
Detection of Human Papillomavirus in Squamous Lesions of the Conjunctiva Using RNA and DNA In-Situ Hybridization

 ,
,
Abstract
:1. Introduction
2. Results
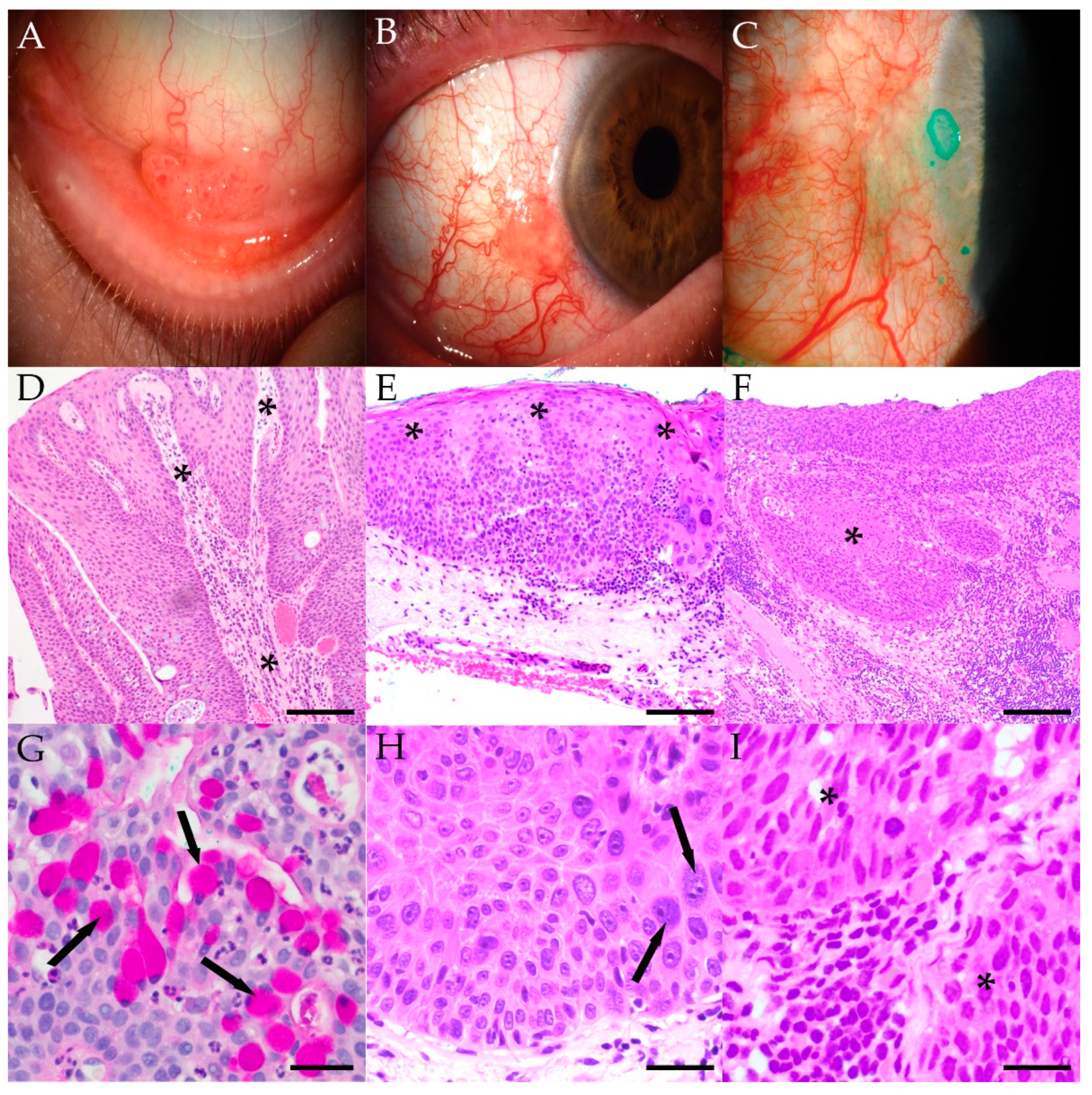
2.1. Clinicopathologic Characteristics
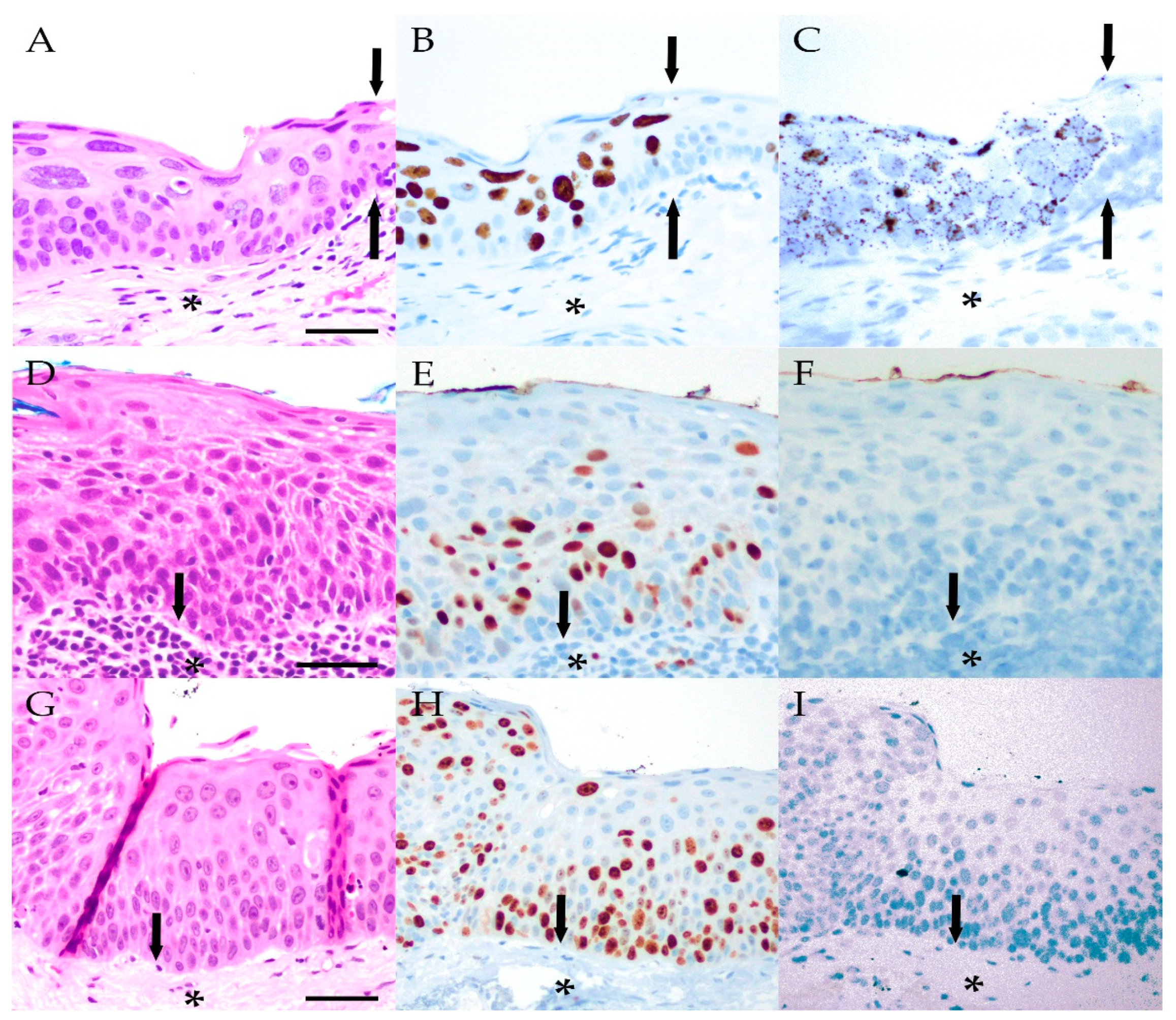
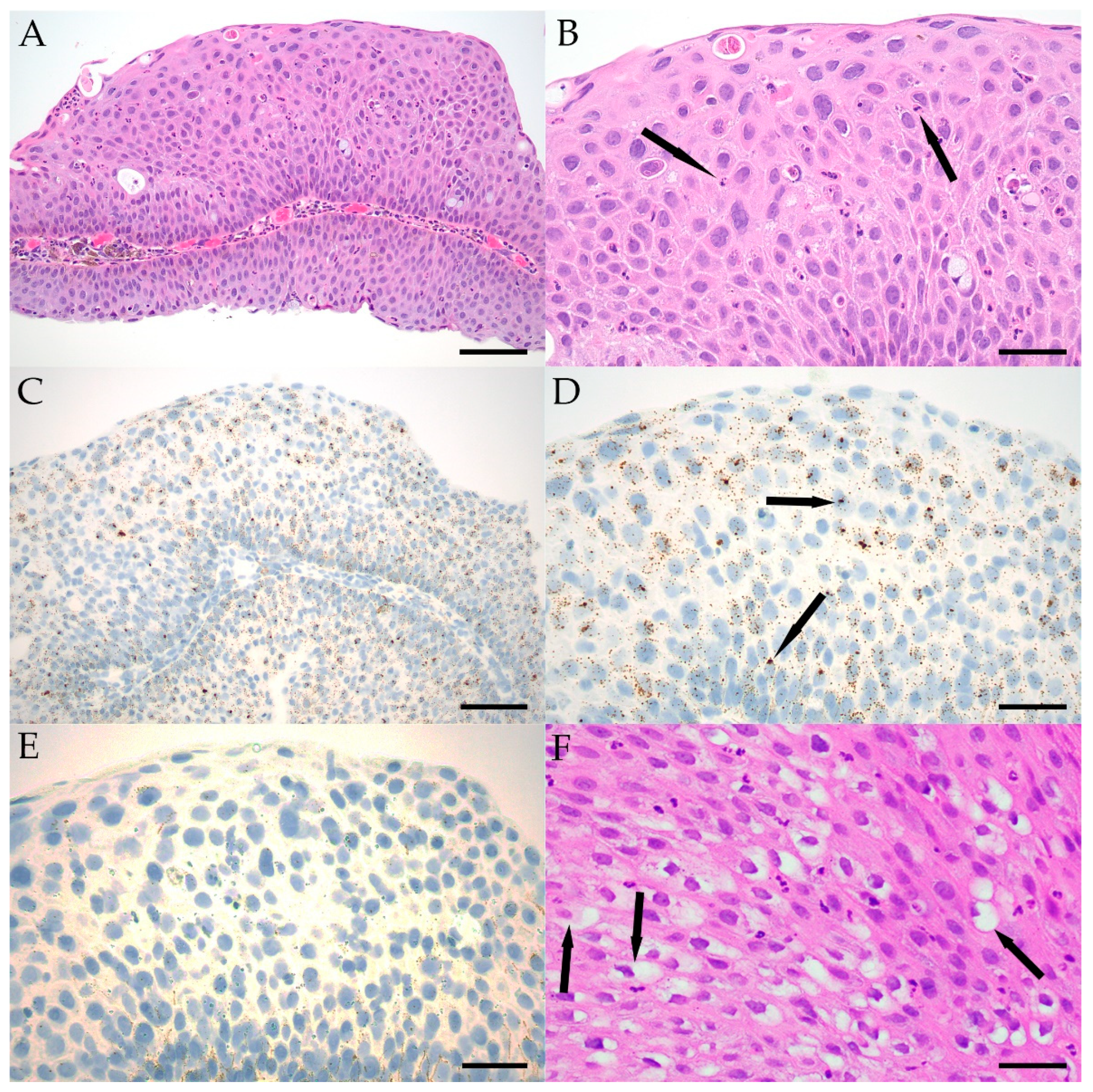
2.2. In-Situ Hybridization
2.3. Correlation of HPV with Histologic Features
2.4. Patient Follow-Up and Atopic History
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. HPV In-Situ Hybridization
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Girolamo, N. Association of Human Papilloma Virus with Pterygia and Ocular-Surface Squamous Neoplasia. Eye 2012, 26, 202–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, V.T.; Merritt, H.A.; Sniegowski, M.; Esmaeli, B. Eyelid and Ocular Surface Carcinoma: Diagnosis and Management. Clin. Dermatol. 2015, 33, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Bellerive, C.; Berry, J.L.; Polski, A.; Singh, A.D. Conjunctival Squamous Neoplasia: Staging and Initial Treatment. Cornea 2018, 37, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Boneva, S.; Schlecht, A.; Zhang, P.; Boehringer, D.; Lapp, T.; Mittelviefhaus, H.; Reinhard, T.; Auw-Haedrich, C.; Schlunck, G.; Wolf, J.; et al. MACE RNA Sequencing Analysis of Conjunctival Squamous Cell Carcinoma and Papilloma Using Formalin-Fixed Paraffin-Embedded Tumor Tissue. Sci. Rep. 2020, 10, 21292. [Google Scholar] [CrossRef]
- Cervantes, G.; Rodríguez, A.A.; Leal, A.G. Squamous Cell Carcinoma of the Conjunctiva: Clinicopathological Features in 287 Cases. Can. J. Ophthalmol. J. Can. Ophtalmol. 2002, 37, 14–19, discussion 19–20. [Google Scholar] [CrossRef]
- Crim, N.; Forniés-Paz, M.E.; Monti, R.; Espósito, E.; Maccio, J.P.; Urrets-Zavalía, J.A. In Situ Carcinoma of the Conjunctiva: Surgical Excision Associated with Cryotherapy. Clin. Ophthalmol. 2013, 7, 1889–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gichuhi, S.; Sagoo, M.S.; Weiss, H.A.; Burton, M.J. Epidemiology of Ocular Surface Squamous Neoplasia in Africa. Trop. Med. Int. Health TMIH 2013, 18, 1424–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basti, S.; Macsai, M.S. Ocular Surface Squamous Neoplasia: A Review. Cornea 2003, 22, 687–704. [Google Scholar] [CrossRef] [PubMed]
- Gichuhi, S.; Ohnuma, S.-I.; Sagoo, M.S.; Burton, M.J. Pathophysiology of Ocular Surface Squamous Neoplasia. Exp. Eye Res. 2014, 129, 172–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez, O.P.; Zein, M.; Galor, A.; Karp, C.L. Management of Ocular Surface Squamous Neoplasia: Bowman Club Lecture 2021. BMJ Open Ophthalmol. 2021, 6, e000842. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Rath, S.; Vemuganti, G.K. Ocular Surface Squamous Neoplasia—Review of Etio-Pathogenesis and an Update on Clinico-Pathological Diagnosis. Saudi J. Ophthalmol. 2013, 27, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Hanbazazh, M.; Gyure, K.A. Ocular Human Papillomavirus Infections. Arch. Pathol. Lab. Med. 2018, 142, 706–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyer, A.B.; Roberts, J.; Olsen, R.J.; Chévez-Barrios, P. Human Papillomavirus—Driven Squamous Lesions: High-Risk Genotype Found in Conjunctival Papillomas, Dysplasia, and Carcinoma. Am. J. Dermatopathol. 2018, 40, 486–490. [Google Scholar] [CrossRef]
