
A microRNA Signature for the Diagnosis of Statins Intolerance

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Parameters between SI and NSI Patients
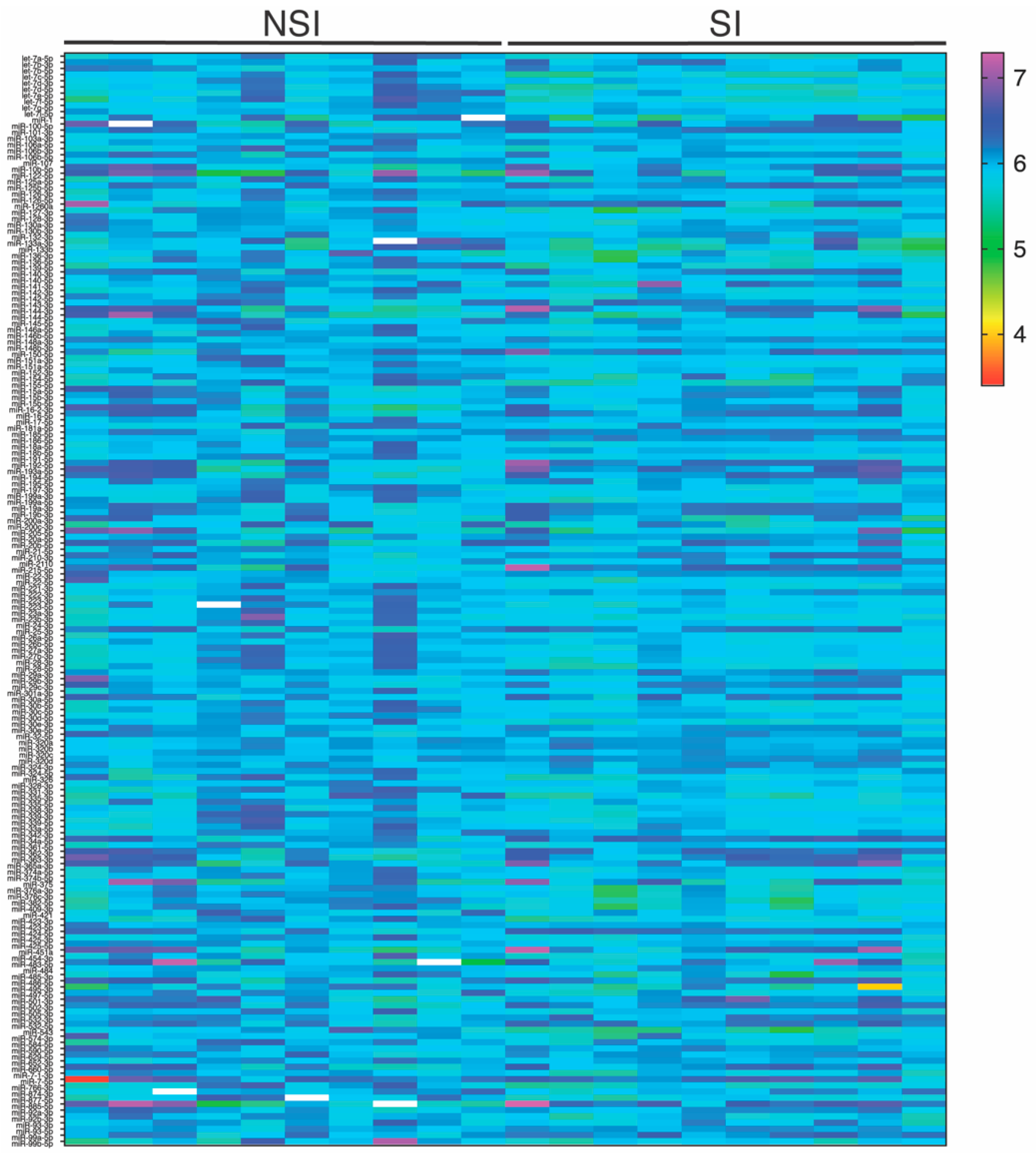
2.2. Plasma miRNA Profile in Patients with SI
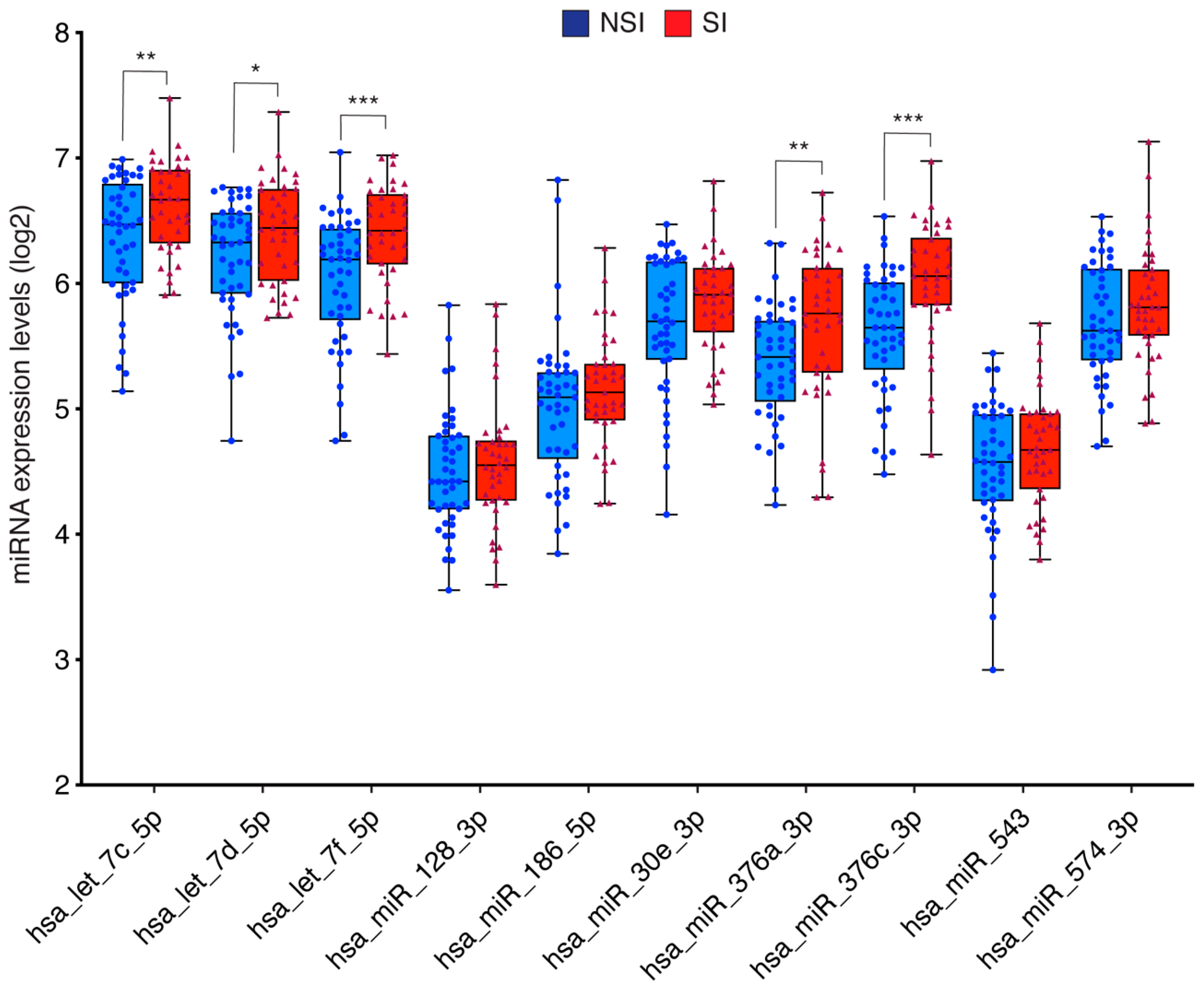
2.3. miRNAs Validation Study and Their Correlation with Clinical Parameters
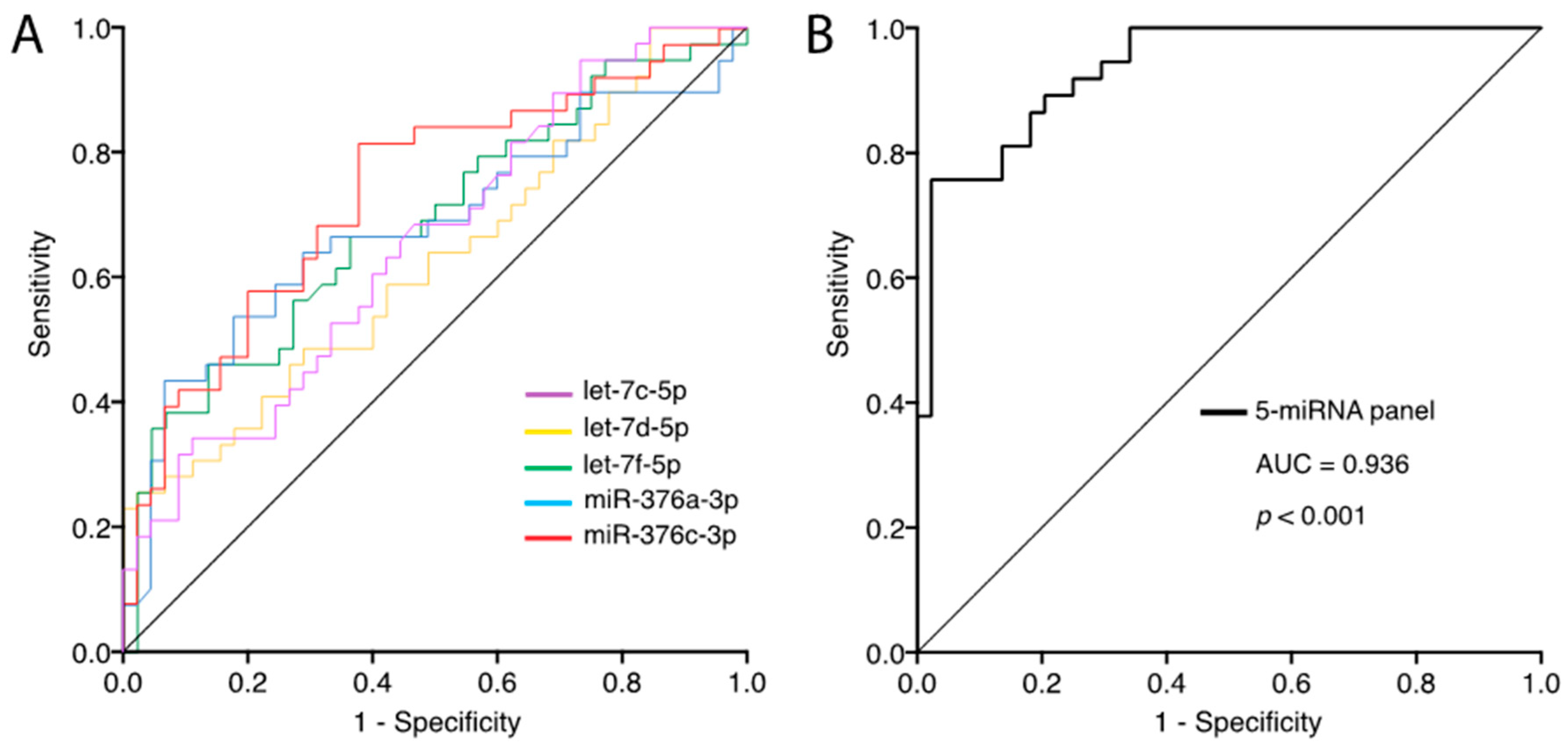
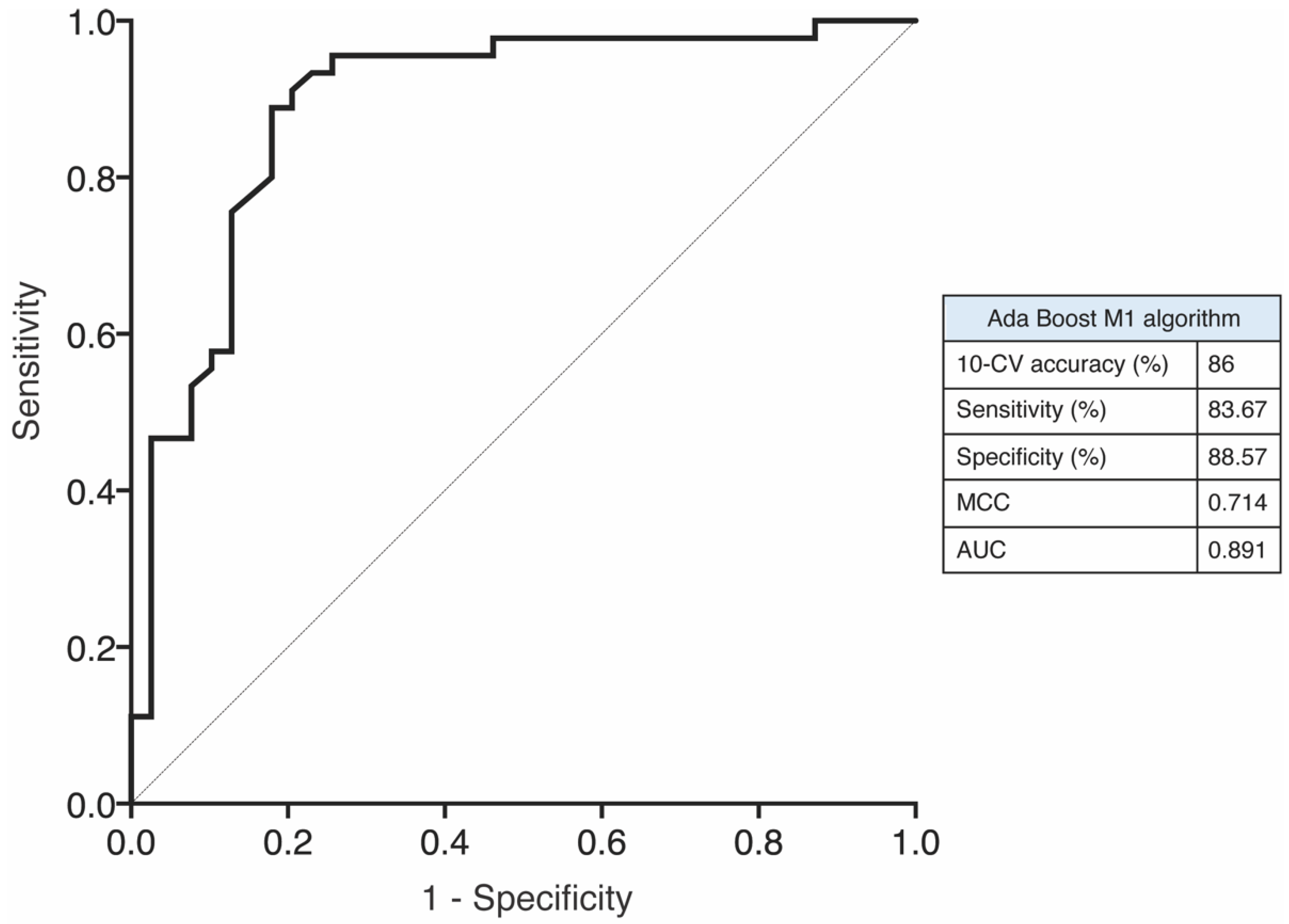
2.4. Circulating miRNA as a Biological Marker of SI
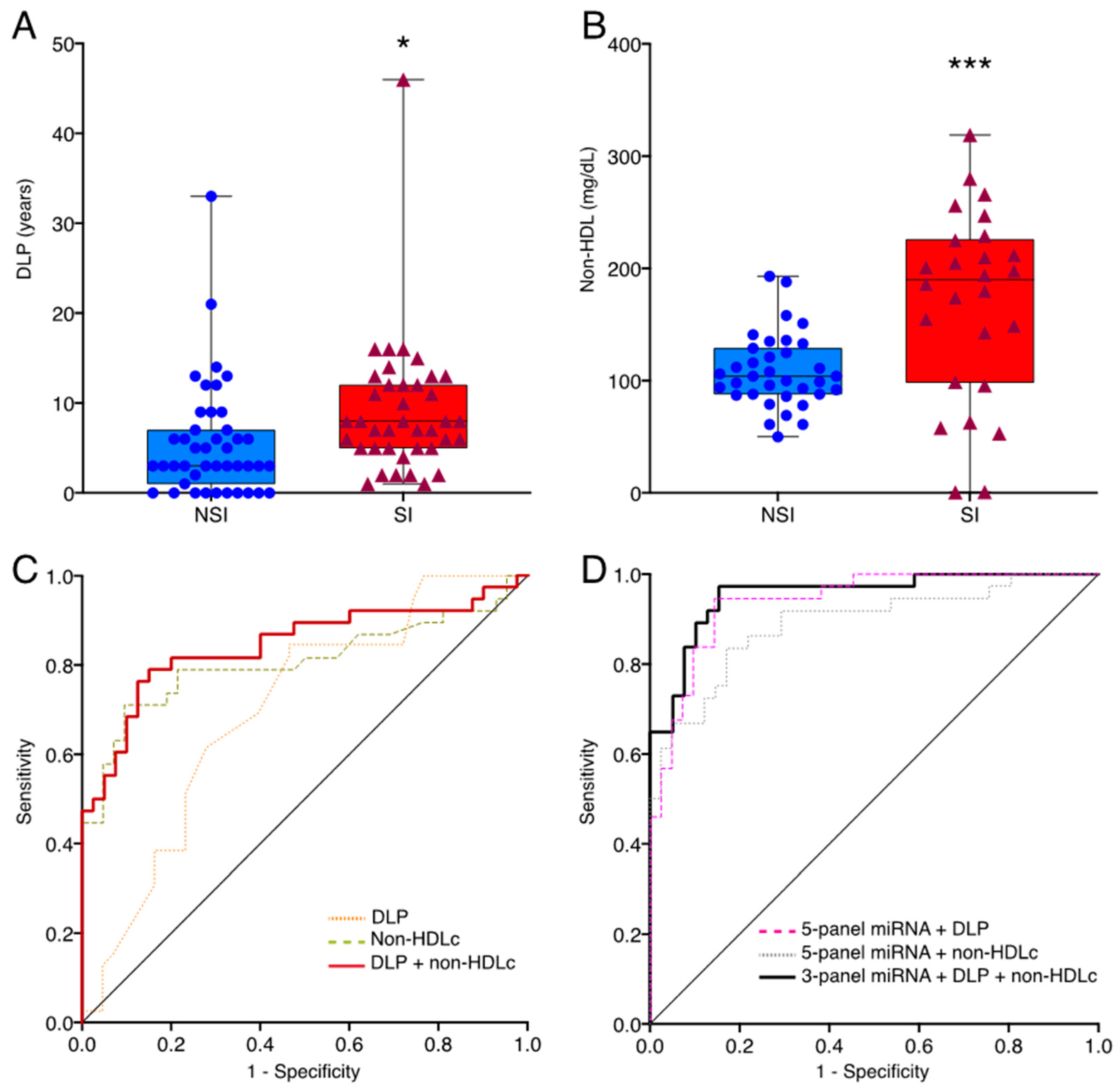
2.5. Combination of miRNAs, Years of Dislipidemia and Non-HDLc to Categorize SI Patients
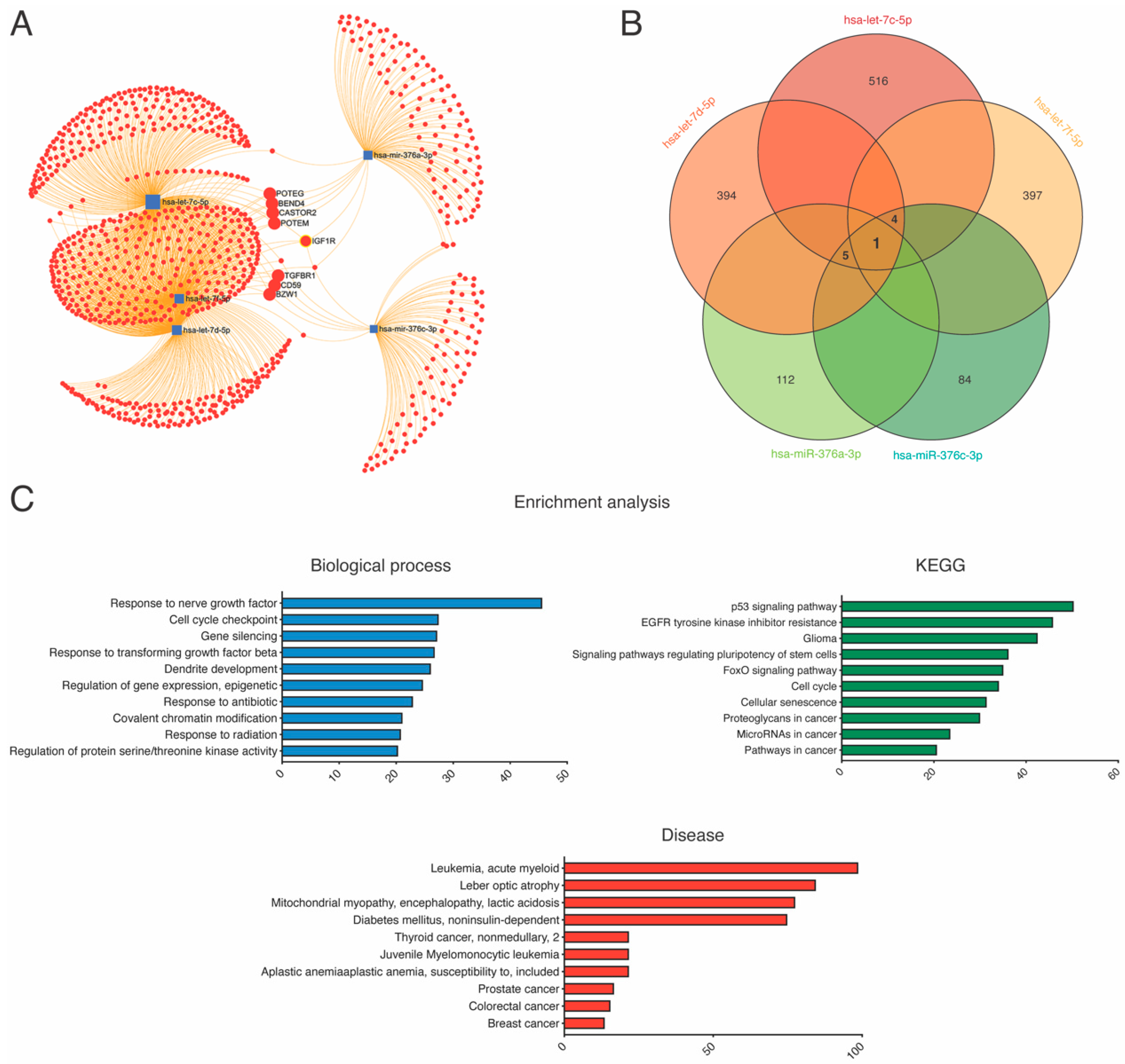
2.6. Kyoto Encyclopedia of Genes and Genomes Pathway and Gene Ontology Enrichment Analysis
3. Discussion
4. Materials and Methods
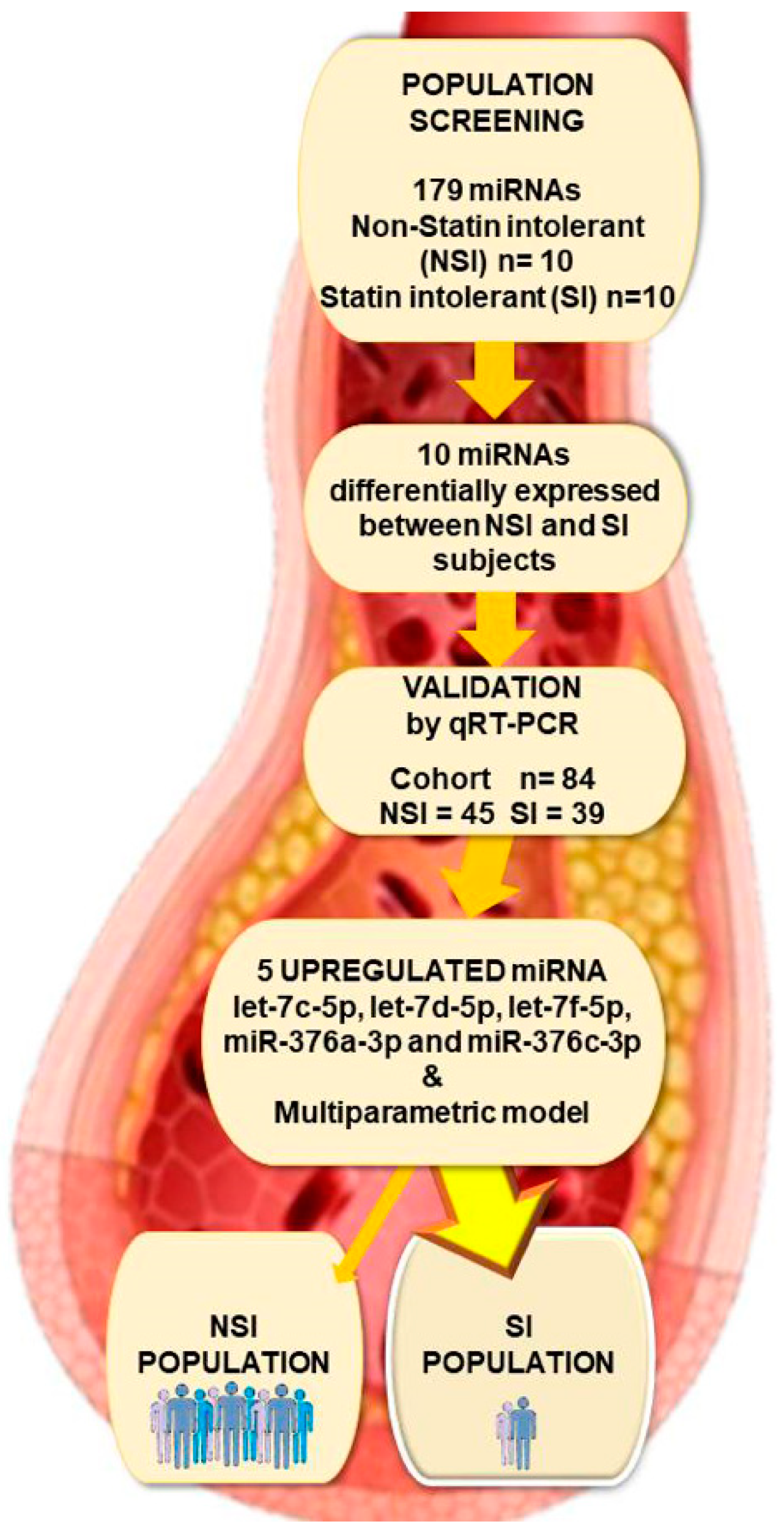
4.1. Study Population and Design
4.2. Blood Collection
4.3. RNA Isolation
4.4. MiRNA Real-Time Reverse Transcriptase-Polymerase Chain Reaction
4.5. Validation of miRNA Profiles
4.6. miRNA-Gene Network Analysis
4.7. KEGG and GO Term Enrichment Analysis
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Approval
Abbreviations
| ACEI | Angiotensin-converting enzyme inhibitors |
| ARB | Angiotensin II receptors blockers |
| ASCVD | Atherosclerotic cardiovascular diseases |
| AUC | Area under the ROC curve |
| CCB | Calcium channel blockers |
| CI | Confidence interval |
| CPK | Creatine kinase |
| CVC | Cardiovascular disease |
| DLP | Years of dyslipidemia |
| ESC | European Society of Cardiology |
| EAS | European Atherosclerosis Society |
| FoxO | Forkhead members of the O class family |
| GO | Gene Ontology |
| HDLc | High-density lipoprotein cholesterol |
| KEGG | Kyoto Encyclopedia of Genes and Genomes |
| LDLc | Plasmatic low-density lipid |
| miRNAs | MicroRNAs |
| Non-HDLc | Non-HDL cholesterol |
| NSI | Non-statin intolerant |
| SAMS | Statin-associated muscle symptoms |
| SD | Standard deviation |
| SI | Statin intolerant |
| STRING | Search Tool for the Retrieval of Interacting Genes |
References
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. ESC Scientific Document Group (2020). 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [Green Version]
- Banach, M.; Stulc, T.; Dent, R.; Toth, P.P. Statin non-adherence and residual cardiovascular risk: There is need for substantial improvement. Int. J. Cardiol. 2016, 225, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S.; Baker, S.K.; Jacobson, T.A.; Kopecky, S.L.; Parker, B.A. The National Lipid Association’s Muscle Safety Expert Panel. An assessment by the Statin Muscle Safety Task Force: 2014 update. J. Clin. Lipidol. 2014, 8, S58–S71. [Google Scholar] [CrossRef] [Green Version]
