A Potential Serum N-glycan Biomarker for Hepatitis C Virus-Related Early-Stage Hepatocellular Carcinoma with Liver Cirrhosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
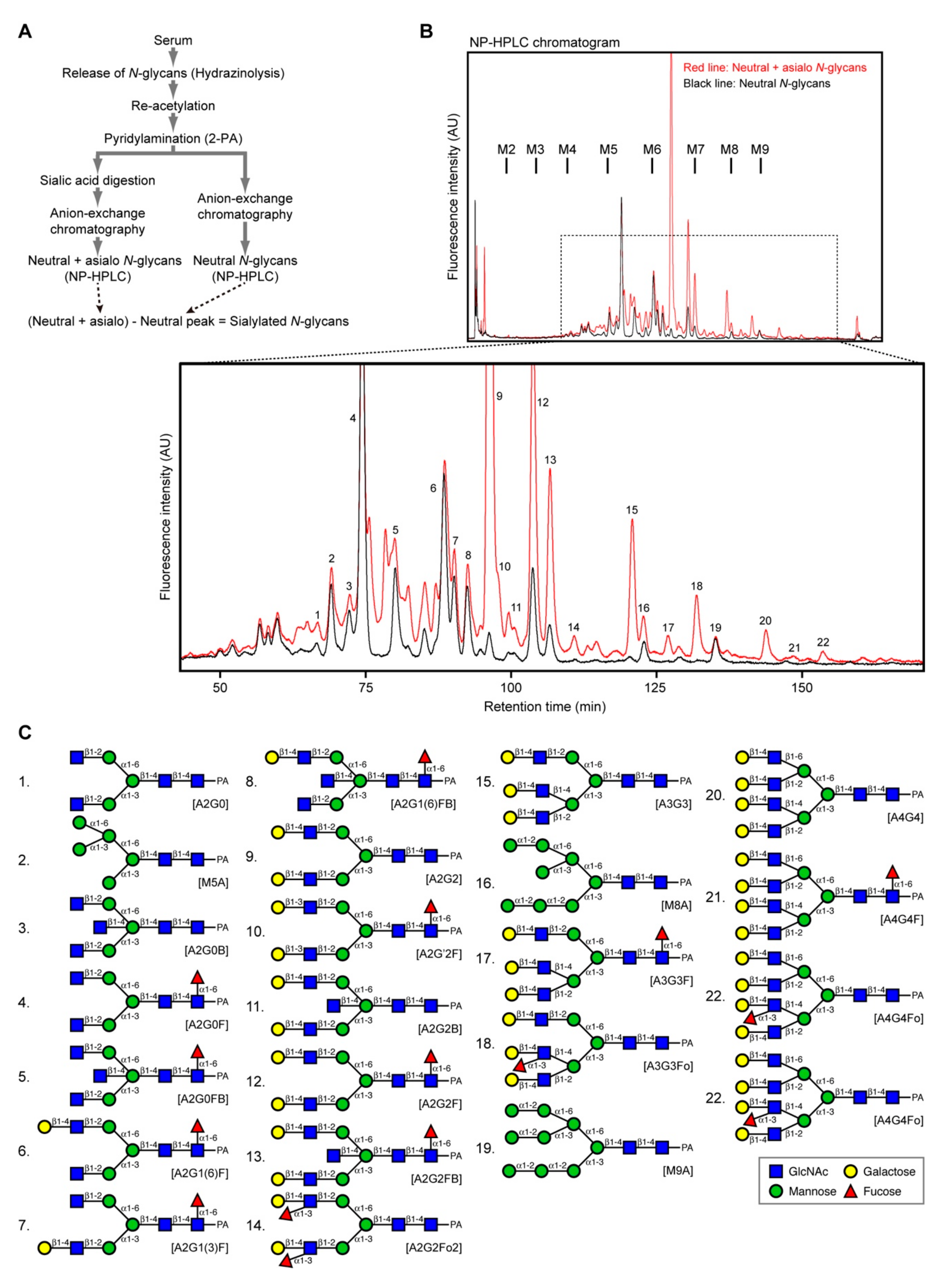
2.1. Experimental Design
2.2. N-Glycans Remain Stable in Sera for at Least One Day
2.3. N-Glycan Recovery Rate Is Highly Reproducible
2.4. N-Glycan Profiles in Human Sera
2.5. Exploring N-Glycans as Potential Early-Stage HCC Markers
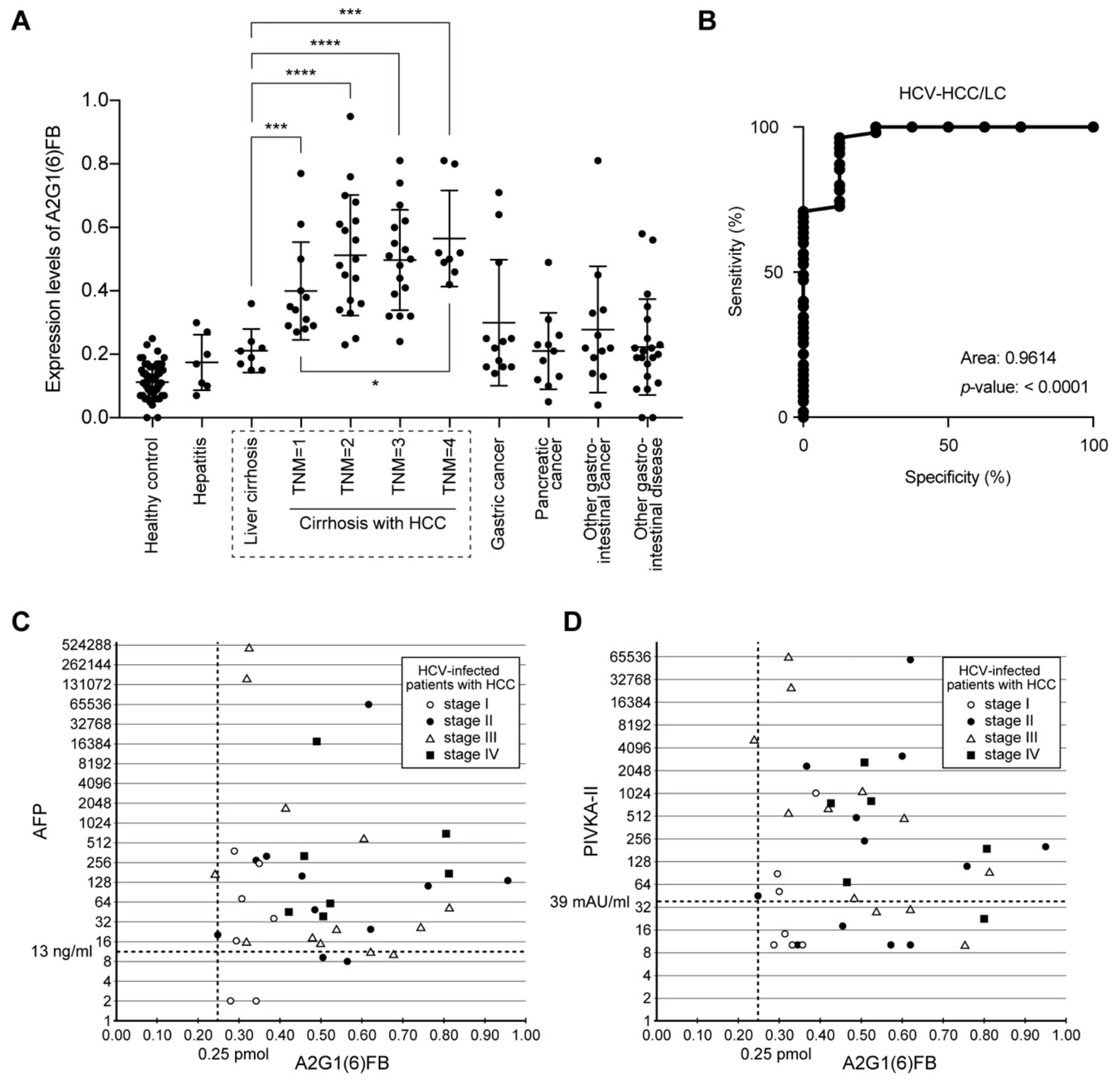
2.6. A2G1(6)FB N-Glycan Marks Early-Stage HCC
2.7. Sensitivity and Specificity of A2G1(6)FB in HCC
2.8. No Correlation between A2G1(6)FB and AFP or PIVKA-II
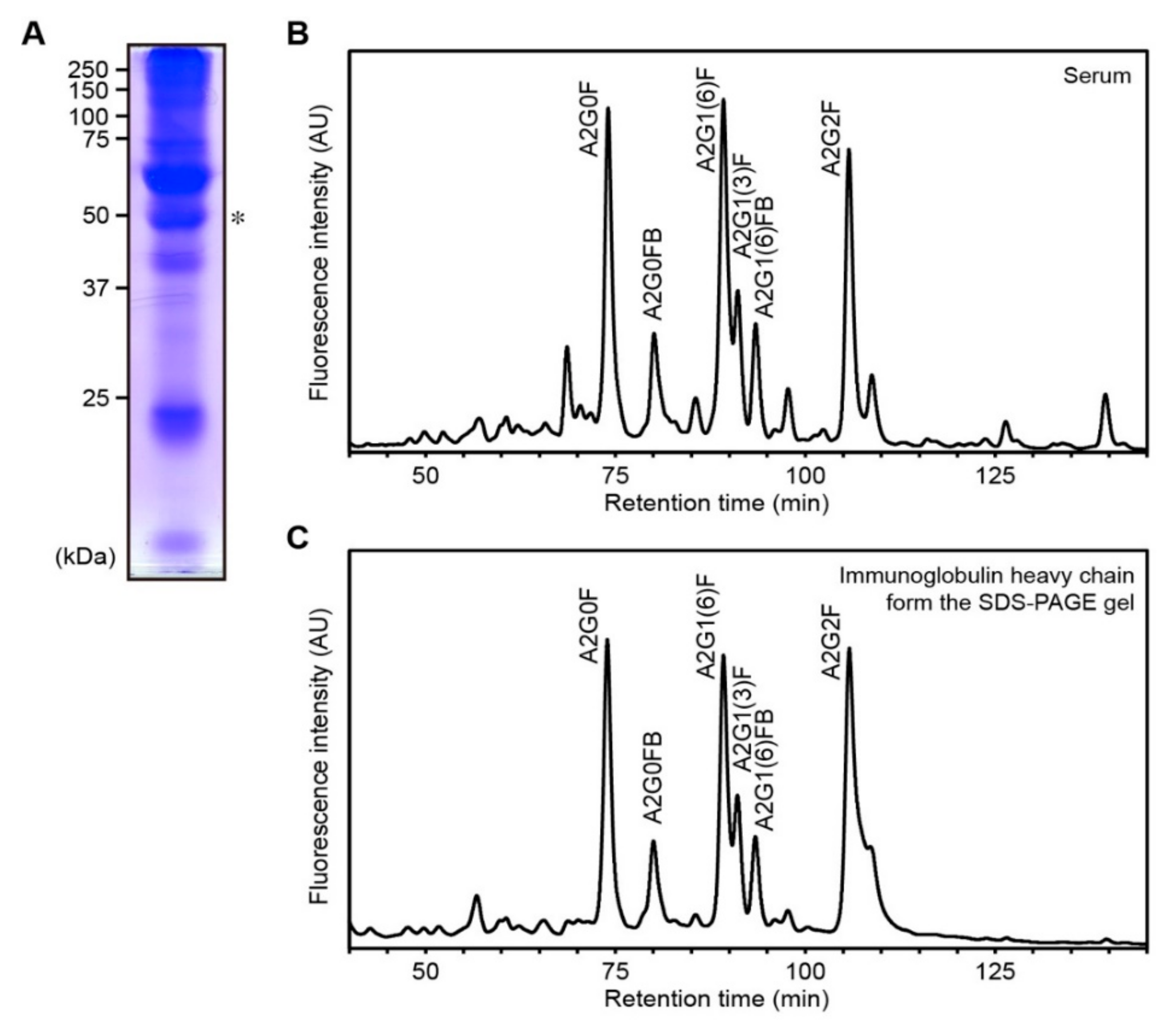
2.9. A2G1(6)FB Is Harbored on Ig Heavy Chain
3. Discussion
3.1. Comparison with Other N-Glycan Markers for HCC
3.2. Characterization and structure of N-glycan A2G1(6)FB
4. Materials and Methods
4.1. Patients, Ethics, and Clinical Diagnosis
4.2. Sample Preparations
4.3. N-Glycan Analyses
4.4. Data Quantification and Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AFP | alpha-fetoprotein |
| AU | arbitrary unit |
| AUC | area under the curve |
| CBB | Coomassie Brilliant Blue |
| E4-PHA | erythroagglutinating phytohemagglutinin |
| GnT | N-acetylglucosaminyltransferase |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| HPLC | high-performance liquid chromatography |
| IgG | immunoglobulin G |
| LC | liver cirrhosis |
| LCA | Lens culinaris agglutinin |
| NP | normal-phase |
| PA | pyridylaminated |
| PIVKA-II | protein induced by vitamin K absence or antagonists-II |
| ROC | receiver operating characteristic |
| RP | reverse-phase |
| SDS-PAGE | sodium dodecyl sulfate polyacrylamide gel electrophoresis |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, F.X.; Ribes, J.; Cléries, R.; Díaz, M. Epidemiology of Hepatocellular Carcinoma. Clin. Liver Dis. 2005, 9, 191–211. [Google Scholar] [CrossRef] [PubMed]