- Sjö, N.C.; von Buchwald, C.; Cassonnet, P.; Norrild, B.; Prause, J.U.; Vinding, T.; Heegaard, S. Human Papillomavirus in Normal Conjunctival Tissue and in Conjunctival Papilloma: Types and Frequencies in a Large Series. Br. J. Ophthalmol. 2007, 91, 1014–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, J.; Coroneo, M.T.; Wakefield, D.; Di Girolamo, N. Ultraviolet Radiation and the Role of Matrix Metalloproteinases in the Pathogenesis of Ocular Surface Squamous Neoplasia. Investig. Opthalmol. Vis. Sci. 2008, 49, 5295–5306. [Google Scholar] [CrossRef] [Green Version]
- Ateenyi-Agaba, C.; Dai, M.; Le Calvez, F.; Katongole-Mbidde, E.; Smet, A.; Tommasino, M.; Franceschi, S.; Hainaut, P.; Weiderpass, E. TP53 Mutations in Squamous-Cell Carcinomas of the Conjunctiva: Evidence for UV-Induced Mutagenesis. Mutagenesis 2004, 19, 399–401. [Google Scholar] [CrossRef]
- Yazu, H.; Dogru, M.; Miyauchi, J.; Tanaka, Y.; Yamaguchi, T.; Den, S.; Satake, Y.; Tsubota, K.; Shimazaki, J. Association of Epithelial Atypia with Recurrence after Surgical Excision in Conjunctival Papilloma. Eye Contact Lens 2018, 44 (Suppl. 1), S77–S81. [Google Scholar] [CrossRef]
- Karcioglu, Z.A.; Issa, T.M. Human Papilloma Virus in Neoplastic and Non-Neoplastic Conditions of the External Eye. Br. J. Ophthalmol. 1997, 81, 595–598. [Google Scholar] [CrossRef] [Green Version]
- Bredow, L.; Martin, G.; Reinhard, T.; Mittelviefhaus, H.; Auw-Haedrich, C. Recurrent Conjunctival Papilloma Progressing into Squamous Cell Carcinoma with Change of HPV-Finding During the Course. Br. J. Ophthalmol. 2009, 93, 1437. [Google Scholar] [CrossRef]
- de la Vega, L.L.; Bick, N.; Hu, K.; Rahrig, S.E.; Silva, C.D.; Matayoshi, S.; Picciarelli, P.; Wang, X.; Sugar, A.; Soong, H.K.; et al. Invasive Squamous Cell Carcinomas and Precursor Lesions on UV-Exposed Epithelia Demonstrate Concordant Genomic Complexity in Driver Genes. Mod. Pathol. 2020, 33, 2280–2294. [Google Scholar] [CrossRef]
- Hamam, R.; Bhat, P.; Foster, C.S. Conjunctival/Corneal Intraepithelial Neoplasia. Int. Ophthalmol. Clin. 2009, 49, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Griffin, H.; Mudhar, H.S.; Rundle, P.; Shiraz, A.; Mahmood, R.; Egawa, N.; Quint, W.; Rennie, I.G.; Doorbar, J. Human Papillomavirus Type 16 Causes a Defined Subset of Conjunctival In Situ Squamous Cell Carcinomas. Mod. Pathol. 2020, 33, 74–90. [Google Scholar] [CrossRef]
- Cheng, J.; Zens, M.S.; Duell, E.; Perry, A.E.; Chapman, M.S.; Karagas, M.R. History of Allergy and Atopic Dermatitis in Relation to Squamous Cell and Basal Cell Carcinoma of the Skin. Cancer Epidemiol. Biomark. Prev. 2015, 24, 749–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, A.O.; Svaerke, C.; Körmendiné Farkas, D.; Olesen, A.B.; Kragballe, K.; Sørensen, H.T. Atopic Dermatitis and Risk of Skin Cancer: A Danish Nationwide Cohort Study (1977–2006). Am. J. Clin. Dermatol. 2012, 13, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Arana, A.; Wentworth, C.E.; Fernández-Vidaurre, C.; Schlienger, R.G.; Conde, E.; Arellano, F.M. Incidence of Cancer in the General Population and in Patients with or without Atopic Dermatitis in the U.K. Br. J. Dermatol. 2010, 163, 1036–1043. [Google Scholar] [CrossRef]
