
Characteristics of BRCA2 Mutated Prostate Cancer at Presentation
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of BRCA2 Mutated Prostate Cancers
2.2. Pathologic Characteristics of BRCA2 Mutated Prostate Cancers
2.3. PSA at Presentation by Initial Stage and by BRCA2 Mutation
2.4. Genomic Characteristics of BRCA2 Mutated Prostate Cancers
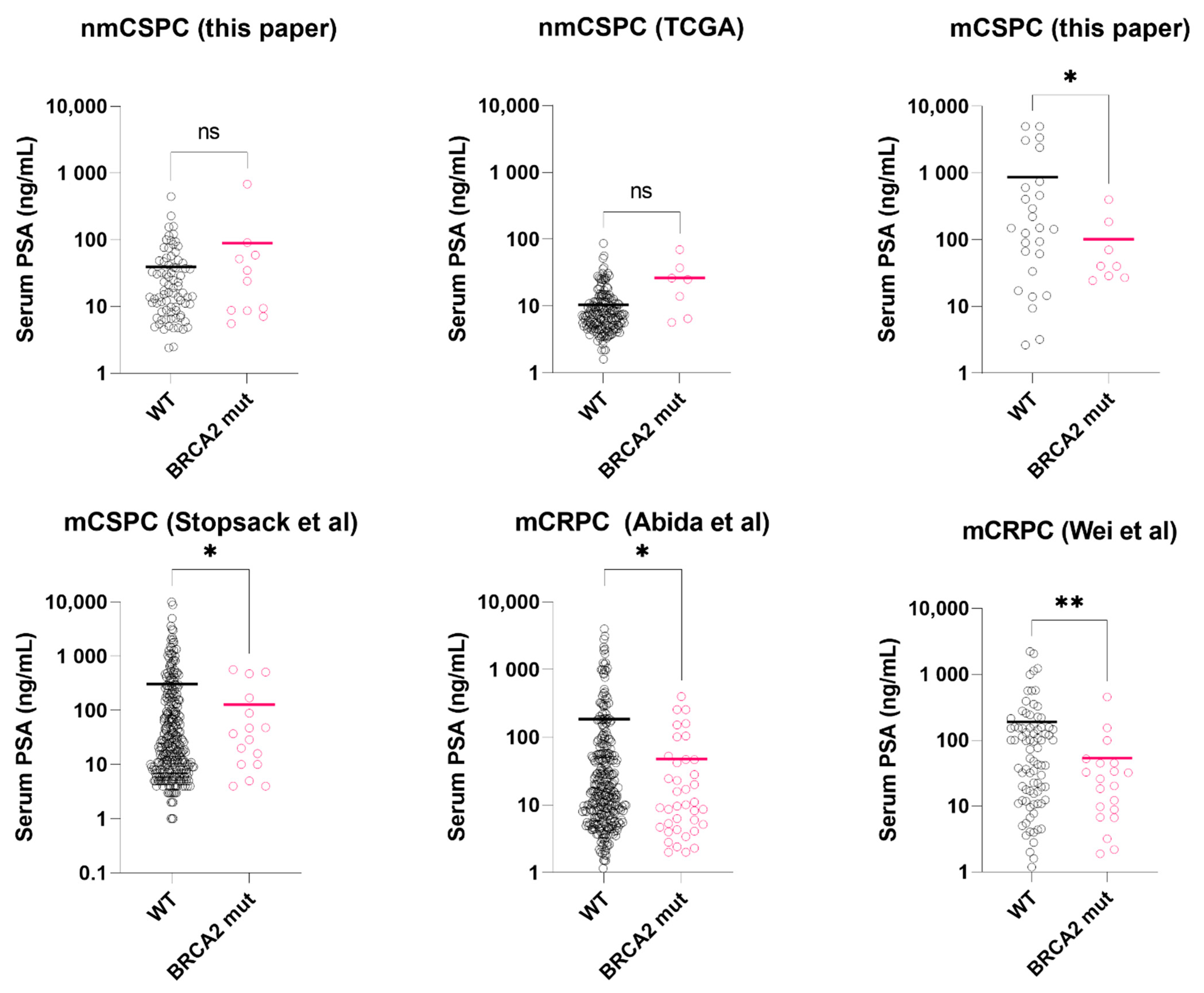
2.5. Serum PSA Level Validation in Public Datasets
2.5.1. Localized BRCA2 Mutated Prostate Cancer
2.5.2. Metastatic Castration-Sensitive BRCA2 Mutated Prostate Cancer
2.5.3. Metastatic Castration-Resistant BRCA2 Mutated Prostate Cancer
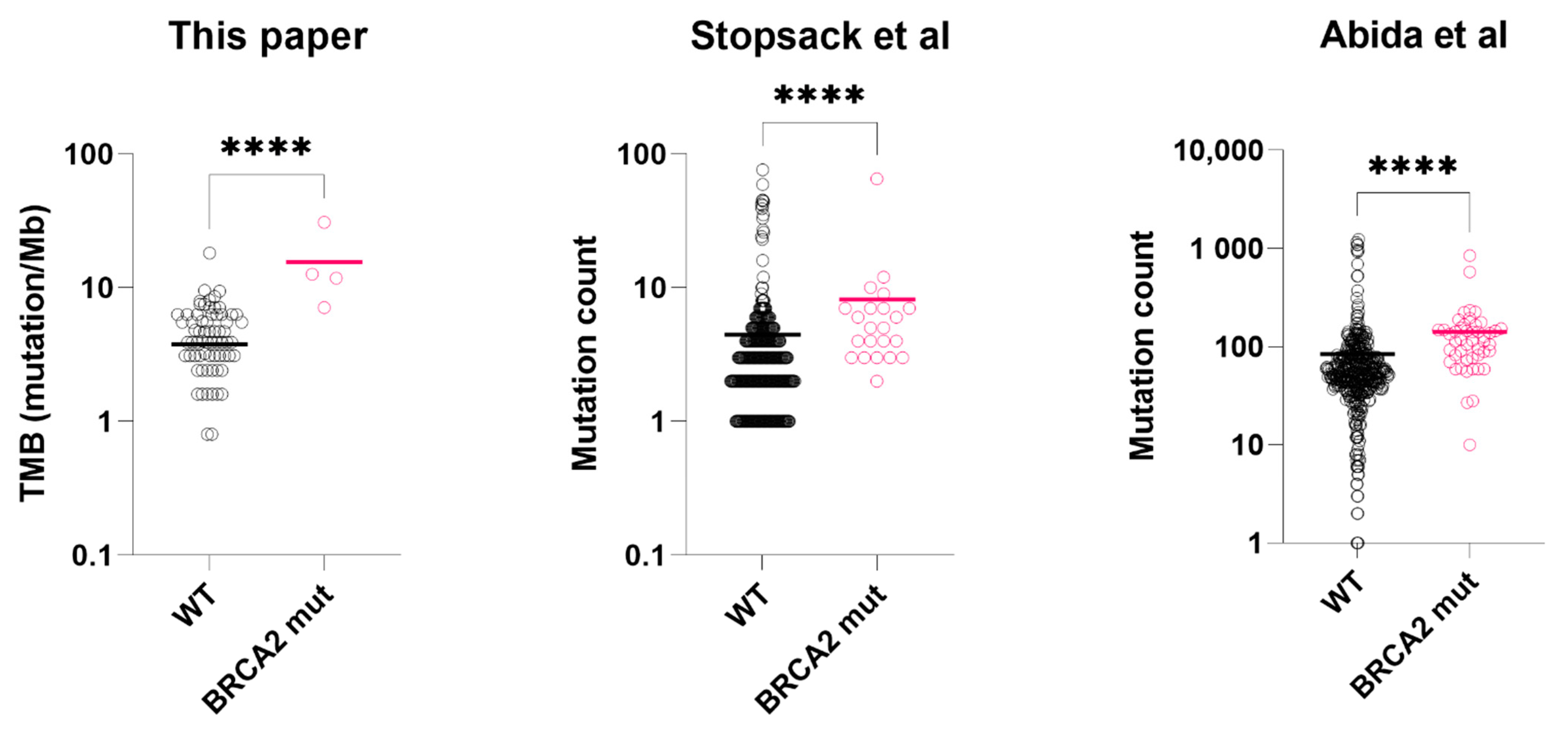
2.6. Genomic Characteristics Validation in Public Dataset
3. Discussion
4. Materials and Methods
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M.; et al. Germline brca mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J. Clin. Oncol. 2013, 31, 1748–1757. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, D.J.; Gaudet, M.M.; Pal, P.; Kirchhoff, T.; Balistreri, L.; Vora, K.; Bhatia, J.; Stadler, Z.; Fine, S.W.; Reuter, V.; et al. Germline brca mutations denote a clinicopathologic subset of prostate cancer. Clin. Cancer Res. 2010, 16, 2115–2121. [Google Scholar] [CrossRef] [Green Version]
- Na, R.; Zheng, S.L.; Han, M.; Yu, H.J.; Jiang, D.K.; Shah, S.; Ewing, C.M.; Zhang, L.T.; Novakovic, K.; Petkewicz, J.; et al. Germline mutations in atm and brca1/2 distinguish risk for lethal and indolent prostate cancer and are associated with early age at death. Eur. Urol. 2017, 71, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Castro, E.; Romero-Laorden, N.; del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. Prorepair-b: A prospective cohort study of the impact of germline DNA repair mutations on the outcomes of patients with metastatic castration-resistant prostate cancer. J. Oflinical Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef]
- Wei, Y.; Wu, J.; Gu, W.; Wang, J.; Lin, G.; Qin, X.; Dai, B.; Gan, H.; Ye, D.; Zhu, Y. Prognostic value of germline DNA repair gene mutations in de novo metastatic and castration-sensitive prostate cancer. Oncologist 2020, 25, e1042–e1050. [Google Scholar] [CrossRef] [Green Version]
