
Protective Effect of Gamma Aminobutyric Acid against Aggravation of Renal Injury Caused by High Salt Intake in Cisplatin-Induced Nephrotoxicity

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
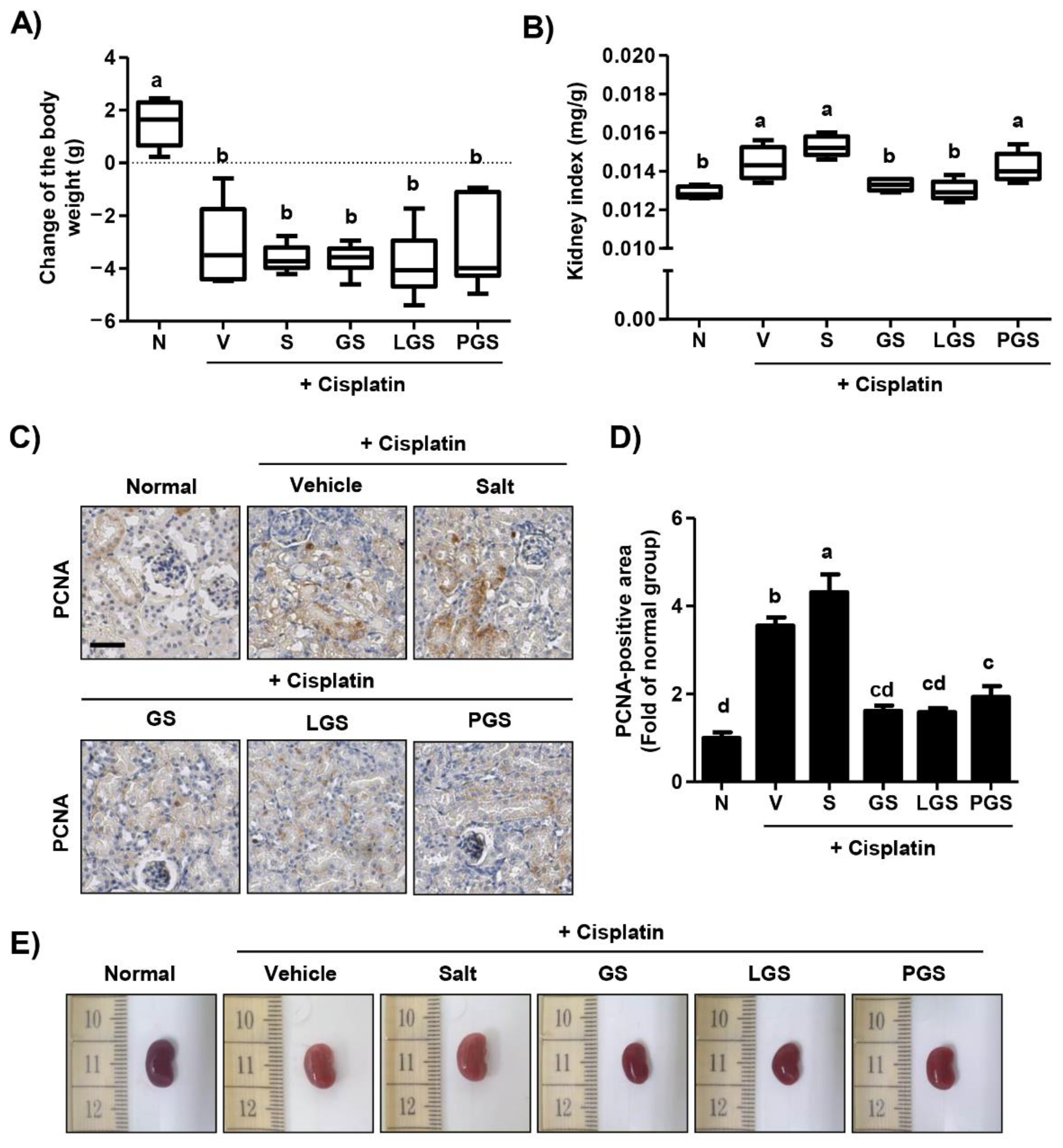
2.1. Effect of GABA on Body Weight Loss and Renal Hypertrophy Caused by High Salt Intake in Cisplatin-Induced Acute Nephrotoxicity
2.2. Effect of GABA on Changes of Hematological and Biochemical Profiles following High Salt Intake in Cisplatin-Induced Acute Nephrotoxicity
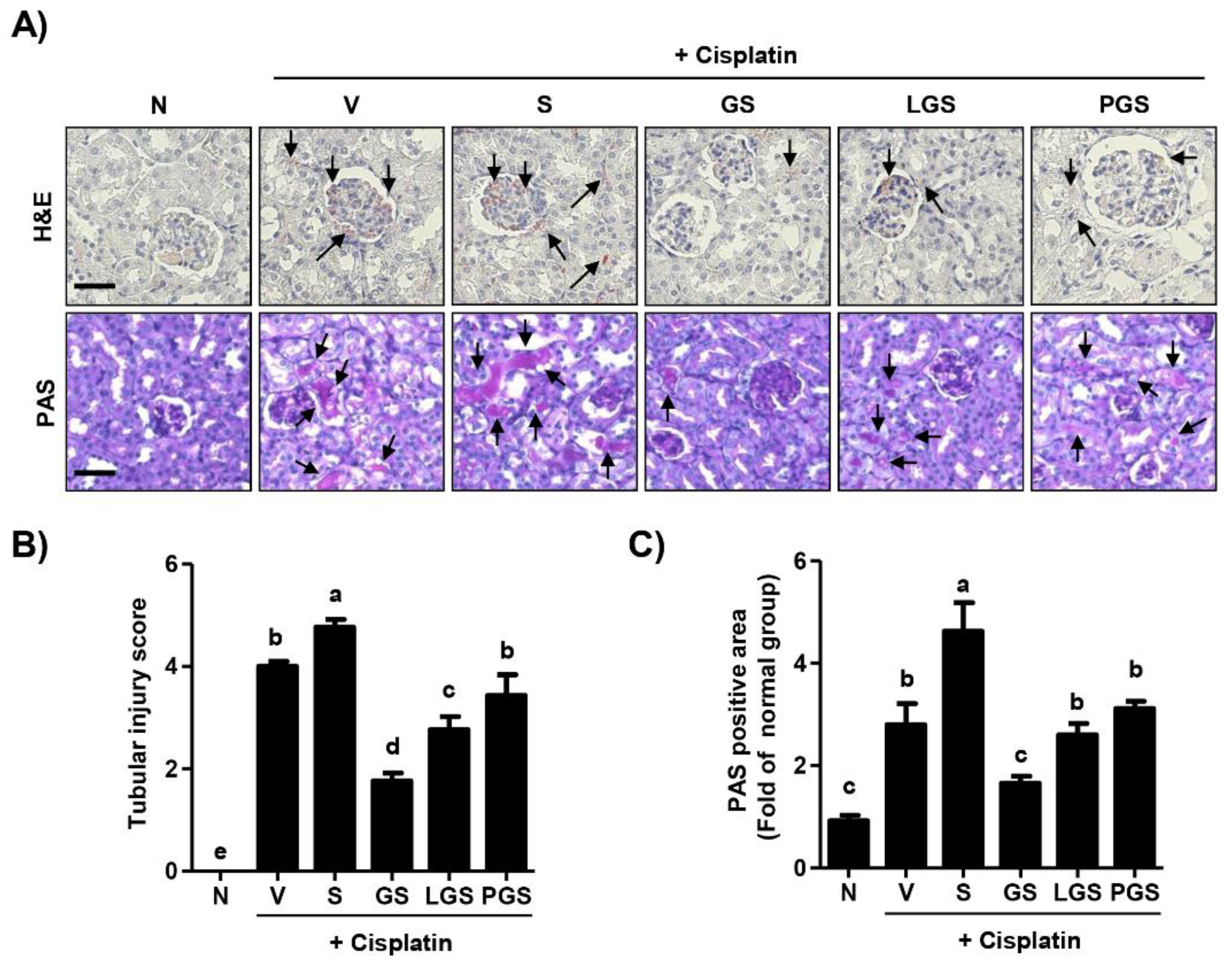
2.3. Effect of GABA on Renal Histologic Changes following High Salt Intake in Cisplatin-Induced Acute Nephrotoxicity
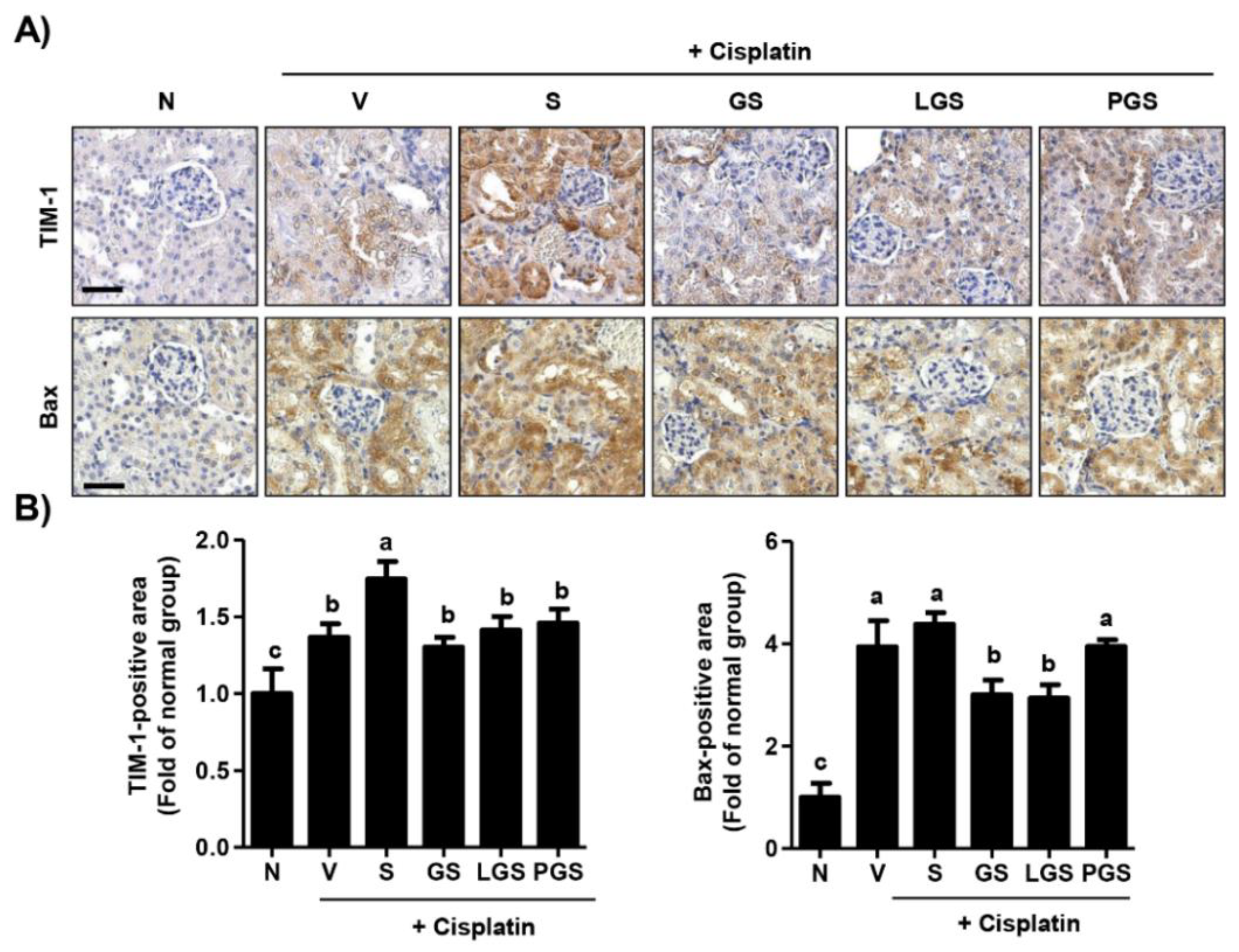
2.4. Effect of GABA Salt on Renal Cell Death in Cisplatin-Induced Acute Nephrotoxicity
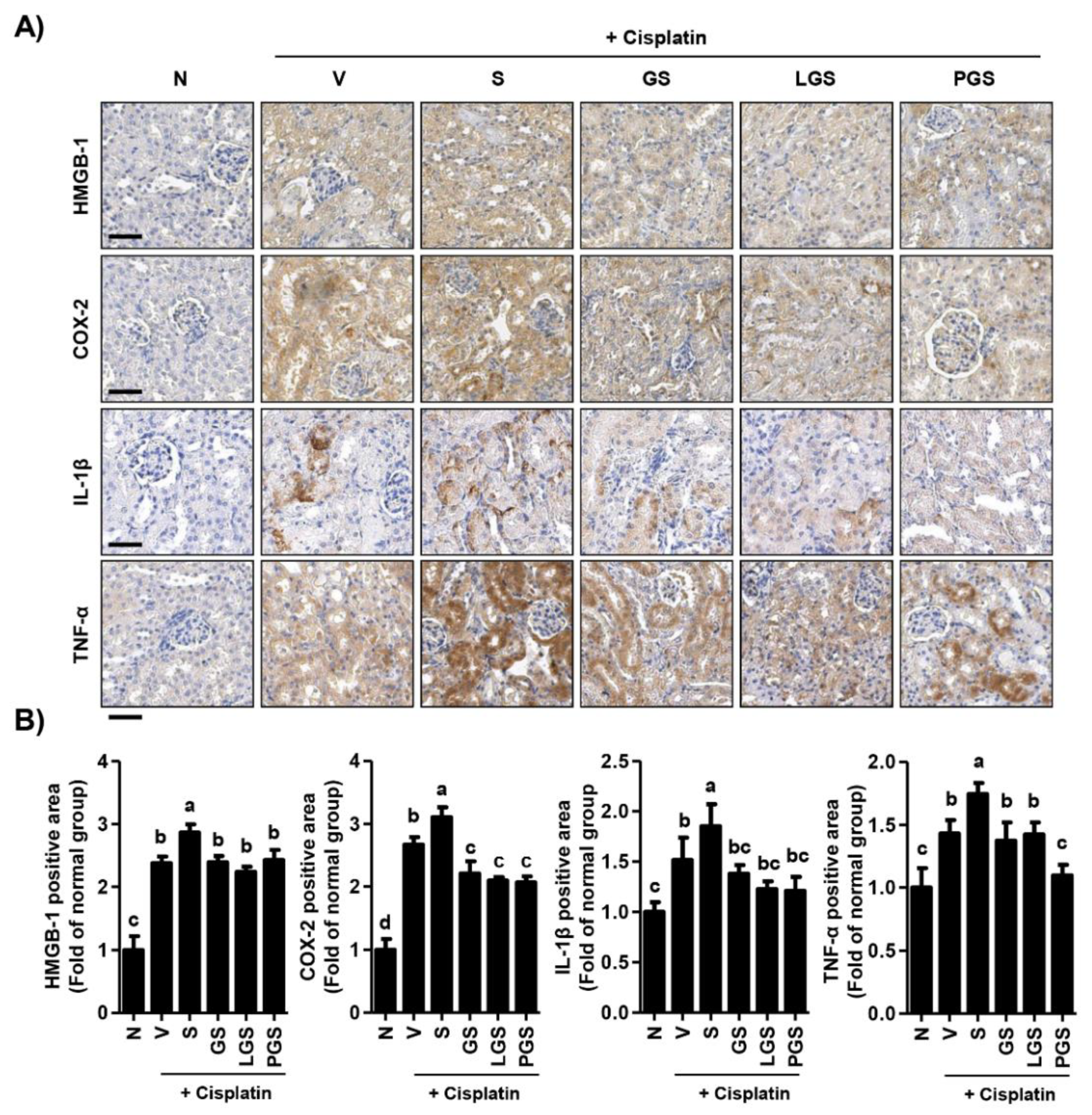
2.5. Effect of GABA Salt on Renal Inflammation in Cisplatin-Induced Acute Nephrotoxicity
3. Discussion
4. Materials and Methods
4.1. Preparation of GABA Salt, Lacto GABA Salt, and Postbiotics GABA Salt
4.2. Animals and Experimental Procedure
4.3. Hematological and Biochemical Analysis
4.4. Histopathological Analysis
4.5. Immunohistochemical Examination
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tuomilehto, J.; Jousilahti, P.; Rastenyte, D.; Moltchanov, V.; Tanskanen, A.; Pietinen, P.; Nissinen, A. Urinary sodium excretion and cardiovascular mortality in Finland: A prospective study. Lancet 2001, 357, 848–851. [Google Scholar] [CrossRef]
- Borrelli, S.; Provenzano, M.; Gagliardi, I.; Michael, A.; Liberti, M.E.; De Nicola, L.; Conte, G.; Garofalo, C.; Andreucci, M. Sodium intake and chronic kidney disease. Int. J. Mol. Sci. 2020, 21, 4744. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Ritz, E.; Koleganova, N.; Piecha, G. Role of sodium intake in the progression of chronic kidney disease. J. Ren. Nutr. 2009, 19, 61–62. [Google Scholar] [CrossRef] [PubMed]