- Wiemels, J.L.; Wiencke, J.K.; Li, Z.; Ramos, C.; Nelson, H.H.; Karagas, M.R. Risk of Squamous Cell Carcinoma of the Skin in Relation to IgE: A Nested Case—Control Study. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2377–2383. [Google Scholar] [CrossRef] [Green Version]
- Sritippho, T.; Chotjumlong, P.; Iamaroon, A. Roles of Human Papillomaviruses and p16 in Oral Cancer. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 6193–6200. [Google Scholar] [CrossRef] [Green Version]
- Bzhalava, D.; Eklund, C.; Dillner, J. International Standardization and Classification of Human Papillomavirus Types. Virology 2015, 476, 341–344. [Google Scholar] [CrossRef]
- Bernard, H.-U.; Burk, R.D.; Chen, Z.; van Doorslaer, K.; zur Hausen, H.; de Villiers, E.-M. Classification of Papillomaviruses (PVs) Based on 189 PV Types and Proposal of Taxonomic Amendments. Virology 2010, 401, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Pim, D.; Banks, L. Interaction of Viral Oncoproteins with Cellular Target Molecules: Infection with High-Risk vs. Low-Risk Human Papillomaviruses. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2010, 118, 471–493. [Google Scholar] [CrossRef]
- Chalkia, A.K.; Bontzos, G.; Spandidos, D.A.; Detorakis, E.T. Human Papillomavirus Infection and Ocular Surface Disease (Review). Int. J. Oncol. 2019, 54, 1503–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burk, R.D.; Harari, A.; Chen, Z. Human Papillomavirus Genome Variants. Virology 2013, 445, 232–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Allergy and Infectious Diseases. PaVE: The Papillomavirus Episteme; National Institutes of Health: Bethesda, MD, USA, 2013. [Google Scholar]
- Afrogheh, A.H.; Jakobiec, F.A.; Hammon, R.; Grossniklaus, H.E.; Rocco, J.; Lindeman, N.I.; Sadow, P.M.; Faquin, W.C. Evaluation for High-Risk HPV in Squamous Cell Carcinomas and Precursor Lesions Arising in the Conjunctiva and Lacrimal Sac. Am. J. Surg. Pathol. 2016, 40, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Ramberg, I.; Møller-Hansen, M.; Toft, P.B.; Funding, M.; Heegaard, S. Human Papillomavirus Infection Plays a Role in Conjunctival Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis of Observational Studies. Acta Ophthalmol. 2021, 99, 478–488. [Google Scholar] [CrossRef]
- Mlakar, J.; Kocjan, B.J.; Hošnjak, L.; Pižem, J.; Beltram, M.; Gale, N.; Drnovšek-Olup, B.; Poljak, M. Morphological Characteristics of Conjunctival Squamous Papillomas in Relation to Human Papillomavirus Infection. Br. J. Ophthalmol. 2015, 99, 431–436. [Google Scholar] [CrossRef]
- Kalogeropoulos, C.; Koumpoulis, I.; Papadiotis, E.; Zioga, A.; Gkrepi, K.; Pappa, C.; Paschides, C.; Malamou-Mitsi, V.; Aspiotis, M. Squamous Cell Papilloma of the Conjunctiva Due to Human Papillomavirus (HPV): Presentation of Two Cases and Review of Literature. Clin. Ophthalmol. 2012, 6, 1553. [Google Scholar] [CrossRef] [Green Version]
