
Clinical and Translational Applications of Serological and Histopathological Biomarkers in Metastatic Breast Cancer: A Comprehensive Review
 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction. Epidemiology, Diagnosis, Molecular Classification, and Prognosis of Metastatic Breast Cancer
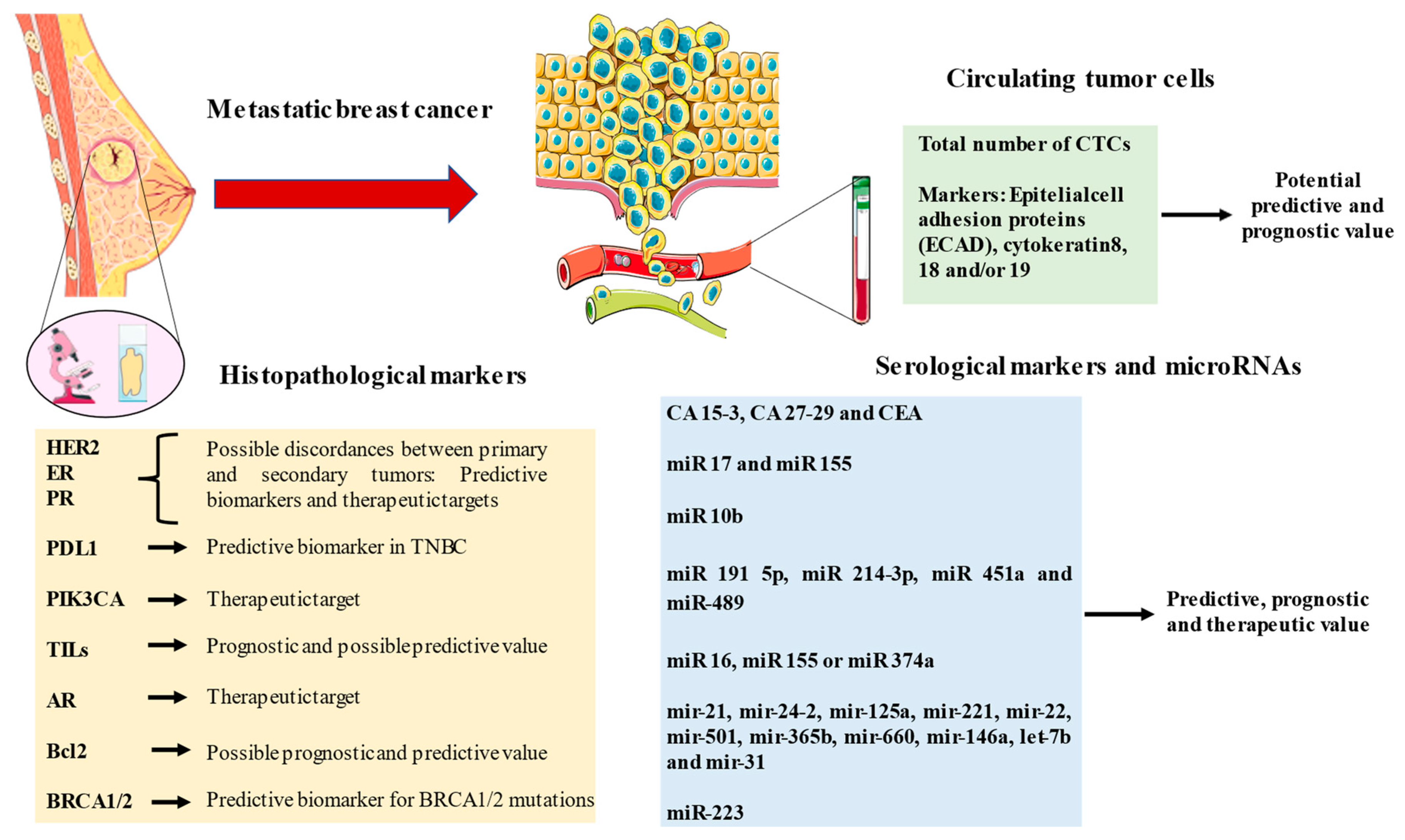
2. Serological Markers in Metastatic Breast Cancer
2.1. Serological CA15-3. Most Clinical Marker Used in MBC
2.2. Serological CA 27-29. Supporting Serological Monitoring
3. Histological Markers
3.1. HER 2. The First Steps of Targeted Therapy in MBC
3.2. PD-L1. The Role of Immunotherapy in MBC
3.3. PIK3CA. The Role of Kinases in MBC
3.4. The Uncommon Markers. Tumor-Infiltrating Lymphocytes, Androgen Receptors, and BCL2
3.5. ADH and ALDH in MBC and Their Potential Use
3.6. BRCA Mutations in MBC. Their Role in Genetic and Hereditary Breast Cancer
4. MicroRNA. Implications in Diagnosis and Prognosis
5. Circulating Tumor Cells. Liquid Biopsy
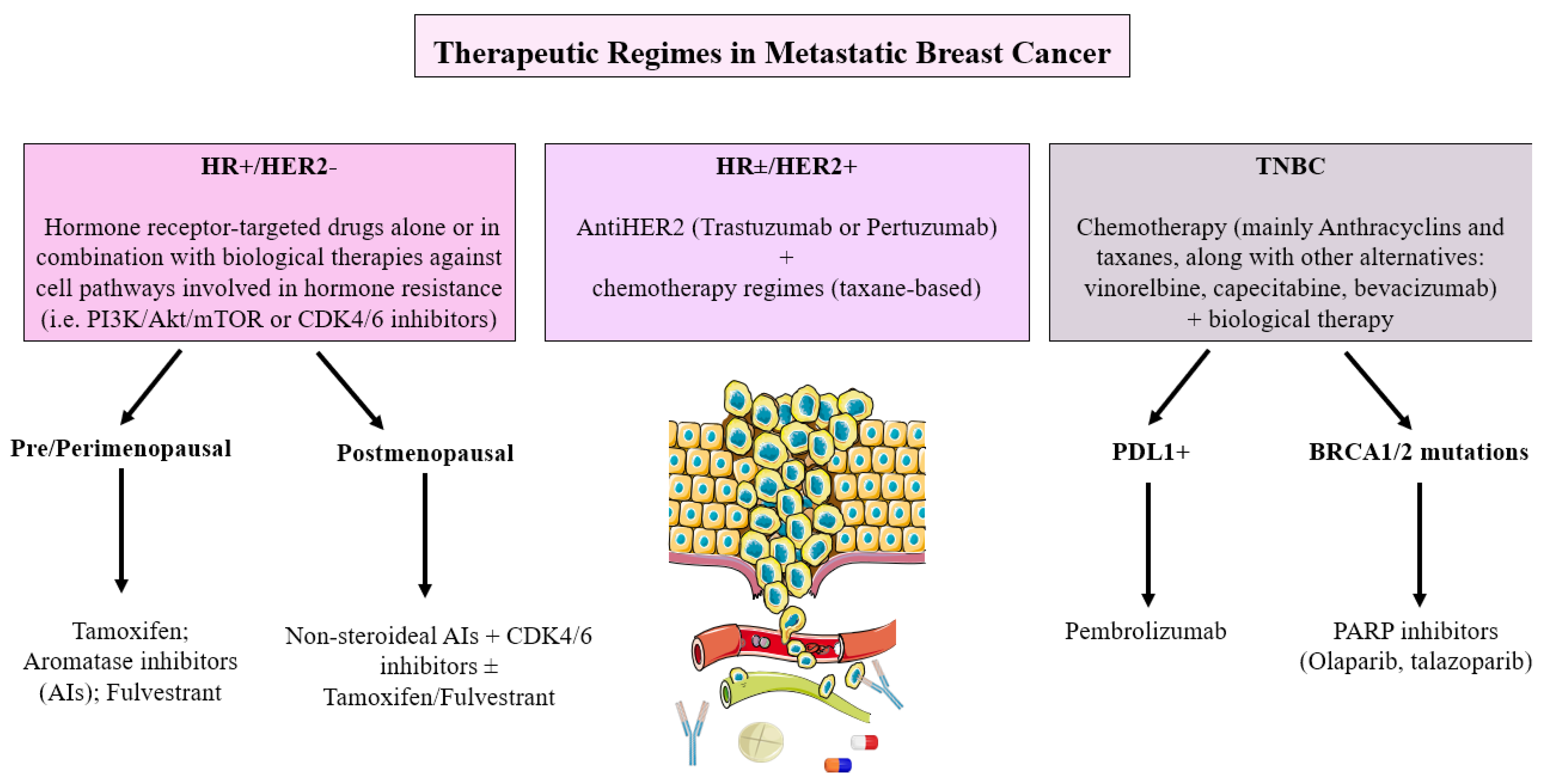
6. Current Therapeutic Decisions Based on the Different Biomarkers in Metastatic Breast Cancer
6.1. Hormone Receptor-Positive/HER2-Negative Metastatic Breast Cancer
6.2. HER2 Positive Metastatic Breast Cancer
6.3. Triple-Negative Metastatic Breast Cancer
6.4. BRCA1/BRCA2 Metastatic Breast Cancer
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giaquinto, A.N.; Sung, H.; Miller, K.D.; Kramer, J.L.; Newman, L.A.; Minihan, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 524–541. [Google Scholar] [CrossRef]
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef]
- Gorasso, V.; Silversmit, G.; Arbyn, M.; Cornez, A.; De Pauw, R.; De Smedt, D.; Grant, I.; Wyper, G.M.A.; Devleesschauwer, B.; Speybroeck, N. The non-fatal burden of cancer in Belgium, 2004–2019: A nationwide registry-based study. BMC Cancer 2022, 22, 58. [Google Scholar] [CrossRef]
- Zaheer, S.; Shah, N.; Maqbool, S.A.; Soomro, N.M. Estimates of past and future time trends in age-specific breast cancer incidence among women in Karachi, Pakistan: 2004–2025. BMC Public Health 2019, 19, 1001. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, M.; Ciszewski, T.; Łopacka-Szatan, K.; Miotła, P.; Starosławska, E. Breast cancer risk factors. Menopausal Rev. 2015, 3, 196–202. [Google Scholar] [CrossRef]
- Collins, A. The genetics of breast cancer: Risk factors for disease. Appl. Clin. Genet. 2011, 4, 11–19. [Google Scholar] [CrossRef]
- Jiralerspong, S.; Goodwin, P. Obesity and Breast Cancer Prognosis: Evidence, Challenges, and Opportunities. J. Clin. Oncol. 2016, 34, 4203–4216. [Google Scholar] [CrossRef]
- Freudenheim, J.L. Alcohols Effects on Breast Cancer in Women. Alcohol Res. Curr. Rev. 2020, 40, 11. [Google Scholar] [CrossRef]
- Vinogradova, Y.; Coupland, C.; Hippisley-Cox, J. Use of hormone replacement therapy and risk of breast cancer: Nested case-control studies using the QResearch and CPRD databases. BMJ 2020, 371, m3873. [Google Scholar] [CrossRef] [PubMed]
