
Ameliorative Effects of a Rhenium (V) Compound with Uracil-Derived Ligand Markers Associated with Hyperglycaemia-Induced Renal Dysfunction in Diet-Induced Prediabetic Rats
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
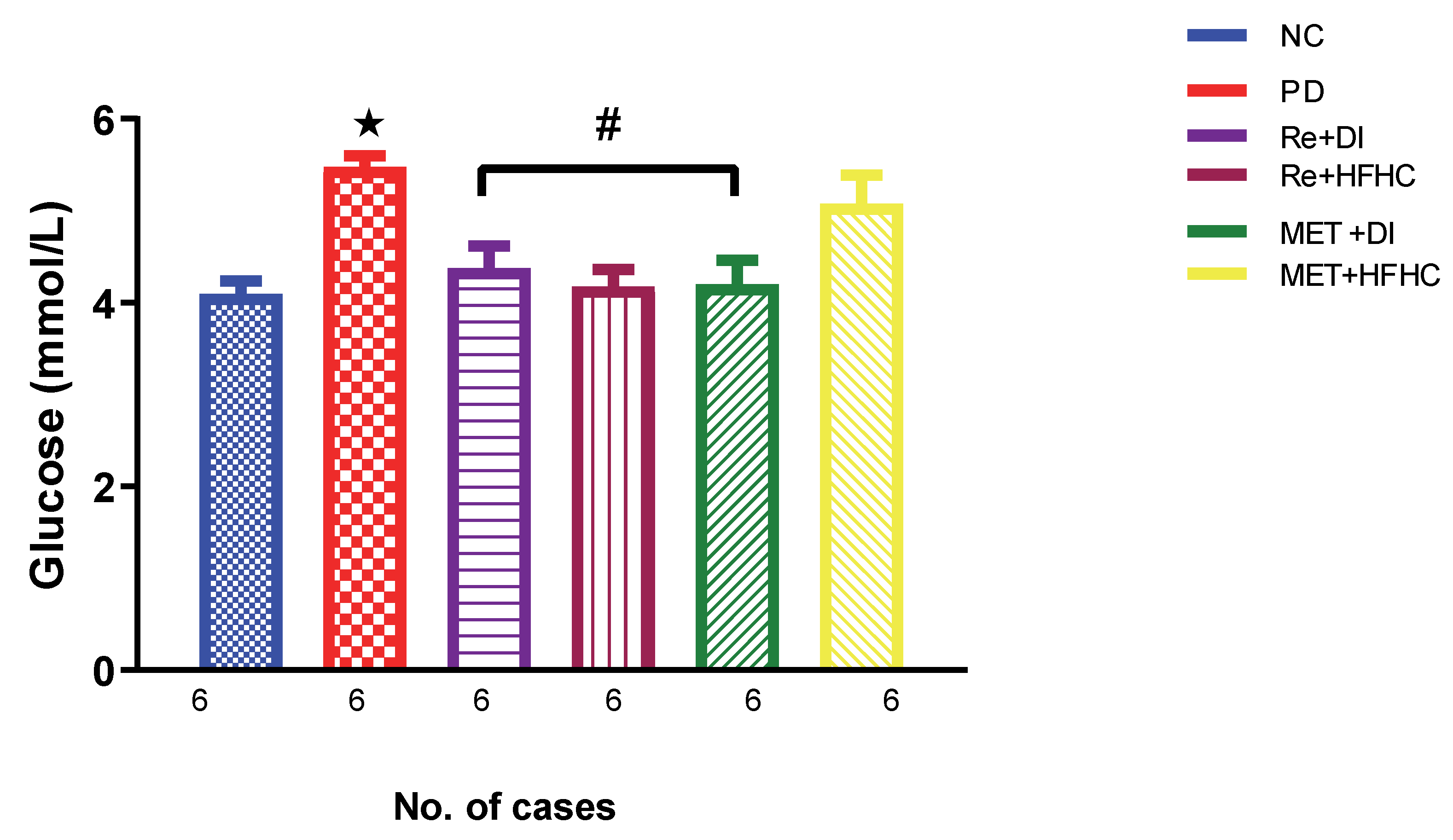
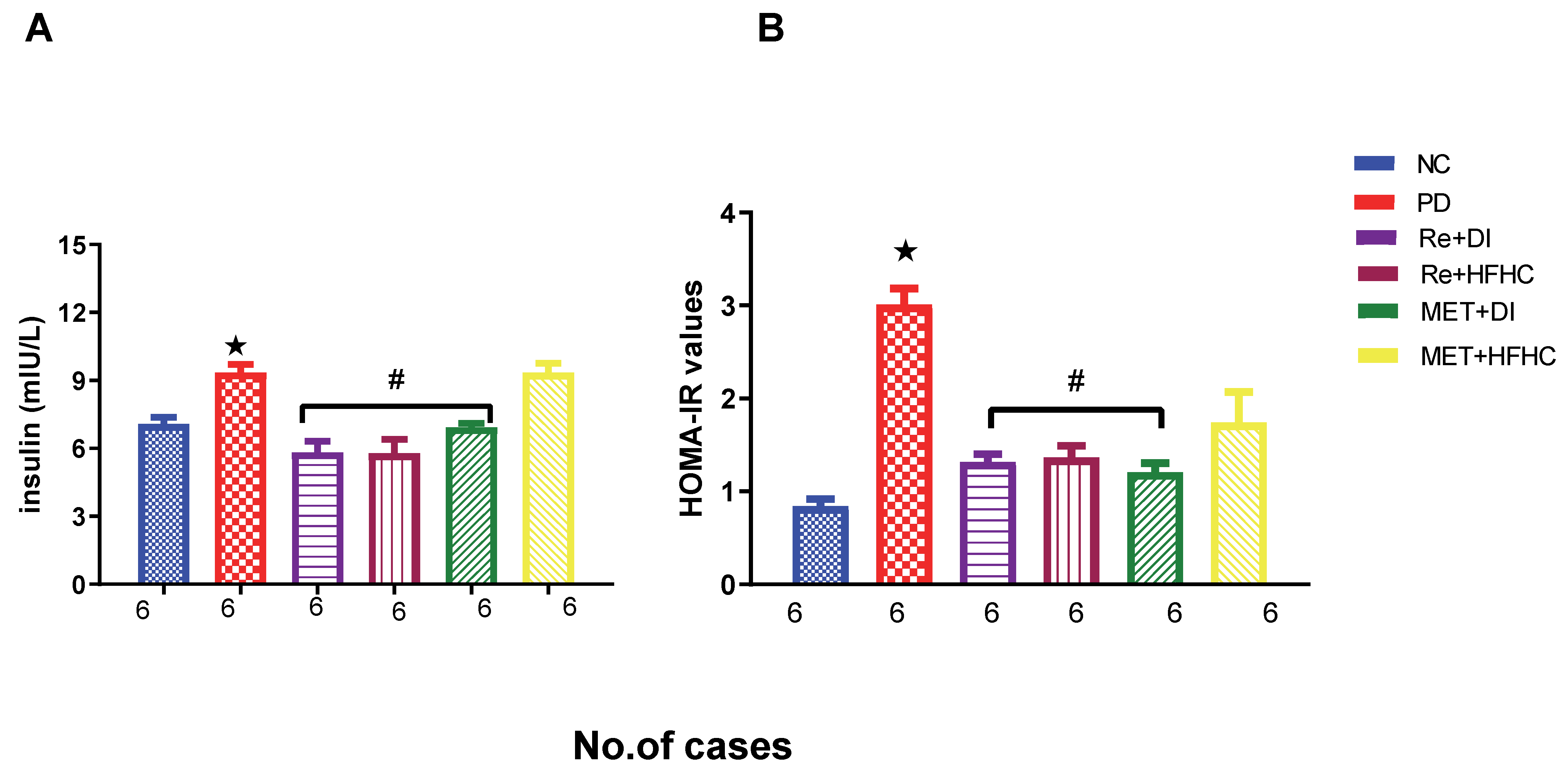
2.1. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Glucose, Insulin Levels and HOMA2-IR Index
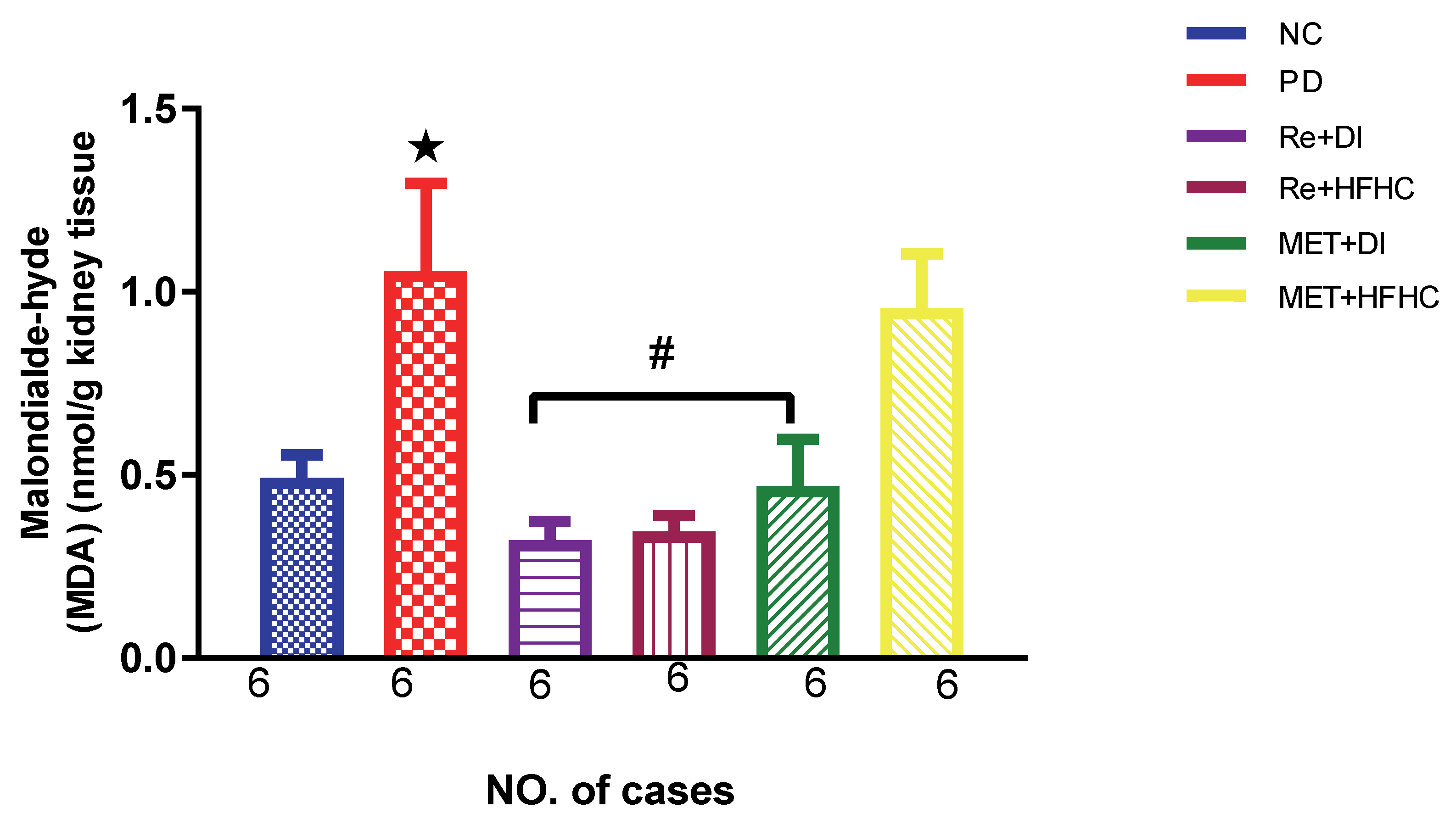
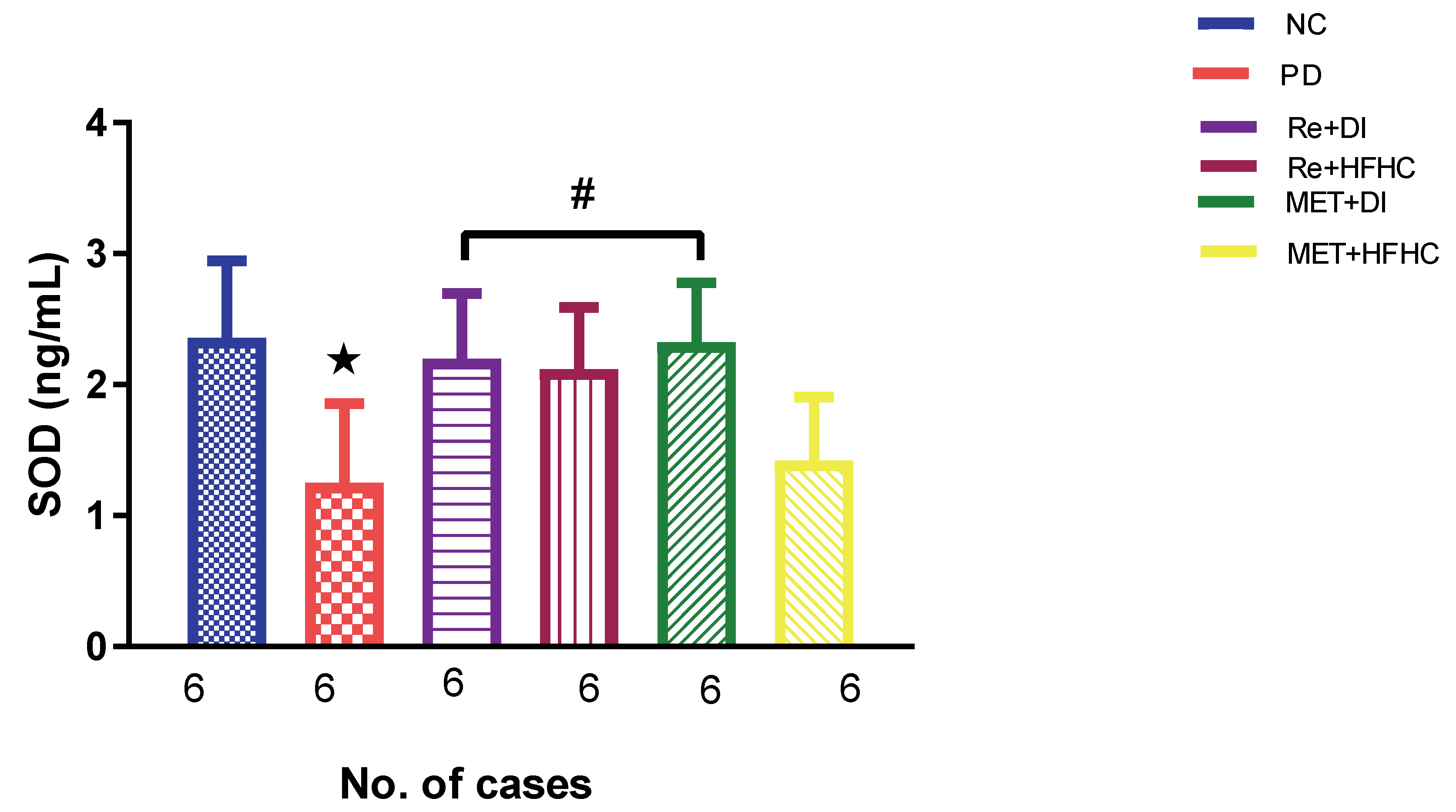
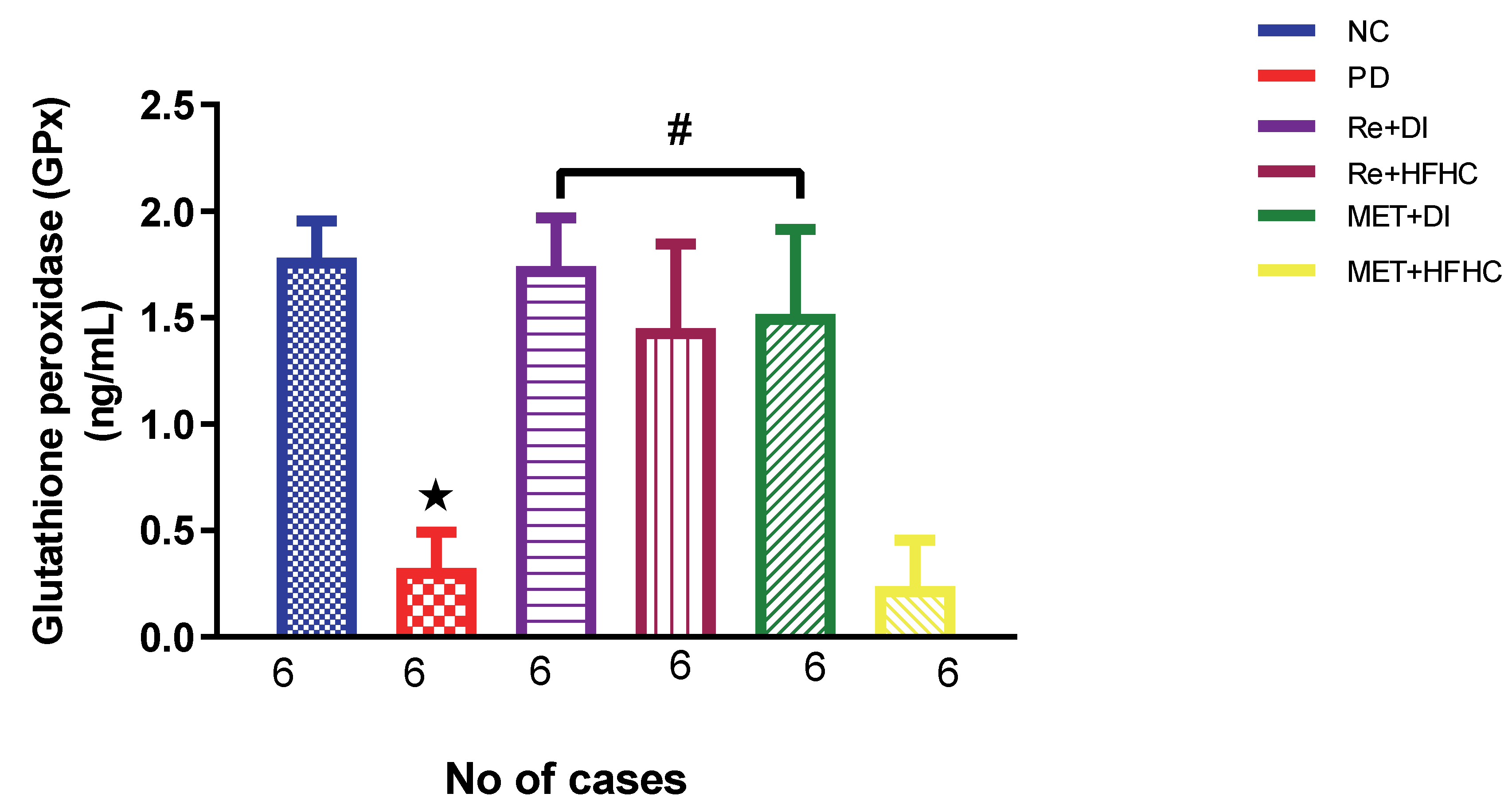
2.2. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Renal Oxidative Stress and Antioxidant Status
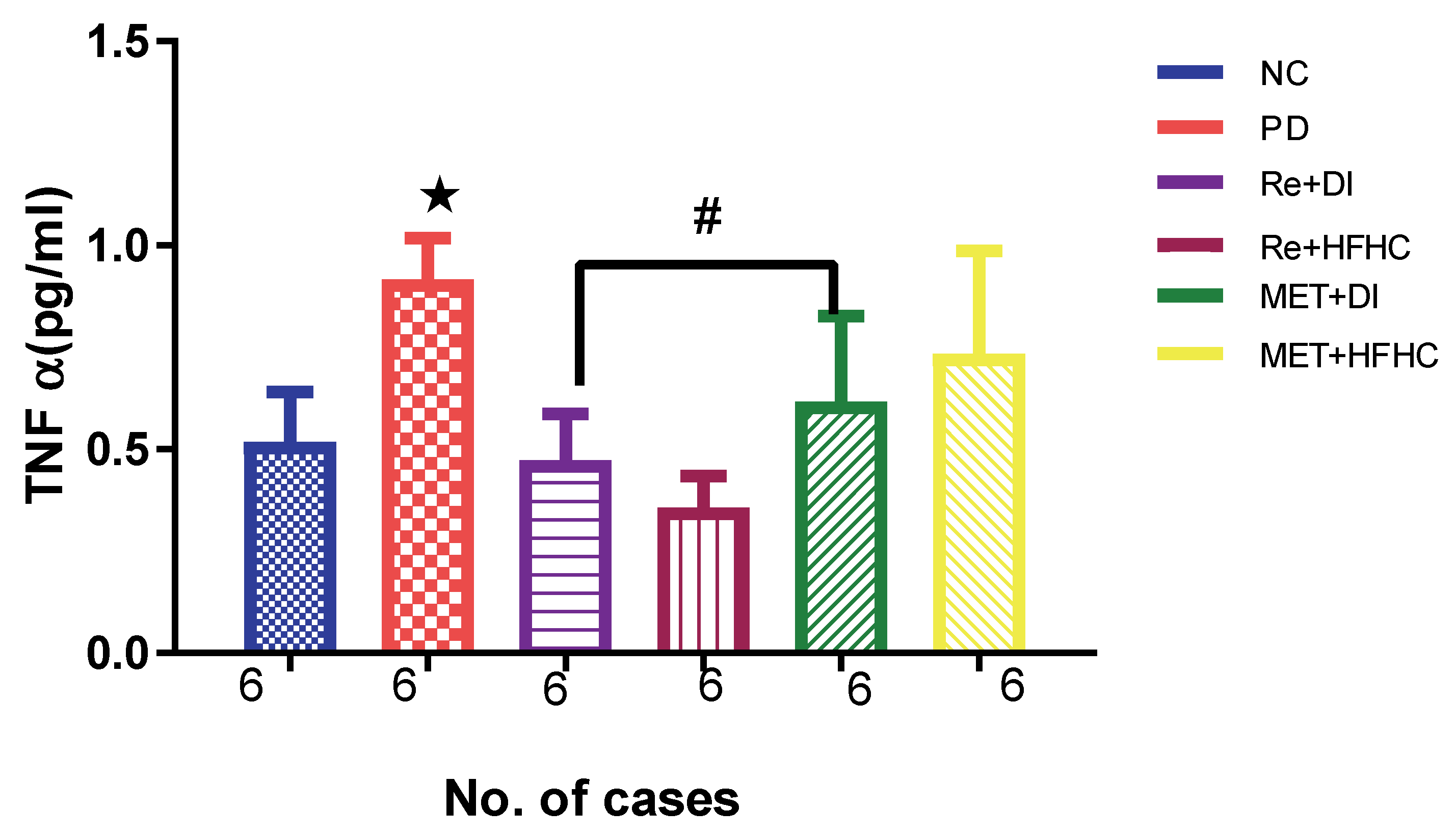
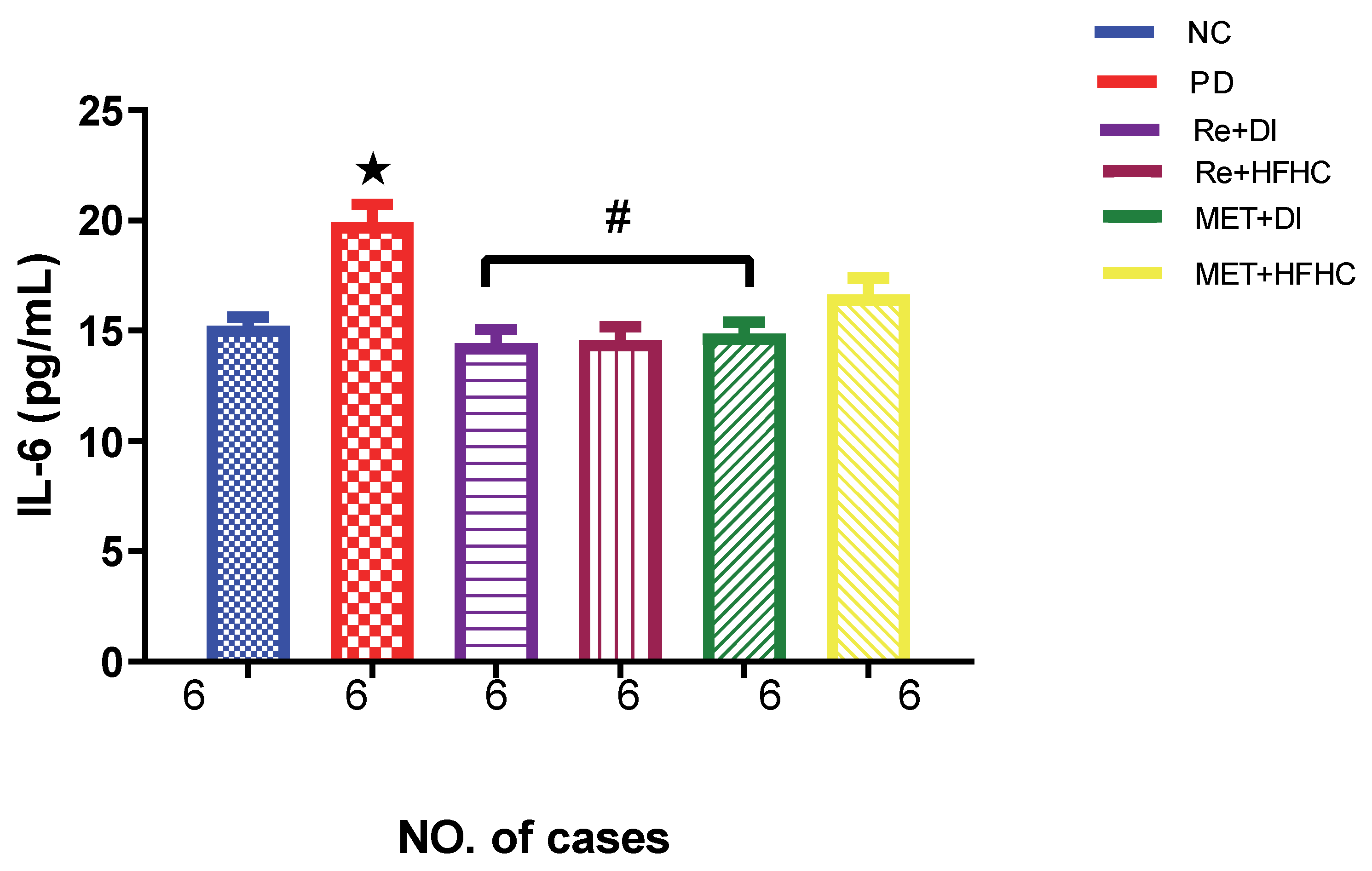
2.3. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Inflammatory Markers: TNF-α and IL-6
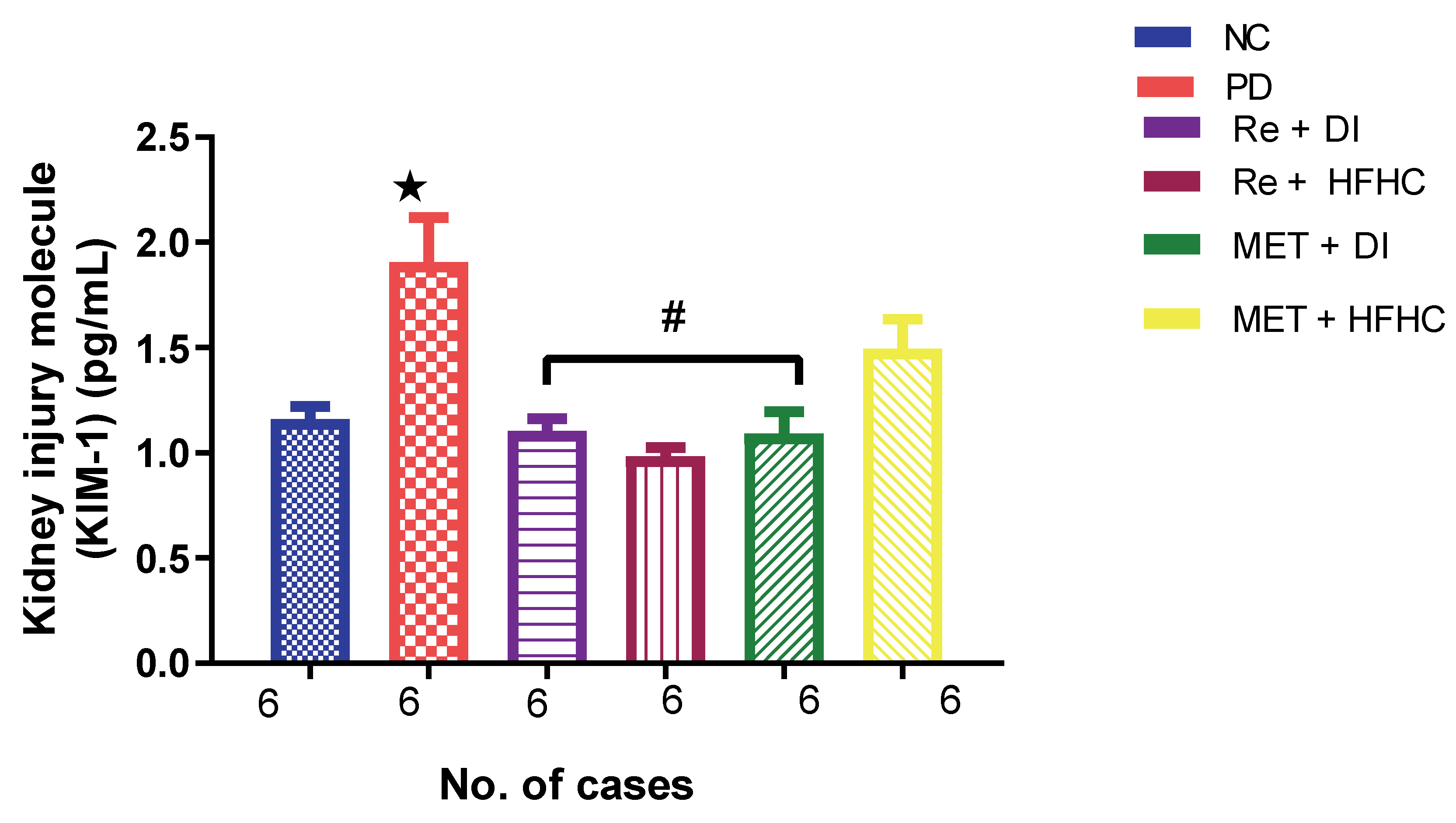
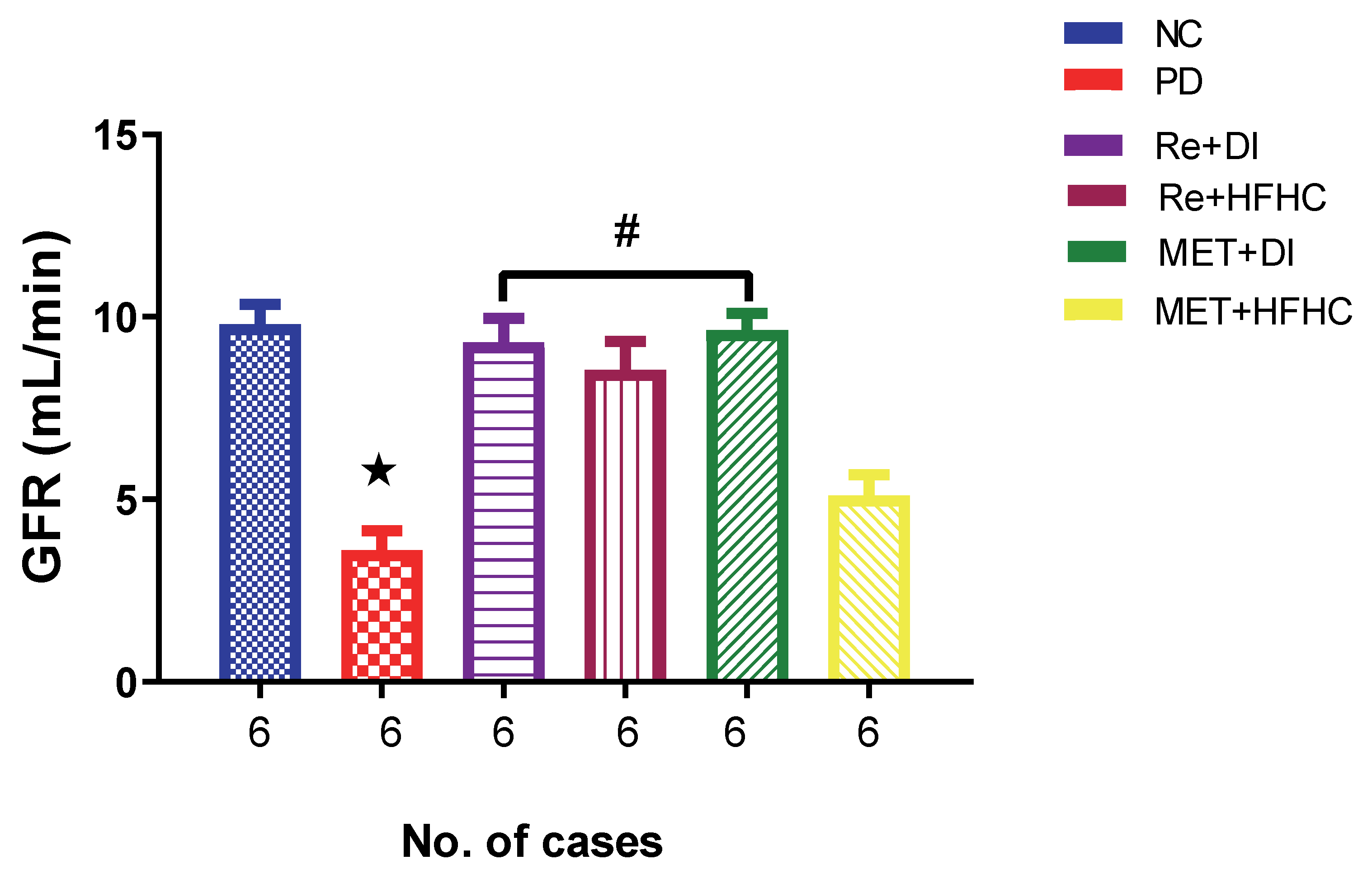
2.4. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on KIM 1 and GFR
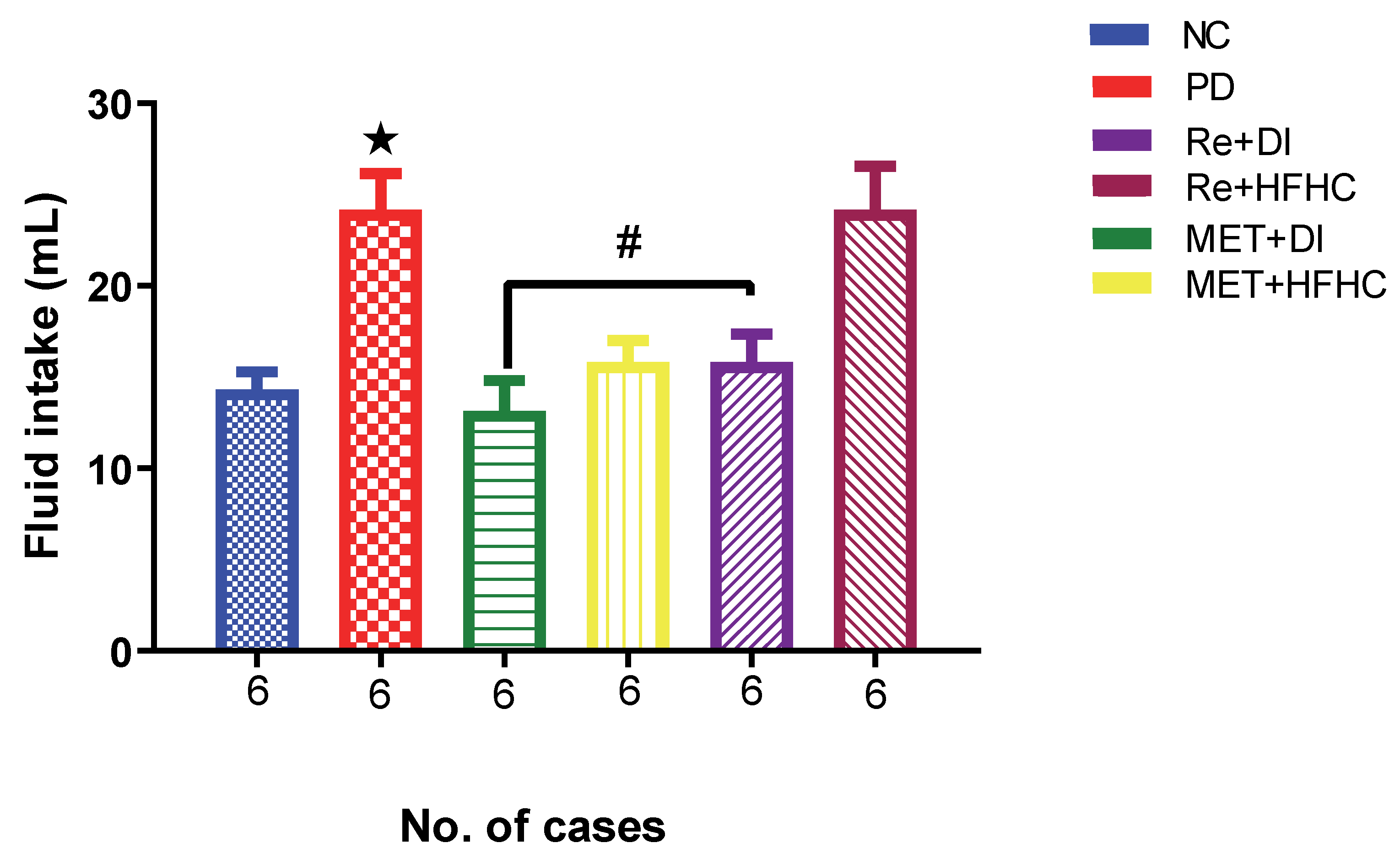
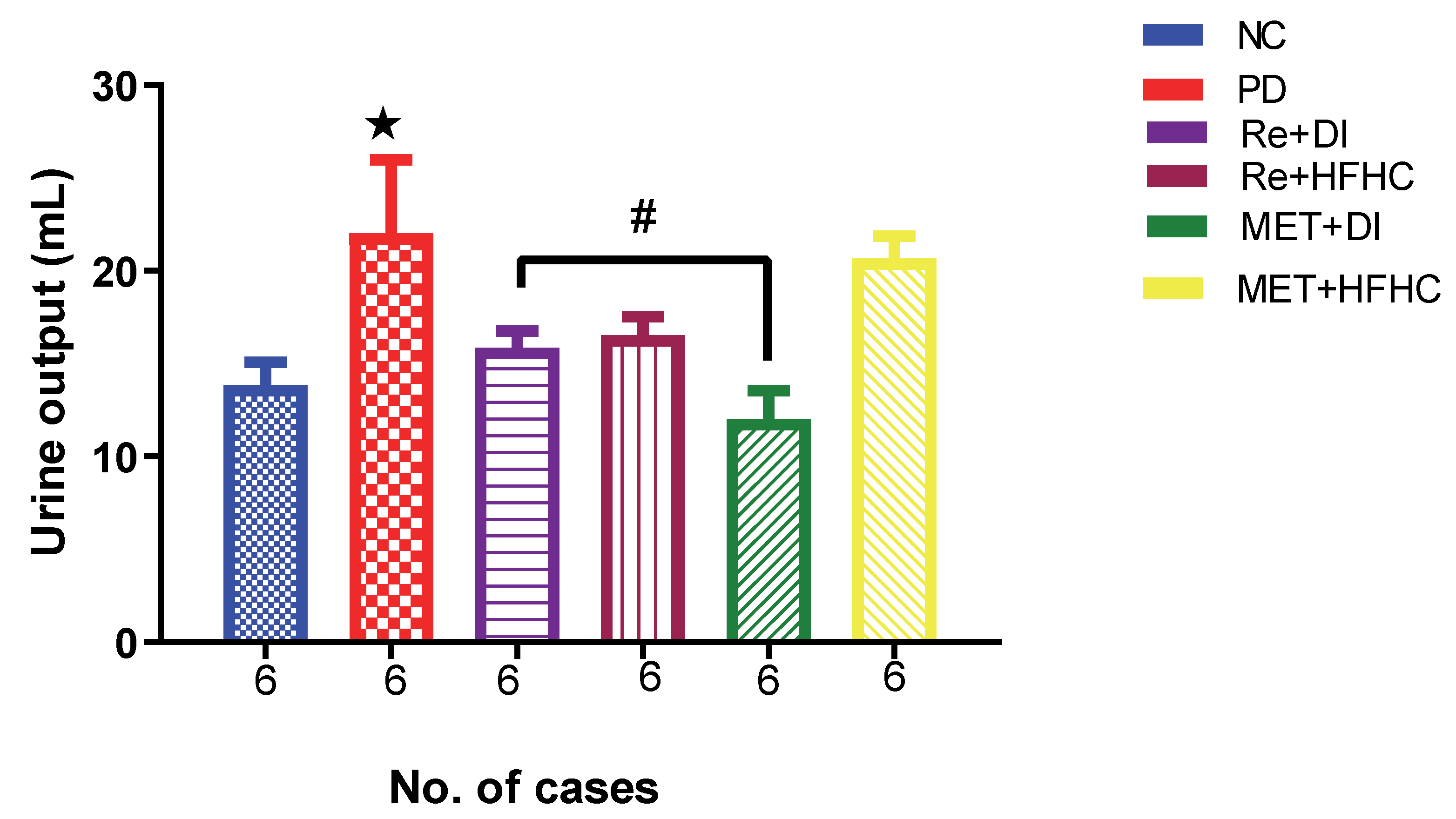
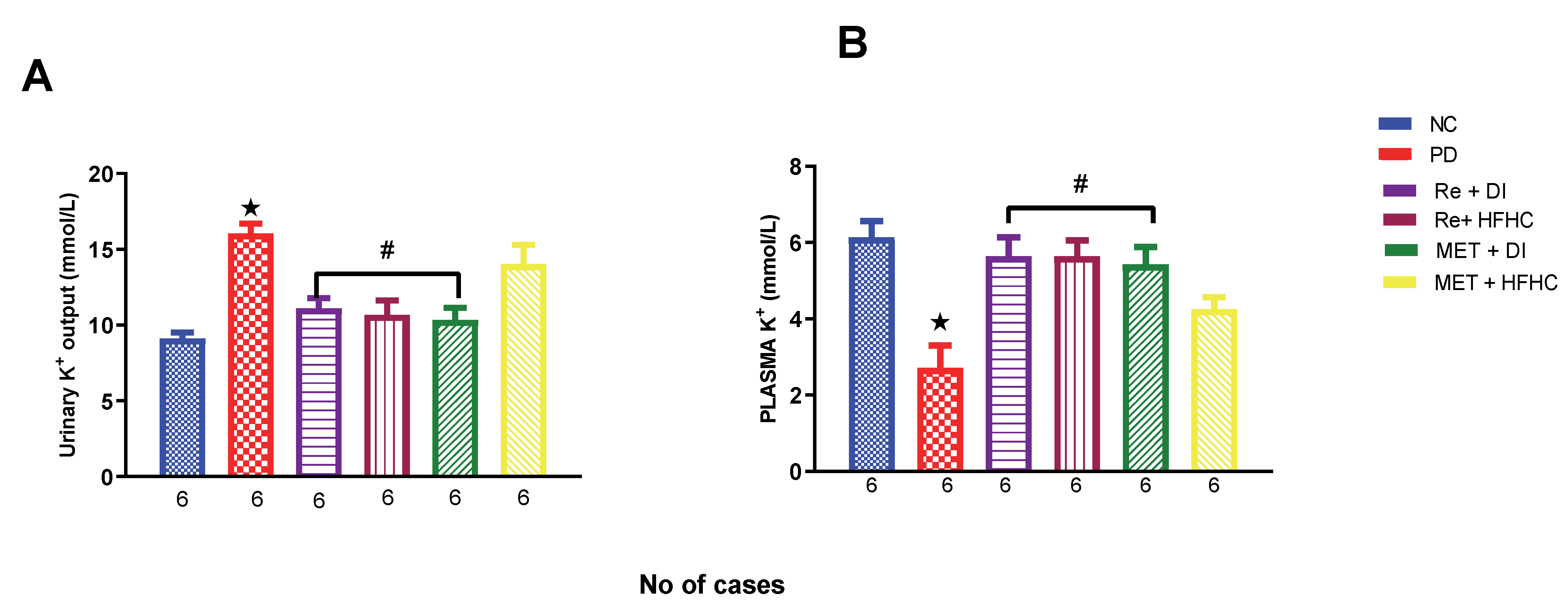
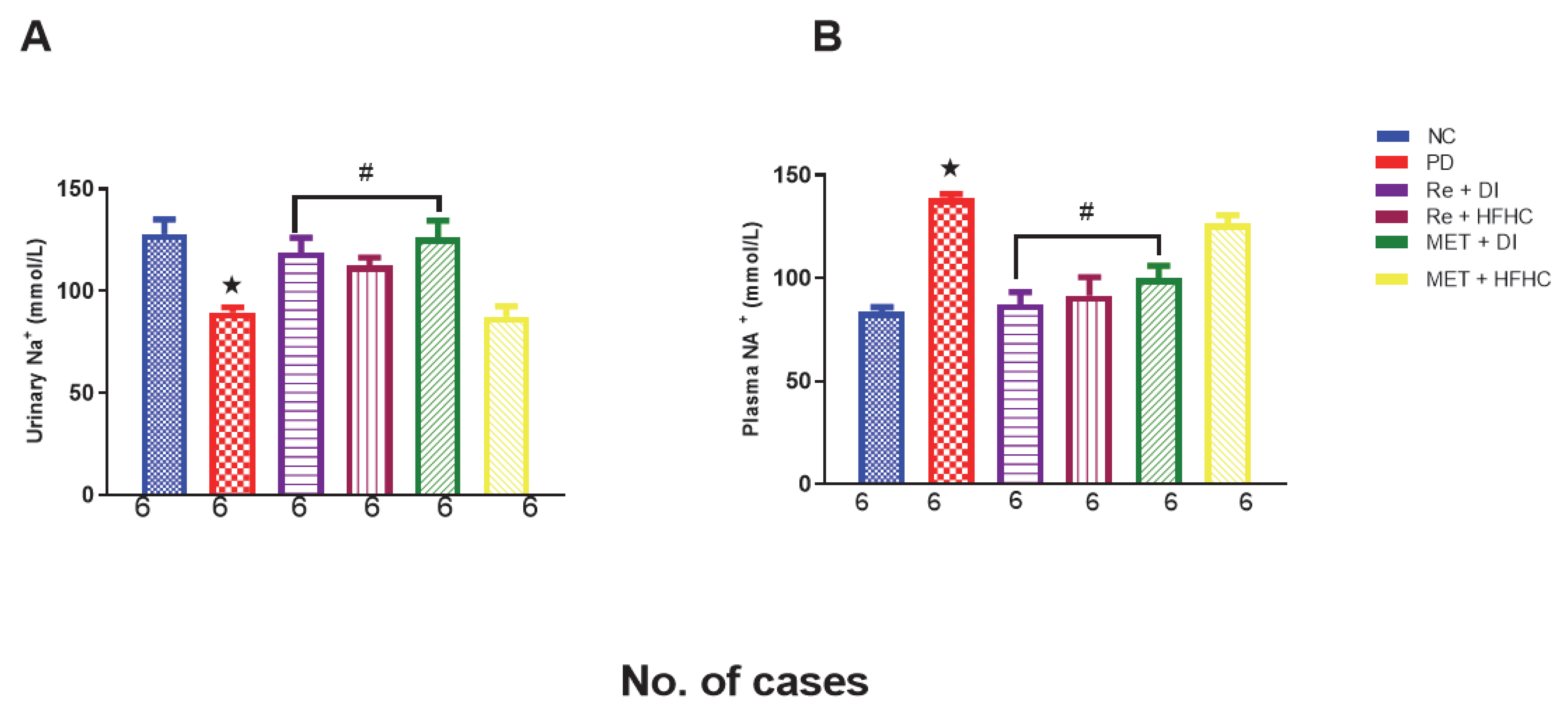
2.5. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Plasma and Urinary Sodium and Potassium (Electrolytes Na+ and K+), Fluid Intake and Urine Output
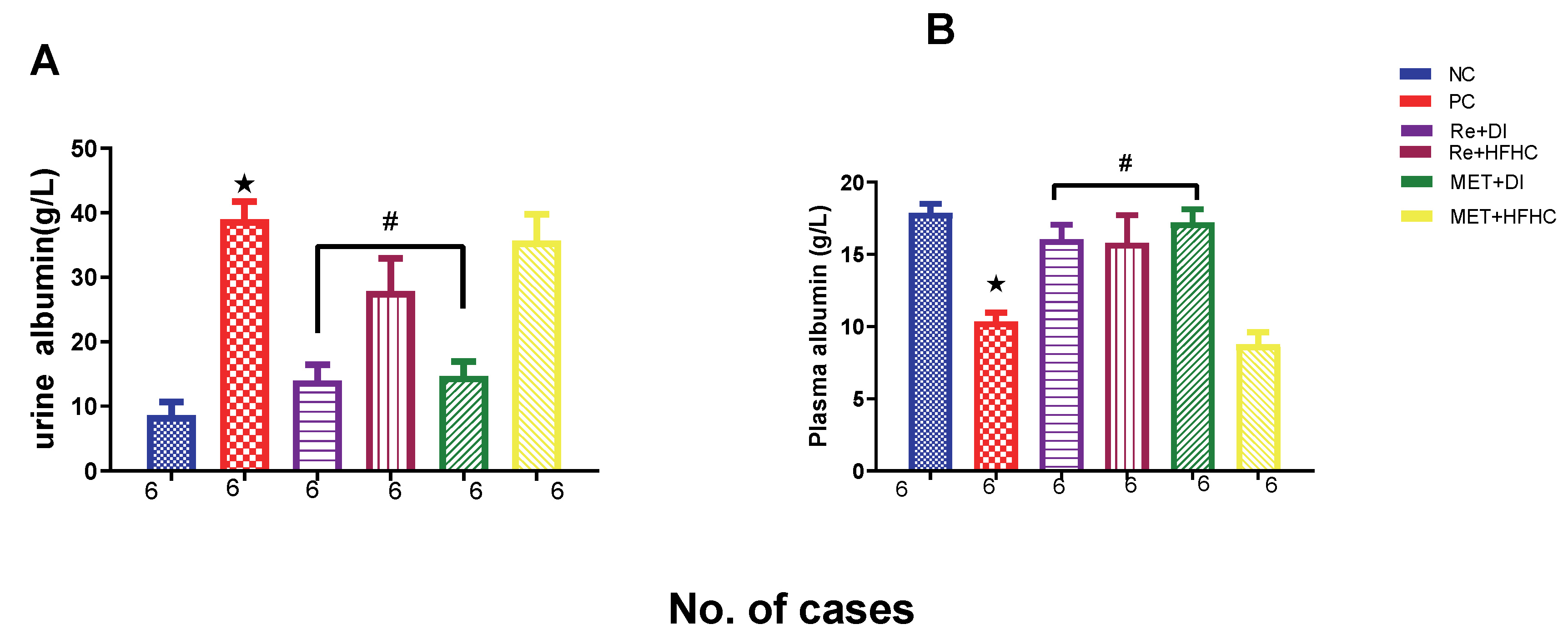
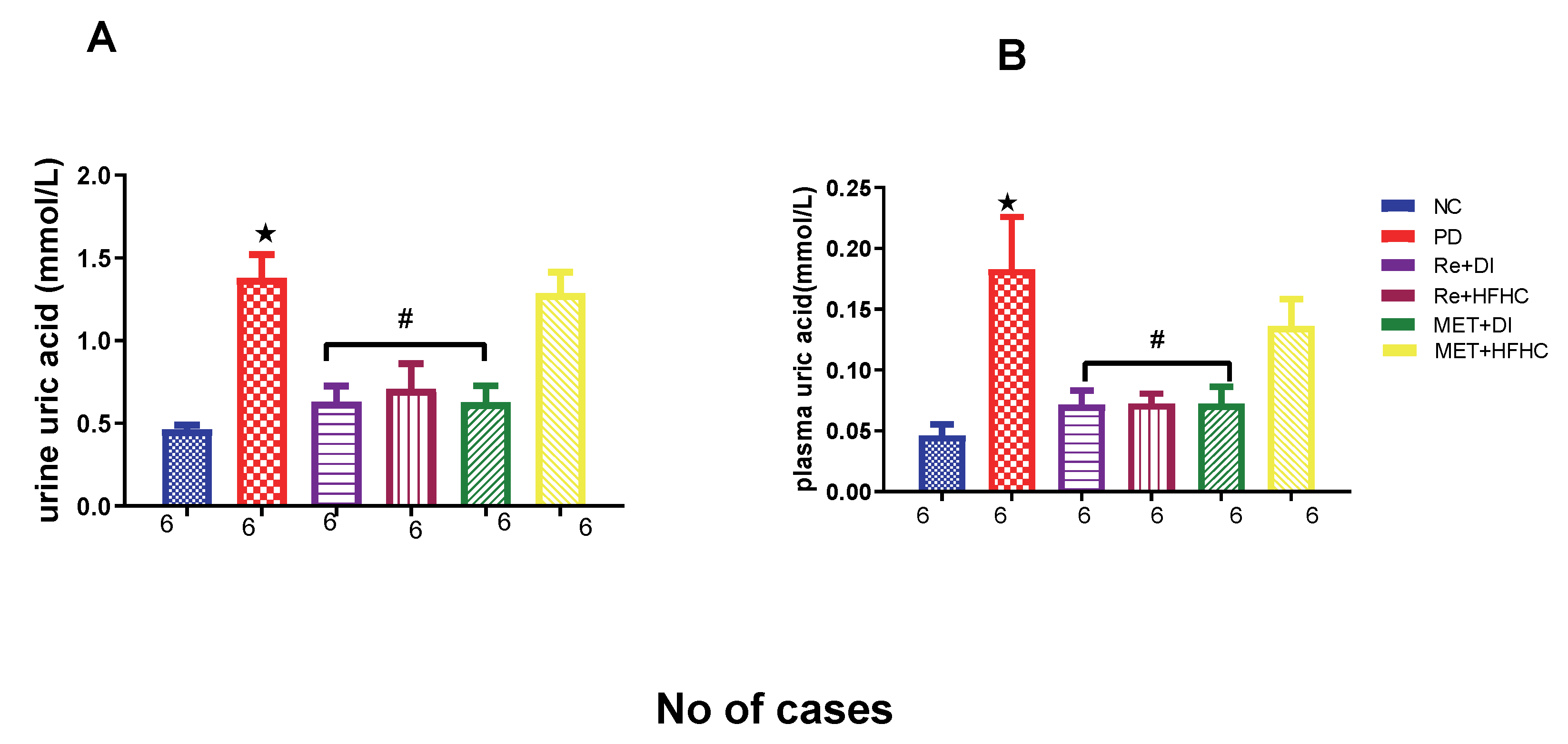
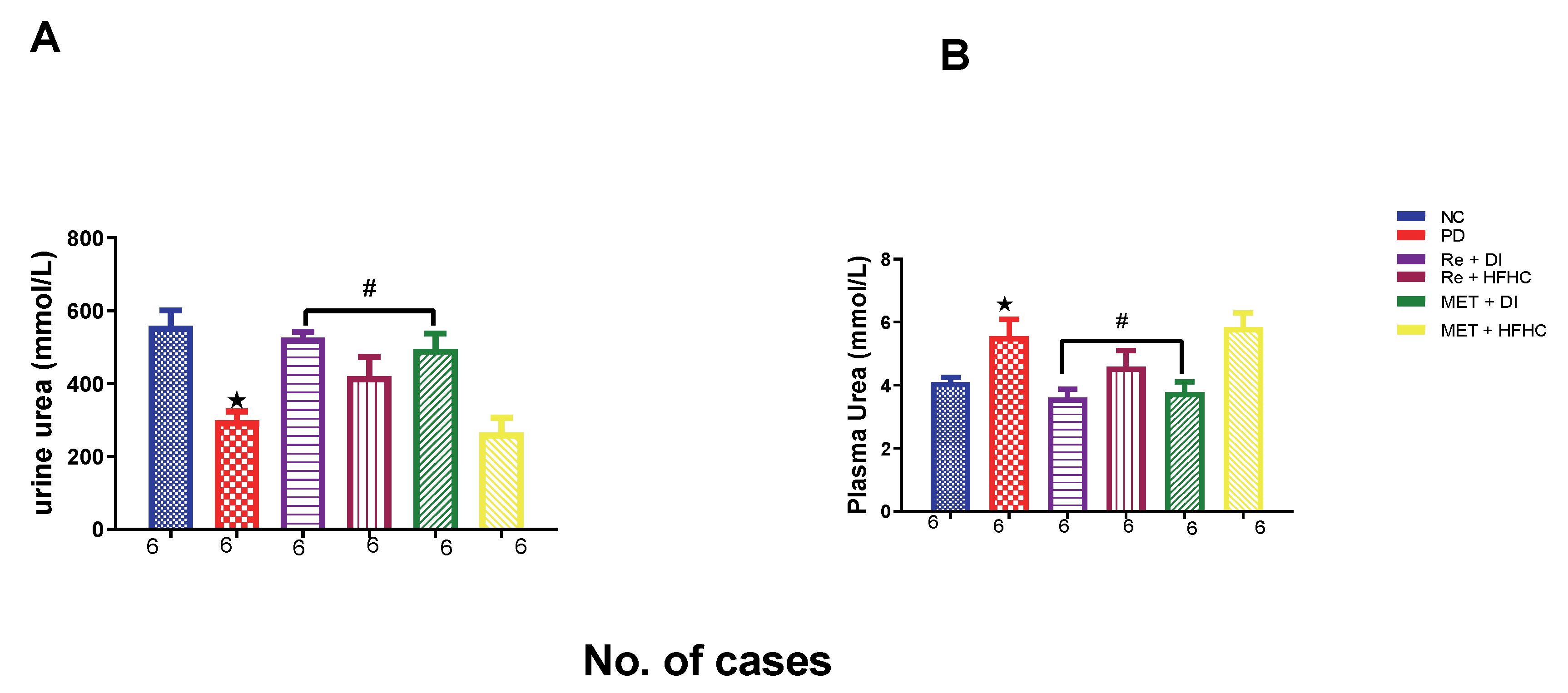
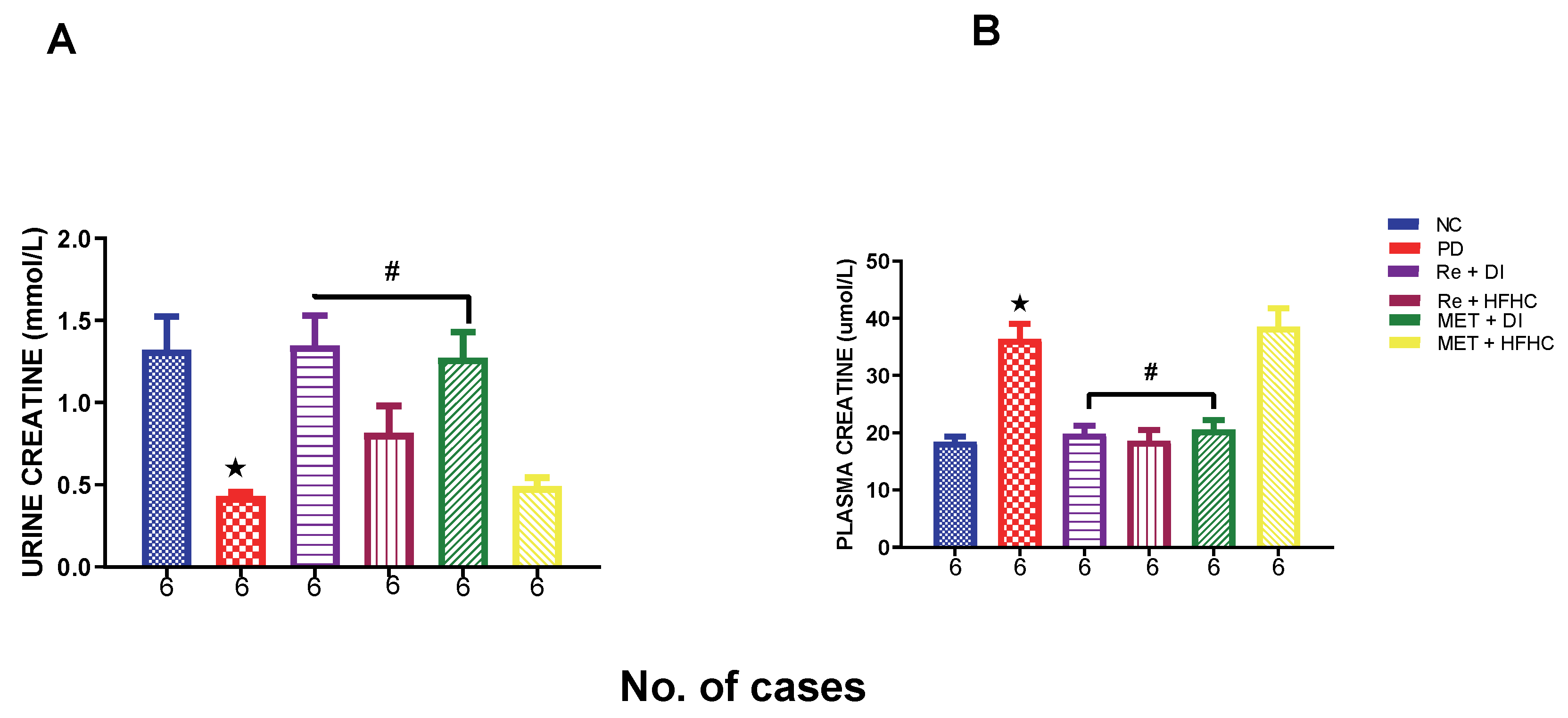
2.6. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Albumin Uric Acid, Urea and Creatinine (Both Plasma and Urine)
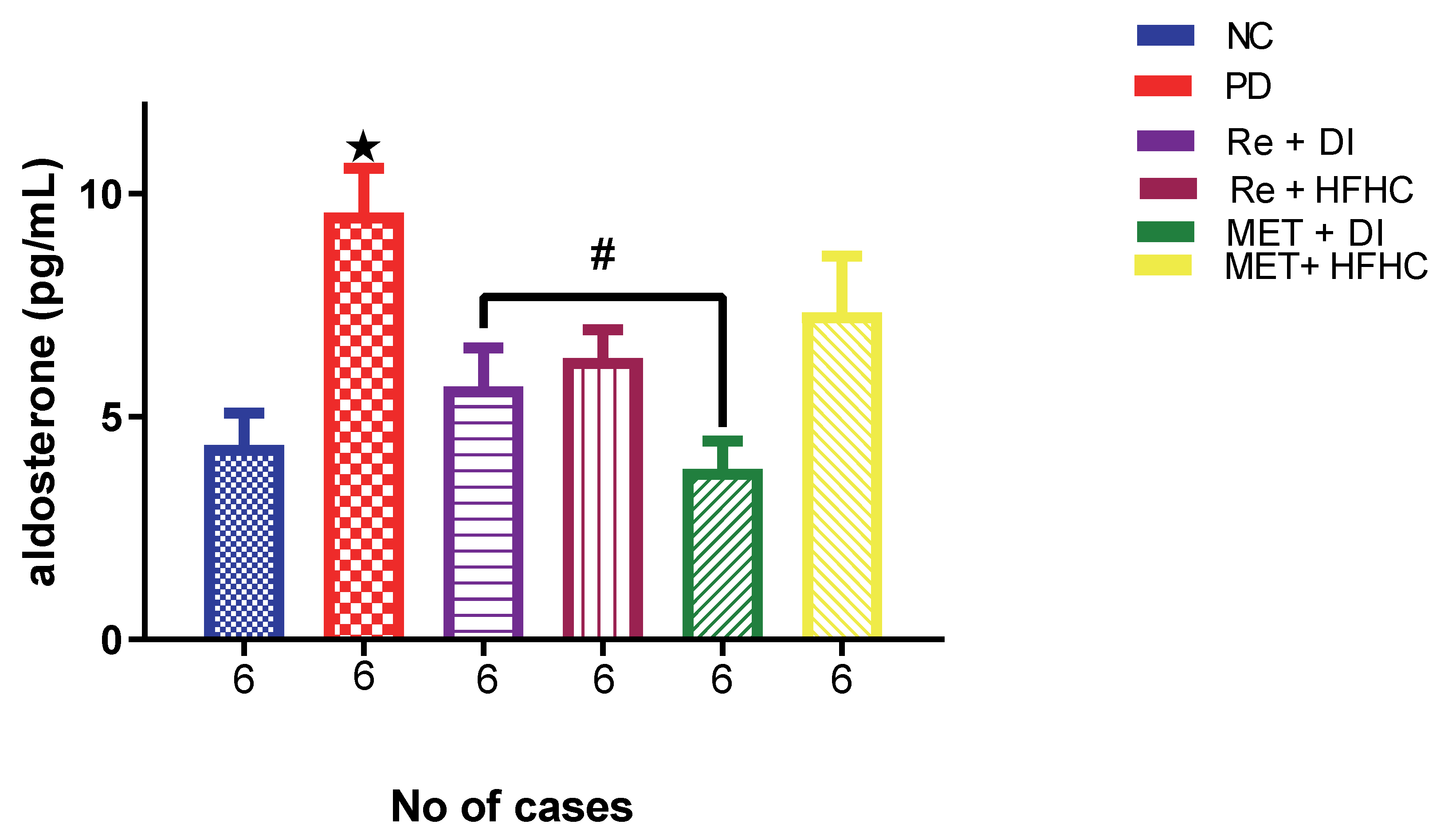
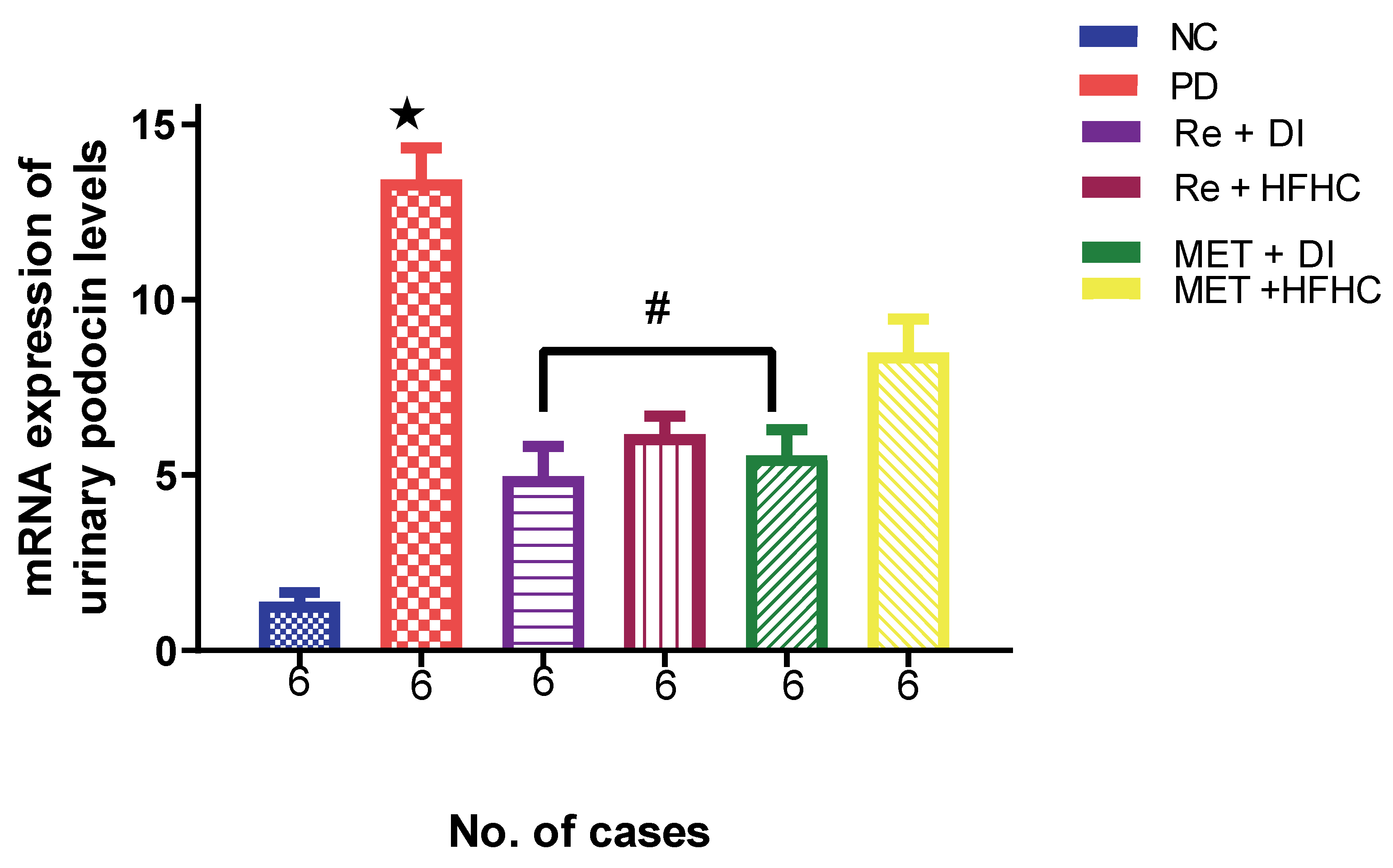
2.7. Effects of Rhenium (V) Compound Administration in the Absence and Presence of Diet Intervention on Aldosterone and Levels of mRNA Expression of Urinary Podocin
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Induction of Prediabetes
4.3. Experimental Design
4.4. Treatment of Prediabetic Animals
4.4.1. Determination of Fluid Intake and Urine Output
4.4.2. Blood Collection and Tissue Harvesting
4.5. Biochemical Analysis
4.5.1. Determination of GFR
4.5.2. Lipid Peroxidation and Antioxidant Status
4.5.3. Urine RNA Isolation
4.5.4. Urine Complementary DNA (cDNA) Synthesis
4.5.5. Real-Time PCR