- George, R.S.; Lewis, D.R.; Archibald, C.W.; Heathcote, G. Bilateral HPV Positive Squamous Cell Carcinoma In Situ of Conjunctiva. Ophthalmic Plast. Reconstr. Surg. 2018, 34, e1–e3. [Google Scholar] [CrossRef]
- Saegusa, M.; Takano, Y.; Hashimura, M.; Okayasu, I.; Shiga, J. HPV Type 16 in Conjunctival and Junctional Papilloma, Dysplasia, and Squamous Cell Carcinoma. J. Clin. Pathol. 1995, 48, 1106–1110. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-M.; Huang, Y.-Y.; Yang, H.-Y.; Tsai, C.-C.; Yu, W.-K.; Kao, S.-C.; Kau, H.-C.; Liu, C.J.-L. Conjunctival Papilloma: Clinical Features, Outcome, and Factors Related to Recurrence. Taiwan J. Ophthalmol. 2018, 8, 15–18. [Google Scholar] [CrossRef]
- Yu, L.; Fei, L.; Liu, X.; Pi, X.; Wang, L.; Chen, S. Application of p16/Ki-67 Dual-Staining Cytology in Cervical Cancers. J. Cancer 2019, 10, 2654–2660. [Google Scholar] [CrossRef] [Green Version]
- Buitrago-Pérez, A.; Garaulet, G.; Vázquez-Carballo, A.; Paramio, J.M.; García-Escudero, R. Molecular Signature of HPV-Induced Carcinogenesis: pRb, p53 and Gene Expression Profiling. Curr. Genom. 2009, 10, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzouri, B.; Luthert, P.J.; Larkin, D.F.P. Papilloma Development and Long-Term Ciclosporin Use in Chronic Ocular Allergy with Associated Keratoconus. Eye Contact Lens 2013, 39, 402–404. [Google Scholar] [CrossRef]
- Verma, V.; Shen, D.; Sieving, P.C.; Chan, C.-C. The Role of Infectious Agents in the Etiology of Ocular Adnexal Neoplasia. Surv. Ophthalmol. 2008, 53, 312–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osahon, A.I.; Ukponmwan, C.U.; Uhunmwangho, O.M. Prevalence of HIV Seropositivity among Patients with Squamous Cell Carcinoma of the Conjunctiva. Asian Pac. J. Trop. Biomed. 2011, 1, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Ramberg, I.; Toft, P.B.; Georgsen, J.B.; Siersma, V.D.; Funding, M.; Jensen, D.H.; von Buchwald, C.; Heegaard, S. Conjunctival Intraepithelial Neoplasia and Carcinoma: Distinct Clinical and Histological Features in Relation to Human Papilloma Virus Status. Br. J. Ophthalmol. 2021, 105, 878–883. [Google Scholar] [CrossRef]
- Abreu, A.L.P.; Souza, R.P.; Gimenes, F.; Consolaro, M.E.L. A Review of Methods for Detect Human Papillomavirusinfection. Virol. J. 2012, 9, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, T.; Choi, W.; Kim, G.E.; Yang, J.M.; Yoon, K.C. Human Papilloma Virus Identification in Ocular Surface Squamous Neoplasia by p16 Immunohistochemistry and DNA Chip Test: A Strobe-Compliant Article. Medicine 2019, 98, e13944. [Google Scholar] [CrossRef]
- Carrilho, C.; Miu, C.; Kim, Y.; Karki, S.; Balmaceda, A.; Challa, B.; Diamond, S.; Monteiro, E.; Marole, E.; Lorenzoni, C.; et al. p16 Expression Correlates with Invasive Ocular Surface Squamous Neoplasms in HIV-Infected Mozambicans. Ocul. Oncol. Pathol. 2020, 6, 123–128. [Google Scholar] [CrossRef]
- Mann, P.; Diamond, S.; Masanganise, R.; Gwanzura, L.; Liu, Y.-T.; Schooley, R.T.; Lin, J.H. HPV16/18 and p16 Gene Expression in Ocular Surface Squamous Neoplasia: A Retrospective Cross-Sectional Analysis. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5594. [Google Scholar]