- Soori, M.; Platz, E.A.; Brawley, O.W.; Lawrence, R.S.; Kanarek, N.F. Inclusion of the US Preventive Services Task Force Recommendation for Mammography in State Comprehensive Cancer Control Plans in the US. JAMA Netw. Open 2022, 5, e229706. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Chen, Z.; Tan, M.; Elingarami, S.; Liu, Y.; Li, T.; Deng, Y.; He, N.; Li, S.; Fu, J.; et al. A review on methods for diagnosis of breast cancer cells and tissues. Cell Prolif. 2020, 53, e12822. [Google Scholar] [CrossRef] [PubMed]
- Wang, L. Early Diagnosis of Breast Cancer. Sensors 2017, 17, 1572. [Google Scholar] [CrossRef]
- Smolarz, B.; Nowak, A.Z.; Romanowicz, H. Breast Cancer—Epidemiology, Classification, Pathogenesis and Treatment (Review of Literature). Cancers 2022, 14, 2569. [Google Scholar] [CrossRef]
- Vondeling, G.T.; Menezes, G.L.; Dvortsin, E.P.; Jansman, F.G.A.; Konings, I.R.; Postma, M.J.; Rozenbaum, M.H. Burden of early, advanced and metastatic breast cancer in The Netherlands. BMC Cancer 2018, 18, 262. [Google Scholar] [CrossRef] [PubMed]
- Kapp, A.V.; Jeffrey, S.S.; Langerød, A.; Børresen-Dale, A.-L.; Han, W.; Noh, D.-Y.; Bukholm, I.R.K.; Nicolau, M.; O Brown, P.; Tibshirani, R. Discovery and validation of breast cancer subtypes. BMC Genom. 2006, 7, 231. [Google Scholar] [CrossRef]
- Yersal, O.; Barutca, S. Biological subtypes of breast cancer: Prognostic and therapeutic implications. World J. Clin. Oncol. 2014, 5, 412–424. [Google Scholar] [CrossRef]
- Esteva, F.J.; Hubbard-Lucey, V.M.; Tang, J.; Pusztai, L. Immunotherapy and targeted therapy combinations in metastatic breast cancer. Lancet Oncol. 2019, 20, e175–e186. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Miglietta, F.; Bottosso, M.; Griguolo, G.; Dieci, M.; Guarneri, V. Major advancements in metastatic breast cancer treatment: When expanding options means prolonging survival. ESMO Open 2022, 7, 100409. [Google Scholar] [CrossRef]
- Duffy, M.J. Serum Tumor Markers in Breast Cancer: Are They of Clinical Value? Clin. Chem. 2006, 52, 345–351. [Google Scholar] [CrossRef]
- Desmedt, C.; Voet, T.; Sotiriou, C.; Campbell, P.J. Next-generation sequencing in breast cancer. Curr. Opin. Oncol. 2012, 24, 597–604. [Google Scholar] [CrossRef]
- Couch, F.J.; Shimelis, H.; Hu, C.; Hart, S.N.; Polley, E.C.; Na, J.; Hallberg, E.; Moore, R.; Thomas, A.; Lilyquist, J.; et al. Associations Between Cancer Predisposition Testing Panel Genes and Breast Cancer. JAMA Oncol. 2017, 3, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Nikanjam, M.; Kato, S.; Kurzrock, R. Liquid biopsy: Current technology and clinical applications. J. Hematol. Oncol. 2022, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.M.; Chae, E.Y.; Cha, J.H.; Kim, H.H.; Shin, H.J.; Choi, W.J. Association of BRCA Mutation Types, Imaging Features, and Pathologic Findings in Patients with Breast Cancer with BRCA1 and BRCA2 Mutations. Am. J. Roentgenol. 2017, 209, 920–928. [Google Scholar] [CrossRef]
- Tung, N.; Battelli, C.; Allen, B.; Kaldate, R.; Bhatnagar, S.; Bowles, K.; Timms, K.; Garber, J.E.; Herold, C.; Ellisen, L.; et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer 2014, 121, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Zubair, M.; Wang, S.; Ali, N. Advanced Approaches to Breast Cancer Classification and Diagnosis. Front. Pharmacol. 2021, 11, 632079. [Google Scholar] [CrossRef]