- Toth, P.P.; Granowitz, C.; Hull, M.; Anderson, A.; Philip, S. Long-term statin persistence is poor among high-risk patients with dyslipidemia: A real-world administrative claims analysis. Lipids Health Dis. 2019, 18, 175. [Google Scholar] [CrossRef] [Green Version]
- Stroes, E.S.; Thompson, P.D.; Corsini, A.; Vladutiu, G.D.; Raal, F.J.; Ray, K.K.; Roden, M.; Stein, E.; Tokgözoğlu, L.; Nordestgaard, B.G.; et al. European Atherosclerosis Society Consensus Panel (2015). Statin-associated muscle symptoms: Impact on statin therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management. Eur. Heart J. 2015, 36, 1012–1022. [Google Scholar] [CrossRef]
- Zhang, H.; Plutzky, J.; Shubina, M.; Turchin, A. Continued Statin Prescriptions after Adverse Reactions and Patient Outcomes: A Cohort Study. Ann. Intern. Med. 2017, 167, 221–227. [Google Scholar] [CrossRef]
- Henning, R.J. Cardiovascular Exosomes and MicroRNAs in Cardiovascular Physiology and Pathophysiology. J. Cardiovasc. Transl. Res. 2021, 14, 195–212. [Google Scholar] [CrossRef]
- Mellis, D.; Caporali, A. MicroRNA-based therapeutics in cardiovascular disease: Screening and delivery to the target. Biochem. Soc. Trans. 2018, 46, 11–21. [Google Scholar] [CrossRef]
- Kalayinia, S.; Arjmand, F.; Maleki, M.; Malakootian, M.; Singh, C.P. MicroRNAs: Roles in cardiovascular development and disease. Cardiovasc. Pathol. 2021, 50, 107296. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.C.; Kurc, S.; Drożdż, A.; Cortez-Dias, N.; Enguita, F.J. The circulating non-coding RNA landscape for biomarker research: Lessons and prospects from cardiovascular diseases. Acta Pharmacol. Sin. 2018, 39, 1085–1099. [Google Scholar] [CrossRef]
- Lu, D.; Thum, T. RNA-based diagnostic and therapeutic strategies for cardiovascular disease. Nat. Rev. Cardiol. 2019, 16, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.K.; Kafert-Kasting, S.; Thum, T. Preclinical and Clinical Development of Noncoding RNA Therapeutics for Cardiovascular Disease. Circ. Res. 2020, 126, 663–678. [Google Scholar] [CrossRef]
- Sodi, R.; Eastwood, J.; Caslake, M.; Packard, C.J.; Denby, L. Relationship between circulating microRNA-30c with total- and LDL-cholesterol, their circulatory transportation and effect of statins. Clin. Chim. Acta. 2017, 466, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Zambrano, T.; Hirata, R.; Hirata, M.H.; Cerda, Á.; Salazar, L.A. Statins differentially modulate microRNAs expression in peripheral cells of hyperlipidemic subjects: A pilot study. Eur. J. Pharm. Sci. 2018, 117, 55–61. [Google Scholar] [CrossRef]
- Stormo, C.; Kringen, M.K.; Lyle, R.; Olstad, O.K.; Sachse, D.; Berg, J.P.; Piehler, A.P. RNA-sequencing analysis of HepG2 cells treated with atorvastatin. PLoS ONE 2014, 9, e105836. [Google Scholar] [CrossRef] [Green Version]
- Cerda, A.; Bortolin, R.H.; Manriquez, V.; Salazar, L.; Zambrano, T.; Fajardo, C.M.; Hirata, M.H.; Hirata, R. Effect of statins on lipid metabolism-related microRNA expression in HepG2 cells. Pharmacol. Rep. 2021, 73, 868–880. [Google Scholar] [CrossRef]