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hall, J.E.; Mouton, A.J.; da Silva, A.A.; Omoto, A.C.M.; Wang, Z.; Li, X.; Carmo, J.M.D. Obesity, kidney dysfunction, and inflammation: Interactions in hypertension. Cardiovasc. Res. 2021, 117, 1859–1876. [Google Scholar] [CrossRef] [PubMed]
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Vavilis, G.; Bäck, M.; Occhino, G.; Trevisan, M.; Bellocco, R.; Evans, M.; Lindholm, B.; Szummer, K.; Carrero, J.J. Kidney Dysfunction and the Risk of Developing Aortic Stenosis. J. Am. Coll. Cardiol. 2019, 73, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Muskiet, M.H.; Wheeler, D.C.; Heerspink, H.J. Endocrinology. New pharmacological strategies for protecting kidney function in type 2 diabetes. Lancet Diabetes Endocrinol. 2019, 7, 397–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liamis, G.; Liberopoulos, E.; Barkas, F.; Elisaf, M. Diabetes mellitus and electrolyte disorders. World J. Clin. Cases 2014, 2, 488. [Google Scholar] [CrossRef]
- Marks, J.B. Perioperative management of diabetes. Am. Fam. Physician 2003, 67, 93–100. [Google Scholar]
- Olatunji, O.J.; Chen, H.; Zhou, Y. Lycium chinense leaves extract ameliorates diabetic nephropathy by suppressing hyperglycemia mediated renal oxidative stress and inflammation. Biomed. Pharmacother. 2018, 102, 1145–1151. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Atkin, S.L.; Sahebkar, A. A review of the molecular mechanisms of hyperglycemia-induced free radical generation leading to oxidative stress. J. Cell. Physiol. 2019, 234, 1300–1312. [Google Scholar] [CrossRef]
- Bingham, M. Diabetes and Prediabetes Increase Risk of All-Cause Hospitalization. Diabetes Care 2016, 39, 651. [Google Scholar]
- Pecoits-Filho, R.; Abensur, H.; Betônico, C.C.R.; Machado, A.D.; Parente, E.B.; Queiroz, M.; Salles, J.E.N.; Titan, S.; Vencio, S. Interactions between kidney disease and diabetes: Dangerous liaisons. Diabetol. Metab. Syndr. 2016, 8, 50. [Google Scholar] [CrossRef]
- Gioacchini, F.M.; Albera, R.; Re, M.; Scarpa, A.; Cassandro, C.; Cassandro, E. Hyperglycemia and diabetes mellitus are related to vestibular organs dysfunction: Truth or suggestion? A literature review. Acta Diabetol. 2018, 55, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Farrokhi, F.R.; Rezaee, R.; Sahebkar, A. Oxidative stress induces renal failure: A review of possible molecular pathways. J. Cell. Biochem. 2018, 119, 2990–2998. [Google Scholar] [CrossRef] [PubMed]