- Lacroix, M. Significance, Detection and Markers of Disseminated Breast Cancer Cells. Endocr.-Relat. Cancer 2006, 13, 1033–1067. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.S.Y.; Sturgeon, C.M.; Seth, J.; Paterson, G.M.; Roulston, J.E.; Leonard, R.C.F. Serological Markers for Metastatic Breast Cancer. Dis. Markers 1993, 11, 217–223. [Google Scholar] [CrossRef]
- Kazarian, A.; Blyuss, O.; Metodieva, G.; Gentry-Maharaj, A.; Ryan, A.; Kiseleva, E.M.; Prytomanova, O.M.; Jacobs, I.J.; Widschwendter, M.; Menon, U.; et al. Testing Breast Cancer Serum Biomarkers for Early Detection and Prognosis in Pre-Diagnosis Samples. Br. J. Cancer 2017, 116, 501–508. [Google Scholar] [CrossRef]
- Tarighati, E.; Keivan, H.; Mahani, H. A review of prognostic and predictive biomarkers in breast cancer. Clin. Exp. Med. 2022, 23, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Heylen, J.; Punie, K.; Smeets, A.; Neven, P.; Weltens, C.; Laenen, A.; Wildiers, H. Elevated CA 15.3 in Newly Diagnosed Breast Cancer: A Retrospective Study. Clin. Breast Cancer 2022, 22, 579–587. [Google Scholar] [CrossRef]
- Hasan, D. Diagnostic impact of CEA and CA 15-3 on monitoring chemotherapy of breast cancer patients. J. Circ. Biomarkers 2022, 11, 57–63. [Google Scholar] [CrossRef] [PubMed]
- De Cock, L.; Heylen, J.; Wildiers, A.; Punie, K.; Smeets, A.; Weltens, C.; Neven, P.; Billen, J.; Laenen, A. Detection of secondary metastatic breast cancer by measurement of plasma CA 15.3. ESMO Open 2021, 6, 100203. [Google Scholar] [CrossRef]
- Goodwin, P.J.; Dowling, R.J.O.; Ennis, M.; Chen, B.E.; Parulekar, W.R.; Shepherd, L.E.; Gelmon, K.A.; Whelan, T.J.; Ligibel, J.A.; Hershman, D.L.; et al. Cancer Antigen 15-3/Mucin 1 Levels in CCTG MA.32: A Breast Cancer Randomized Trial of Metformin vs Placebo. JNCI Cancer Spectr. 2021, 5, pkab066. [Google Scholar] [CrossRef]
- Hepp, P.; Andergassen, U.; Jäger, B.; Trapp, E.; Alunni-Fabbroni, M.; Friedl, T.W.; Hecker, N.; Lorenz, R.; Fasching, P.; Schneeweiss, A.; et al. Association of CA27.29 and Circulating Tumor Cells Before and at Different Times After Adjuvant Chemotherapy in Patients with Early-stage Breast Cancer—The SUCCESS Trial. Anticancer. Res. 2016, 36, 4771–4776. [Google Scholar] [CrossRef]
- Gion, M.; Mione, R.; Leon, A.E.; Lüftner, D.; Molina, R.; Possinger, K.; Robertson, J. CA27.29: A valuable marker for breast cancer management. A confirmatory multicentric study on 603 cases. Eur. J. Cancer 2001, 37, 355–363. [Google Scholar] [CrossRef] [PubMed]
- De Dueñas, E.M.; Hernández, A.L.; Zotano, Á.G.; Carrión, R.M.P.; López-Muñiz, J.I.C.; Novoa, S.A.; Rodríguez, Á.L.; Fidalgo, J.A.P.; Lozano, J.F.; Gasión, O.B.; et al. Prospective evaluation of the conversion rate in the receptor status between primary breast cancer and metastasis: Results from the GEICAM 2009-03 ConvertHER study. Breast Cancer Res. Treat. 2014, 143, 507–515. [Google Scholar] [CrossRef]
