
A Reduced Tryptophan Diet in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome Improves Their Abdominal Symptoms and Their Quality of Life through Reduction of Serotonin Levels and Its Urinary Metabolites

 , , and
, , and
Abstract
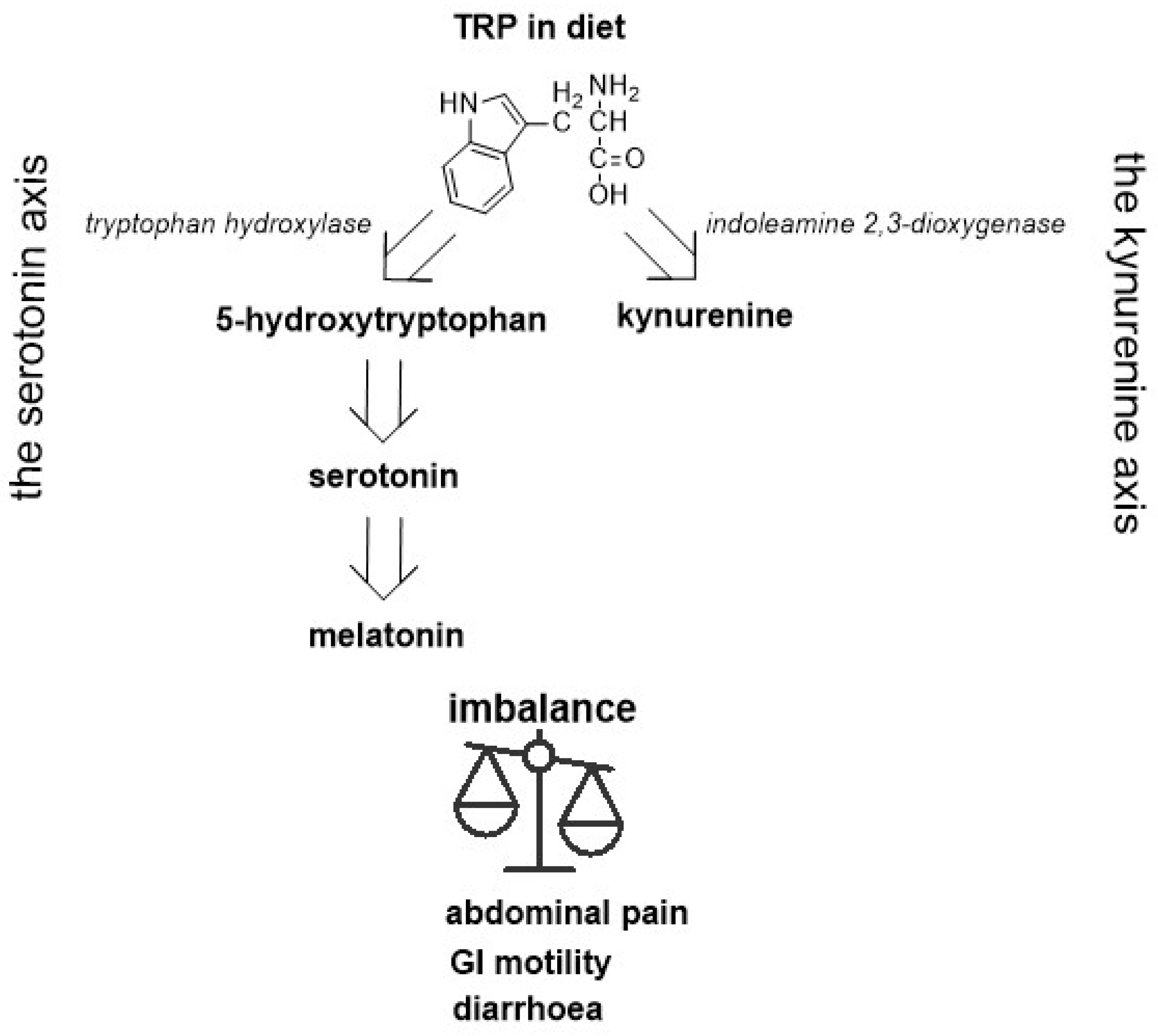
:1. Introduction
2. Results
2.1. Baseline Comparison between Control and Intervention Group
2.2. Pre and Post-Intervention Findings for the IBS-D Group
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Diagnostic Procedures
4.3. Laboratory Tests
4.4. Dietary Treatment
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bassotti, G. Irritable Bowel Syndrome: A Multifaceted World Still to Discover. J. Clin. Med. 2022, 11, 4103. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Patel, N.K. Rome Criteria and a Diagnostic Approach to Irritable Bowel Syndrome. J. Clin. Med. 2017, 6, 99. [Google Scholar] [CrossRef]
- Cangemi, D.J.; Lacy, B.E. Management of irritable bowel syndrome with diarrhoea: A review of nonpharmacological and pharmacological interventions. Ther. Adv. Gastroenterol. 2019, 12, 1756284819878950. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Ford, A.C. Pharmacotherapy for Irritable Bowel Syndrome. J. Clin. Med. 2017, 6, 101. [Google Scholar] [CrossRef] [Green Version]
- Zia, J.; Chung, C.-F.; Xu, K.; Dong, Y.; Schenk, J.; Cain, C.; Munson, S.; Heitkemper, M.M. Inter-Rather Reliability of Provider Interpretations of Irritable Bowel Syndrome Food and Symptom. J. Clin. Med. 2017, 6, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakudo, S.; Okumura, T.; Inamori, M.; Okuyama, Y.; Kanazawa, M.; Kamiya, T.; Sato, K.; Shiotani, A.; Fujikawa, Y.; Hokari, R.; et al. Evidence-based clinical practice guidelines for irritable bowel syndrome 2020. J. Gastroenterol. 2021, 56, 193–217. [Google Scholar] [CrossRef]
- Rej, A.; Aziz, I.; Tornblom, H.; Sanders, D.S.; Simrén, M. The role of the diet in irritable bowel syndrome: Indications for dietary 849 advice. J. Int. Med. 2019, 286, 490–502. [Google Scholar] [CrossRef] [Green Version]
