
Determination of the Predictive Roles and Potentially Pathogenic Antigen Epitopes of α-Enolase Related to the Development of Miscarriage in Females with Autoimmune Thyroiditis
Abstract
:1. Introduction
2. Results
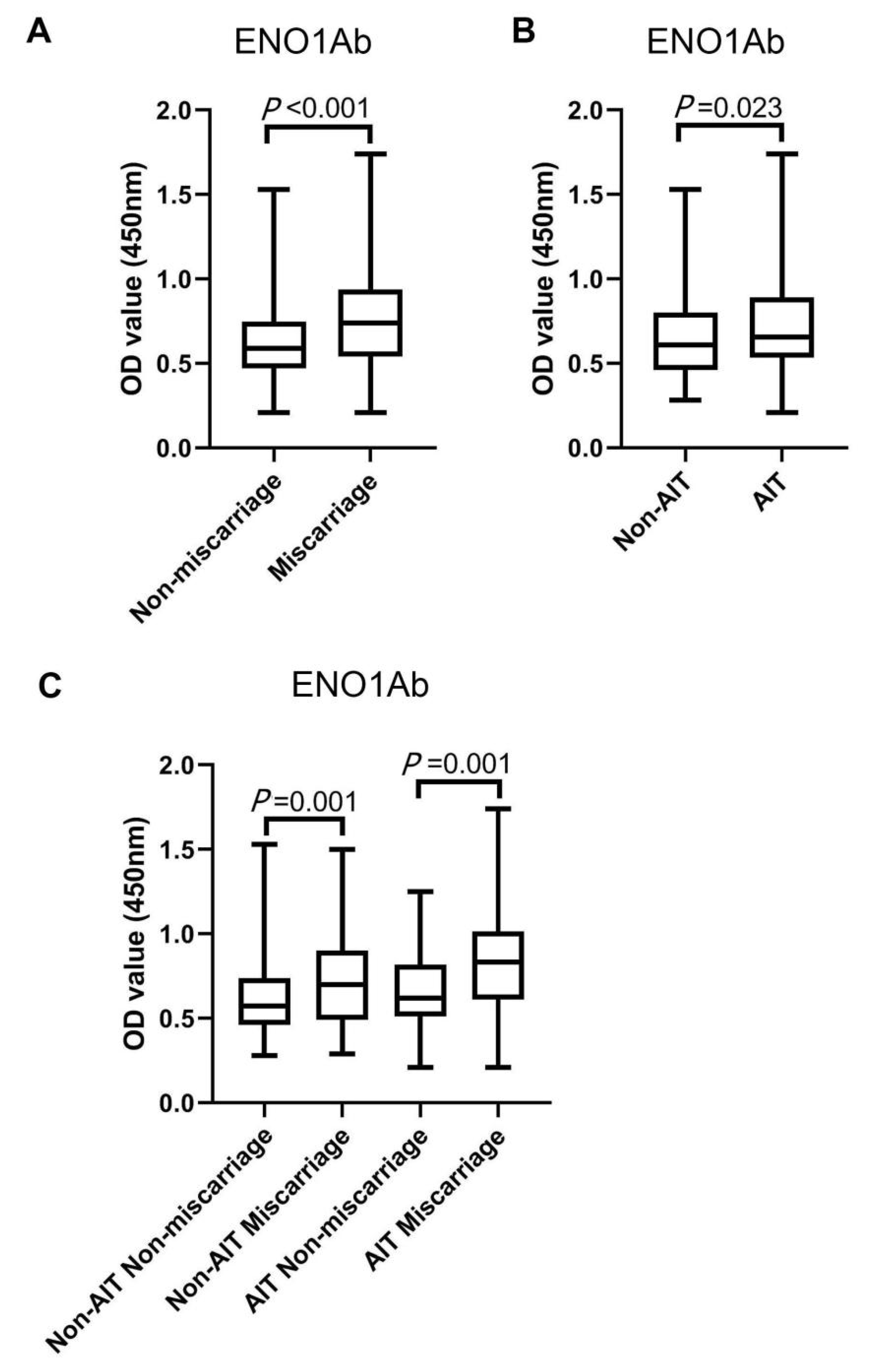
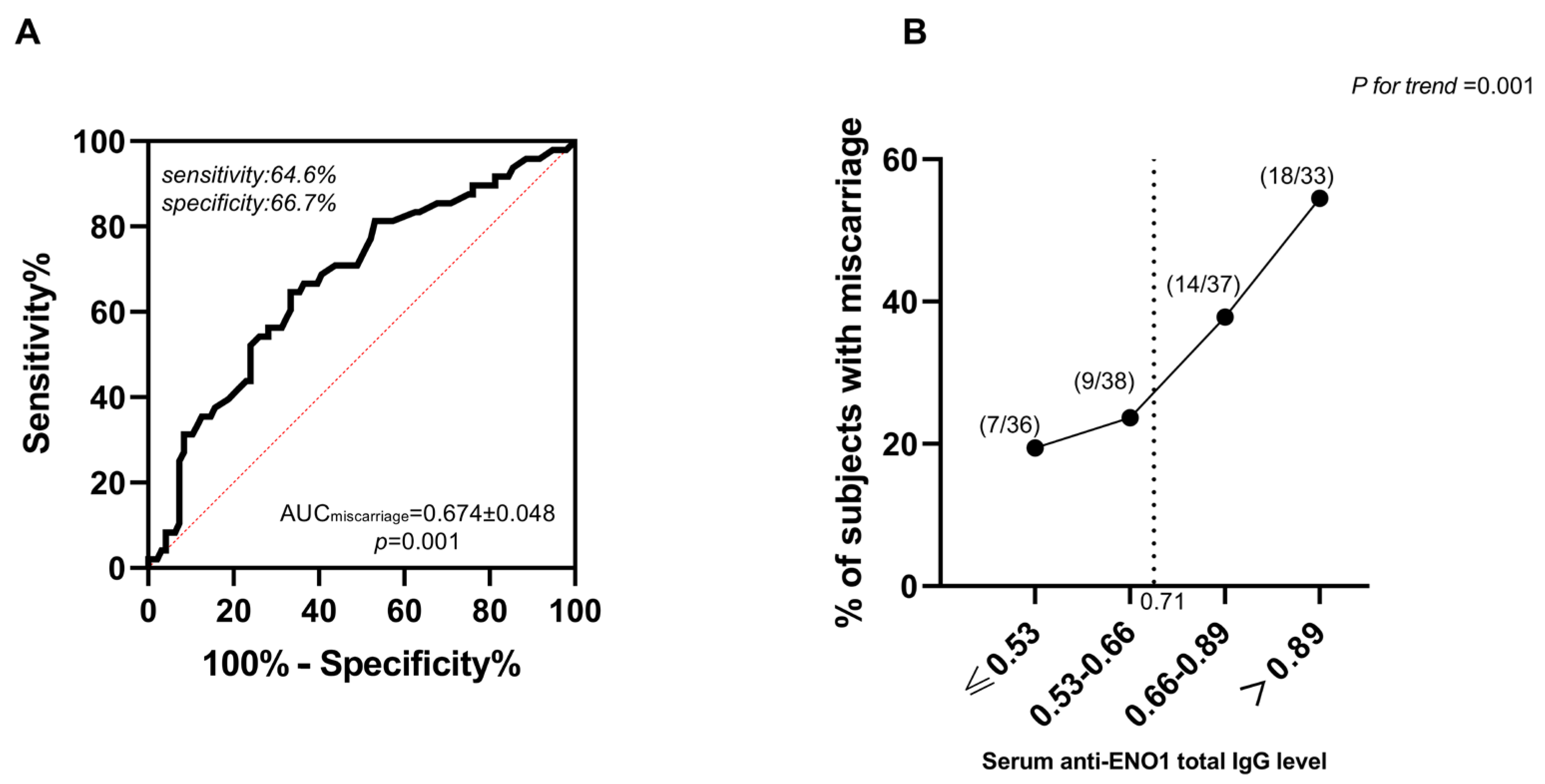
2.1. The Correlation between Serum Antibody Expressions against ENO1Ab and the Occurrence of Miscarriage in AIT Women


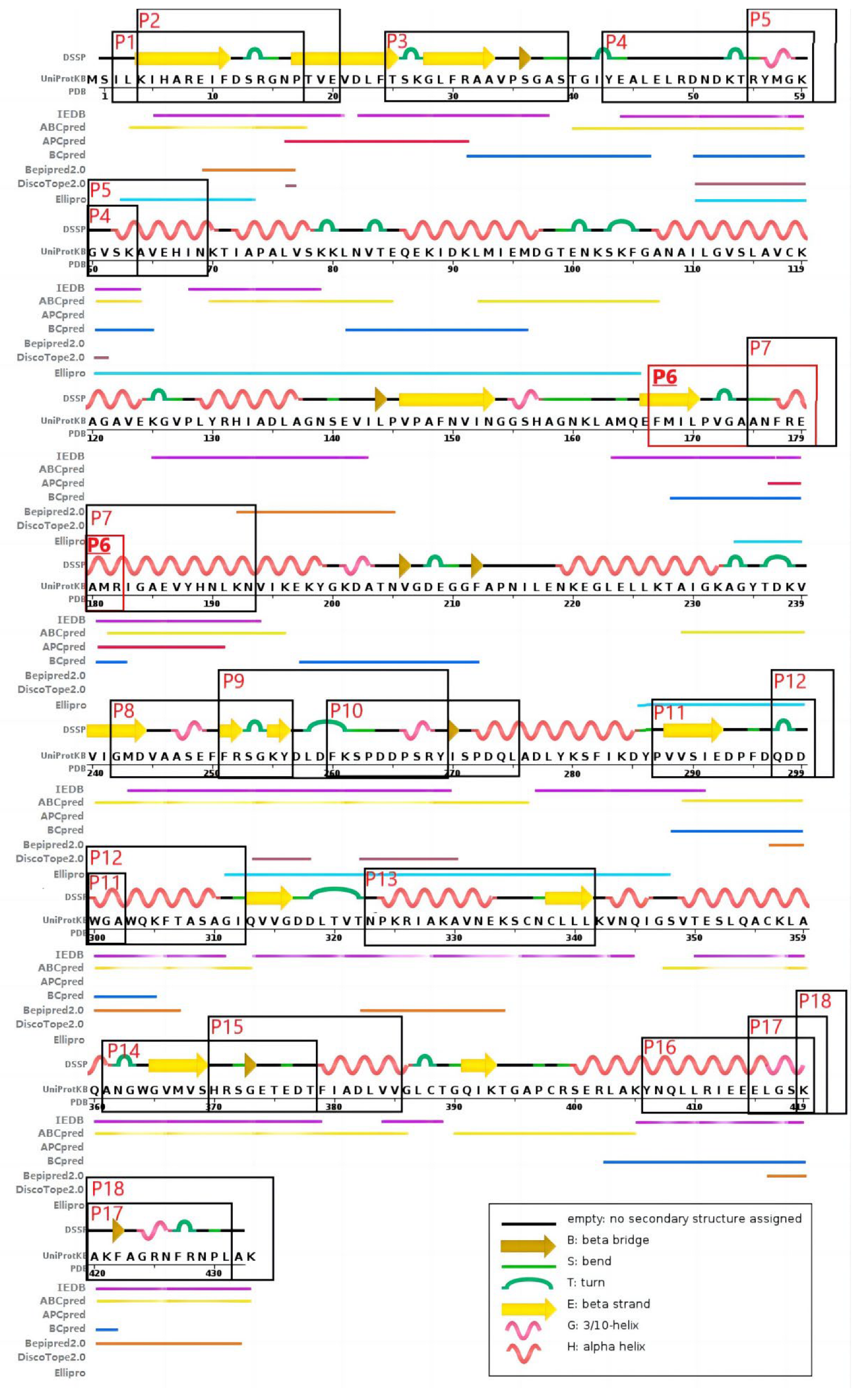
2.2. Serum Autoantibody Expressions against the 18 Predicted Antigenic Epitopes of ENO1
3. Discussion
4. Materials and Methods
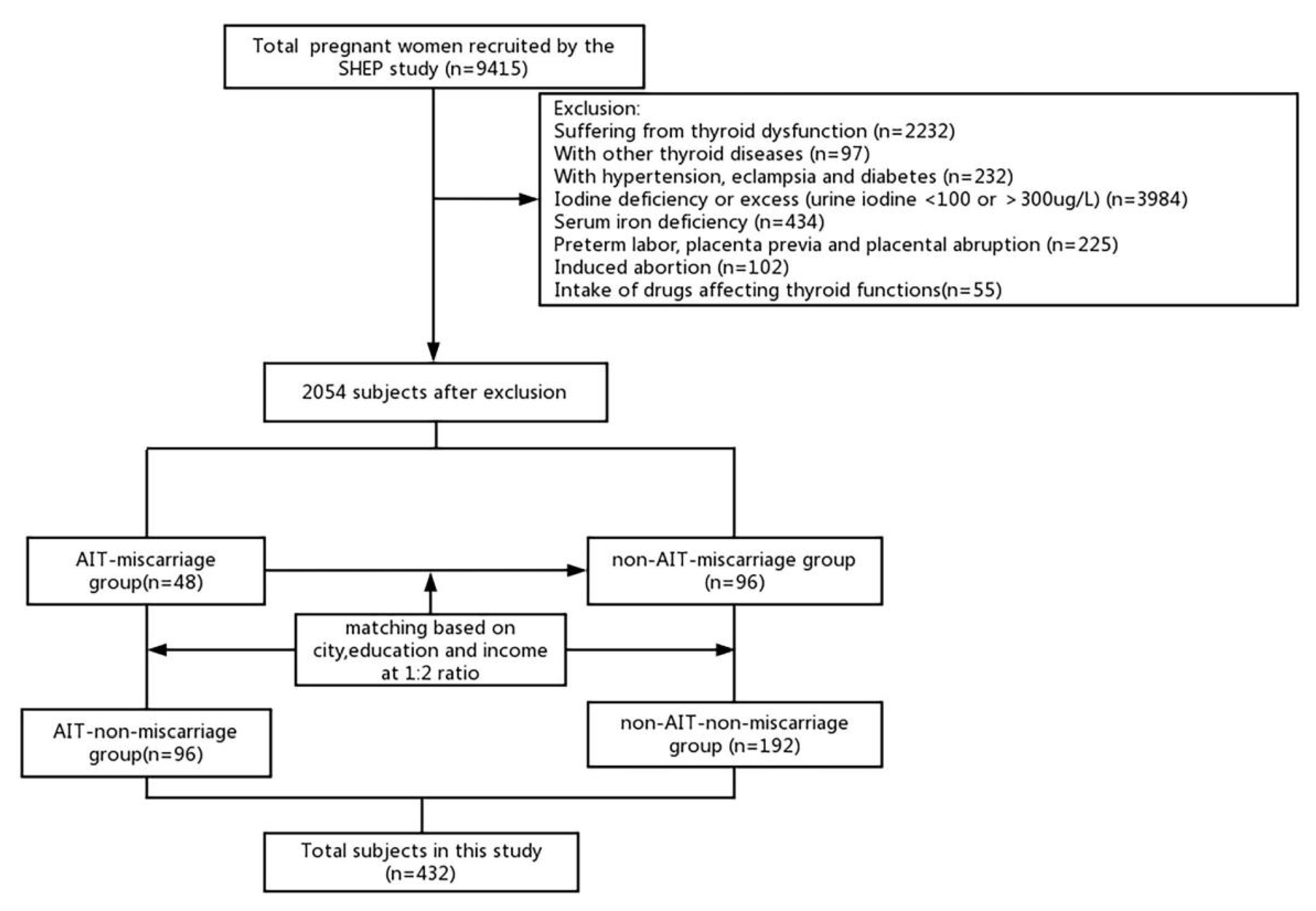
4.1. Patients
4.2. Prediction of the Potential Epitopes in ENO1 Protein
4.3. Enzyme-Linked Immunosorbent Assay
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, W.; Xiang, Y.; Zhang, H.; Shan, Z.; Li, J.; Teng, W. The role of protein disulphide-isomerase A3 as autoantigen in the pathogenesis of autoimmune thyroiditis and related brain damage in adult mice. Clin. Immunol. 2020, 212, 108350. [Google Scholar] [CrossRef] [PubMed]
- De Leo, S.; Pearce, E.N. Autoimmune thyroid disease during pregnancy. Lancet Diabetes Endocrinol. 2018, 6, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shan, Z.; Li, C.; Mao, J.; Xie, X.; Wang, W.; Fan, C.; Wang, H.; Zhang, H.; Han, C.; et al. Maternal subclinical hypothyroidism, thyroid autoimmunity, and the risk of miscarriage: A prospective cohort study. Thyroid 2014, 24, 1642–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakosta, P.; Alegakis, D.; Georgiou, V.; Roumeliotaki, T.; Fthenou, E.; Vassilaki, M.; Boumpas, D.; Castanas, E.; Kogevinas, M.; Chatzi, L. Thyroid dysfunction and autoantibodies in early pregnancy are associated with increased risk of gestational diabetes and adverse birth outcomes. J. Clin. Endocrinol. Metab. 2012, 97, 4464–4472. [Google Scholar] [CrossRef] [PubMed]
- Cleary-Goldman, J.; Malone, F.D.; Lambert-Messerlian, G.; Sullivan, L.; Canick, J.; Porter, T.F.; Luthy, D.; Gross, S.; Bianchi, D.W.; D’Alton, M.E. Maternal thyroid hypofunction and pregnancy outcome. Obstet. Gynecol. 2008, 112, 85–92. [Google Scholar] [CrossRef]
- Thangaratinam, S.; Tan, A.; Knox, E.; Kilby, M.D.; Franklyn, J.; Coomarasamy, A. Association between thyroid autoantibodies and miscarriage and preterm birth: Meta-analysis of evidence. BMJ 2011, 342, d2616. [Google Scholar] [CrossRef] [Green Version]
- Poppe, K.; Velkeniers, B.; Glinoer, D. The role of thyroid autoimmunity in fertility and pregnancy. Nat. Rev. Endocrinol. 2008, 4, 394–405. [Google Scholar] [CrossRef]