- Okuda, K.; Tanaka, M.; Kanazawa, N.; Nagashima, J.; Satomura, S.; Kinoshita, H.; Eriguchi, N.; Aoyagi, S.; Kojiro, M. Evaluation of curability and prediction of prognosis after surgical treatment for hepatocellular carcinoma by lens culinaris agglutinin-reactive alpha-fetoprotein. Int. J. Oncol. 1999, 14, 265–336. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, Y.; Mita, Y.; Suda, T.; Kawai, K.; Kuroiwa, T.; Igarashi, M.; Kobayashi, M.; Waguri, N.; Asakura, H. The fucosylation index of serum α-fetoprotein as useful prognostic factor in patients with hepatocellular carcinoma in special reference to chronological changes. Hepatol. Res. 2002, 23, 287–295. [Google Scholar] [CrossRef]
- Igarashi, H.; Aoyagi, Y.; Suda, T.; Mita, Y.; Kawai, K. Studies on the correlation among the fucosylation index, concentration of alpha-fetoprotein and des-gamma-carboxy prothrombin as prognostic indicators in hepatocellular carcinoma. Hepatol. Res. 2003, 27, 280–288. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Suzuki, Y.; Isemura, M.; Nomoto, M.; Sekine, C.; Igarashi, K.; Ichida, F. The fucosylation index of alpha-fetoprotein and its usefulness in the early diagnosis of hepatocellular carcinoma. Cancer 1988, 61, 769–774. [Google Scholar] [CrossRef]
- Comunale, M.A.; Lowman, M.; Long, R.E.; Krakover, J.; Philip, R.; Seeholzer, S.; Evans, A.A.; Hann, H.-W.L.; Block, T.M.; Mehta, A.S. Proteomic Analysis of Serum Associated Fucosylated Glycoproteins in the Development of Primary Hepatocellular Carcinoma. J. Proteome Res. 2006, 5, 308–315. [Google Scholar] [CrossRef]