- Barmeyer, C.; Schumann, M. Long-term response to gluten-free diet as evidence for non-celiac wheat sensitivity in one third 876 of patients with diarrhoea–dominant and mixed-type irritable bowel syndrome. Int. J. Colorect. Dis. 2017, 32, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Austin, G.L.; Dalton, C.B.; Hu, Y.; Morris, C.B.; Hankins, J.; Weinland, S.R.; Westman, E.C.; Yancy, W.S.; Drossman, D.A. A very low-carbohydrate diet improves symptoms and quality of life in diarrhea-predominant irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2009, 7, 706–708. [Google Scholar] [CrossRef] [Green Version]
- Varjú, P.; Gede, N.; Szakacs, Z.; Hegyi, P.; Cazacu, I.M.; Pecsi, D.; Fabian, A.; Szeepes, Z.; Vincze, A.; Tenk, J.; et al. Lactose intolerance but not lactose maldigestion is more frequent in patients with irritable bowel syndrome than in healthy controls: A meta-analysis. Neurogastroenterol. Motil. 2019, 31, 13527. [Google Scholar] [CrossRef]
- Cancarevic, I.; Rehman, M.; Iskander, B.; Lalani, S.; Malik, B.H. Is there a correlation between irritable bowel syndrome and lactose intolerance? Cureus 2020, 12, e6710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.K.; Kraft, N.; Zimmerman, B.; Jackson, M.; Rao, S.S.C. Fructose intolerance in IBS and utility of fructose-restricted diet. J. Clin. Gastroenterol. 2008, 42, 233–238. [Google Scholar] [CrossRef]
- Zahedi, M.J.; Behrouz, V.; Azimi, M. Low fermentable oligo-di-mono-saccharides and poliols diet versus general dietary 712 advice in patients with diarrhea-predominant irritable bowel syndrome: A randomized controlled trial. J. Gastroenterol. Hepatol. 2018, 33, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Goyal, O.; Batta, S.; Nohira, S.; Kishore, H.; Goyal, P.; Sehgal, R.; Sood, A. Low fermentable oligosaccharide, disaccharide, monosaccharide, and polyol diet in patients with diarrhoea–predominant irritable bowel syndrome: A prospective, randomized trial. J. Gastroenterol. Hepatol. 2021, 36, 2107–2115. [Google Scholar] [CrossRef] [PubMed]
- Vakil, N. Diatary Fermentable Oligosacchrides, Disaccharides, Monosaccharides, and Polyols(FODMAPs) and Gastrointestinal Diseases. Nutr. Clin. Pract. 2018, 33, 468–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, H.; Li, Y.T.; Li, Y.T.; Heitkemper, M.M.; Zia, J. Effects of Low-FODMAPS diet on irritable bowel syndrome symptoms and gut microbiome. Gastroenterol. Nurses 2019, 42, 150–158. [Google Scholar] [CrossRef]