- Cianciaruso, B.; Bellizzi, V.; Minutolo, R.; Tavera, A.; Capuano, A.; Conte, G.; De Nicola, L. Salt intake and renal outcome in patients with progressive renal disease. Miner. Electrolyte Metab. 1998, 24, 296–301. [Google Scholar] [CrossRef]
- Dworkin, L.D.; Benstein, J.A.; Tolbert, E.; Feiner, H.D. Salt restriction inhibits renal growth and stabilizes injury in rats with established renal disease. J. Am. Soc. Nephrol. 1996, 7, 437–442. [Google Scholar] [CrossRef]
- Sanders, P.W. Salt intake, endothelial cell signaling, and progression of kidney disease. Hypertension 2004, 43, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Yamamoto, T.; Ikegaya, N.; Hishida, A. Dietary salt intake modulates progression of antithymocyte serum nephritis through alteration of glomerular angiotensin II receptor expression. Am. J. Physiol. Renal Physiol. 2004, 286, F267–F277. [Google Scholar] [CrossRef]
- Balafa, O.; Kalaitzidis, R.G. Salt sensitivity and hypertension. J. Hum. Hypertens. 2021, 35, 184–192. [Google Scholar] [CrossRef]
- Hirohama, D.; Fujita, T. Evaluation of the pathophysiological mechanisms of salt-sensitive hypertension. Hypertens. Res. 2019, 42, 1848–1857. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- Bowery, N.G.; Smart, T.G. GABA and glycine as neurotransmitters: A brief history. Br. J. Pharmacol. 2006, 147, S109–S119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oketch-Rabah, H.A.; Madden, E.F.; Roe, A.L.; Betz, J.M. United States Pharmacopeia (USP) safety review of gamma-aminobutyric acid (GABA). Nutrients 2021, 13, 2742. [Google Scholar] [CrossRef]
- Hepsomali, P.; Groeger, J.A.; Nishihira, J.; Scholey, A. Effects of oral gamma-aminobutyric acid (GABA) administration on stress and sleep in humans: A systematic review. Front. Neurosci. 2020, 14, 923. [Google Scholar] [CrossRef]