- Page, E.C.; Bancroft, E.K.; Brook, M.N.; Assel, M.; Hassan Al Battat, M.; Thomas, S.; Taylor, N.; Chamberlain, A.; Pope, J.; Raghallaigh, H.N.; et al. Interim results from the impact study: Evidence for prostate-specific antigen screening in brca2 mutation carriers. Eur. Urol. 2019, 76, 831–842. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Fei, X.; Zhu, Y.; Pan, J.; Sha, J.; Chi, C.; Gong, Y.; Du, X.; Zhou, L.; Dong, B.; et al. Comparative analysis of genomic alterations across castration sensitive and castration resistant prostate cancer via circulating tumor DNA sequencing. J. Urol. 2021, 205, 461–469. [Google Scholar] [CrossRef]
- Beltran, H.; Yelensky, R.; Frampton, G.M.; Park, K.; Downing, S.R.; MacDonald, T.Y.; Jarosz, M.; Lipson, D.; Tagawa, S.T.; Nanus, D.M.; et al. Targeted next-generation sequencing of advanced prostate cancer identifies potential therapeutic targets and disease heterogeneity. Eur. Urol. 2013, 63, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Nientiedt, C.; Heller, M.; Endris, V.; Volckmar, A.L.; Zschabitz, S.; Tapia-Laliena, M.A.; Duensing, A.; Jager, D.; Schirmacher, P.; Sultmann, H.; et al. Mutations in brca2 and taxane resistance in prostate cancer. Sci. Rep. 2017, 7, 4574. [Google Scholar] [CrossRef]
- Annala, M.; Vandekerkhove, G.; Khalaf, D.; Taavitsainen, S.; Beja, K.; Warner, E.W.; Sunderland, K.; Kollmannsberger, C.; Eigl, B.J.; Finch, D.; et al. Circulating tumor DNA genomics correlate with resistance to abiraterone and enzalutamide in prostate cancer. Cancer Discov. 2018, 8, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Abida, W.; Patnaik, A.; Campbell, D.; Shapiro, J.; Bryce, A.H.; McDermott, R.; Sautois, B.; Vogelzang, N.J.; Bambury, R.M.; Voog, E.; et al. Rucaparib in men with metastatic castration-resistant prostate cancer harboring a brca1 or brca2 gene alteration. J. Clin. Oncol. 2020, 38, 3763–3772. [Google Scholar] [CrossRef]
- Stopsack, K.H. Efficacy of parp inhibition in metastatic castration-resistant prostate cancer is very different with non-brca DNA repair alterations: Reconstructing prespecified endpoints for cohort b from the phase 3 profound trial of olaparib. Eur. Urol. 2021, 79, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Mahal, B.A.; Yang, D.D.; Wang, N.Q.; Alshalalfa, M.; Davicioni, E.; Choeurng, V.; Schaeffer, E.M.; Ross, A.E.; Spratt, D.E.; Den, R.B.; et al. Clinical and genomic characterization of low-prostate-specific antigen, high-grade prostate cancer. Eur. Urol. 2018, 74, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Beltran, H.; Tomlins, S.; Aparicio, A.; Arora, V.; Rickman, D.; Ayala, G.; Huang, J.; True, L.; Gleave, M.E.; Soule, H.; et al. Aggressive variants of castration-resistant prostate cancer. Clin. Cancer Res. 2014, 20, 2846–2850. [Google Scholar] [CrossRef] [Green Version]