- Napoleone, L.; Solé, C.; Juanola, A.; Ma, A.T.; Carol, M.; Pérez-Guasch, M.; Rubio, A.B.; Cervera, M.; Avitabile, E.; Bassegoda, O.; et al. Patterns of kidney dysfunction in acute-on-chronic liver failure: Relationship with kidney and patients’ outcome. Hepatol. Commun. 2022, 6, 2121–2131. [Google Scholar] [CrossRef]
- Marre, M. Importance of intensive blood pressure control in type 2 diabetes: Mechanisms, treatments and current guidelines. Diabetes Obes. Metab. 2020, 22, 33–42. [Google Scholar] [CrossRef]
- Bergmark, B.A.; Bhatt, D.L.; McGuire, D.K.; Cahn, A.; Mosenzon, O.; Steg, P.G.; Im, K.; Kanevsky, E.; Gurmu, Y.; Raz, I.; et al. Metformin use and clinical outcomes among patients with diabetes mellitus with or without heart failure or kidney dysfunction: Observations from the SAVOR-TIMI 53 trial. Circulation 2019, 140, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Kim, Y.C.; Park, J.Y.; Lee, J.; An, J.N.; Kim, C.T.; Oh, S.; Park, S.; Kim, D.K.; Oh, Y.K.; et al. The Long-term Effects of Metformin on Patients With Type 2 Diabetic Kidney Disease. Diabetes Care 2020, 43, 948–955. [Google Scholar] [CrossRef]
- Hsu, W.-H.; Hsiao, P.-J.; Lin, P.-C.; Chen, S.-C.; Lee, M.-Y.; Shin, S.-J. Effect of metformin on kidney function in patients with type 2 diabetes mellitus and moderate chronic kidney disease. Oncotarget 2018, 9, 5416–5423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siboto, A.; Akinnuga, A.M.; Khumalo, B.N.; Ismail, M.B.; Booysen, I.N.; Sibiya, N.H.; Ngubane, P.S.; Khathi, A. The effects of a [3+1] oxo-free rhenium (V) compound with uracil-derived ligands on selected parameters of glucose homeostasis in diet-induced pre-diabetic rats. Obes. Med. 2020, 19, 100258. [Google Scholar] [CrossRef]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: Examining the links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar]
- Siboto, A.; Akinnuga, A.M.; Ismail, M.B.; Booysen, I.N.; Sibiya, N.H.; Ngubane, P.; Khathi, A. Investigating the Protective Effects of a Rhenium (V) Compound with Uracil-Derived Ligands on Liver Damage Associated with Prediabetes in Diet-Induced Prediabetic Rats. Diabetology 2022, 3, 524–538. [Google Scholar] [CrossRef]