- Stagnaro-Green, A.; Roman, S.H.; Cobin, R.H.; el-Harazy, E.; Alvarez-Marfany, M.; Davies, T.F. Detection of at-risk pregnancy by means of highly sensitive assays for thyroid autoantibodies. JAMA 1990, 264, 1422–1425. [Google Scholar] [CrossRef]
- Colicchia, M.; Campagnolo, L.; Baldini, E.; Ulisse, S.; Valensise, H.; Moretti, C. Molecular basis of thyrotropin and thyroid hormone action during implantation and early development. Hum. Reprod. Update 2014, 20, 884–904. [Google Scholar] [CrossRef]
- Matalon, S.T.; Blank, M.; Levy, Y.; Carp, H.J.; Arad, A.; Burek, L.; Grunebaum, E.; Sherer, Y.; Ornoy, A.; Refetoff, S.; et al. The pathogenic role of anti-thyroglobulin antibody on pregnancy, evidence from an active immunization model in mice. Hum. Reprod. 2003, 18, 1094–1099. [Google Scholar] [CrossRef]
- Twig, G.; Shina, A.; Amital, H.; Shoenfeld, Y. Pathogenesis of infertility and recurrent pregnancy loss in thyroid autoimmunity. J. Autoimmun. 2012, 38, J275–J281. [Google Scholar] [CrossRef]
- Vissenberg, R.; Manders, V.D.; Mastenbroek, S.; Fliers, E.; Afink, G.B.; Ris-Stalpers, C.; Goddijn, M.; Bisschop, P. Pathophysiological aspects of thyroid hormone disorders/thyroid peroxidase autoantibodies and reproduction. Hum. Reprod. Update 2015, 21, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Monteleone, P.; Faviana, P.; Artini, P.G. Thyroid peroxidase identified in human granulosa cells, another piece to the thyroid-ovary puzzle? Gynecol. Endocrinol. 2017, 33, 574–576. [Google Scholar] [CrossRef]
- Wang, H.; Gao, H.; Chi, H.; Zeng, L.; Xiao, W.; Wang, Y.; Li, R.; Liu, P.; Wang, C.; Tian, Q.; et al. Effect of Levothyroxine on Miscarriage Among Women With Normal Thyroid Function and Thyroid Autoimmunity Undergoing In Vitro Fertilization and Embryo Transfer: A Randomized Clinical Trial. JAMA 2017, 318, 2190–2198. [Google Scholar] [CrossRef]
- Dhillon-Smith, R.K.; Middleton, L.J.; Sunner, K.K.; Cheed, V.; Baker, K.; Farrell-Carver, S.; Bender-Atik, R.; Agrawal, R.; Bhatia, K.; Edi-Osagie, E.; et al. Levothyroxine in Women with Thyroid Peroxidase Antibodies before Conception. N. Engl. J. Med. 2019, 380, 1316–1325. [Google Scholar] [CrossRef]
- Gharesi-Fard, B.; Zolghadri, J.; Kamali-Sarvestani, E. Alteration in the expression of proteins in unexplained recurrent pregnancy loss compared with in the normal placenta. J. Reprod. Dev. 2014, 60, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Pietsch, J.; Sickmann, A.; Weber, G.; Bauer, J.; Egli, M.; Wildgruber, R.; Infanger, M.; Grimm, D. Metabolic enzyme diversity in different human thyroid cell lines and their sensitivity to gravitational forces. Proteomics 2012, 12, 2539–2546. [Google Scholar] [CrossRef]