- Comunale, M.A.; Wang, M.; Hafner, J.; Krakover, J.; Rodemich, L.; Kopenhaver, B.; Long, R.E.; Junaidi, O.; Di Bisceglie, A.M.; Block, T.M.; et al. Identification and Development of Fucosylated Glycoproteins as Biomarkers of Primary Hepatocellular Carcinoma. J. Proteome Res. 2009, 8, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.-E.; Desmyter, L.; Gao, C.-F.; Laroy, W.; Dewaele, S.; Vanhooren, V.; Wang, L.; Zhuang, H.; Callewaert, N.; Libert, C.; et al. N-glycomic changes in hepatocellular carcinoma patients with liver cirrhosis induced by hepatitis B virus. Hepatology 2007, 46, 1426–1435. [Google Scholar] [CrossRef]
- Debruyne, E.N.; Vanderschaeghe, D.; Van Vlierberghe, H.; Vanhecke, A.; Callewaert, N.; Delanghe, J. Diagnostic Value of the Hemopexin N-Glycan Profile in Hepatocellular Carcinoma Patients. Clin. Chem. 2010, 56, 823–831. [Google Scholar] [CrossRef]
- Hase, S.; Ikenaka, K.; Mikoshiba, K.; Ikenaka, T. Analysis of tissue glycoprotein sugar chains by two-dimensional high-performance liquid chromatographic mapping. J. Chromatogr. B: Biomed. Sci. Appl. 1988, 434, 51–60. [Google Scholar] [CrossRef]
- Takahashi, N. Three-dimensional mapping of N-linked oligosaccharides using anion-exchange, hydrophobic and hydrophilic interaction modes of high-performance liquid chromatography. J. Chromatogr. A 1996, 720, 217–225. [Google Scholar] [CrossRef]
- Torii, T.; Yoshimura, T.; Narumi, M.; Hitoshi, S.; Takaki, Y.; Tsuji, S.; Ikenaka, K. Determination of major sialylated N-glycans and identification of branched sialylated N-glycans that dynamically change their content during development in the mouse cerebral cortex. Glycoconj. J. 2014, 31, 671–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanabe, K.; Ikenaka, K. In-column removal of hydrazine and N-acetylation of oligosaccharides released by hydrazionolysis. Anal. Biochem. 2006, 348, 324–326. [Google Scholar] [CrossRef]