- Ismail, M.B.; Booysen, I.N.; Akerman, M.P. DNA interaction studies of rhenium compounds with Schiff base chelates encompassing biologically relevant moieties. Nucleosides, Nucleotides Nucleic Acids 2019, 38, 950–971. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.B. Complexes of the Facial Tricarbonyl Rhenium (I) and Oxorhenium (V) Moieties with Aromatic, Multidentate, N-donor Ligands. Ph.D. Dissertation, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2013. [Google Scholar]
- Maisuls, I.; Wolcan, E.; Piro, O.E.; Castellano, E.E.; Petroselli, G.; Erra-Balsells, R.; Cabrerizo, F.M.; Ruiz, G.T. Synthesis, Structural Characterization and Biological Evaluation of Rhenium (I) Tricarbonyl Complexes with β-Carboline Ligands. ChemistrySelect 2017, 2, 8666–8672. [Google Scholar] [CrossRef]
- Rusanov, D.A.; Zou, J.; Babak, M.V. Biological Properties of Transition Metal Complexes with Metformin and Its Analogues. Pharm. 2022, 15, 453. [Google Scholar] [CrossRef] [PubMed]
- Rafique, S.; Idrees, M.; Nasim, A.; Akbar, H.; Athar, A. Transition metal complexes as potential therapeutic agents. Biotechnol. Mol. Biol. Rev. 2010, 5, 38–45. [Google Scholar]
- Hu, X.; Rong, S.; Wang, Q.; Sun, T.; Bao, W.; Chen, L.; Liu, L. Association between plasma uric acid and insulin resistance in type 2 diabetes: A Mendelian randomization analysis. Diabetes Res. Clin. Pr. 2021, 171, 108542. [Google Scholar] [CrossRef]
- Baker, C.; Retzik-Stahr, C.; Singh, V.; Plomondon, R.; Anderson, V.; Rasouli, N. Should metformin remain the first-line therapy for treatment of type 2 diabetes? Ther. Adv. Endocrinol. Metab. 2021, 12, 2042018820980225. [Google Scholar] [CrossRef]
- Dave, G.; Kalia, K. Hyperglycemia induced oxidative stress in type-1 and type-2 diabetic patients with and without nephropathy. Cell Mol. Biol. (Noisy-le-Grand) 2007, 53, 68–78. [Google Scholar]
- Yan, L.j. Redox imbalance stress in diabetes mellitus: Role of the polyol pathway. Anim. Model. Exp. Med. 2018, 1, 7–13. [Google Scholar] [CrossRef]
- Luc, K.; Schramm-Luc, A.; Guzik, T.; Mikolajczyk, T.J. Oxidative stress and inflammatory markers in prediabetes and diabetes. J. Physiol. Pharmacol. 2019, 70, 111–113. [Google Scholar]
- Luvuno, M.; Kathi, A.; Mabandla, M. Voluntary Ingestion of a High-Fat High-Carbohydrate Diet: A Model for Prediabetes. Master’s Dissertation, University of KwaZulu-Natal, KwaZulu-Natal, South Africa, 2017. [Google Scholar]