- Ukpo, O.C.; Flanagan, J.J.; Ma, X.-J.; Luo, Y.; Thorstad, W.L.; Lewis, J.S. High-Risk Human Papillomavirus E6/E7 mRNA Detection by a Novel In Situ Hybridization Assay Strongly Correlates with p16 Expression and Patient Outcomes in Oropharyngeal Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2011, 35, 1343–1350. [Google Scholar] [CrossRef]
- Venuti, A.; Paolini, F. HPV Detection Methods in Head and Neck Cancer. Head Neck Pathol. 2012, 6 (Suppl. 1), 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Wang, L.; Zhong, J.; Chen, S. Diagnostic value of p16INK4A, Ki-67, and Human Papillomavirus L1 Capsid Protein Immunochemical Staining on Cell Blocks from Residual Liquid-Based Gynecologic Cytology Specimens. Cancer Cytopathol. 2010, 118, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Ihloff, A.S.; Görögh, T.; Weise, J.B.; Fazel, A.; Krams, M.; Rittgen, W.; Schwarz, E.; Kahn, T. p16INK4a Overexpression Predicts Translational Active Human Papillomavirus Infection in Tonsillar Cancer. Int. J. Cancer 2010, 127, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Ren, C.; Yang, L.; Zhang, X.; Liu, L.; Wang, Z. Performance of p16/Ki67 Immunostaining, HPV E6/E7 mRNA Testing, and HPV DNA Assay to Detect High-Grade Cervical Dysplasia in Women with ASCUS. BMC Cancer 2019, 19, 271. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhao, Y.; Zou, X.; Wang, L. Relationship of p16 and Ki67 in Recurrence of HPV Infection and Cervical Intraepithelial Neoplasia. Int. J. Clin. Exp. Pathol. 2020, 13, 3174–3180. [Google Scholar]
- Bulten, J.; van der Avoort, I.A.M.; Melchers, W.J.G.; Massuger, L.F.A.G.; Grefte, J.M.M.; Hanselaar, A.G.J.M.; de Wilde, P.C.M. p14ARF and p16INK4A, Two Products of the Same Gene, Are Differently Expressed in Cervical Intraepithelial Neoplasia. Gynecol. Oncol. 2006, 101, 487–494. [Google Scholar] [CrossRef]
- Wong, K.S.; Krane, J.F.; Jo, V.Y. Heterogeneity of p16 Immunohistochemistry and Increased Sensitivity of RNA In Situ Hybridization in Cytology Specimens of HPV-Related Head and Neck Squamous Cell Carcinoma. Cancer Cytopathol. 2019, 127, 632–642. [Google Scholar] [CrossRef]
- Abi-Raad, R.; Prasad, M.L.; Gilani, S.; Garritano, J.; Barlow, D.; Cai, G.; Adeniran, A.J. Quantitative Assessment of p16 Expression in FNA Specimens from Head and Neck Squamous Cell Carcinoma and Correlation with HPV Status. Cancer Cytopathol. 2021, 129, 394–404. [Google Scholar] [CrossRef]
- Rooper, L.M.; Gandhi, M.; Bishop, J.A.; Westra, W.H. RNA In-Situ Hybridization is a Practical and Effective Method for Determining HPV Status of Oropharyngeal Squamous Cell Carcinoma Including Discordant Cases That Are p16 Positive by Immunohistochemistry but HPV Negative by DNA In-Situ Hybridization. Oral Oncol. 2016, 55, 11–16. [Google Scholar] [CrossRef]