- Lee, S.; Dong, H.H. FoxO integration of insulin signaling with glucose and lipid metabolism. J. Endocrinol. 2017, 233, R67–R79. [Google Scholar] [CrossRef] [Green Version]
- Mallinson, J.E.; Constantin-Teodosiu, D.; Sidaway, J.; Westwood, F.R.; Greenhaff, P.L. Blunted Akt/FOXO signalling and activation of genes controlling atrophy and fuel use in statin myopathy. J. Physiol. 2009, 587, 219–230. [Google Scholar] [CrossRef]
- Naderi, S.H.; Bestwick, J.P.; Wald, D.S. Adherence to drugs that prevent cardiovascular disease: Meta-analysis on 376,162 patients. Am. J. Med. 2012, 125, 882–887.e1. [Google Scholar] [CrossRef] [PubMed]
- Vinci, P.; Panizon, E.; Tosoni, L.M.; Cerrato, C.; Pellicori, F.; Mearelli, F.; Biasinutto, C.; Fiotti, N.; Di Girolamo, F.G.; Biolo, G. Statin-Associated Myopathy: Emphasis on Mechanisms and Targeted Therapy. Int. J. Mol. Sci. 2021, 22, 11687. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.M.; Yin, P.; Hanson, A.; FitzGerald, R.; Morris, A.P.; Stables, R.H.; Jorgensen, A.L.; Pirmohamed, M.J. Investigating the prevalence, predictors, and prognosis of suboptimal statin use early after a non-ST elevation acute coronary syndrome. Clin. Lipidol. 2017, 11, 204–214. [Google Scholar] [CrossRef] [Green Version]
- Alonso, R.; Cuevas, A.; Cafferata, A. Diagnosis and Management of Statin Intolerance. J. Atheroscler. Thromb. 2019, 26, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Parker, B.A.; Capizzi, J.A.; Grimaldi, A.S.; Clarkson, P.M.; Cole, S.M.; Keadle, J.; Chipkin, S.; Pescatello, L.S.; Simpson, K.; White, C.M.; et al. Effect of statins on skeletal muscle function. Circulation 2013, 127, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Colantonio, L.D.; Kent, S.T.; Huang, L.; Chen, L.; Monda, K.L.; Serban, M.C.; Manthripragada, A.; Kilgore, M.L.; Rosenson, R.S.; Muntner, P. Algorithms to identify statin intolerance in Medicare administrative claim data. Cardiovasc. Drugs Ther. 2016, 30, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Mancini, G.B.; Baker, S.; Bergeron, J.; Fitchett, D.; Frohlich, J.; Genest, J.; Gupta, M.; Hegele, R.A.; Ng, D.; Pearson, G.J.; et al. Diagnosis, Prevention, and Management of Statin Adverse Effects and Intolerance: Canadian Consensus Working Group Update. Can. J. Cardiol. 2016, 32, S35–S65. [Google Scholar] [CrossRef] [PubMed]
- Leal, K.; Saavedra, K.; Rebolledo, C.; Salazar, L.A. MicroRNAs hsa-miR-618 and hsa-miR-297 Might Modulate the Pleiotropic Effects Exerted by Statins in Endothelial Cells through the Inhibition of ROCK2 Kinase: In-silico Approach. Front. Cardiovasc. Med. 2021, 8, 704175. [Google Scholar] [CrossRef]