- Yoshimura, T.; Yamada, G.; Narumi, M.; Koike, T.; Ishii, A.; Sela, I.; Mitrani-Rosenbaum, S.; Ikenaka, K. Detection of N-glycans on small amounts of glycoproteins in tissue samples and sodium dodecyl sulfate–polyacrylamide gels. Anal. Biochem. 2012, 423, 253–260. [Google Scholar] [CrossRef]
- Gornik, O.; Wagner, J.; Pučić, M.; Knežević, A.; Redžić, I.; Lauc, G. Stability of N-glycan profiles in human plasma. Glycobiology 2009, 19, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Miura, Y.; Hato, M.; Shinohara, Y.; Kuramoto, H.; Kurogochi, M.; Shimaoka, H.; Tada, M.; Nakanishi, K.; Ozaki, M.; Furukawa, J.-I.; et al. BlotGlycoABC™, an Integrated Glycoblotting Technique for Rapid and Large Scale Clinical Glycomics. Mol. Cell. Proteom. 2007, 7, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Kamiyama, T.; Yokoo, H.; Furukawa, J.-I.; Kurogochi, M.; Togashi, T.; Miura, N.; Nakanishi, K.; Kamachi, H.; Kakisaka, T.; Tsuruga, Y.; et al. Identification of novel serum biomarkers of hepatocellular carcinoma using glycomic analysis. Hepatology 2013, 57, 2314–2325. [Google Scholar] [CrossRef]
- Taketa, K.; Endo, Y.; Sekiya, C.; Tanikawa, K.; Koji, T.; Taga, H.; Satomura, S.; Matsuura, S.; Kawai, T.; Hirai, H. A collaborative study for the evaluation of lectin-reactive alpha-fetoproteins in early detection of hepatocellular carcinoma. Cancer Res. 1993, 53, 5419–5423. [Google Scholar]
- Ishibashi, K.; Nishikawa, A.; Hayashi, N.; Kasahara, A.; Sato, N.; Fujii, S.; Kamada, T.; Taniguchi, N. N-Acetylglucosaminyltransferase III in human serum, and liver and hepatoma tissues: Increased activity in liver cirrhosis and hepatoma patients. Clin. Chim. Acta 1989, 185, 325–332. [Google Scholar] [CrossRef]
