Scholar] [CrossRef]
- Lee, K.; Kye, M.; Jang, J.S.; Lee, O.J.; Kim, T.; Lim, D. Proteomic Analysis Revealed a Strong Association of a High Level of Alpha1-Antitrypsin in Gastric Juice with Gastric Cancer. Proteomics 2004, 4, 3343–3352. [Google Scholar] [CrossRef]
- Leal, M.F.; Wisnieski, F.; de Oliveira Gigek, C.; do Santos, L.C.; Calcagno, D.Q.; Burbano, R.R.; Smith, M.C. What Gastric Cancer Proteomic Studies Show about Gastric Carcinogenesis? Tumour Biol. 2016, 37, 9991–10010. [Google Scholar] [CrossRef]
- Mohri, Y.; Toiyama, Y.; Kusunoki, M. Progress and Prospects for the Discovery of Biomarkers for Gastric Cancer: A Focus on Proteomics. Expert. Rev. Proteom. 2016, 13, 1131–1139. [Google Scholar] [CrossRef]
- Kang, C.; Lee, Y.; Lee, J.E. Recent Advances in Mass Spectrometry-Based Proteomics of Gastric Cancer. World J. Gastroenterol. 2016, 22, 8283–8293. [Google Scholar] [CrossRef]
- Shi, W.; Wang, Y.; Xu, C.; Li, Y.; Ge, S.; Bai, B.; Zhang, K.; Wang, Y.; Zheng, N.; Wang, J.; et al. Multilevel Proteomic Analyses Reveal Molecular Diversity between Diffuse-Type and Intestinal-Type Gastric Cancer. Nat. Commun. 2023, 14, 835. [Google Scholar] [CrossRef]
- Wu, W.; Chung, M.C.M. The Gastric Fluid Proteome as a Potential Source of Gastric Cancer Biomarkers. J. Proteom. 2013, 90, 3–13. [Google Scholar] [CrossRef]
- Kam, S.Y.; Hennessy, T.; Chua, S.C.; Gan, C.S.; Philp, R.; Hon, K.K.; Lai, L.; Chan, W.H.; Ong, H.S.; Wong, W.K.; et al. Characterization of the Human Gastric Fluid Proteome Reveals Distinct PH-Dependent Protein Profiles: Implications for Biomarker Studies. J. Proteome Res. 2011, 10, 4535–4546. [Google Scholar] [CrossRef] [PubMed]
- Ito, G.; Kaneko, E.; Sakakibara, T.; Takeuchi, Y.; Kitahara, H.; Kobashi, H.; Araki, A.; Tokunaga, T.; Hasegawa, J.; Kobayashi, N.; et al. The PH Measurement of Fasting Gastric Juice in Acute Gastric Mucosal Lesions. Dig. Endosc. 1989, 1, 10–17. [Google Scholar] [CrossRef]
- Lu, P.-J.; Hsu, P.-I.; Chen, C.-H.; Hsiao, M.; Chang, W.-C.; Tseng, H.-H.; Lin, K.-H.; Chuah, S.-K.; Chen, H.-C. Gastric Juice Acidity in Upper Gastrointestinal Diseases. World J. Gastroenterol. 2010, 16, 5496–5501. [Google Scholar] [CrossRef] [PubMed]
- Cheney, G.; Bloomfield, A.L. Gastric Function in Cases of Gastric and Duodenal Ulcer. J. Clin. Invest. 1928, 5, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Apperly, F.L. Gastric Acidity and its Significance. Lancet 1936, 227, 5–10. [Google Scholar] [CrossRef]
- Furuta, T.; Baba, S.; Takashima, M.; Futami, H.; Arai, H.; Kajimura, M.; Hanai, H.; Kaneko, E. Effect of Helicobacter pylori Infection on Gastric Juice PH. Scand. J. Gastroenterol. 1998, 33, 357–363. [Google Scholar] [CrossRef]
- Kon, O.L.; Yip, T.-T.; Ho, M.F.; Chan, W.H.; Wong, W.K.; Tan, S.Y.; Ng, W.H.; Kam, S.Y.; Eng, A.K.; Ho, P.; et al. The Distinctive Gastric Fluid Proteome in Gastric Cancer Reveals a Multi-Biomarker Diagnostic Profile. BMC Med. Genom. 2008, 1, 54. [Google Scholar] [CrossRef]
- Chang, W.-C.; Hsu, P.-I.; Chen, Y.-Y.; Hsiao, M.; Lu, P.-J.; Chen, C.-H. Observation of Peptide Differences between Cancer and Control in Gastric Juice. Proteom. Clin. Appl. 2008, 2, 55–62. [Google Scholar] [CrossRef]
- Tan, S.; Liang, C.R.M.Y.; Yeoh, K.G.; So, J.; Hew, C.L.; Chung, M.C.M. Gastrointestinal Fluids Proteomics. Proteom. Clin. Appl. 2007, 1, 820–833. [Google Scholar] [CrossRef]