- Lu, Y.; Qin, J.; Xiang, Y.; Sun, R.; Feng, Y.; Zhang, H.; Ding, S.; Li, J.; Shan, Z.; Teng, W. Experimental evidence for alpha enolase as one potential autoantigen in the pathogenesis of both autoimmune thyroiditis and its related encephalopathy. Int. Immunopharmacol. 2020, 85, 106563. [Google Scholar] [CrossRef]
- Ye, Y.; Kuhn, C.; Kösters, M.; Arnold, G.J.; Ishikawa-Ankerhold, H.; Schulz, C.; Rogenhofer, N.; Thaler, C.J.; Mahner, S.; Fröhlich, T.; et al. Anti α-enolase antibody is a novel autoimmune biomarker for unexplained recurrent miscarriages. EBioMedicine 2019, 41, 610–622. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Liu, Y.; Wang, H.; Sun, W.; Lu, Y.; Shan, Z.; Teng, W.; Li, J. A Predictive Role of Autoantibodies Against the Epitope aa168-183 of ENO1 in the Occurrence of Miscarriage Related to Thyroid Autoimmunity. Front. Immunol. 2022, 13, 890502. [Google Scholar] [CrossRef]
- Lin, C.; Xiang, Y.; Li, J. The contribution of thyroid autoimmunity to miscarriage in euthyroid women. Minerva. Med. 2016, 107, 173–181. [Google Scholar] [PubMed]
- Zhu, Q.; Xu, Q.-H.; Xie, T.; Wang, L.-L.; Liu, H.; Muyayalo, K.P.; Huang, X.-B.; Zhao, S.-J.; Liao, A.-H. Recent insights into the impact of immune dysfunction on reproduction in autoimmune thyroiditis. Clin. Immunol. 2021, 224, 108663. [Google Scholar] [CrossRef] [PubMed]
- Pratt, D.; Novotny, M.; Kaberlein, G.; Dudkiewicz, A.; Gleicher, N. Antithyroid antibodies and the association with non-organ-specific antibodies in recurrent pregnancy loss. Am. J. Obstet. Gynecol. 1993, 168, 837–841. [Google Scholar] [CrossRef] [PubMed]
- Didiasova, M.; Schaefer, L.; Wygrecka, M. When Place Matters: Shuttling of Enolase-1 Across Cellular Compartments. Front. Cell Dev. Biol. 2019, 7, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz-Ramos, A.; Roig-Borrellas, A.; García-Melero, A.; López-Alemany, R. α-Enolase, a multifunctional protein: Its role on pathophysiological situations. J. Biomed. Biotechnol. 2012, 2012, 156795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrier, B.; Degand, N.; Guilpain, P.; Servettaz, A.; Guillevin, L.; Mouthon, L. Alpha-enolase: A target of antibodies in infectious and autoimmune diseases. Autoimmun. Rev. 2007, 6, 176–182. [Google Scholar] [CrossRef]