- Ngo, D.H.; Vo, T.S. An updated review on pharmaceutical properties of gamma-aminobutyric acid. Molecules 2019, 24, 2678. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Shirai, T.; Ochiai, H.; Kasao, M.; Hayakawa, K.; Kimura, M.; Sansawa, H. Blood-pressure-lowering effect of a novel fermented milk containing gamma-aminobutyric acid (GABA) in mild hypertensives. Eur. J. Clin. Nutr. 2003, 57, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Hayakawa, K.; Kimura, M.; Kasaha, K.; Matsumoto, K.; Sansawa, H.; Yamori, Y. Effect of a gamma-aminobutyric acid-enriched dairy product on the blood pressure of spontaneously hypertensive and normotensive Wistar-Kyoto rats. Br. J. Nutr. 2004, 92, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Yoshida, S.; Haramoto, M.; Mizuno, H.; Fukuda, T.; Kagami-Katsuyama, H.; Tanaka, A.; Ohkawara, T.; Sato, Y.; Nishihira, J. Effects of white rice containing enriched gamma-aminobutyric acid on blood pressure. J. Tradit. Complement Med. 2015, 6, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.; Lee, Y.M.; Oh, J.; Jung, S.; Oh, J.W. Effects of gamma-aminobutyric acid and piperine on gene regulation in pig kidney epithelial cell lines. Asian-Australas J. Anim. Sci. 2020, 33, 1497–1506. [Google Scholar] [CrossRef] [Green Version]
- Li, H.B.; Huo, C.J.; Su, Q.; Li, X.; Bai, J.; Zhu, G.Q.; Kang, Y.M. Exercise training attenuates proinflammatory cytokines, oxidative stress and modulates neurotransmitters in the rostral ventrolateral medulla of salt-induced hypertensive rats. Cell. Physiol. Biochem. 2018, 48, 1369–1381. [Google Scholar] [CrossRef]
- Son, M.; Oh, S.; Lee, H.S.; Choi, J.; Lee, B.J.; Park, J.H.; Park, C.H.; Son, K.H.; Byun, K. Gamma-aminobutyric acid-salt attenuated high cholesterol/high salt diet induced hypertension in mice. Korean J. Physiol. Pharmacol. 2021, 25, 27–38. [Google Scholar] [CrossRef]
- Arany, I.; Safirstein, R.L. Cisplatin nephrotoxicity. Semin. Nephrol. 2003, 23, 460–464. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S. Cisplatin: The first metal based anticancer drug. Bioorg. Chem. 2019, 88, 102925. [Google Scholar] [CrossRef]