- Bishop, J.A.; Ma, X.-J.; Wang, H.; Luo, Y.; Illei, P.B.; Begum, S.; Taube, J.M.; Koch, W.M.; Westra, W.H. Detection of Transcriptionally Active High-risk HPV in Patients with Head and Neck Squamous Cell Carcinoma as Visualized by a Novel E6/E7 mRNA In Situ Hybridization Method. Am. J. Surg. Pathol. 2012, 36, 1874–1882. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.S., Jr.; Ukpo, O.C.; Ma, X.-J.; Flanagan, J.J.; Luo, Y.; Thorstad, W.L.; Chernock, R.D. Transcriptionally-Active High-Risk Human Papillomavirus Is Rare in Oral Cavity and Laryngeal/Hypopharyngeal Squamous Cell Carcinomas—A Tissue Microarray Study Utilizing E6/E7 mRNA In Situ Hybridization. Histopathology 2012, 60, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Flanagan, J.; Su, N.; Wang, L.-C.; Bui, S.; Nielson, A.; Wu, X.; Vo, H.-T.; Ma, X.-J.; Luo, Y. RNAscope: A Novel In Situ RNA Analysis Platform for Formalin-Fixed, Paraffin-Embedded Tissues. J. Mol. Diagn. 2012, 14, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelesidis, T.; Aish, L.; Steller, M.A.; Aish, I.S.; Shen, J.; Foukas, P.; Panayiotides, J.; Petrikkos, G.; Karakitsos, P.; Tsiodras, S. Human Papillomavirus (HPV) Detection Using In Situ Hybridization in Histologic Samples. Am. J. Clin. Pathol. 2011, 136, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, J.A.; Best, S.R.; Rooper, L.M. HPV RNA In-Situ Hybridization as a Diagnostic aid in Papillary Laryngeal Lesions. Laryngoscope 2020, 130, 955–960. [Google Scholar] [CrossRef]
- Pagliusi, S.R.; Garland, S.M. International Standard Reagents for HPV Detection. Dis. Markers 2007, 23, 283–296. [Google Scholar] [CrossRef] [Green Version]
- Pandey, M.; Bhosale, P.G.; Mahimkar, M.B. Detection of HPV E6/E7 mRNA in Clinical Samples Using RNA In Situ Hybridization. Methods Mol. Biol. 2018, 1726, 167–175. [Google Scholar] [CrossRef]
- Coppock, J.D.; Willis, B.C.; Stoler, M.H.; Mills, A.M. HPV RNA In Situ Hybridization Can Inform Cervical Cytology-Histology Correlation. Cancer Cytopathol. 2018, 126, 533–540. [Google Scholar] [CrossRef] [Green Version]
- Suresh, K.; Shah, P.V.; Coates, S.; Alexiev, B.A.; Samant, S. In Situ Hybridization for High Risk HPV E6/E7 mRNA in Oropharyngeal Squamous Cell Carcinoma. Am. J. Otolaryngol. 2021, 42, 102782. [Google Scholar] [CrossRef]
- Outh-Gauer, S.; Augustin, J.; Mandavit, M.; Grard, O.; Denize, T.; Nervo, M.; Lépine, C.; Rassy, M.; Tartour, E.; Badoual, C. Chromogenic In Situ Hybridization as a Tool for HPV-Related Head and Neck Cancer Diagnosis. J. Vis. Exp. JoVE 2019, 148, e59422. [Google Scholar] [CrossRef] [Green Version]
- Henley-Smith, R.; Santambrogio, A.; Andoniadou, C.L.; Odell, E.; Thavaraj, S. RNA In Situ Hybridization for Human Papillomavirus Testing in Oropharyngeal Squamous Cell Carcinoma on a Routine Clinical Diagnostic Platform. J. Oral Pathol. Med. 2021, 50, 68–75. [Google Scholar] [CrossRef]
- Ramberg, I.; Heegaard, S. Human Papillomavirus Related Neoplasia of the Ocular Adnexa. Viruses 2021, 13, 1522. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Mashima, Y.; Kameyama, K.; Mukai, M.; Oguchi, Y. Detection of Human Papillomavirus Infection in Squamous Tumours of the Conjunctiva and Lacrimal Sac by Immunohistochemistry, In Situ Hybridisation, and Polymerase Chain Reaction. Br. J. Ophthalmol. 1997, 81, 308–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annadanam, A.; Vizcaino, M.A.; Eberhart, C.G.; Khurshid, G.S.; Gupta, P. Long Standing Exophytic Conjunctival Papilloma Infected with Human Papillomavirus. J. Eye Ophthalmol. 2017, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Michel, J.; Guiguen, Y.; Léger, F.; Gain, P.; Valanconny, C.; Cambazard, F. Human papilloma virus 6/11 inconjunctival papilloma. Ann. Dermatol. Venereol. 1996, 123, 90–92. [Google Scholar] [PubMed]