- Altomare, A.; Di Rosa, C.; Imperia, E.; Emerenziani, S.; Cicala, M.; Guarino, P.L. Diarrhoea predominant-Irritable bowel syndrome(IBS-D): Effects of different nutritional patterns on intestinal dysbiosis and symptoms. Nutrients 2021, 13, 1506. [Google Scholar] [CrossRef]
- Goyal, O.; Batta, S.; Nohira, S.; Kishore, H.; Goyal, P.; Sehgal, R.; Sood, A. Low fermentable oligosaccharide, disaccharide, monosaccharide, and polyol diet versus traditional dietary advice for functional dyspepsia: A randomized controlled trial. J. Gastroenterol. Hepatol. 2022, 37, 301–309. [Google Scholar] [CrossRef]
- Gross, M.; Gros, B.; Mesonero, J.E.; Latorre, E. Naurotransmitter Dysfunction I Irritable Bowel Syndrome: Emerging Approaches for Manegement. J. Clin. Med. 2021, 10, 3429. [Google Scholar] [CrossRef]
- Chojnacki, C.; Błońska, A.; Kaczka, A.; Chojnacki, J.; Stępień, A.; Gąsiorowska, A. Evaluation of serotonin and dopamine secretion and metabolism in patients with irritable bowel syndrome. Pol. Arch. Int. Med. 2018, 128, 711–713. [Google Scholar] [CrossRef]
- Beacroft, C.O.; Perret, D.; Farthing, M.J. Postprandial plasma 5-hudroxytryptamine in diarrhea predominant syndrome. Gut 1998, 42, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, L.A.; Atkinson, W.; Lockhart, C.; Whorwell, J.P.; Keevil, B. Sigmoid-colon motility in healthy and irritable bowel syndrome: A role for 5-hydroxytryptamine. Neurogastroenterol. Motil. 2007, 19, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, W.; Lockhart, S.; Whorwell, P.J.; Houghton, L.A. Altered 5-hydroxytryptamine signaling in patients with constipation and diarrhea irritable bowel syndrome. Gastroenterology 2006, 130, 34–43. [Google Scholar] [CrossRef]
- Spiller, R. Recent advances in understanding the role of serotonin in gastrointestinal motility in functional bowel disorders: Alteration in 5-HT signaling and metabolism in human diseases. Neurogastroenterol. Motil. 2007, 19 (Suppl. S2), 23–25. [Google Scholar] [CrossRef]