- Morgan, T.M.; Welty, C.J.; Vakar-Lopez, F.; Lin, D.W.; Wright, J.L. Ductal adenocarcinoma of the prostate: Increased mortality risk and decreased psa secretion. J. Urol. 2010, 183, E95–E96. [Google Scholar] [CrossRef] [Green Version]
- Markowski, M.C.; Eisenberger, M.A.; Zahurak, M.; Epstein, J.I.; Paller, C.J. Sarcomatoid carcinoma of the prostate: Retrospective review of a case series from the johns hopkins hospital. Urology 2015, 86, 539–543. [Google Scholar] [CrossRef] [Green Version]
- Risbridger, G.P.; Taylor, R.A.; Clouston, D.; Sliwinski, A.; Thorne, H.; Hunter, S.; Li, J.; Mitchell, G.; Murphy, D.; Frydenberg, M.; et al. Patient-derived xenografts reveal that intraductal carcinoma of the prostate is a prominent pathology in brca2 mutation carriers with prostate cancer and correlates with poor prognosis. Eur. Urol. 2015, 67, 496–503. [Google Scholar] [CrossRef]
- Schweizer, M.T.; Antonarakis, E.S.; Bismar, T.A.; Guedes, L.B.; Cheng, H.H.; Tretiakova, M.S.; Vakar-Lopez, F.; Klemfuss, N.; Konnick, E.Q.; Mostaghel, E.A.; et al. Genomic characterization of prostatic ductal adenocarcinoma identifies a high prevalence of DNA repair gene mutations. JCO Precis. Oncol. 2019, 3, 1–9. [Google Scholar] [CrossRef]
- Lozano, R.; Salles, D.C.; Sandhu, S.; Aragon, I.M.; Thorne, H.; Lopez-Campos, F.; Rubio-Briones, J.; Gutierrez-Pecharroman, A.M.; Maldonado, L.; di Domenico, T.; et al. Association between brca2 alterations and intraductal and cribriform histologies in prostate cancer. Eur. J. Cancer 2021, 147, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Abida, W.; Cyrta, J.; Heller, G.; Prandi, D.; Armenia, J.; Coleman, I.; Cieslik, M.; Benelli, M.; Robinson, D.; Van Allen, E.M.; et al. Genomic correlates of clinical outcome in advanced prostate cancer. Proc. Natl. Acad. Sci. USA 2019, 116, 11428–11436. [Google Scholar] [CrossRef] [Green Version]
- Stopsack, K.H.; Nandakumar, S.; Wibmer, A.G.; Haywood, S.; Weg, E.S.; Barnett, E.S.; Kim, C.J.; Carbone, E.A.; Vasselman, S.E.; Nguyen, B.; et al. Oncogenic genomic alterations, clinical phenotypes, and outcomes in metastatic castration-sensitive prostate cancer. Clin. Cancer Res. 2020, 26, 3230–3238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Lichtenberg, T.; Hoadley, K.A.; Poisson, L.M.; Lazar, A.J.; Cherniack, A.D.; Kovatich, A.J.; Benz, C.C.; Levine, D.A.; Lee, A.V.; et al. An integrated tcga pan-cancer clinical data resource to drive high-quality survival outcome analytics. Cell 2018, 173, 400–416.e11. [Google Scholar] [CrossRef] [Green Version]