- Mkhize, B.C.; Mosili, P.; Ngubane, P.S.; Sibiya, N.H.; Khathi, A. Diet-induced prediabetes: Effects on the activity of the renin–angiotensin–aldosterone system in selected organs. J. Diabetes Investig. 2022, 13, 768–780. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Z.; Sun, W.; Tan, Y.; Liu, Y.; Zheng, Y.; Liu, Q.; Cai, L.; Sun, J. Sulforaphane Attenuation of Type 2 Diabetes-Induced Aortic Damage Was Associated with the Upregulation of Nrf2 Expression and Function. Oxidative Med. Cell. Longev. 2014, 2014, 123963. [Google Scholar] [CrossRef] [Green Version]
- David, J.A.; Rifkin, W.J.; Rabbani, P.S.; Ceradini, D.J. The Nrf2/Keap1/ARE pathway and oxidative stress as a therapeutic target in type II diabetes mellitus. J. Diabetes Res. 2017, 2017, 4826724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero-Hue, M.; Rayego-Mateos, S.; Vázquez-Carballo, C.; Palomino-Antolín, A.; García-Caballero, C.; Opazo-Rios, L.; Morgado-Pascual, J.L.; Herencia, C.; Mas, S.; Ortiz, A.; et al. Protective Role of Nrf2 in Renal Disease. Antioxidants 2020, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; An, E.J.; Kim, J.; Bae, Y.S. Function of NADPH oxidases in diabetic nephropathy and development of Nox inhibitors. Biomol. Ther. 2020, 28, 25. [Google Scholar] [CrossRef]
- Jeong, B.Y.; Lee, H.Y.; Park, C.G.; Kang, J.; Yu, S.-L.; Choi, D.-R.; Han, S.-Y.; Park, M.H.; Cho, S.; Lee, S.Y.; et al. Oxidative stress caused by activation of NADPH oxidase 4 promotes contrast-induced acute kidney injury. PLoS ONE 2018, 13, e0191034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagoo, M.K.; Gnudi, L. Diabetic nephropathy: Is there a role for oxidative stress? Free. Radic. Biol. Med. 2018, 116, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.C. Targeting the Pathobiology of Diabetic Kidney Disease. Adv. Chronic Kidney Dis. 2021, 28, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Sibiya, N.; Mabandla, M. The application of pectin-insulin patch on streptozotocin-induced diabetic rats: Implications in the hippocampal function. J. Diabetes. Metabol. 2017, 8, 12. [Google Scholar] [CrossRef]
- Lay, A.C.; Barrington, A.F.; Hurcombe, J.A.; Ramnath, R.D.; Graham, M.; Lewis, P.A.; Wilson, M.C.; Heesom, K.J.; Butler, M.J.; Perrett, R.M.; et al. A role for NPY-NPY2R signaling in albuminuric kidney disease. Proc. Natl. Acad. Sci. USA 2020, 117, 15862–15873. [Google Scholar] [CrossRef]