- Thébault, S.; Gilbert, D.; Hubert, M.; Drouot, L.; Machour, N.; Lange, C.; Charlionet, R.; Tron, F. Orderly pattern of development of the autoantibody response in (New Zealand White × BXSB)F1 lupus mice: Characterization of target antigens and antigen spreading by two-dimensional gel electrophoresis and mass spectrometry. J. Immunol. 2002, 169, 4046–4053. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kwon, B.; Hur, G.; Choi, S.; Nahm, D.; Park, H. Isotype and IgG subclass distribution of autoantibody response to alpha-enolase protein in adult patients with severe asthma. Yonsei. Med. J. 2008, 49, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Kimura, Y.; Miura, N.; Debiec, H.; Morita, H.; Yamada, H.; Banno, S.; Ronco, P.; Imai, H. Circulating antibodies to α-enolase and phospholipase A receptor and composition of glomerular deposits in Japanese patients with primary or secondary membranous nephropathy. Clin. Exp. Nephrol. 2017, 21, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Orth, T.; Kellner, R.; Diekmann, O.; Faust, J.; Meyer, B.; Mayet, W. Identification and characterization of autoantibodies against catalase and alpha-enolase in patients with primary sclerosing cholangitis. Clin. Exp. Immunol. 1998, 112, 507–515. [Google Scholar] [CrossRef]
- Pratesi, F.; Moscato, S.; Sabbatini, A.; Chimenti, D.; Bombardieri, S.; Migliorini, P. Autoantibodies specific for alpha-enolase in systemic autoimmune disorders. J. Rheumatol. 2000, 27, 109–115. [Google Scholar]
- Versini, M. Thyroid Autoimmunity and Antiphospholipid Syndrome: Not Such a Trivial Association. Front. Endocrinol. (Lausanne) 2017, 8, 175. [Google Scholar] [CrossRef] [Green Version]
- Hee, J.Y.; Huang, S.; Leong, K.P.; Chun, L.; Zhang, Y.O.; Gongye, R.; Tang, K. Pregnancy loss and the risk of rheumatoid arthritis in Chinese women: Findings from the China Kadoorie biobank. BMC Public Health 2022, 22, 1768. [Google Scholar] [CrossRef]
- Bălănescu, A.; Donisan, T.; Bălănescu, D. An ever-challenging relationship: Lupus and pregnancy. Reumatologia 2017, 55, 29–37. [Google Scholar] [CrossRef]
- Sun, W.; Feng, Y.; Li, H.; He, X.; Lu, Y.; Shan, Z.; Teng, W.; Li, J. The effects of maternal anti-alpha-enolase antibody expression on the brain development in offspring. Clin. Exp. Immunol. 2022, 210, 187–198. [Google Scholar] [CrossRef]
- Perconti, G.; Maranto, C.; Romancino, D.P.; Rubino, P.; Feo, S.; Bongiovanni, A.; Giallongo, A. Pro-invasive stimuli and the interacting protein Hsp70 favour the route of alpha-enolase to the cell surface. Sci. Rep. 2017, 7, 3841. [Google Scholar] [CrossRef] [Green Version]
- Fujii, A.; Yoneda, M.; Ito, T.; Yamamura, O.; Satomi, S.; Higa, H.; Kimura, A.; Suzuki, M.; Yamashita, M.; Yuasa, T.; et al. Autoantibodies against the amino terminal of alpha-enolase are a useful diagnostic marker of Hashimoto’s encephalopathy. J. Neuroimmunol. 2005, 162, 130–136. [Google Scholar] [CrossRef]