- Velho, P.I.; Silberstein, J.L.; Markowski, M.C.; Luo, J.; Lotan, T.L.; Isaacs, W.B.; Antonarakis, E.S. Intraductal/ductal histology and lymphovascular invasion are associated with germline DNA-repair gene mutations in prostate cancer. Prostate 2018, 78, 401–407. [Google Scholar] [CrossRef]
- Bryce, A.H.; Alumkal, J.J.; Armstrong, A.; Higano, C.S.; Iversen, P.; Sternberg, C.N.; Rathkopf, D.; Loriot, Y.; de Bono, J.; Tombal, B.; et al. Radiographic progression with nonrising psa in metastatic castration-resistant prostate cancer: Post hoc analysis of prevail. Prostate Cancer Prostatic Dis. 2017, 20, 221–227. [Google Scholar] [CrossRef]
- Chakraborty, G.; Armenia, J.; Mazzu, Y.Z.; Nandakumar, S.; Stopsack, K.H.; Atiq, M.O.; Komura, K.; Jehane, L.; Hirani, R.; Chadalavada, K.; et al. Significance of brca2 and rb1 co-loss in aggressive prostate cancer progression. Clin. Cancer Res. 2020, 26, 2047–2064. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network. The molecular taxonomy of primary prostate cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef] [Green Version]
- Cooperberg, M.R.; Erho, N.; Chan, J.M.; Feng, F.Y.; Fishbane, N.; Zhao, S.G.; Simko, J.P.; Cowan, J.E.; Lehrer, J.; Alshalalfa, M.; et al. The diverse genomic landscape of clinically low-risk prostate cancer. Eur. Urol. 2018, 74, 444–452. [Google Scholar] [CrossRef]
- Marshall, C.H.; Sokolova, A.O.; McNatty, A.L.; Cheng, H.H.; Eisenberger, M.A.; Bryce, A.H.; Schweizer, M.T.; Antonarakis, E.S. Differential response to olaparib treatment among men with metastatic castration-resistant prostate cancer harboring brca1 or brca2 versus atm mutations. Eur. Urol. 2019, 76, 452–458. [Google Scholar] [CrossRef]
- Karlsson, Q.; Brook, M.N.; Dadaev, T.; Wakerell, S.; Saunders, E.J.; Muir, K.; Neal, D.E.; Giles, G.G.; MacInnis, R.J.; Thibodeau, S.N.; et al. Rare germline variants in atm predispose to prostate cancer: A practical consortium study. Eur. Urol. Oncol. 2021, 4, 570–579. [Google Scholar] [CrossRef]
- Kaur, H.; Salles, D.C.; Murali, S.; Hicks, J.L.; Nguyen, M.; Pritchard, C.C.; De Marzo, A.M.; Lanchbury, J.S.; Trock, B.J.; Isaacs, W.B.; et al. Genomic and clinicopathologic characterization of atm-deficient prostate cancer. Clin. Cancer Res. 2020, 26, 4869–4881. [Google Scholar] [CrossRef] [PubMed]