- Lay, A.C.; Coward, R.J. The evolving importance of insulin signaling in podocyte health and disease. Front. Endocrinol. 2018, 9, 693. [Google Scholar] [CrossRef] [Green Version]
- Mabuza, L.P.; Gamede, M.W.; Maikoo, S.; Booysen, I.N.; Ngubane, P.S.; Khathi, A. Amelioration of risk factors associated with diabetic nephropathy in diet-induced pre-diabetic rats by an uracil-derived diimine ruthenium (II) compound. Biomed. Pharmacother. 2020, 129, 110483. [Google Scholar] [CrossRef] [PubMed]
- Donate-Correa, J.; Martín-Núñez, E.; Muros-de-Fuentes, M.; Mora-Fernández, C.; Navarro-González, J.F. Inflammatory cytokines in diabetic nephropathy. J. Diabetes Res. 2015, 2015, 948417. [Google Scholar] [CrossRef] [PubMed]
- Sindhughosa, D.A.; Pranamartha, A. The involvement of proinflammatory cytokines in diabetic nephropathy: Focus on interleukin 1 (IL-1), interleukin 6 (IL-6), and tumor necrosis factor-alpha (TNF-α) signaling mechanism. Bali Med. J. 2017, 201, 1. [Google Scholar] [CrossRef]
- Pedruzzi, L.M.; Stockler-Pinto, M.B.; Leite, M., Jr.; Mafra, D. Nrf2–keap1 system versus NF-κB: The good and the evil in chronic kidney disease? Biochimie 2012, 94, 2461–2466. [Google Scholar] [CrossRef]
- Teixeira, T.M.; da Costa, D.C.; Resende, A.C.; Soulage, C.O.; Bezerra, F.F.; Daleprane, J.B. Activation of Nrf2-antioxidant signaling by 1, 25-dihydroxycholecalciferol prevents leptin-induced oxidative stress and inflammation in human endothelial cells. J. Nutr. 2017, 147, 506–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakai, K.; Fujii, H.; Kono, K.; Goto, S.; Kitazawa, R.; Kitazawa, S.; Hirata, M.; Shinohara, M.; Fukagawa, M.; Nishi, S. Vitamin D Activates the Nrf2-Keap1 Antioxidant Pathway and Ameliorates Nephropathy in Diabetic Rats. Am. J. Hypertens. 2014, 27, 586–595. [Google Scholar] [CrossRef]
- Armato, J.P.; DeFronzo, R.A.; Abdul-Ghani, M.; Ruby, R.J. Successful treatment of prediabetes in clinical practice using physiological assessment (STOP DIABETES). Lancet Diabetes Endocrinol. 2018, 6, 781–789. [Google Scholar] [CrossRef]
- Braunwald, E. Diabetes, heart failure, and renal dysfunction: The vicious circles. Prog. Cardiovasc. Dis. 2019, 62, 298–302. [Google Scholar] [CrossRef]