- Amir, E.; Clemons, M.; Purdie, C.A.; Miller, N.; Quinlan, P.; Geddie, W.; Coleman, R.E.; Freedman, O.C.; Jordan, L.B.; Thompson, A.M. Tissue confirmation of disease recurrence in breast cancer patients: Pooled analysis of multi-centre, multi-disciplinary prospective studies. Cancer Treat. Rev. 2011, 38, 708–714. [Google Scholar] [CrossRef]
- Knight, W.A.; Livingston, R.B.; Gregory, E.J.; McGuire, W.L. Estrogen receptor as an independent prognostic factor for early recurrence in breast cancer. Cancer Res. 1977, 37, 4669–4671. [Google Scholar]
- Damodaran, S.; Hortobagyi, G.N. Estrogen Receptor: A Paradigm for Targeted Therapy. Cancer Res. 2021, 81, 5396–5398. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.J.; Cheng, J.; Bloomquist, E.; Sanchez, J.; Wedam, S.B.; Singh, H.; Amiri-Kordestani, L.; Ibrahim, A.; Sridhara, R.; Goldberg, K.B.; et al. CDK4/6 inhibitor treatment for patients with hormone receptor-positive, HER2-negative, advanced or metastatic breast cancer: A US Food and Drug Administration pooled analysis. Lancet Oncol. 2020, 21, 250–260. [Google Scholar] [CrossRef]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Baselga, J.; Kim, S.-B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.-M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, Trastuzumab, and Docetaxel in HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.E.; Kim, S.-B.; Martin, A.G.; LoRusso, P.M.; Ferrero, J.-M.; Badovinac-Crnjevic, T.; Hoersch, S.; Smitt, M.; Wildiers, H. Trastuzumab emtansine versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): Final overall survival results from a randomised open-label phase 3 trial. Lancet Oncol. 2017, 18, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Oliveira, M.; Feng, Y.-H.; Dai, M.-S.; Chen, S.-W.; Hurvitz, S.A.; Kim, S.-B.; Moy, B.; Delaloge, S.; Gradishar, W.; et al. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated With ≥ 2 HER2-Directed Regimens: Phase III NALA Trial. J. Clin. Oncol. 2020, 38, 3138–3149. [Google Scholar] [CrossRef]
- A Hurvitz, S.; Hegg, R.; Chung, W.-P.; Im, S.-A.; Jacot, W.; Ganju, V.; Chiu, J.W.Y.; Xu, B.; Hamilton, E.; Madhusudan, S.; et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: Updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet 2022, 401, 105–117. [Google Scholar] [CrossRef]
- Planes-Laine, G.; Rochigneux, P.; Bertucci, F.; Chrétien, A.-S.; Viens, P.; Sabatier, R.; Gonçalves, A. PD-1/PD-L1 Targeting in Breast Cancer: The First Clinical Evidences are Emerging—A Literature Review. Cancers 2019, 11, 1033. [Google Scholar] [CrossRef]
- Oner, G.; Önder, S.; Karatay, H.; Ak, N.; Tükenmez, M.; Müslümanoğlu, M.; Iğci, A.; Dincçağ, A.; Özmen, V.; Aydiner, A.; et al. Clinical impact of PD-L1 expression in triple-negative breast cancer patients with residual tumor burden after neoadjuvant chemotherapy. World J. Surg. Oncol. 2021, 19, 264. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Rugo, H.S.; Cescon, D.W.; Im, S.-A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Perez-Garcia, J.; Iwata, H.; et al. Pembrolizumab plus Chemotherapy in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2022, 387, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Curtis, C.; Shah, S.P.; Chin, S.