- Brenes, A.; Hukelmann, J.; Bensaddek, D.; Lamond, A.I. Multibatch TMT Reveals False Positives, Batch Effects and Missing Values. Mol. Cell. Proteom. 2019, 18, 1967–1980. [Google Scholar] [CrossRef]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Björkesten, J.; Thorsen, S.B.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-Plex PEA Immunoassay Exhibiting High Sensitivity, Specificity, and Excellent Scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Gu, Y.; Shi, Z.; Min, L.; Zhang, Z.; Zhou, P.; Luo, R.; Wang, Y.; Cui, Y.; Sun, Y.; et al. Multiplex Immune Profiling Reveals the Role of Serum Immune Proteomics in Predicting Response to Preoperative Chemotherapy of Gastric Cancer. Cell. Rep. Med. 2023, 4, 100931. [Google Scholar] [CrossRef] [PubMed]
- Camargo, M.C.; Song, M.; Sawada, N.; Inoue, M.; Shimazu, T.; Charvat, H.; Pfeiffer, R.M.; Yamaji, T.; Tsugane, S.; Rabkin, C.S. Prediagnostic Circulating Inflammation-Related Biomarkers and Gastric Cancer: A Case-Cohort Study in Japan. Cytokine 2021, 144, 155558. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Rabkin, C.S.; Ito, H.; Oze, I.; Koyanagi, Y.N.; Pfeiffer, R.M.; Kasugai, Y.; Matsuo, K.; Camargo, M.C. Circulating Immune- and Inflammation-Related Biomarkers and Early-Stage Noncardia Gastric Cancer Risk. Eur. J. Cancer Prev. 2022, 31, 270–273. [Google Scholar] [CrossRef]
- Shen, Q.; Polom, K.; Williams, C.; de Oliveira, F.M.S.; Guergova-Kuras, M.; Lisacek, F.; Karlsson, N.G.; Roviello, F.; Kamali-Moghaddam, M. A Targeted Proteomics Approach Reveals a Serum Protein Signature as Diagnostic Biomarker for Resectable Gastric Cancer. EBioMedicine 2019, 44, 322–333. [Google Scholar] [CrossRef]
- Camargo, M.C.; Sivins, A.; Isajevs, S.; Folkmanis, V.; Rudzīte, D.; Gulley, M.L.; Offerhaus, G.J.; Leja, M.; Rabkin, C.S. Associations of Epstein-Barr Virus-Positive Gastric Adenocarcinoma with Circulating Mediators of Inflammation and Immune Response. Cancers 2018, 10, 284. [Google Scholar] [CrossRef]
- Tin, A.; Yu, B.; Ma, J.; Masushita, K.; Daya, N.; Hoogeveen, R.C.; Ballantyne, C.M.; Couper, D.; Rebholz, C.M.; Grams, M.E.; et al. Reproducibility and Variability of Protein Analytes Measured Using a Multiplexed Modified Aptamer Assay. J. Appl. Lab. Med. 2019, 4, 30–39. [Google Scholar] [CrossRef]
- Bowker, N.; Hansford, R.; Burgess, S.; Foley, C.N.; Auyeung, V.P.W.; Erzurumluoglu, A.M.; Stewart, I.D.; Wheeler, E.; Pietzner, M.; Gribble, F.; et al. Genetically Predicted Glucose-Dependent Insulinotropic Polypeptide (GIP) Levels and Cardiovascular Disease Risk Are Driven by Distinct Causal Variants in the GIPR Region. Diabetes 2021, 70, 2706–2719. [Google Scholar] [CrossRef]
- Dreyfuss, J.M.; Yuchi, Y.; Dong, X.; Efthymiou, V.; Pan, H.; Simonson, D.C.; Vernon, A.; Halperin, F.; Aryal, P.; Konkar, A.; et al. High-Throughput Mediation Analysis of Human Proteome and Metabolome Identifies Mediators of Post-Bariatric Surgical Diabetes Control. Nat. Commun. 2021, 12, 6951. [Google Scholar] [CrossRef]
- Mulla, C.M.; Goldfine, A.B.; Dreyfuss, J.M.; Houten, S.; Pan, H.; Pober, D.M.; Wewer Albrechtsen, N.J.; Svane, M.S.; Schmidt, J.B.; Holst, J.J.; et al. Plasma FGF-19 Levels Are Increased in Patients with Post-Bariatric Hypoglycemia. Obes. Surg. 2019, 29, 2092–2099. [Google Scholar] [CrossRef]