- Fuertes, M.A.; Castilla, J.; Alonso, C.; Pérez, J.M. Cisplatin biochemical mechanism of action: From cytotoxicity to induction of cell death through interconnections between apoptotic and necrotic pathways. Curr. Med. Chem. 2003, 10, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Ma, H.; Shao, J.; Wu, J.; Zhou, L.; Zhang, Z.; Wang, Y.; Huang, Z.; Ren, J.; Liu, S.; et al. A role for tubular necroptosis in cisplatin-induced AKI. J. Am. Soc. Nephrol. 2015, 26, 2647–2658. [Google Scholar] [CrossRef] [Green Version]
- Heyman, S.N.; Rosen, S.; Rosenberger, C. Animal models of renal dysfunction: Acute kidney injury. Expert. Opin. Drug Discov. 2009, 4, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Perše, M.; Večerić-Haler, Ž. Cisplatin-induced rodent model of kidney injury: Characteristics and challenges. Biomed. Res. Int. 2018, 2018, 1462802. [Google Scholar] [CrossRef]
- Awdishu, L.; Mehta, R.L. The 6R’s of drug induced nephrotoxicity. BMC Nephrol. 2017, 18, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naushad, M.; Urooj, M.; Ahmad, T.; Husain, G.M.; Kazmi, M.H.; Zakir, M. Nephroprotective effect of Tukhm-e-Karafs (Apium graveolens L.) against cisplatin-induced nephrotoxicity. J. Ayurveda Integr. Med. 2021, 12, 607–615. [Google Scholar] [CrossRef]
- Ma, Z.N.; Li, Y.Z.; Li, W.; Yan, X.T.; Yang, G.; Zhang, J.; Zhao, L.C.; Yang, L.M. Nephroprotective effects of saponins from leaves of Panax quinquefolius against cisplatin-induced acute kidney injury. Int. J. Mol. Sci. 2017, 18, 1407. [Google Scholar] [CrossRef]
- Aladaileh, S.H.; Al-Swailmi, F.K.; Abukhalil, M.H.; Ahmeda, A.F.; Mahmoud, A.M. Punicalagin prevents cisplatin-induced nephrotoxicity by attenuating oxidative stress, inflammatory response, and apoptosis in rats. Life Sci. 2021, 286, 120071. [Google Scholar] [CrossRef]