-F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The genomic and transcriptomic architecture of 2000 breast tumours reveals novel subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Fusco, N.; Malapelle, U.; Fassan, M.; Marchiò, C.; Buglioni, S.; Zupo, S.; Criscitiello, C.; Vigneri, P.; Tos, A.P.D.; Maiorano, E.; et al. PIK3CA Mutations as a Molecular Target for Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer. Front. Oncol. 2021, 11, 644737. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Kensler, K.H.; Regan, M.M.; Heng, Y.J.; Baker, G.M.; Pyle, M.E.; Schnitt, S.J.; Hazra, A.; Kammler, R.; Thürlimann, B.; Colleoni, M.; et al. Prognostic and predictive value of androgen receptor expression in postmenopausal women with estrogen receptor-positive breast cancer: Results from the Breast International Group Trial 1–98. Breast Cancer Res. 2019, 21, 30. [Google Scholar] [CrossRef]
- Jelski, W.; Chrostek, L.; Markiewicz, W.; Szmitkowski, M. Activity of alcohol dehydrogenase (adh) isoenzymes and aldehyde dehydrogenase (ALDH) in the sera of patients with breast cancer. J. Clin. Lab. Anal. 2006, 20, 105–108. [Google Scholar] [CrossRef]
- Jelski, W.; Chrostek, L.; Szmitkowski, M.; Markiewicz, W. The activity of class I, II, III and IV alcohol dehydrogenase isoenzymes and aldehyde dehydrogenase in breast cancer. Clin. Exp. Med. 2006, 6, 89–93. [Google Scholar] [CrossRef]
- Xia, J.; Li, S.; Liu, S.; Zhang, L. Aldehyde dehydrogenase in solid tumors and other diseases: Potential biomarkers and thera-peutic targets. MedComm 2023, 4, e195. [Google Scholar] [CrossRef]
- Wright, R.M.; McManaman, J.L.; Repine, J.E. Alcohol-induced breast cancer: A proposed mechanism. Free. Radic. Biol. Med. 1999, 26, 348–354. [Google Scholar] [CrossRef]
- Narod, S.A. BRCA mutations in the management of breast cancer: The state of the art. Nat. Rev. Clin. Oncol. 2010, 7, 702–707. [Google Scholar] [CrossRef]
- Bordeleau, L.; Panchal, S.; Goodwin, P. Prognosis of BRCA-associated breast cancer: A summary of evidence. Breast Cancer Res. Treat. 2009, 119, 13–24. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Wang, N.; Li, K.; Huang, W.; Kong, W.; Liu, X.; Shi, W.; Xie, F.; Jiang, H.; Song, G.; Di, L.; et al. Efficacy of platinum in advanced triple-negative breast cancer with germline BRCA mutation determined by next generation sequencing. Chin. J. Cancer Res. 2020, 32, 149–162. [Google Scholar] [CrossRef]
- Peng, Y.; Croce, C.M. The role of MicroRNAs in human cancer. Signal Transduct. Target. Ther. 2016, 1, 15004. [Google Scholar] [CrossRef]
- McGuire, A.; Brown, J.A.L.; Kerin, M.J. Metastatic breast cancer: The potential of miRNA for diagnosis and treatment monitoring. Cancer Metastasis Rev. 2015, 34, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Asaga, S.; Kuo, C.; Nguyen, T.; Terpenning, M.; Giuliano, A.E.; Hoon, D.S.B. Direct Serum Assay for MicroRNA-21 Concen-trations in Early and Advanced Breast Cancer. Clin. Chem. 2011, 57, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenbach, H.; Milde-Langosch, K.; Steinbach, B.; Müller, V.; Pantel, K. Diagnostic potential of PTEN-targeting miR-214 in the blood of breast cancer patients. Breast Cancer Res. Treat. 2012, 134, 933–941. [Google Scholar] [CrossRef]