- Yousri, N.A.; Engelke, R.; Sarwath, H.; McKinlay, R.D.; Simper, S.C.; Adams, T.D.; Schmidt, F.; Suhre, K.; Hunt, S.C. Proteome-Wide Associations with Short- and Long-Term Weight Loss and Regain after Roux-En-Y Gastric Bypass Surgery. Obesity 2022, 30, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Grover, M.; Dasari, S.; Bernard, C.E.; Chikkamenahalli, L.L.; Yates, K.P.; Pasricha, P.J.; Sarosiek, I.; McCallum, R.; Koch, K.L.; Abell, T.L.; et al. Proteomics in Gastroparesis: Unique and Overlapping Protein Signatures in Diabetic and Idiopathic Gastroparesis. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 317, G716–G726. [Google Scholar] [CrossRef]
- Dammer, E.B.; Ping, L.; Duong, D.M.; Modeste, E.S.; Seyfried, N.T.; Lah, J.J.; Levey, A.I.; Johnson, E.C.B. Multi-Platform Proteomic Analysis of Alzheimer’s Disease Cerebrospinal Fluid and Plasma Reveals Network Biomarkers Associated with Proteostasis and the Matrisome. Alzheimers Res. Ther. 2022, 14, 174. [Google Scholar] [CrossRef]
- Pietzner, M.; Wheeler, E.; Carrasco-Zanini, J.; Kerrison, N.D.; Oerton, E.; Koprulu, M.; Luan, J.; Hingorani, A.D.; Williams, S.A.; Wareham, N.J.; et al. Synergistic Insights into Human Health from Aptamer- and Antibody-Based Proteomic Profiling. Nat. Commun. 2021, 12, 6822. [Google Scholar] [CrossRef]
- Raffield, L.M.; Dang, H.; Pratte, K.A.; Jacobson, S.; Gillenwater, L.A.; Ampleford, E.; Barjaktarevic, I.; Basta, P.; Clish, C.B.; Comellas, A.P.; et al. Comparison of Proteomic Assessment Methods in Multiple Cohort Studies. Proteomics 2020, 20, e1900278. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.H.; Tahir, U.A.; Bick, A.G.; Pampana, A.; Ngo, D.; Benson, M.D.; Yu, Z.; Robbins, J.M.; Chen, Z.-Z.; Cruz, D.E.; et al. Whole Genome Sequence Analysis of the Plasma Proteome in Black Adults Provides Novel Insights into Cardiovascular Disease. Circulation 2022, 145, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Finkernagel, F.; Reinartz, S.; Schuldner, M.; Malz, A.; Jansen, J.M.; Wagner, U.; Worzfeld, T.; Graumann, J.; von Strandmann, E.P.; Müller, R. Dual-Platform Affinity Proteomics Identifies Links between the Recurrence of Ovarian Carcinoma and Proteins Released into the Tumor Microenvironment. Theranostics 2019, 9, 6601–6617. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.R.M.Y.; Tan, S.; Tan, H.T.; Lin, Q.; Lim, T.K.; Liu, Y.; Yeoh, K.G.; So, J.; Chung, M.C.M. Proteomic Analysis of Human Gastric Juice: A Shotgun Approach. Proteomics 2010, 10, 3928–3931. [Google Scholar] [CrossRef]
- Wu, W.; Yong, W.W.; Chung, M.C.M. A Simple Biomarker Scoring Matrix for Early Gastric Cancer Detection. Proteomics 2016, 16, 2921–2930. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felípez, N.; Montori, S.; Mendizuri, N.; Llach, J.; Delgado, P.G.; Moreira, L.; Santamaría, E.; Fernández-Irigoyen, J.; Albéniz, E. The Human Gastric Juice: A Promising Source for Gastric Cancer Biomarkers. Int. J. Mol. Sci. 2023, 24, 9131. https://doi.org/10.3390/ijms24119131
Felípez N, Montori S, Mendizuri N, Llach J, Delgado PG, Moreira L, Santamaría E, Fernández-Irigoyen J, Albéniz E. The Human Gastric Juice: A Promising Source for Gastric Cancer Biomarkers. International Journal of Molecular Sciences. 2023; 24(11):9131. https://doi.org/10.3390/ijms24119131
Chicago/Turabian StyleFelípez, Nayra, Sheyla Montori, Naroa Mendizuri, Joan Llach, Pedro G. Delgado, Leticia Moreira, Enrique Santamaría, Joaquín Fernández-Irigoyen, and Eduardo Albéniz. 2023. "The Human Gastric Juice: A Promising Source for Gastric Cancer Biomarkers" International Journal of Molecular Sciences 24, no. 11: 9131. https://doi.org/10.3390/ijms24119131