- Mori, S.; Aoyagi, Y.; Yanagi, M.; Suzuki, Y.; Asakura, H. Serum N-acetylglucosaminyltransferase III activities in hepatocellular carcinoma. J. Gastroenterol. Hepatol. 1998, 13, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Fujii, S.; Nishiura, T.; Nishikawa, A.; Miura, R.; Taniguchi, N. Structural heterogeneity of sugar chains in immunoglobulin G. Conformation of immunoglobulin G molecule and substrate specificities of glycosyltransferases. J. Biol. Chem. 1990, 265, 6009–6018. [Google Scholar] [PubMed]
- Theodoratou, E.; Thaçi, K.; Agakov, F.; Timofeeva, M.N.; Štambuk, J.; Pučić-Baković, M.; Vučković, F.; Orchard, P.; Agakova, A.; Din, F.V.N.; et al. Glycosylation of plasma IgG in colorectal cancer prognosis. Sci. Rep. 2016, 6, 28098. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Wang, Y.; Kristic, J.; Dong, J.; Chu, X.; Ge, S.; Wang, H.; Fang, H.; Gao, Q.; Liu, D.; et al. Profiling IgG N-glycans as potential biomarker of chronological and biological ages. Medicine 2016, 95, e4112. [Google Scholar] [CrossRef] [PubMed]
- Lauc, G.; Huffman, J.E.; Pučić, M.; Zgaga, L.; Adamczyk, B.; Mužinić, A.; Novokmet, M.; Polašek, O.; Gornik, O.; Krištić, J.; et al. Loci Associated with N-Glycosylation of Human Immunoglobulin G Show Pleiotropy with Autoimmune Diseases and Haematological Cancers. PLoS Genet. 2013, 9, e1003225. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Serra, P.; Marcilla, M.; Villanueva, A.; Ramos-Fernandez, A.; Palau, A.; Leal, L.; Wahi, J.E.; Setien-Baranda, F.; Szczesna, K.; Moutinho, C.; et al. A DERL3-associated defect in the degradation of SLC2A1 mediates the Warburg effect. Nat. Commun. 2014, 5, 3608. [Google Scholar] [CrossRef] [Green Version]
- Hase, S.; Natsuka, S.; Oku, H.; Ikenaka, T. Identification method for twelve oligomannose-type sugar chains thought to be processing intermediates of glycoproteins. Anal. Biochem. 1987, 167, 321–326. [Google Scholar] [CrossRef]