- Eichelser, C.; Flesch-Janys, D.; Chang-Claude, J.; Pantel, K.; Schwarzenbach, H. Deregulated Serum Concentrations of Circulating Cell–Free MicroRNAs miR-17, miR-34a, miR-155, and miR-373 in Human Breast Cancer Development and Progression. Clin. Chem. 2013, 59, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.-L.; Hu, G.-D.; Wang, X.-F.; Zhang, X.-H.; Zhang, Y.-K.; Yu, Z.-S. Serum Overexpression of MicroRNA-10b in Patients with Bone Metastatic Primary Breast Cancer. J. Int. Med. Res. 2012, 40, 859–866. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Y.-W.; Zhu, W.-J.; Li, Y.; Liu, L.; Yin, G.; Gao, P. A 4-microRNA signature predicts lymph node metastasis and prognosis in breast cancer. Hum. Pathol. 2018, 76, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Cascione, L.; Gasparini, P.; Lovat, F.; Carasi, S.; Pulvirenti, A.; Ferro, A.; Alder, H.; He, G.; Vecchione, A.; Croce, C.M.; et al. Integrated MicroRNA and mRNA Signatures Associated with Survival in Triple Negative Breast Cancer. PLoS ONE 2013, 8, e55910. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, P.; Cascione, L.; Fassan, M.; Lovat, F.; Guler, G.; Balci, S.; Irkkan, C.; Morrison, C.; Croce, C.M.; Shapiro, C.L.; et al. microRNA expression profiling identifies a four microRNA signature as a novel diagnostic and prognostic biomarker in triple negative breast cancers. Oncotarget 2014, 5, 1174–1184. [Google Scholar] [CrossRef]
- Jayasingam, S.D.; Citartan, M.; Zin, A.A.M.; Rozhdestvensky, T.S.; Tang, T.-H.; Ch’ng, E.S. An Eleven-microRNA Signature Related to Tumor-Associated Macrophages Predicts Prognosis of Breast Cancer. Int. J. Mol. Sci. 2022, 23, 6994. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: Biology and clinical significance. Signal Transduct. Target. Ther. 2021, 6, 404. [Google Scholar] [CrossRef]
- Parise, C.A.; Bauer, K.R.; Brown, M.M.; Caggiano, V. Breast Cancer Subtypes as Defined by the Estrogen Receptor (ER), Progesterone Receptor (PR), and the Human Epidermal Growth Factor Receptor 2 (HER2) among Women with Invasive Breast Cancer in California, 1999-2004. Breast J. 2009, 15, 593–602. [Google Scholar] [CrossRef]
- Castro-Giner, F.; Aceto, N. Tracking cancer progression: From circulating tumor cells to metastasis. Genome Med. 2020, 12, 31. [Google Scholar] [CrossRef]
- Maly, V.; Maly, O.; Kolostova, K.; Bobek, V. Circulating Tumor Cells in Diagnosis and Treatment of Lung Cancer. In Vivo 2019, 33, 1027–1037. [Google Scholar] [CrossRef]
- Duque, G.; Manterola, C.; Otzen, T.; Arias, C.; Galindo, B.; Mora, M.; Guerrero, E.; Garcia, N. Clinical Utility of Liquid Biopsy in Breast Cancer: A Systematic Review. Clin. Genet. 2022, 101, 285–295. [Google Scholar] [CrossRef]
- Cueva Bañuelos, J.F.; Rodríguez López, C.; Cortegoso Mosquera, A.; Palacios Ozores, P.; Curiel García, T. Clinical Relevance and Therapeutic Application of CTCs in Advanced Breast Cancer. In Circulating Tumor Cells in Breast Cancer Metastatic Disease; Springer International Publishing: Berlin, Germany, 2020; pp. 147–164. [Google Scholar] [CrossRef]