- Raucci, A.; Macrì, F.; Castiglione, S.; Badi, I.; Vinci, M.C.; Zuccolo, E. MicroRNA-34a: The bad guy in age-related vascular diseases. Cell. Mol. Life Sci. 2021, 78, 7355–7378. [Google Scholar] [CrossRef]
- Hirota, T.; Fujita, Y.; Ieiri, I. An updated review of pharmacokinetic drug interactions and pharmacogenetics of statins. Expert Opin. Drug Metab. Toxicol. 2020, 16, 809–822. [Google Scholar] [CrossRef]
- Mohammadzadeh, N.; Montecucco, F.; Carbone, F.; Xu, S.; Al-Rasadi, K.; Sahebkar, A. Statins: Epidrugs with effects on endothelial health? Eur. J. Clin. Investig. 2020, 50, e13388. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.J.; D’Souza, R.F.; Schierding, W.; Zeng, N.; Ramzan, F.; O’Sullivan, J.M.; Poppitt, S.D.; Cameron-Smith, D. Identification of human skeletal muscle miRNA related to strength by high-throughput sequencing. Physiol. Genom. 2018, 50, 416–424. [Google Scholar] [CrossRef]
- Liu, D.; Black, B.L.; Derynck, R. TGF-beta inhibits muscle differentiation through functional repression of myogenic transcription factors by Smad3. Genes. Dev. 2001, 15, 2950–2966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorillo, A.A.; Heier, C.R.; Huang, Y.F.; Tully, C.B.; Punga, T.; Punga, A.R. Estrogen Receptor, Inflammatory, and FOXO Transcription Factors Regulate Expression of Myasthenia Gravis-Associated Circulating microRNAs. Front. Immunol. 2020, 11, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, L.; Xu, Z.; Wang, X.; Liu, F. Integrated bioinformatics analysis identifies microRNA-376a-3p as a new microRNA biomarker in patient with coronary artery disease. Am. J. Transl. Res. 2020, 12, 633–648. [Google Scholar] [PubMed]
- Min, P.K.; Park, J.; Isaacs, S.; Taylor, B.A.; Thompson, P.D.; Troyanos, C.; D’Hemecourt, P.; Dyer, S.; Chan, S.Y.; Baggish, A.L. Influence of statins on distinct circulating microRNAs during prolonged aerobic exercise. J. Appl. Physiol. 2016, 120, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Siracusa, J.; Koulmann, N.; Sourdrille, A.; Chapus, C.; Verret, C.; Bourdon, S.; Goriot, M.E.; Banzet, S. Phenotype-Specific Response of Circulating miRNAs Provides New Biomarkers of Slow or Fast Muscle Damage. Front. Physiol. 2018, 9, 684. [Google Scholar] [CrossRef] [Green Version]
- Fu, C.N.; Song, J.W.; Song, Z.P.; Wang, Q.W.; Bai, W.W.; Guo, T.; Li, P.; Liu, C.; Wang, S.X.; Dong, B. Excessive expression of miR-1a by statin causes skeletal injury through targeting mitogen-activated protein kinase kinase kinase 1. Aging 2021, 13, 11470–11490. [Google Scholar] [CrossRef]
- Bouitbir, J.; Daussin, F.; Charles, A.L.; Rasseneur, L.; Dufour, S.; Richard, R.; Piquard, F.; Geny, B.; Zoll, J. Mitochondria of trained skeletal muscle are protected from deleterious effects of statins. Muscle. Nerve. 2012, 46, 367–373. [Google Scholar] [CrossRef]