- Hase, S. [13] High-performance liquid chromatography of pyridylaminated saccharides. Methods Enzymol. 1994, 230, 225–237. [Google Scholar] [CrossRef]
- Fujimoto, I.; Menon, K.K.; Otake, Y.; Tanaka, F.; Wada, H.; Takahashi, H.; Tsuji, S.; Natsuka, S.; Nakakita, S.-I.; Hase, S.; et al. Systematic Analysis ofN-Linked Sugar Chains from Whole Tissue Employing Partial Automation. Anal. Biochem. 1999, 267, 336–343. [Google Scholar] [CrossRef]
- Otake, Y.; Fujimoto, I.; Tanaka, F.; Nakagawa, T.; Ikeda, T.; Menon, K.K.; Hase, S.; Wada, H.; Ikenaka, K. Isolation and characterization of an N-linked oligosaccharide that is significantly increased in sera from patients with non-small cell lung cancer. J. Biochem. 2001, 129, 537–542. [Google Scholar] [CrossRef]
- Ishii, A.; Ikeda, T.; Hitoshi, S.; Fujimoto, I.; Torii, T.; Sakuma, K.; Nakakita, S.-I.; Hase, S.; Ikenaka, K. Developmental changes in the expression of glycogenes and the content of N-glycans in the mouse cerebral cortex. Glycobiology 2007, 17, 261–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimura, T.; Hayashi, A.; Handa-Narumi, M.; Yagi, H.; Ohno, N.; Koike, T.; Yamaguchi, Y.; Uchimura, K.; Kadomatsu, K.; Sedzik, J.; et al. GlcNAc6ST-1 regulates sulfation of N-glycans and myelination in the peripheral nervous system. Sci. Rep. 2017, 7, 42257. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Healthy Control | Hepatitis | Liver Cirrhosis | Liver Cancer | Gastric Cancer | Pancreatic Cancer | Other Gastrointestinal Cancers | Other Gastrointestinal Diseases | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | 71 | 11 | 24 | 76 | 12 | 12 | 15 | 25 | |||
| Etiology (HBV/HCV/other) | 0/7/4 | 3/8/13 | 9/55/12 | ||||||||
| Tumor stage (HBV/HCV/other) | T1 | 2/12/3 | |||||||||
| T2 | 3/18/4 | ||||||||||
| T3 | 1/17/2 | ||||||||||