- Vasseur, A.; Kiavue, N.; Bidard, F.-C.; Pierga, J.-Y.; Cabel, L. Clinical utility of circulating tumor cells: An update. Mol. Oncol. 2021, 15, 1647–1666. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.M.M.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.; Mosele, F.; Verret, B.; Bachelot, T.; Bedard, P.L.; Cortes, J.; Hyman, D.M.; Juric, D.; Krop, I.; Bieche, I.; et al. Genomic alterations in breast cancer: Level of evidence for actionability according to ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann. Oncol. 2019, 30, 365–373. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Nelson, M.A.; Ngamcherdtrakul, W.; Luoh, S.-W.; Yantasee, W. Prognostic and therapeutic role of tumor-infiltrating lymphocyte subtypes in breast cancer. Cancer Metastasis Rev. 2021, 40, 519–536. [Google Scholar] [CrossRef] [PubMed]
- Kolyvas, E.A.; Caldas, C.; Kelly, K.; Ahmad, S.S. Androgen receptor function and targeted therapeutics across breast cancer subtypes. Breast Cancer Res. 2022, 24, 79. [Google Scholar] [CrossRef]
- Eom, Y.H.; Kim, H.S.; Lee, A.; Song, B.J.; Chae, B.J. BCL2 as a Subtype-Specific Prognostic Marker for Breast Cancer. J. Breast Cancer 2016, 19, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Lok, S.W.; Whittle, J.R.; Vaillant, F.; Teh, C.E.; Lo, L.L.; Policheni, A.N.; Bergin, A.R.T.; Desai, J.; Ftouni, S.; Gandolfo, L.C.; et al. A Phase Ib Dose-Escalation and Expansion Study of the BCL2 Inhibitor Venetoclax Combined with Tamoxifen in ER and BCL2–Positive Metastatic Breast Cancer. Cancer Discov. 2019, 9, 354–369. [Google Scholar] [CrossRef] [PubMed]
- Orywal, K.; Szmitkowski, M. Alcohol dehydrogenase and aldehyde dehydrogenase in malignant neoplasms. Clin. Exp. Med. 2016, 17, 131–139. [Google Scholar] [CrossRef]
- Clark, D.W.; Palle, K. Aldehyde dehydrogenases in cancer stem cells: Potential as therapeutic targets. Ann. Transl. Med. 2016, 4, 518. [Google Scholar] [CrossRef]
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; Liu, Q.; Cochran, C.; Bennett, L.M.; Ding, W.; et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef]
- Chen, L.; Zhu, X.; Han, B.; Ji, L.; Yao, L.; Wang, Z. High Expression of microRNA-223 Indicates a Good Prognosis in Triple-Negative Breast Cancer. Front. Oncol. 2021, 11, 630432. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.H.; Hall, C.; Lucci, A. Circulating Tumor Cells in Breast Cancer. Tumor Liq. Biopsies 2019, 215, 127–145. [Google Scholar] [CrossRef]
- Bidard, F.-C.; Proudhon, C.; Pierga, J.-Y. Circulating tumor cells in breast cancer. Mol. Oncol. 2016, 10, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Ning, D.; Cui, K.; Liu, M.; Ou, Y.; Wang, Z.; Zou, B.; Shen, Y.; Lu, X.; Li, S.; Li, P. Comparison of CellSearch and Circulating Tumor Cells (CTC)-Biopsy Systems in Detecting Peripheral Blood Circulating Tumor Cells in Patients with Gastric Cancer. Experiment 2020, 27, e926565. [Google Scholar] [CrossRef]
- Tay, T.K.Y.; Tan, P.H. Liquid Biopsy in Breast Cancer: A Focused Review. Arch. Pathol. Lab. Med. 2020, 145, 678–686. [Google Scholar] [CrossRef]