- Loeffler, I.; Wolf, G. Transforming growth factor-β and the progression of renal disease. Nephrol. Dial. Transpl. 2014, 29, i37–i45. [Google Scholar] [CrossRef] [Green Version]
- Menshikh, A.; Scarfe, L.; Delgado, R.; Finney, C.; Zhu, Y.; Yang, H.; de Caestecker, M.P. Capillary rarefaction is more closely associated with CKD progression after cisplatin, rhabdomyolysis, and ischemia-reperfusion-induced AKI than renal fibrosis. Am. J. Physiol. Renal Physiol. 2019, 317, F1383–F1397. [Google Scholar] [CrossRef]
- Qi, J.; Xue, Q.; Kuang, L.; Xie, L.; Luo, R.; Nie, X. Berberine alleviates cisplatin-induced acute kidney injury by regulating mitophagy via PINK 1/Parkin pathway. Transl. Androl. Urol. 2020, 9, 1712–1724. [Google Scholar] [CrossRef] [PubMed]
- Pabla, N.; Dong, Z. Cisplatin nephrotoxicity: Mechanisms and renoprotective strategies. Kidney Int. 2008, 73, 994–1007. [Google Scholar] [CrossRef] [Green Version]
- Rana, A.; Sathyanarayana, P.; Lieberthal, W. Role of apoptosis of renal tubular cells in acute renal failure: Therapeutic implications. Apoptosis 2001, 6, 83–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xia, W.; Long, G.; Pei, Z.; Li, Y.; Wu, M.; Wang, Q.; Zhang, Y.; Jia, Z.; Chen, H. Isoquercitrin ameliorates cisplatin-induced nephrotoxicity via the inhibition of apoptosis, inflammation, and oxidative stress. Front. Pharmacol. 2020, 11, 599416. [Google Scholar] [CrossRef]
- Faubel, S.; Lewis, E.C.; Reznikov, L.; Ljubanovic, D.; Hoke, T.S.; Somerset, H.; Oh, D.J.; Lu, L.; Klein, C.L.; Dinarello, C.A.; et al. Cisplatin-induced acute renal failure is associated with an increase in the cytokines interleukin (IL)-1beta, IL-18, IL-6, and neutrophil infiltration in the kidney. J. Pharmacol. Exp. Ther. 2007, 322, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; De Leon, M.; Devarajan, P. Cisplatin induces apoptosis in LLC-PK1 cells via activation of mitochondrial pathways. J. Am. Soc. Nephrol. 2002, 13, 858–865. [Google Scholar] [CrossRef]