- You, F.Y.; Huang, S.G.; Zhang, H.Y.; Ye, H.; Chi, H.G.; Zou, Y.; Lv, R.X.; Zheng, X.B. Comparison of 5-hydroxytryptamine signaling pathway charaxteristics in diarrhea-predominant irritable bowel syndrome and ulcerative colitis. World J. Gastroenterol. 2016, 22, 3451–3459. [Google Scholar] [CrossRef] [PubMed]
- Christmas, D.M.; Badawy, A.A.; Hince, D.; Davies, S.J.; Probert, C.; Creed, T.; Smithson, J.; Afzal, M.; Nutt, D.J.; Potokar, J.P. Increased serum free tryptophan in patients with diarrhea-predominant irritable bowel syndrome. Nutr. Res. 2010, 30, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, S.Y.; Chun, Y.S.; Chun, Y.J.; Shin, S.Y.; Choi, C.H.; Choi, H.K. Characteristics of fecal metabolic profiles in patients with irritable bowel syndrome with predominant diarrhea investigated using 1 H-NMR coupled with multivariate statistical analysis. Neurogastroenterol. Motil. 2020, 32, e13830. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Agarval, S.; Fulgoni, V.L. Tryptophan Intake in the US Adult Population is not Related to Liver or Kidney Function but is Associated with Depression and Sleep Outcomes. J. Nutr. 2016, 146, 26095–26155. [Google Scholar] [CrossRef]
- Hiratsuka, C.; Fukuwatari, T.; Sano, M.; Saito, S.; Shibata, K. Supplementing Healthy Women with up to 5.o g/d of L-Tryptophan has no Adverse Effects. J. Nutr. 2013, 143, 859–866. [Google Scholar] [CrossRef] [Green Version]
- Booij, L.; Van der Does, A.; Hoffmans, P.M.J.; Riedel, W.J.; Fekkes, D.; Blom, M.J.B. The effects of high-dose and low-dose tryptophan depletion on mood and cognitive functions of remitted depressed patients. Psychopharmacology 2005, 19, 267–275. [Google Scholar] [CrossRef]
- Reuter, M.; Zamoscik, V.; Plieger, T.; Ugertemendia, L.; Rodriguez, A.B.; Kirsch, P. Tryptophan-rich diet is negatively associated with depression and positively linked to social cognition. Nutr. Res. 2021, 85, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Fermstrom, J.D. Effects and side effects associated with the non-nutritional use of tryptophan bay humans. J. Nutr. 2012, 142, 2236–2244. [Google Scholar] [CrossRef] [Green Version]