- Sant, M.; Bernat-Peguera, A.; Felip, E.; Margelí, M. Role of ctDNA in Breast Cancer. Cancers 2022, 14, 310. [Google Scholar] [CrossRef]
- Brett, J.O.; Spring, L.M.; Bardia, A.; Wander, S.A. ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer. Breast Cancer Res. 2021, 23, 85. [Google Scholar] [CrossRef]
- Dustin, D.; Gu, G.; Fuqua, S.A.W. ESR1 mutations in breast cancer. Cancer 2019, 21, 3714–3728. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Biomarker | Utility | Reference |
|---|---|---|
| CA 15-3/CA 27-29 | Serological marker to monitor disease progression and/or response to a given treatment | [28,29,30,31,32,33,34,35,36] |
| HER2 and Hormonal Receptors | Molecular classification of breast cancer in luminal A, luminal B, Her 2, and triple-negative breast cancer. | [37,38,39,40,41,42,43,44,45,46,47,48,49,50] |
| PDL1 | Expression of more than >1% defines sensitivity to PDL1 inhibitors in triple-negative breast cancer. | [48,49,50,51] |
| PIK3CA | Usefulness of PI3K inhibitors such as alpelisib in hormone-positive receptor/HER2-negative metastatic breast cancer. | [52,53,54] |
| Androgen receptor | More favorable prognosis in ER-positive breast cancer. | [55] |
| BRCA1/2 | Sensitivity to targeted therapies (PARP inhibitor) such as olaparib and talazoparib in patients with BRCA mutations. | [56,57,58,59] |
| MicroRNA (miR-21, miR- miR 17, miR 155, of miR-10b, miR 191 5p, miR 214-3p, miR 451a and miR-489, miR 16, miR 155 or miR 374a) | Impact in prognosis and diagnosis of metastatic breast cancer. | [60,61,62,63,64,65,66,67,68,69,70,71,72,73] |
| Circulating tumor cells. | Count ≥ 5 CTCs/7.5 mL of blood is related to metastatic disease, and >62.2 cells/7.5 mL is related to a worse prognosis in MBC. | [74,75] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pekarek, L.; Sánchez Cendra, A.; Roberts Cervantes, E.D.; Sánchez Cendra, C.; Fraile-Martinez, O.; García-Montero, C.; Diaz-Pedrero, R.; Torres-Carranza, D.; Lopez-Gonzalez, L.; Aguado-Henche, S.; et al. Clinical and Translational Applications of Serological and Histopathological Biomarkers in Metastatic Breast Cancer: A Comprehensive Review. Int. J. Mol. Sci. 2023, 24, 8396. https://doi.org/10.3390/ijms24098396
Pekarek L, Sánchez Cendra A, Roberts Cervantes ED, Sánchez Cendra C, Fraile-Martinez O, García-Montero C, Diaz-Pedrero R, Torres-Carranza D, Lopez-Gonzalez L, Aguado-Henche S, et al. Clinical and Translational Applications of Serological and Histopathological Biomarkers in Metastatic Breast Cancer: A Comprehensive Review. International Journal of Molecular Sciences. 2023; 24(9):8396. https://doi.org/10.3390/ijms24098396
Chicago/Turabian StylePekarek, Leonel, Alicia Sánchez Cendra, Eduardo D. Roberts Cervantes, Cristina Sánchez Cendra, Oscar Fraile-Martinez, Cielo García-Montero, Raul Diaz-Pedrero, Diego Torres-Carranza, Laura Lopez-Gonzalez, Soledad Aguado-Henche, and et al. 2023. "Clinical and Translational Applications of Serological and Histopathological Biomarkers in Metastatic Breast Cancer: A Comprehensive Review" International Journal of Molecular Sciences 24, no. 9: 8396. https://doi.org/10.3390/ijms24098396