- Gatei, M.; Scott, S.P.; Filippovitch, I.; Soronika, N.; Lavin, M.F.; Weber, B.; Khanna, K.K. Role for atm in DNA damage-induced phosphorylation of brca1. Cancer Res. 2000, 60, 3299–3304. [Google Scholar] [PubMed]
- Khoronenkova, S.V.; Dianov, G.L. Regulation of usp7/hausp in response to DNA damage: Yet another role for atm. Cell Cycle 2012, 11, 2409–2410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibata, A.; Jeggo, P.A. Atm’s role in the repair of DNA double-strand breaks. Genes 2021, 12, 1370. [Google Scholar] [CrossRef]
- Xiong, H.; Liao, Z.; Liu, Z.; Xu, T.; Wang, Q.; Liu, H.; Komaki, R.; Gomez, D.; Wang, L.E.; Wei, Q. Atm polymorphisms predict severe radiation pneumonitis in patients with non-small cell lung cancer treated with definitive radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1066–1073. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, A.; Suga, T.; Shoji, Y.; Kato, S.; Ohno, T.; Ishikawa, H.; Yoshinaga, S.; Ohara, K.; Ariga, H.; Nomura, K.; et al. Genetic variants of npat-atm and aurka are associated with an early adverse reaction in the gastrointestinal tract of patients with cervical cancer treated with pelvic radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1144–1152. [Google Scholar] [CrossRef]
- Andreassen, C.N.; Rosenstein, B.S.; Kerns, S.L.; Ostrer, H.; De Ruysscher, D.; Cesaretti, J.A.; Barnett, G.C.; Dunning, A.M.; Dorling, L.; West, C.M.L.; et al. Individual patient data meta-analysis shows a significant association between the atm rs1801516 snp and toxicity after radiotherapy in 5456 breast and prostate cancer patients. Radiother. Oncol. 2016, 121, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Lee, H.H.; Choi, K.; Moon, Y.J.; Heo, J.E.; Ham, W.S.; Jang, W.S.; Rha, K.H.; Cho, N.H.; Giancotti, F.G.; et al. Prostate epithelial genes define therapy-relevant prostate cancer molecular subtype. Prostate Cancer 2021, 24, 1080–1092. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and guidelines for the interpretation and reporting of sequence variants in cancer: A joint consensus recommendation of the association for molecular pathology, american society of clinical oncology, and college of american pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the american college of medical genetics and genomics and the association for molecular pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopanos, C.; Tsiolkas, V.; Kouris, A.; Chapple, C.E.; Albarca Aguilera, M.; Meyer, R.; Massouras, A. Varsome: The human genomic variant search engine. Bioinformatics 2019, 35, 1978–1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| BRCA2 Mutated N = 19 | BRCA2 Wild Type N = 107 | p Value | |