- Su, J.; Liu, X.; Xu, C.; Lu, X.; Wang, F.; Fang, H.; Lu, A.; Qiu, Q.; Li, C.; Yang, T. NF-κB-dependent upregulation of (pro)renin receptor mediates high-NaCl-induced apoptosis in mouse inner medullary collecting duct cells. Am. J. Physiol. Cell Physiol. 2017, 313, C612–C620. [Google Scholar] [CrossRef] [PubMed]
- Michea, L.; Ferguson, D.R.; Peters, E.M.; Andrews, P.M.; Kirby, M.R.; Burg, M.B. Cell cycle delay and apoptosis are induced by high salt and urea in renal medullary cells. Am. J. Physiol. Renal Physiol. 2000, 278, F209–F218. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Bailly, V.; Abichandani, R.; Thadhani, R.; Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A novel biomarker for human renal proximal tubule injury. Kidney Int. 2002, 62, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Kim, B.; Sim, H.; Lee, T.K.; Tae, H.J.; Lee, J.C.; Park, J.H.; Cho, J.H.; Won, M.H.; Park, Y.; et al. Hypothermic treatment reduces matrix metalloproteinase-9 expression and damage in the liver following asphyxial cardiac arrest in rats. Lab. Anim. Res. 2021, 37, 16. [Google Scholar] [CrossRef] [PubMed]
- Rosen, S.; Heyman, S.N. Difficulties in understanding human “acute tubular necrosis”: Limited data and flawed animal models. Kidney Int. 2001, 60, 1220–1224. [Google Scholar] [CrossRef] [Green Version]
- Sharp, C.N.; Siskind, L.J. Developing better mouse models to study cisplatin-induced kidney injury. Am. J. Physiol. Renal Physiol. 2017, 313, F835–F841. [Google Scholar] [CrossRef] [Green Version]
- Dehghani, A.; Saberi, S.; Nematbakhsh, M. Cisplatin-induced nephrotoxicity alters blood pressure response to angiotensin II administration in rats. Adv. Biomed. Res. 2016, 5, 53. [Google Scholar]
- McSweeney, K.R.; Gadanec, L.K.; Qaradakhi, T.; Ali, B.A.; Zulli, A.; Apostolopoulos, V. Mechanisms of cisplatin-induced acute kidney injury: Pathological mechanisms, pharmacological interventions, and genetic mitigations. Cancers 2021, 13, 1572. [Google Scholar] [CrossRef]