- Swets, J. Measuring the accuracy of diagnostic systems. Source Sci. New Ser. 1988, 240, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Fischer, J.; Bachmann, L.; Jaeschke, R. A readers’ guide to the interpretation of diagnostic test properties: Clinical example of sepsis. Intensive Care Med. 2003, 29, 1043–1051. [Google Scholar] [CrossRef] [Green Version]
- Walter, M.; Berg, H.; Leidenberger, F.; Schweppe, K.; Northemann, W. Autoreactive epitopes within the human alpha-enolase and their recognition by sera from patients with endometriosis. J Autoimmun. 1995, 8, 931–945. [Google Scholar] [CrossRef]
- Adamus, G.; Amundson, D.; Seigel, G.; Machnicki, M. Anti-enolase-alpha autoantibodies in cancer-associated retinopathy: Epitope mapping and cytotoxicity on retinal cells. J. Autoimmun. 1998, 11, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, M.; Sinico, R.A.; Moroni, G.; Pratesi, F.; Migliorini, P.; Galetti, M.; Murtas, C.; Tincani, A.; Madaio, M.; Radice, A.; et al. Glomerular autoimmune multicomponents of human lupus nephritis in vivo: α-enolase and annexin AI. J. Am. Soc. Nephrol. 2014, 25, 2483–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstner, C.; Dubnovitsky, A.; Sandin, C.; Kozhukh, G.; Malmstrm, V. Functional and structural characterization of a novel hla-drb1*04:01-restricted α-enolase t cell epitope in rheumatoid arthritis. Front. Immunol. 2016, 7, 494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pancholi, V. Multifunctional alpha-enolase: Its role in diseases. Cell Mol. Life Sci. 2001, 58, 902–920. [Google Scholar] [CrossRef] [PubMed]
- Pringle, K.; Kind, K.; Sferruzzi-Perri, A.; Thompson, J.; Roberts, C. Beyond oxygen: Complex regulation and activity of hypoxia inducible factors in pregnancy. Hum. Reprod. Update 2010, 16, 415–431. [Google Scholar] [CrossRef] [Green Version]
- Hammond, L.; Lowdell, M.; Cerrano, P.; Goode, A.; Bottazzo, G.; Mirakian, R. Analysis of apoptosis in relation to tissue destruction associated with Hashimoto’s autoimmune thyroiditis. J. Pathol. 1997, 182, 138–144. [Google Scholar] [CrossRef]
- Giordano, C.; Stassi, G.; De Maria, R.; Todaro, M.; Richiusa, P.; Papoff, G.; Ruberti, G.; Bagnasco, M.; Testi, R.; Galluzzo, A. Potential involvement of Fas and its ligand in the pathogenesis of Hashimoto’s thyroiditis. Science 1997, 275, 960–963. [Google Scholar] [CrossRef]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG subclasses and allotypes: From structure to effector functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [Green Version]
- Glinoer, D.; Riahi, M.; Grün, J.P.; Kinthaert, J. Risk of subclinical hypothyroidism in pregnant women with asymptomatic autoimmune thyroid disorders. J. Clin. Endocrinol. Metab. 1994, 79, 197–204. [Google Scholar]