- Minchiotti, S.; Masucci, L.; Santos, M.S.D.; Perrella, E.; Graffeo, R.; Lambiase, A.; Bonini, S. Conjunctival Papilloma and Human Papillomavirus: Identification of HPV Types by PCR. Eur. J. Ophthalmol. 2006, 16, 473–477. [Google Scholar] [CrossRef]
- Sjö, N.; Heegaard, S.; Prause, J.U. Conjunctival Papilloma. Acta Ophthalmol. Scand. 2000, 78, 663–666. [Google Scholar] [CrossRef]
- Ikegami, T.; Kise, N.; Kinjyo, H.; Kondo, S.; Suzuki, M.; Tsukahara, N.; Murakami, A.; Kiyuna, A.; Agena, S.; Tanaka, K.; et al. Development of Antibodies against HPV-6 and HPV-11 for the Study of Laryngeal Papilloma. Viruses 2021, 13, 2024. [Google Scholar] [CrossRef]
- Amiling, R.; Meites, E.; Querec, T.D.; Stone, L.; Singh, V.; Unger, E.R.; Derkay, C.S.; Markowitz, L.E. Juvenile-Onset Recurrent Respiratory Papillomatosis in the United States, Epidemiology and HPV Types—2015–2020. J. Pediatr. Infect. Dis. Soc. 2021, 10, 774–781. [Google Scholar] [CrossRef]
- Li, H.; Torabi, S.J.; Yarbrough, W.G.; Mehra, S.; Osborn, H.A.; Judson, B. Association of Human Papillomavirus Status at Head and Neck Carcinoma Subsites with Overall Survival. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 519. [Google Scholar] [CrossRef] [Green Version]
- McCord, C.; Xu, J.; Xu, W.; Qiu, X.; Muhanna, N.; Irish, J.; Leong, I.; McComb, R.J.; Perez-Ordonez, B.; Bradley, G. Association of Human Papilloma Virus with Atypical and Malignant Oral Papillary Lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Mannarini, L.; Kratochvil, V.; Calabrese, L.; Gomes Silva, L.; Morbini, P.; Betka, J.; Benazzo, M. Human Papilloma Virus (HPV) in Head and Neck Region: Review of Literature. Acta Otorhinolaryngol. Ital. 2009, 29, 119–126. [Google Scholar] [PubMed]
- Paver, E.C.; Currie, A.M.; Gupta, R.; Dahlstrom, J.E. Human Papilloma Virus Related Squamous Cell Carcinomas of the Head and Neck: Diagnosis, Clinical Implications and Detection of HPV. Pathology 2020, 52, 179–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatini, M.E.; Chiocca, S. Human Papillomavirus as a Driver of Head and Neck Cancers. Br. J. Cancer 2020, 122, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, P.; El-Hadad, C.; Gruschkus, S.K.; Ning, J.; Hudgens, C.W.; Sagiv, O.; Gross, N.; Tetzlaff, M.T.; Esmaeli, B. PD-L1/PD1 Expression, Composition of Tumor-Associated Immune Infiltrate, and HPV Status in Conjunctival Squamous Cell Carcinoma. Investig. Opthalmol. Vis. Sci. 2019, 60, 2388–2398. [Google Scholar] [CrossRef] [Green Version]
- Galor, A.; Garg, N.; Nanji, A.; Joag, M.; Nuovo, G.; Palioura, S.; Wang, G.; Karp, C.L. Human Papilloma Virus Infection Does Not Predict Response to Interferon Therapy in Ocular Surface Squamous Neoplasia. Ophthalmology 2015, 122, 2210–2215. [Google Scholar] [CrossRef] [Green Version]
- Kaliki, S.; Arepalli, S.; Shields, C.L.; Klein, K.; Sun, H.; Hysenj, E.; Lally, S.E.; Shields, J.A. Conjunctival Papilloma. JAMA Ophthalmol. 2013, 131, 585. [Google Scholar] [CrossRef] [Green Version]