- Young, S.N. Acute tryptophan depletion in humans: A review of thereotical, practical and ethical aspects. J. Psych. Neurosci. 2013, 38, 294–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shopman, S.M.E.; Bosman, R.C.; Muntinght, A.D.T.; van Balkom, A.J.L.M.; Batelaan, N.M. Effects of tryptophan depletion on anxiety, a systemic review. Transl. Psych. 2021, 11, 118. [Google Scholar] [CrossRef] [PubMed]
- Shufflebotham, J.; Hood, S.; Hendry, J.; Hince, D.A.; Morris, K.; Nutt, D.; Probert, C.; Potokar, J. Acute tryptophan depletion alters gastrointestinal and anxiety symptoms in irritable bowel syndrome. Am. J. Gastroenterol. 2006, 101, 2582–2587. [Google Scholar] [CrossRef]
- Ljotsson, B.; Jones, M.; Talley, N.J.; Kjellström, L.; Agreus, L.; Andreasson, A. Discriminant and convergent validity of GSRS-IBS symptom severity measure for irritable bowel syndrome: A population study. Eur. Gastroenterol. J. 2020, 8, 284–292. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Feature 1 | Controls-Mean (SD) | Patients-Mean (SD) | p-Value |
|---|---|---|---|
| Age (years) | 44.2 (7.6) | 45.9 (9.3) | p > 0.05 |
| Gender (M/F) | 17/23 (42.5/57.5%) | 14/26 (35.0/65.0%) | p > 0.05 |
| BMI (kg/m2) | 23.9 (1.8) | 22.6 (2.1) | p > 0.05 |
| CRP (mg/L) | 1.48 (0.3) | 6.5 (2.9) | p = 0.038 |
| FC (µg/g) | 24.3 (6.2) | 45.4 (19.5) | p = 0.048 |
| AST (U/L) | 16.1 (3.2) | 17.3 (9.5) | p > 0.05 |
| ALT (U/L) | 17.3 (4.8) | 22.1 (7.9) | p > 0.05 |
| Amylase (U/L) | 36.8 (13.1) | 43.2 (21.9) | p > 0.05 |
| Lipase (U/L) | 73.4 (21.3) | 48.3 (16.6) | p > 0.05 |
| Creatinine (mg/dL) | 0.74 (0.2) | 0.88 (0.2) | p > 0.05 |
| GFR (mL/min) | 96.5 (10.7) | 89.5 (11.1) | p > 0.05 |
| TRP (mg daily) | 1269 (191) | 1324 (223) | p > 0.05 |
| TRP (mg/kg) | 21.8 (3.8) | 23.2 (4.1) | p > 0.05 |
| HAM-A | 7.85 (1.2) | 21.3 (4.7) | p = 0.00002 |
| HAM-D | 8.56 (2.6) | 14.4 (2.01) | p = 0.004 |
| ISI | 14.5 (1.6) | 9.12 (3) | p = 0.00003 |
| Compound | Controls-Mean (SD) | IBS-D-Mean (SD) | p-Value |
|---|---|---|---|
| SER (ng/mL) | 142.3 (36.4) | 198.2 (38.1) | p = 0.0009 |
| MEL (pg/mL) | 9.4 (2.4) | 8.6 (1.2) | p > 0.05 |