| T4 | 3/8/3 | ||||||||||
| Age (years) | 44.1 ± 13.1 | 53.6 ± 9.9 | 65.9 ± 9.4 | 72.3 ± 6.5 | 70.8 ± 7.6 | 64.8 ± 11.3 | 67.2 ± 13.3 | 71.1 ± 10.1 | |||
| AST (IU/L) | 20.2 ± 6.3 | 144.0 ± 484.7 | 59.5 ± 40.5 | 76.9 ± 69.6 | 20.0 ± 5.2 | 93.9 ± 140.3 | 48.9 ± 51.6 | 32.4 ± 29.0 | |||
| ALT (IU/L) | 18.5 ± 14.2 | 103.3 ± 248.9 | 36.4 ± 21.5 | 55.5 ± 63.1 | 19.9 ± 8.0 | 182.6 ± 272.5 | 58.9 ± 101.7 | 30.6 ± 46.5 | |||
| Albumin (g/dL) | 4.5 ± 0.2 | 4.2 ± 0.5 | 3.2 ± 0.6 | 3.1 ± 0.6 | 4.1 ± 0.3 | 3.6 ± 0.3 | 3.5 ± 0.1 | 3.7 ± 0.7 | |||
| Total serum protein (g/dL) | 7.1 ± 0.3 | 7.1 ± 0.5 | 7.2 ± 0.6 | 6.9 ± 0.8 | 6.7 ± 0.6 | 6.5 ± 0.7 | 6.6 ± 0.8 | 6.4 ± 0.5 | |||
| Total bilirubin (mg/dL) | 1.0 ± 0.4 | 0.9 ± 0.3 | 2.3 ± 2.2 | 1.7 ± 1.8 | 0.5 ± 0.2 | 3.8 ± 4.6 | 2.4 ± 4.0 | 1.5 ± 2.7 | |||
| AFP (ng/mL) | 11.5 ± 8.1 | 12.0 ± 16.0 | 18,202.7 ± 73,224.8 | ||||||||
| PIVKA-II (mAU/mL) | 30.7 ± 23.3 | 172.9 ± 417.3 | 3692.4 ± 12,058.9 | ||||||||
| CEA (ng/mL) | 3.2 ± 1.2 | 4.2 ± 3.2 | 23.2 ± 59.0 | ||||||||
| CA19-9 (U/mL) | 165.9 ± 441.3 | 5987.2 ± 14,636.8 | 18,955.0 ± 55,958.0 | ||||||||
| N-glycan (type) | Healthy control | Hepatitis | Liver cirrhosis | Liver cancer | Gastric cancer | Pancreatic cancer | Other gastrointestinal cancers | Other gastrointestinal diseases | |||
| A2G0 (neutral) | 0.033 ± 0.017 | HBV | n.d. | 0.227 ± 0.148 | 0.180 ± 0.100 | 0.096 ± 0.070 | 0.103 ± 0.061 | 0.115 ± 0.084 | 0.119 ± 0.104 | ||
| HCV | 0.065 ± 0.037 | 0.090 ± 0.068 | 0.214 ± 0.126 | ||||||||
| other | 0.077 ± 0.014 | 0.220 ± 0.118 | 0.209 ± 0.136 | ||||||||
| M5A (neutral) | 0.193± 0.063 | HBV | n.d. | 0.512 ± 0.148 | 0.541 ± 0.201 | 0.360 ± 0.104 | 0.324 ± 0.130 | 0.416 ± 0.199 | 0.273 ± 0.145 | ||
| HCV | 0.265 ± 0.090 | 0.216 ± 0.113 | 0.507 ± 0.128 | ||||||||
| other | 0.313 ± 0.066 | 0.597 ± 0.264 | 0.413 ± 0.106 | ||||||||