- Berman, H.M.; Westbrook, J.; Feng, Z.; Gilliland, G.; Bhat, T.N.; Weissig, H.; Shindyalov, I.N.; Bourne, P.E. The Protein Data Bank. Nucleic Acids Res. 2000, 28, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.; Jung, S.; Kim, S.; Chung, S. Biological crystallography, Structure of human alpha-enolase (hENO1), a multifunctional glycolytic enzyme. Acta Crystallogr. D Biol. Crystallogr. 2008, 64, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.; Jin, Q.; Li, L.; Yang, Y.; Zhang, H.; Liu, M.; Fan, C.; Li, J.; Shan, Z.; Teng, W. Physiological low-dose oestrogen promotes the development of experimental autoimmune thyroiditis through the up-regulation of Th1/Th17 responses. J. Reprod. Immunol. 2018, 126, 23–31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variants | B | SE | Wald | p | OR (95%CI) |
|---|---|---|---|---|---|
| Age (years) | 0.085 | 0.063 | 1.799 | 0.180 | 1.088 (0.962–1.231) |
| Gestational age (weeks) | −0.166 | 0.161 | 1.062 | 0.303 | 0.847 (0.618–1.161) |
| BMI (kg/m2) | −0.027 | 0.078 | 0.115 | 0.735 | 0.974 (0.835–1.136) |
| Urine iodine/creatinine (μg/g) | 0.007 | 0.005 | 1.985 | 0.159 | 1.007 (0.997–1.017) |
| Serum ferritin (μg/L) | 0.004 | 0.004 | 0.96 | 0.327 | 1.004 (0.996–1.012) |
| TSH (mIU/L) | 0.403 | 0.254 | 2.514 | 0.113 | 1.497 (0.909–2.464) |
| FT4 (pmol/L) | −0.133 | 0.151 | 0.773 | 0.379 | 0.875 (0.651–1.178) |
| TPOAb (IU/mL) | 0.001 | 0.002 | 0.301 | 0.583 | 1.001 (0.998–1.004) |
| TgAb (IU/mL) | −0.001 | 0.001 | 1.106 | 0.293 | 0.999 (0.997–1.001) |
| ENO1Ab a | 2.728 | 0.921 | 8.773 | 0.003 | 15.295 (2.516–92.982) |
| Variants | B | SE | Wald | p | OR(95%CI) |
|---|---|---|---|---|---|
| Age (years) | 0.095 | 0.04 | 5.642 | 0.018 | 1.099 (1.017–1.189) |
| Gestational age (weeks) | −0.695 | 0.138 | 25.519 | <0.001 | 0.499 (0.381–0.654) |
| BMI (kg/m2) | −0.04 | 0.038 | 1.113 | 0.291 | 0.96 (0.891–1.035) |
| Urine iodine/creatinine (μg/g) | −0.002 | 0.002 | 0.991 | 0.32 | 0.998 (0.995–1.002) |
| Serum ferritin (μg/L) | 0.002 | 0.003 | 0.479 | 0.489 | 1.002 (0.997–1.007) |
| TSH (mIU/L) | 0.173 | 0.165 | 1.103 | 0.294 | 1.189 (0.86–1.644) |
| FT4 (pmol/L) | −0.006 | 0.087 | 0.006 | 0.941 | 0.994 (0.838–1.178) |
| ENO1Ab a | 1.568 | 0.56 | 7.834 | 0.005 | 4.795 (1.6–14.37) |
| ENO1Ab | FT4 | TSH | TPOAb | TgAb |
|---|---|---|---|---|
| AIT non-miscarriage group | rs = 0.078 | rs = −0.201 | rs = 0.131 | rs = −0.039 |
| (n = 96) | NS | 0.049 | NS | NS |
| AIT miscarriage group | rs = −0.009 | rs = −0.055 | rs = −0.311 | rs = −0.171 |
| (n = 48) | NS | NS | 0.031 | NS |