- Thomas, M.C.; Cherney, D.Z. The actions of SGLT2 inhibitors on metabolism, renal function and blood pressure. Diabetologia 2018, 61, 2098–2107. [Google Scholar] [CrossRef] [Green Version]
- Freeman, A.M.; Pennings, N. Insulin Resistance; StatPearls Publishing: Lumberton, NC, USA, 2021. [Google Scholar]
- Kawasoe, S.; Maruguchi, Y.; Kajiya, S.; Uenomachi, H.; Miyata, M.; Kawasoe, M.; Kubozono, T.; Ohishi, M. Mechanism of the blood pressure-lowering effect of sodium-glucose cotransporter 2 inhibitors in obese patients with type 2 diabetes. BMC Pharmacol. Toxicol. 2017, 18, 23. [Google Scholar] [CrossRef] [Green Version]
- Flory, J.; Lipska, K. Metformin in 2019. JAMA 2019, 321, 1926–1927. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G.; Penno, G.; Natali, A.; Barutta, F.; Di Paolo, S.; Reboldi, G.; Gesualdo, L.; De Nicola, L.; Society, I.D. Diabetic kidney disease: New clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on “The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function”. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1127–1150. [Google Scholar] [PubMed] [Green Version]
- Sluijs, I.; Beulens, J.W.; Van Der, A.D.L.; Spijkerman, A.M.; Schulze, M.B.; Van Der Schouw, Y.T. Plasma uric acid is associated with increased risk of type 2 diabetes independent of diet and metabolic risk factors. J. Nutr. 2013, 143, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Bonito, P.; Valerio, G.; Licenziati, M.R.; Campana, G.; Del Giudice, E.M.; Di Sessa, A.; Morandi, A.; Maffeis, C.; Chiesa, C.; Pacifico, L.; et al. Uric acid, impaired fasting glucose and impaired glucose tolerance in youth with overweight and obesity. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 675–680. [Google Scholar] [CrossRef]
- Mkhize, B.; Mosili, P.; Ngubane, P.; Sibiya, N.; Khathi, A. Diet-induced prediabetes: Effects on the systemic and renal renin-angiotensin-aldosterone system. J. Diabetes Invest. 2020, 13, 768–780. [Google Scholar] [CrossRef]
- Araki, S.-i.; Haneda, M.; Koya, D.; Kondo, K.; Tanaka, S.; Arima, H.; Kume, S.; Nakazawa, J.; Chin-Kanasaki, M.; Ugi, S.; et al. Urinary potassium excretion and renal and cardiovascular complications in patients with type 2 diabetes and normal renal function. Clin. J. Am. Soc. Nephrol. 2015, 10, 2152–2158. [Google Scholar] [CrossRef]
- Reed, J.W. Impact of sodium–glucose cotransporter 2 inhibitors on blood pressure. Vasc. Health Risk Manag. 2016, 12, 393. [Google Scholar] [CrossRef] [Green Version]