|---|---|---|---|
| Age at diagnosis (years) Mean (range) | 64.1 (43–88) | 66.3 (44–86) | 0.432 1 |
| PSA at diagnosis (ng/mL) Mean (range) | 94.7 (5.6–682) | 242.7 (2.4–5000) | 0.101 1 |
| cT stage, N (%) | 0.925 2 | ||
| T2 | 3 (16%) | 16 (15%) | |
| T3/4 | 16 (84%) | 91 (85%) | |
| N1 stage, N (%) | 6 (32%) | 48 (45%) | 0.324 3 |
| M1 stage, N (%) | 8 (42%) | 27 (25%) | 0.165 3 |
| Gleason grade group, N (%) * | 0.140 2 | ||
| 1–4 | 6 (32%) | 51 (50%) | |
| 5 | 13 (68%) | 51 (50%) | |
| Histologic Type, N (%) * | 0.070 3 | ||
| Adenocarcinoma, acinar type | 16 (84%) | 86 (84%) | |
| Adenocarcinoma, ductal type | 1 (5%) | 15 (15%) | |
| Neuroendocrine small cell | 2 (11%) | 1 (1%) | |
| Adenosquamous | 0 (0%) | 1 (1%) |
| BRCA2 Mutated N = 19 | BRCA2 Wild Type N = 107 | p Value | |
|---|---|---|---|
| TMPRSS2-ERG fusion, N (%) | 3(16%) | 27(25%) | 0.560 1 |
| TP53, N (%) | 2(11%) | 22(22%) | 0.522 1 |
| AR, N (%) | 7(37%) | 19(18%) | 0.070 1 |
| MYC, N (%) | 7(37%) | 18(17%) | 0.061 1 |
| CDK12, N (%) | 3(16%) | 16(15%) | >0.999 1 |
| FGFR1, N (%) | 1(5%) | 17(16%) | 0.140 1 |
| ATM | 8(42%) | 11(10%) | 0.002 1 |
| APC | 7(37%) | 9(8%) | 0.003 1 |
| BRCA1 | 4(21%) | 4(4%) | 0.018 1 |
| Source (Disease State) | BRCA2 Mutated | BRCA2 Wild Type |
|---|---|---|
| This paper (nmCSPC) | 11 (12%) | 80 (88%) |
| TCGA (nmCSPC) | 7 (4%) | 180 (96%) |
| This paper (mCSPC) | 8 (23%) | 27 (77%) |
| Stopsack et al. (mCSPC) | 17 (5%) | 303 (95%) |
| Abida et al. (mCRPC) | 56 (15%) | 321 (85%) |
| Wei et al. (mCRPC) | 20 (19%) | 83 (81%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, H.; Park, C.K.; Cho, N.H.; Lee, J.; Jang, W.S.; Ham, W.S.; Choi, Y.D.; Cho, K.S. Characteristics of BRCA2 Mutated Prostate Cancer at Presentation. Int. J. Mol. Sci. 2022, 23, 13426. https://doi.org/10.3390/ijms232113426
Han H, Park CK, Cho NH, Lee J, Jang WS, Ham WS, Choi YD, Cho KS. Characteristics of BRCA2 Mutated Prostate Cancer at Presentation. International Journal of Molecular Sciences. 2022; 23(21):13426. https://doi.org/10.3390/ijms232113426
Chicago/Turabian StyleHan, Hyunho, Cheol Keun Park, Nam Hoon Cho, Jongsoo Lee, Won Sik Jang, Won Sik Ham, Young Deuk Choi, and Kang Su Cho. 2022. "Characteristics of BRCA2 Mutated Prostate Cancer at Presentation" International Journal of Molecular Sciences 23, no. 21: 13426. https://doi.org/10.3390/ijms232113426