| Group | p Value | ||||||
|---|---|---|---|---|---|---|---|
| Non-AIT | AIT | Non-AIT | AIT | Miscarriage | |||
| Non-Miscarriage (n = 8) | Miscarriage (n = 8) | Non-Miscarriage (n = 8) | Miscarriage (n = 8) | Miscarriage vs. Non-Miscarriage | Miscarriage vs. Non-Miscarriage | AIT vs. non-AIT | |
| P1Ab a | 0.37 (0.16–0.93) | 0.94 (0.37–1.20) | 0.71 (0.38–2.00) | 0.16 (0.13–0.47) | 0.189 | 0.016 b | 0.018 |
| P2Ab a | 0.67 (0.57–0.88) | 0.40 (0.32–0.80) | 0.48 (0.27–0.60) | 0.31 (0.23–0.50) | 0.093 | 0.248 | 0.248 |
| P3Ab a | 0.48 (0.42–0.72) | 0.29 (0.20–0.57) | 0.69 (0.45–0.97) | 0.60 (0.34–0.87) | 0.141 | 0.563 | 0.115 |
| P4Ab a | 1.07 (0.77–1.45) | 0.22 (0.17–0.68) | 0.55 (0.25–1.00) | 0.84 (0.47–1.03) | 0.046 | 0.401 | 0.036 |
| P5Ab a | 0.17 (0.13–0.36) | 0.45 (0.24–1.00) | 0.34 (0.28–0.69) | 0.31 (0.12–1.09) | 0.040 | 0.752 | 0.344 |
| P6Ab a | 0.29 (0.15–0.46) | 0.23 (0.16–0.71) | 0.46 (0.41–0.59) | 1.05 (0.86–1.14) | 0.752 | 0.005 b | 0.013 b |
| P7Ab a | 1.19 (0.65–1.38) | 0.71 (0.59–1.10) | 0.37 (0.28–0.48) | 0.24 (0.17–0.40) | 0.207 | 0.103 | 0.005 b |
| P8Ab a | 0.62 (0.26–0.90) | 0.70 (0.39–1.10) | 0.76 (0.43–1.14) | 0.83 (0.70–0.89) | 0.462 | 0.916 | 0.529 |
| P9Ab a | 0.71 (0.46–0.87) | 1.04 (0.88–1.21) | 0.73 (0.30–1.10) | 1.13 (0.49–1.18) | 0.013 b | 0.247 | 1.000 |
| P10Ab a | 0.52 (0.15–1.06) | 1.02 (0.63–1.28) | 0.23 (0.13–0.88) | 0.59 (0.18–0.79) | 0.156 | 0.431 | 0.052 |
| P11Ab a | 0.23 (0.17–0.26) | 0.15 (0.12–0.20) | 0.27 (0.23–0.45) | 0.30 (0.23–0.42) | 0.03 | 0.958 | 0.002 b |
| P12Ab a | 0.79 (0.53–1.67) | 0.43 (0.23–0.64) | 0.55 (0.48–1.29) | 0.35 (0.12–0.58) | 0.036 | 0.052 | 0.400 |
| P13Ab a | 1.00 (0.40–1.22) | 0.26 (0.23–0.78) | 0.74 (0.44–1.10) | 0.20 (0.15–0.39) | 0.046 | 0.003 b | 0.083 |
| P14Ab a | 0.65 (0.58–0.78) | 0.56 (0.23–0.90) | 0.51 (0.44–0.66) | 0.68 (0.47–0.85) | 0.431 | 0.293 | 0.462 |
| P15Ab a | 0.83 (0.34–1.27) | 0.93 (0.45–1.51) | 0.90 (0.34–1.16) | 0.76 (0.61–1.09) | 0.461 | 0.958 | 0.401 |
| P16Ab a | 1.52 (1.29–1.85) | 1.14 (0.98–1.46) | 1.01 (0.84–1.16) | 0.80 (0.36–1.07) | 0.115 | 0.115 | 0.021 |
| P17Ab a | 0.80 (0.56–0.81) | 0.53 (0.32–0.76) | 0.51 (0.42–0.60) | 0.37 (0.23–0.62) | 0.045 | 0.208 | 0.270 |
| P18Ab a | 0.20 (0.17–0.24) | 0.29 (0.23–0.32) | 0.20 (0.18–0.40) | 0.22 (0.17–0.30) | 0.114 | 0.526 | 0.343 |
| No. | Amino Acid Sequence | Location of Epitope | Length of Peptide | Database | Reported Potential Function |
|---|---|---|---|---|---|
| P1 | ILKIHAREIFDSRGNP | 3–18 | 16 | IEDB, ABCpred, Ellipro | NA |
| P2 | KIHAREIFDSRGNPTVE | 5–21 | 17 | IEDB, Bepipred2.0, DiscoTope2.0 | NA |