| 5-HIAA (mg/24 h) | 6.0 (1.7) | 7.7 (1.5) | p = 0.0004 |
| aMT6s (µg/24 h) | 11.2 (4.3) | 10.6 (2.4) | p > 0.05 |
| A Pair of Variable | Spearmans’rho | p-Value |
|---|---|---|
| GSRS and SER | 0.3567 | 0.0241 |
| GSRS and MEL | −0.1605 | 0.4012 |
| GSRS and 5-HIAA | 0.4216 | 0.0105 |
| GSRS and aMT6s | −0.2083 | 0.2718 |
| Feature | Before-Mean (SD) | After-Mean (SD) | p-Value |
|---|---|---|---|
| SER (ng/mL) | 198.2 (38.1) | 123.2 (24.6) | p = 0.00002 |
| MEL (pg/mL) | 8.6 (1.2) | 7.8 (1.9) | p > 0.05 |
| 5-HIAA (mg/24 h) | 7.7 (1.5) | 5.5 (0.8) | p = 0.00007 |
| aMT6s (µg/24 h) | 10.6 (2.4) | 10.5 (1.9) | p > 0.05 |
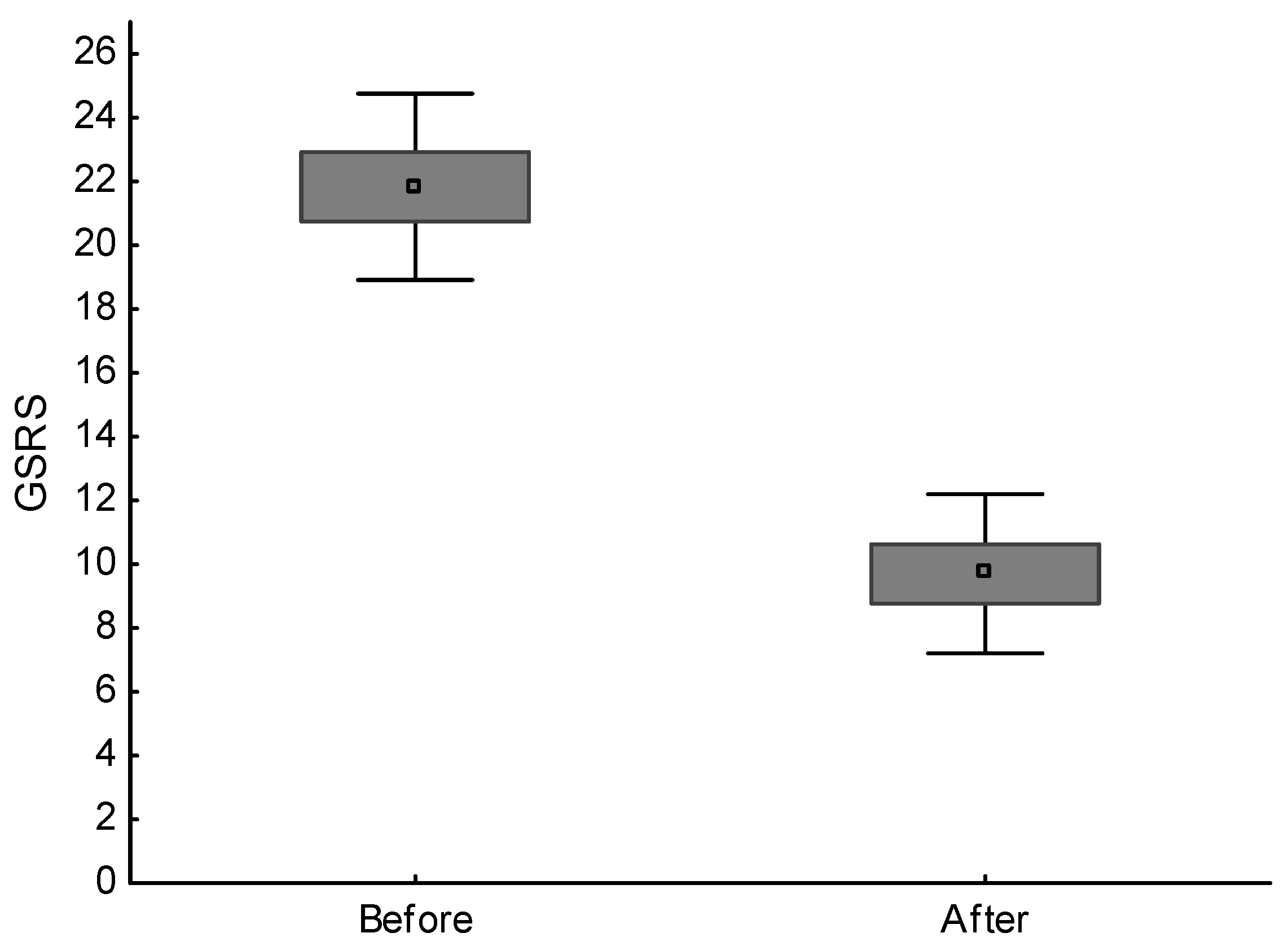
| GSRS (points) | 21.8 (2.9) | 9.7 (2.5) | p = 0.00002 |
| HAM-A (points) | 19.3 (4.7) | 14.9 (3.4) | p = 0.00002 |
| HAM-D (points) | 14.4 (2.1) | 12.9 (3.2) | p > 0.05 |
| ISI (points) | 14.5 (1.6) | 13.8 (1.5) | p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chojnacki, C.; Medrek-Socha, M.; Blonska, A.; Zajdel, R.; Chojnacki, J.; Poplawski, T. A Reduced Tryptophan Diet in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome Improves Their Abdominal Symptoms and Their Quality of Life through Reduction of Serotonin Levels and Its Urinary Metabolites. Int. J. Mol. Sci. 2022, 23, 15314. https://doi.org/10.3390/ijms232315314
Chojnacki C, Medrek-Socha M, Blonska A, Zajdel R, Chojnacki J, Poplawski T. A Reduced Tryptophan Diet in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome Improves Their Abdominal Symptoms and Their Quality of Life through Reduction of Serotonin Levels and Its Urinary Metabolites. International Journal of Molecular Sciences. 2022; 23(23):15314. https://doi.org/10.3390/ijms232315314
Chicago/Turabian StyleChojnacki, Cezary, Marta Medrek-Socha, Aleksandra Blonska, Radoslaw Zajdel, Jan Chojnacki, and Tomasz Poplawski. 2022. "A Reduced Tryptophan Diet in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome Improves Their Abdominal Symptoms and Their Quality of Life through Reduction of Serotonin Levels and Its Urinary Metabolites" International Journal of Molecular Sciences 23, no. 23: 15314. https://doi.org/10.3390/ijms232315314