- Theotoka, D.; Morkin, M.I.; Galor, A.; Karp, C.L. Update on Diagnosis and Management of Conjunctival Papilloma. Eye Vis. 2019, 6, 18. [Google Scholar] [CrossRef]
- Galati, L.; Combes, J.D.; Gupta, P.; Sen, R.; Robitaille, A.; Brancaccio, R.N.; Atsou, K.; Cuenin, C.; McKay-Chopin, S.; Tornesello, M.L.; et al. Detection of a Large Spectrum of Viral Infections in Conjunctival Premalignant and Malignant Lesions. Int. J. Cancer 2020, 147, 2862–2870. [Google Scholar] [CrossRef]
- Füst, Á.; Tóth, J.; Imre, L.; Nagy, Z.Z. Non-Malignant Conjunctival Epithelial Masses with Ocular Surface Squamous Neoplasia-Like Optical Coherence Tomography Features. Int. Ophthalmol. 2021, 41, 1827–1834. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lesion Type | Cases | Age Mean ± SD (Range) | Sex N (%) | Bulbar (%) | Palpebral (%) | Forniceal (%) |
|---|---|---|---|---|---|---|
| Papilloma | 33 | 43 ± 17 (9–86) | Male 18 (54) Female 15 (46) | 4/27 (15) | 21/27 (78) | 2/27 (7) |
| CIN/cCIS | 16 | 68 ± 10 (49–90) | Male 11 (69) Female 5 (31) | 9/11 (82) | 2/11 (18) | 0/11 |
| SCC | 4 | 74 ± 12 (61–90) | Male 1 (25) | 0/1 | 1/1 | 0/1 |
| Female 3 (75) | ||||||
| Total | 53 | 53 ± 20 (9–90) | Male 30 (56) Female 23 (44) | 13/39 (33) | 24/39 (62) | 2/39 (5) |
| Cases | Low-Risk Types Positive | High-Risk Types Positive | ||
|---|---|---|---|---|
| RNA ISH | Papilloma | 19 | 17/18 (94%) | 1/15 (7%) |
| CIN/cCIS | 12 | 0/8 | 1/12 (8%) | |
| SCC | 4 | 0/1 | 2/4 (50%) | |
| Papilloma | 14 | 8/12 (75%) | 1/13 (8%) | |
| DNA ISH | CIN/cCIS | 4 | 0/3 | 0/4 |
| SCC | 0 | -- | -- | |
| Overall | Papilloma | 33 | 25/30 (83%) | 2/28 (7%) |
| CIN/cCIS | 16 | 0/11 | 1/16 (6%) | |
| SCC | 4 | 0/1 | 2/4 (50%) |
| HPV Prevalence | Method of Detection | Low-Risk Types Positive | High-Risk Types Positive | Reference |
|---|---|---|---|---|
| 0/14 | PCR | 0/14 | 0/14 | [13] |
| 86/106 (81%) | PCR | 85/86 (99%) | 1/86 (1%) | [14] |
| 19/25 (76%) | PCR | 19/19 | -- | [36] |
| ISH (DNA) | 9/19 (47%) | -- | ||
| 4/4 | PCR | 4/4 | 0/4 | [76] |
| 48/52 (92%) | PCR | 41/47 (87%) | 1/47 (2%) | [77] |
| 4/7 (57%) | PCR | 3/4 (75%) | 0/4 | [73] |
| ISH (DNA) | 1/4 (25%) | 0/4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peterson, C.; Parikh, R.N.; Ahmad, M.T.; Campbell, A.A.; Daoud, Y.; Mahoney, N.; Siadati, S.; Eberhart, C.G. Detection of Human Papillomavirus in Squamous Lesions of the Conjunctiva Using RNA and DNA In-Situ Hybridization. Int. J. Mol. Sci. 2022, 23, 7249. https://doi.org/10.3390/ijms23137249
Peterson C, Parikh RN, Ahmad MT, Campbell AA, Daoud Y, Mahoney N, Siadati S, Eberhart CG. Detection of Human Papillomavirus in Squamous Lesions of the Conjunctiva Using RNA and DNA In-Situ Hybridization. International Journal of Molecular Sciences. 2022; 23(13):7249. https://doi.org/10.3390/ijms23137249
Chicago/Turabian StylePeterson, Cornelia, Rupin N. Parikh, Meleha T. Ahmad, Ashley A. Campbell, Yassine Daoud, Nicholas Mahoney, Sepideh Siadati, and Charles G. Eberhart. 2022. "Detection of Human Papillomavirus in Squamous Lesions of the Conjunctiva Using RNA and DNA In-Situ Hybridization" International Journal of Molecular Sciences 23, no. 13: 7249. https://doi.org/10.3390/ijms23137249