- Mbatha, B.; Khathi, A.; Sibiya, N.; Booysen, I.; Mangundu, P.; Ngubane, P. Cardio-protective effects of a dioxidovanadium (V) complex in male sprague–dawley rats with streptozotocin-induced diabetes. BioMetals 2021, 34, 161–173. [Google Scholar] [CrossRef]
- Luvuno, M.; Mbongwa, H.; Khathi, A. Development of a novel prediabetes animal model using a high fat high carbohydrate diet: Implications for type 2 diabetes. PLoS ONE 2017, 13, 8–14. [Google Scholar]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Heikes, K.E.; Eddy, D.M.; Arondekar, B.; Schlessinger, L. Diabetes Risk Calculator: A simple tool for detecting undiagnosed diabetes and pre-diabetes. Diabetes Care 2008, 31, 1040–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mkhwanazi, B.N.; Serumula, M.R.; Myburg, R.B.; Van Heerden, F.R.; Musabayane, C.T. Antioxidant effects of maslinic acid in livers, hearts and kidneys of streptozotocin-induced diabetic rats: Effects on kidney function. Ren. Fail. 2014, 36, 419–431. [Google Scholar] [CrossRef] [PubMed]



















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siboto, A.; Akinnuga, A.M.; Khumalo, B.; Ismail, M.B.; Booysen, I.N.; Sibiya, N.H.; Ngubane, P.; Khathi, A. Ameliorative Effects of a Rhenium (V) Compound with Uracil-Derived Ligand Markers Associated with Hyperglycaemia-Induced Renal Dysfunction in Diet-Induced Prediabetic Rats. Int. J. Mol. Sci. 2022, 23, 15400. https://doi.org/10.3390/ijms232315400
Siboto A, Akinnuga AM, Khumalo B, Ismail MB, Booysen IN, Sibiya NH, Ngubane P, Khathi A. Ameliorative Effects of a Rhenium (V) Compound with Uracil-Derived Ligand Markers Associated with Hyperglycaemia-Induced Renal Dysfunction in Diet-Induced Prediabetic Rats. International Journal of Molecular Sciences. 2022; 23(23):15400. https://doi.org/10.3390/ijms232315400
Chicago/Turabian StyleSiboto, Angezwa, Akinjide Moses Akinnuga, Bongiwe Khumalo, Muhammed Bilaal Ismail, Irvin Noel Booysen, Ntethelelo Hopewell Sibiya, Phikelelani Ngubane, and Andile Khathi. 2022. "Ameliorative Effects of a Rhenium (V) Compound with Uracil-Derived Ligand Markers Associated with Hyperglycaemia-Induced Renal Dysfunction in Diet-Induced Prediabetic Rats" International Journal of Molecular Sciences 23, no. 23: 15400. https://doi.org/10.3390/ijms232315400