- Kim, M.J.; Moon, D.; Jung, S.; Lee, J.; Kim, J. Cisplatin nephrotoxicity is induced via poly(ADP-ribose) polymerase activation in adult zebrafish and mice. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 318, R843–R854. [Google Scholar] [CrossRef]
- Wada, Y.; Iyoda, M.; Matsumoto, K.; Shindo-Hirai, Y.; Kuno, Y.; Yamamoto, Y.; Suzuki, T.; Saito, T.; Iseri, K.; Shibata, T. Epidermal growth factor receptor inhibition with erlotinib partially prevents cisplatin-induced nephrotoxicity in rats. PLoS ONE 2014, 9, e111728. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Lee, C.H. Development of therapeutic antibodies and modulating the characteristics of therapeutic antibodies to maximize the therapeutic efficacy. Biotechnol. Bioprocess Eng. 2021, 26, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Jennes, L. Immunohistochemical detection of neuropeptides/transmitters in mammalian brain. Methods Cell Biol. 2013, 113, 123–147. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| +Cisplatin | ||||||
|---|---|---|---|---|---|---|
| Normal | Vehicle | Salt | GS | LGS | PGS | |
| RBC (106/μL) | 10.14 ± 0.37 NS | 10.55 ± 0.56 | 10.71 ± 0.51 | 10.67 ± 0.39 | 10.86 ± 0.26 | 10.81 ± 0.56 |
| WBC (103/μL) | 2.43 ± 0.69 a | 1.27 ± 0.31 b | 1.28 ± 0.32 b | 1.62 ± 0.23 b | 1.35 ± 0.12 b | 1.30 ± 0.33 b |
| Hematocrit (%) | 57.30 ± 2.51 NS | 57.15 ± 2.74 | 59.45 ± 2.33 | 58.77 ± 1.85 | 60.22 ± 2.05 | 60.62 ± 3.12 |
| Hemoglobin (g/dL) | 16.10 ± 0.71 NS | 16.43 ± 0.87 | 16.75 ± 0.87 | 16.78 ± 0.50 | 16.96 ± 0.67 | 17.07 ± 0.62 |
| MCV (fL) | 56.57 ± 0.99 NS | 55.23 ± 1.17 | 55.08 ± 0.53 | 55.91 ± 1.20 | 55.07 ± 0.86 | 56.16 ± 0.42 |
| MCH (pg) | 16.13 ± 0.40 NS | 15.87 ± 0.28 | 15.68 ± 0.10 | 15.71 ± 0.23 | 15.67 ± 0.28 | 15.70 ± 0.42 |