- Lotteau, S.; Ivarsson, N.; Yang, Z.; Restagno, D.; Colyer, J.; Hopkins, P.; Weightman, A.; Himori, K.; Yamada, T.; Bruton, J.; et al. A Mechanism for Statin-Induced Susceptibility to Myopathy. JACC Basic Transl. Sci. 2019, 4, 509–523. [Google Scholar] [CrossRef]
- Liu, L.; Cao, P.; Zhang, L.; Qi, M.; Wang, L.; Li, Z.; Shao, G.; Ding, L.; Zhao, X.; Zhao, X.; et al. Comparisons of adipogenesis- and lipid metabolism-related gene expression levels in muscle, adipose tissue and liver from Wagyu-cross and Holstein steers. PLoS ONE 2021, 16, e0247559. [Google Scholar] [CrossRef]
- Bai, W.; Ren, M.; Cheng, W.; Lu, X.; Liu, D.; Wang, B. Qindan Capsule Attenuates Myocardial Hypertrophy and Fibrosis in Pressure Overload-Induced Mice Involving mTOR and TGF-β1/Smad Signaling Pathway Inhibition. Evid. Based Complementary Altern. Med. 2021, 2021, 5577875. [Google Scholar] [CrossRef] [PubMed]
- Oyabu, M.; Takigawa, K.; Mizutani, S.; Hatazawa, Y.; Fujita, M.; Ohira, Y.; Sugimoto, T.; Suzuki, O.; Tsuchiya, K.; Suganami, T.; et al. FOXO1 cooperates with C/EBPδ and ATF4 to regulate skeletal muscle atrophy transcriptional program during fasting. FASEB J. 2022, 36, e22152. [Google Scholar] [CrossRef] [PubMed]
- Hillege, M.; Shi, A.; Galli, R.A.; Wu, G.; Bertolino, P.; Hoogaars, W.; Jaspers, R.T. Lack of Tgfbr1 and Acvr1b synergistically stimulates myofibre hypertrophy and accelerates muscle regeneration. Elife 2022, 11, e77610. [Google Scholar] [CrossRef] [PubMed]
- Burks, T.N.; Cohn, R.D. Role of TGF-beta signalling in inherited and acquired myopathies. Skelet. Muscle 2011, 1, 19. [Google Scholar] [CrossRef] [Green Version]
- Forbes, K.; Shah, V.K.; Siddals, K.; Gibson, J.M.; Aplin, J.; Westwood, M. Statins inhibit insulin-like growth factor action in first trimester placenta by altering insulin-like growth factor 1 receptor glycosylation. Mol. Hum. Reprod. 2015, 21, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Jang, H.J.; Hong, E.M.; Park, S.W.; Byun, H.W.; Koh, D.H.; Choi, M.H.; Kae, S.H.; Lee, J. Statin induces apoptosis of human colon cancer cells and downregulation of insulin-like growth factor 1 receptor via proapoptotic ERK activation. Oncol. Lett. 2016, 12, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Nordstrand, A.; Lundholm, M.; Larsson, A.; Lerner, U.H.; Widmark, A.; Wikström, P. Inhibition of the insulin-like growth factor-1 receptor enhances effects of simvastatin on prostate cancer cells in co-culture with bone. Cancer Microenviron. 2013, 6, 231–240. [Google Scholar] [CrossRef] [Green Version]
- Bonifacio, A.; Sanvee, G.M.; Bouitbir, J.; Krähenbühl, S. The AKT/mTOR signaling pathway plays a key role in statin-induced myotoxicity. Biochim. Biophys. Acta 2015, 1853, 1841–1849. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Chi, M.; Chen, L.; Sun, X.; Wan, L.; Yang, Q.; Guo, C. Linalool Prevents Cisplatin Induced Muscle Atrophy by Regulating IGF-1/Akt/FoxO Pathway. Front. Pharmacol. 2020, 11, 598166. [Google Scholar] [CrossRef]