| P3 | TSKGLFRAAVPSGAS | 26–40 | 15 | IEDB | Related to rheumatoid arthritis [43] |
| P4 | YEALELRDNDKTRYMGKGVSK | 44–64 | 21 | IEDB, ABCpred, DiscoTope2.0, Ellipro | Related to cancer-associated retinopathy syndrome and endometriosis [40,41] |
| P5 | RYMGKGVSKAVEHIN | 56–70 | 15 | IEDB | Related to cancer-associated retinopathy syndrome and endometriosis [40,41] |
| P6 | FMILPVGAANFREAMR | 168–183 | 16 | IEDB, BCpred, Ellipro | A functional glycolytic segment [44] |
| P7 | ANFREAMRIGAEVYHNLKN | 176–194 | 19 | IEDB, ABCpred, APCpred | NA |
| P8 | GMDVAASEFFRSGKY | 243–263 | 21 | IEDB, ABCpred | A functional glycolytic segment [44] |
| P9 | FRSGKYDLDFKSPDDPSRY | 252–270 | 19 | IEDB, ABCpred, DiscoTope2.0, Ellipro | A functional glycolytic segment anda plasminogen-binding site [44,51] |
| P10 | FKSPDDPSRYISPDQL | 261–276 | 16 | ABCpred, DiscoTope2.0 | A functional glycolytic segment [44] |
| P11 | PVVSIEDPFDQDDWGA | 288–307 | 16 | ABCpred, BCpred, Bepipred2.0 | |
| P12 | QDDWGAWQKFTASAGI | 298–313 | 16 | IEDB, ABCpred | NA |
| P13 | NPKRIAKAVNEKSCNCLL | 324–341 | 18 | IEDB, Bepipred2.0 | NA |
| P14 | ANGWGVMVSHRSGETEDT | 362–379 | 18 | IEDB, ABCpred | NA |
| P15 | HRSGETEDTFIADLVV | 371–389 | 19 | IEDB, ABCpred | |
| P16 | YNQLLRIEEELGSKAK | 405–422 | 16 | IEDB, BCpred | Binding with c-myc promoter [44] |
| P17 | ELGSKAKFAGRNFRNPL | 415–432 | 18 | IEDB, Bepipred2.0 | Binding with c-myc promoter [44] |
| P18 | KAKFAGRNFRNPLAK | 420–434 | 15 | IEDB | Binding with c-myc promoter [44] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, J.; Lu, Y.; He, X.; Li, J.; Fan, C.; Zhang, H.; Teng, W.; Shan, Z.; Li, J. Determination of the Predictive Roles and Potentially Pathogenic Antigen Epitopes of α-Enolase Related to the Development of Miscarriage in Females with Autoimmune Thyroiditis. Int. J. Mol. Sci. 2023, 24, 1021. https://doi.org/10.3390/ijms24021021
Guo J, Lu Y, He X, Li J, Fan C, Zhang H, Teng W, Shan Z, Li J. Determination of the Predictive Roles and Potentially Pathogenic Antigen Epitopes of α-Enolase Related to the Development of Miscarriage in Females with Autoimmune Thyroiditis. International Journal of Molecular Sciences. 2023; 24(2):1021. https://doi.org/10.3390/ijms24021021
Chicago/Turabian StyleGuo, Jiahui, Yihan Lu, Xiaoqing He, Jiashu Li, Chenling Fan, Hongmei Zhang, Weiping Teng, Zhongyan Shan, and Jing Li. 2023. "Determination of the Predictive Roles and Potentially Pathogenic Antigen Epitopes of α-Enolase Related to the Development of Miscarriage in Females with Autoimmune Thyroiditis" International Journal of Molecular Sciences 24, no. 2: 1021. https://doi.org/10.3390/ijms24021021