| MCHC (g/dL) | 28.09 ± 0.64 NS | 28.73 ± 0.27 | 28.51 ± 0.50 | 28.33 ± 0.63 | 28.30 ± 0.86 | 27.74 ± 0.84 |
| Platelet (103/μL) | 922.75 ± 121.44 a | 599.83 ± 128.30 bc | 450.43 ± 132.07 c | 652.83 ± 104.90 b | 601.67 ± 82.69 bc | 596.00 ± 124.38 bc |
| AST (U/L) | 101.90 ± 15.30 NS | 93.55 ± 16.89 | 90.84 ± 20.84 | 96.01 ± 17.40 | 95.70 ± 31.31 | 103.96 ± 19.24 |
| ALT (U/L) | 19.55 ± 2.20 NS | 24.68 ± 3.17 | 22.15 ± 2.40 | 19.03 ± 6.89 | 20.47 ± 5.79 | 22.33 ± 6.03 |
| ALP (U/L) | 265.72 ± 37.43 NS | 236.38 ± 13.16 | 244.94 ± 26.36 | 223.56 ± 68.77 | 224.13 ± 52.65 | 223.08 ± 30.54 |
| BUN (mg/dL) | 14.31 ± 0.54 c | 18.74 ± 1.45 a | 20.46 ± 2.83 a | 16.15 ± 1.53 b | 18.86 ± 1.65 a | 19.21 ± 1.93 a |
| Creatinine (mg/dL) | 0.40 ± 0.06 d | 0.60 ± 0.06 bc | 0.69 ± 0.05 a | 0.56 ± 0.02 c | 0.62 ± 0.03 b | 0.66 ± 0.03 ab |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Ji, S.Y.; Hwangbo, H.; Kim, M.Y.; Kim, D.H.; Park, B.S.; Park, J.-H.; Lee, B.-J.; Kim, G.-Y.; Jeon, Y.-J.; et al. Protective Effect of Gamma Aminobutyric Acid against Aggravation of Renal Injury Caused by High Salt Intake in Cisplatin-Induced Nephrotoxicity. Int. J. Mol. Sci. 2022, 23, 502. https://doi.org/10.3390/ijms23010502
Lee H, Ji SY, Hwangbo H, Kim MY, Kim DH, Park BS, Park J-H, Lee B-J, Kim G-Y, Jeon Y-J, et al. Protective Effect of Gamma Aminobutyric Acid against Aggravation of Renal Injury Caused by High Salt Intake in Cisplatin-Induced Nephrotoxicity. International Journal of Molecular Sciences. 2022; 23(1):502. https://doi.org/10.3390/ijms23010502
Chicago/Turabian StyleLee, Hyesook, Seon Yeong Ji, Hyun Hwangbo, Min Yeong Kim, Da Hye Kim, Beom Su Park, Joung-Hyun Park, Bae-Jin Lee, Gi-Young Kim, You-Jin Jeon, and et al. 2022. "Protective Effect of Gamma Aminobutyric Acid against Aggravation of Renal Injury Caused by High Salt Intake in Cisplatin-Induced Nephrotoxicity" International Journal of Molecular Sciences 23, no. 1: 502. https://doi.org/10.3390/ijms23010502