- Apostolopoulou, M.; Corsini, A.; Roden, M. The role of mitochondria in statin-induced myopathy. Eur. J. Clin. Investig. 2015, 45, 745–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auer, J.; Sinzinger, H.; Franklin, B.; Berent, R. Muscle- and skeletal-related side-effects of statins: Tip of the iceberg? Eur. J. Prev. Cardiol. 2016, 23, 88–110. [Google Scholar] [CrossRef] [PubMed]
- Mollazadeh, H.; Tavana, E.; Fanni, G.; Bo, S.; Banach, M.; Pirro, M.; von Haehling, S.; Jamialahmadi, T.; Sahebkar, A. Effects of statins on mitochondrial pathways. J. Cachexia Sarcopenia Muscle 2021, 12, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, R.; Hovingh, G.K.; Boekholdt, S.M. Non-high-density lipoprotein cholesterol: Current status as cardiovascular marker. Curr. Opin. Lipidol. 2015, 26, 502–510. [Google Scholar] [CrossRef]
- SCORE2 working group and ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- SCORE2-OP working group and ESC Cardiovascular risk collaboration. SCORE2-OP risk prediction algorithms: Estimating incident cardiovascular event risk in older persons in four geographical risk regions. Eur. Heart J. 2021, 42, 2455–2467. [Google Scholar] [CrossRef]
- Ference, B.A.; Majeed, F.; Penumetcha, R.; Flack, J.M.; Brook, R.D. Effect of naturally random allocation to lower low-density lipoprotein cholesterol on the risk of coronary heart disease mediated by polymorphisms in NPC1L1, HMGCR, or both: A 2 × 2 factorial Mendelian randomization study. J. Am. Coll. Cardiol. 2015, 65, 1552–1561. [Google Scholar] [CrossRef] [Green Version]
- Andersen, C.L.; Jensen, J.L.; Ørntoft, T.F. Normalization of real-time quantitative reverse transcription-PCR data: A model-based variance estimation approach to identify genes suited for normalization, applied to bladder and colon cancer data sets. Cancer Res. 2004, 64, 5245–5250. [Google Scholar] [CrossRef] [Green Version]
- Belmonte, T.; Mangas, A.; Calderon-Dominguez, M.; Quezada-Feijoo, M.; Ramos, M.; Campuzano, O.; Gomez, S.; Peña, M.L.; Cubillos-Arango, A.M.; Dominguez, F.; et al. Peripheral microRNA panels to guide the diagnosis of familial cardiomyopathy. Transl. Res. 2020, 218, 1–15. [Google Scholar] [CrossRef]
- Mi, H.; Muruganujan, A.; Ebert, D.; Huang, X.; Thomas, P.D. PANTHER version 14: More genomes, a new PANTHER GO-slim and improvements in enrichment analysis tools. Nucleic Acids Res. 2019, 47, D419–D426. [Google Scholar] [CrossRef]
- Clum, A.; Huntemann, M.; Bushnell, B.; Foster, B.; Foster, B.; Roux, S.; Hajek, P.P.; Varghese, N.; Mukherjee, S.; Reddy, T.; et al. DOE JGI Metagenome Workflow. Msystems 2021, 6, e00804–e00820. [Google Scholar] [CrossRef] [PubMed]
- Szklarczyk, D.; Gable, A.L.; Lyon, D.; Junge, A.; Wyder, S.; Huerta-Cepas, J.; Simonovic, M.; Doncheva, N.T.; Morris, J.H.; Bork, P.; et al. STRING v11: Protein–protein association networks with increased coverage, supporting functional discovery in genome-wide experimental datasets. Nucleic Acids Res. 2019, 47, D607–D613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Y.; Wang, J.; Jaehnig, E.J.; Shi, Z.; Zhang, B. WebGestalt 2019: Gene set analysis toolkit with revamped UIs and APIs. Nucleic Acids Res. 2019, 47, W199–W205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motulsky, H.J.; Brown, R.E. Detecting outliers when fitting data with nonlinear regression—A new method based on robust nonlinear regression and the false discovery rate. BMC Bioinform. 2006, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | NSI | SI | p Value |
|---|---|---|---|
| n | 45 | 39 | |
| Demographics | |||
| Age (years) a | 66.6 ± 11.5 | 63.6 ± 10.9 | NS |
| Sex (female, %) b | 31 | 61.5 | 0.01 |
| DLP (years) c | 5.6 ± 6.3 | 9.1 ± 7.5 | 0.003 |
| High blood pressure (%) b | 73 | 41 | 0.006 |
| Diseases | |||
| Diabetes Mellitus (%) b | 38 | 20.5 | NS |
| ASCVD (%) b | 71 | 13 | <0.001 |
| Chronic kidney disease (%) b | 18 | 12.8 | NS |
| Analytical profile | |||
| Basal blood glucose a | 118.5 ± 36.2 | 110 ± 44.6 | NS |
| Non-HDLc (mg/dL) a | 104.9 ± 32.7 | 169.9 ± 63.5 | <0.001 |
| Triglycerides (mg/dL) a | 151.7 ± 97.4 | 164 ± 93 | NS |
| MDRD-4 (mL/min) a | 76.5 ± 25.6 | 82 ± 31.6 | NS |
| Transaminase GOT (U/L) a | 23.1 ± 13 | 23.5 ± 8 | NS |
| Transaminase GPT (U/L) a | 27.3 ± 23 | 24.6 ± 18.9 | NS |
| CPK (U/L) a | 82.8 ± 40.4 | 165.9 ± 14.7 | NS |
| Medication | |||
| ACEI (%) b | 11 | 2.5 | NS |
| ARB (%) b | 67 | 33.3 | 0.004 |
| OAD (%) b | 33 | 18 | NS |
| Insulin (%) b | 11 | 10.5 | NS |
| Diuretic (%) b | 51 | 18 | 0.003 |
| CCB (%) b | 31 | 18 | NS |
| Beta-blockers (%) b | 62 | 15.4 | <0.001 |
| Alpha-blockers (%) b | 22 | 5 | 0.03 |
| Aspirin (%) b | 64 | 18 | <0.001 |
| Atorvastatin 40 mg (%) | 20 | - | |
| Atorvastatin 80 mg (%) | 15.5 | - | |
| Rosuvastatin 10 mg (%) | 17.7 | - | |
| Rosuvastatin 20 mg (%) | 35.5 | - | |
| Pitavastatin 4mg (%) | 6.6 | - | |
| Simvastatin 40 mg (%) | 4.4 | - | |
| PCSK9 inhibitors: Evolucumab (%) b | 13 | 7.6 | NS |
| PCSK9 inhibitors Alirocumab (%) b | 11 | 2.5 | NS |
| Fenofibrate (%) b | 18 | 7.6 | NS |
| Omega-3 (%) | - | 5.1 | |
| Colesevelam (%) | - | 2.5 | |
| Colestiramine (%) | - | 12.8 | |
| Armolipid plus * (%) | - | 41.0 | |
| Ezetimibe 10 mg * (%) b | 42 | 38 | NS |
| Acenocumarol (%) b | 7 | 7.6 | NS |
| microRNAs | SI Cohort | |||
|---|---|---|---|---|
| DLP (Years) | Non-HDLc (mg/dL) | |||
| Pearson r | p | Pearson r | p | |
| Let-7c-5p | −0.164 | 0.281 | 0.177 | 0.244 |
| Let-7d-5p | −0.079 | 0.603 | 0.226 | 0.131 |
| Let-7f-5p | −0.136 | 0.368 | 0.168 | 0.266 |
| miR-376a-3p | −0.173 | 0.250 | 0.103 | 0.498 |
| miR-376c-3p | −0.265 | 0.079 | 0.176 | 0.248 |
| miRNA | AUC (95% CI) | Sensitivity % | Specificity % | Accuracy % | p Value |
|---|---|---|---|---|---|
| Let-7c-5p | 0.652 (0.535 to 0.770) | 61.70 | 55.56 | 59.04 | 0.017 |
| Let-7d-5p | 0.627 (0.507 to 0.747) | 52.63 | 58.70 | 55.95 | 0.046 |
| Let-7f-5p | 0.688 (0.573 to 0.803) | 60.53 | 64.44 | 62.65 | 0.003 |
| miR-376a-3p | 0.682 (0.563 to 0.800) | 68.89 | 64.10 | 66.67 | 0.004 |
| miR-376c-3p | 0.736 (0.627 to 0.845) | 70.45 | 64.10 | 67.47 | <0.001 |
| 5-miRNA panel | 0.936 (0.887 to 0.985) | 81.25 | 84.85 | 82.72 | <0.001 |
| Multiparametric Model | AUC (95% CI) | Sensitivity % | Specificity % | Accuracy % | p Value |
|---|---|---|---|---|---|
| DLP (years) | 0.700 (0.587 to 0.814) | 57.89 | 60.00 | 58.54 | 0.017 |
| Non-HDLc (mg/dL) | 0.807 (0.703 to 0.911) | 77.08 | 84.38 | 80.00 | <0.001 |
| DLP + non-HDLc | 0.844 (0.751 to 0.937) | 79.55 | 85.29 | 82.05 | <0.001 |
| 5-miRNA panel + DLP | 0.940 (0.892 to 0.989) | 85.71 | 83.78 | 84.81 | <0.001 |
| 5-miRNA panel + non-HDLc | 0.889 (0.814 to 0.964) | 85.00 | 81.08 | 83.12 | <0.001 |
| 3-miRNA panel + DLP + non-HDLc | 0.954 (0.911 to 0.998) | 89.74 | 89.19 | 89.47 | <0.001 |
| Very High CVD Risk | High CVD Risk |
|---|---|
| Presence of ASCVD clinically/imaging. | Total cholesterol over 310 mg/dL, LDLc over 190 mg/dL or blood pressure ≥ 180/110 mmHg. |
| DM patients with target organ damage or at least three major risk factor or early onset of DM type 1 with a length over 20 years. | DM patients without target organ damage. Over 10 years with DM. |
| Severe CKD (eGFR < 30 mL/min/1.73 m2). | Moderate CKD (eGFR = 30–39 mL/min/1.73 m2). |
| A calculated SCORE ≥ 10% for 10 years risk of fatal CVD. | A calculated SCORE ≥ 5% and < 10% for 10 years’ risk of fatal CVD. |
| FH with a ASCVD or with another major risk factor. | FH without any other major risk factor. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangas, A.; Pérez-Serra, A.; Bonet, F.; Muñiz, O.; Fuentes, F.; Gonzalez-Estrada, A.; Campuzano, O.; Rodriguez Roca, J.S.; Alonso-Villa, E.; Toro, R. A microRNA Signature for the Diagnosis of Statins Intolerance. Int. J. Mol. Sci. 2022, 23, 8146. https://doi.org/10.3390/ijms23158146
Mangas A, Pérez-Serra A, Bonet F, Muñiz O, Fuentes F, Gonzalez-Estrada A, Campuzano O, Rodriguez Roca JS, Alonso-Villa E, Toro R. A microRNA Signature for the Diagnosis of Statins Intolerance. International Journal of Molecular Sciences. 2022; 23(15):8146. https://doi.org/10.3390/ijms23158146
Chicago/Turabian StyleMangas, Alipio, Alexandra Pérez-Serra, Fernando Bonet, Ovidio Muñiz, Francisco Fuentes, Aurora Gonzalez-Estrada, Oscar Campuzano, Juan Sebastian Rodriguez Roca, Elena Alonso-Villa, and Rocio Toro. 2022. "A microRNA Signature for the Diagnosis of Statins Intolerance" International Journal of Molecular Sciences 23, no. 15: 8146. https://doi.org/10.3390/ijms23158146