| A2G0B (neutral) | 0.060 ± 0.022 | HBV | n.d. | 0.565 ± 0.326 | 0.363 ± 0.196 | 0.157 ± 0.077 | 0.180 ± 0.102 | 0.224 ± 0.156 | 0.149 ± 0.137 | ||
| HCV | 0.129 ± 0.034 | 0.131 ± 0.114 | 0.374 ± 0.176 | ||||||||
| other | 0.147 ± 0.027 | 0.739 ± 0.342 | 0.351 ± 0.207 | ||||||||
| A2G1(6)FB (neutral) | 0.112 ± 0.047 | HBV | n.d. | 0.562 ± 0.288 | 0.459 ± 0.256 | 0.299 ± 0.200 | 0.211 ± 0.121 | 0.275 ± 0.186 | 0.223 ± 0.151 | ||
| HCV | 0.175 ± 0.087 | 0.210 ± 0.068 | 0.489 ± 0.176 | ||||||||
| other | 0.236 ± 0.093 | 0.538 ± 0.238 | 0.521 ± 0.208 | ||||||||
| A2G2B (neutral) | 0.025 ± 0.011 | HBV | n.d. | 0.049 ± 0.009 | 0.057 ± 0.016 | 0.053 ± 0.025 | 0.034 ± 0.017 | 0.046 ± 0.027 | 0.033 ± 0.018 | ||
| HCV | 0.031 ± 0.018 | 0.024 ± 0.012 | 0.058 ± 0.023 | ||||||||
| other | 0.037± 0.002 | 0.054± 0.010 | 0.043± 0.012 | ||||||||
| A2G2Fo2 (neutral+asialo) | 0.056 ± 0.031 | HBV | n.d. | 0.254 ± 0.109 | 0.251 ± 0.182 | 0.134 ± 0.082 | 0.228 ± 0.142 | 0.206 ± 0.265 | 0.230 ± 0.082 | ||
| HCV | 0.169 ± 0.204 | 0.084 ± 0.039 | 0.231 ± 0.137 | ||||||||
| other | 0.370 ± 0.082 | 0.281 ± 0.115 | 0.209 ± 0.147 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higashi, M.; Yoshimura, T.; Usui, N.; Kano, Y.; Deguchi, A.; Tanabe, K.; Uchimura, Y.; Kuriyama, S.; Suzuki, Y.; Masaki, T.; et al. A Potential Serum N-glycan Biomarker for Hepatitis C Virus-Related Early-Stage Hepatocellular Carcinoma with Liver Cirrhosis. Int. J. Mol. Sci. 2020, 21, 8913. https://doi.org/10.3390/ijms21238913
Higashi M, Yoshimura T, Usui N, Kano Y, Deguchi A, Tanabe K, Uchimura Y, Kuriyama S, Suzuki Y, Masaki T, et al. A Potential Serum N-glycan Biomarker for Hepatitis C Virus-Related Early-Stage Hepatocellular Carcinoma with Liver Cirrhosis. International Journal of Molecular Sciences. 2020; 21(23):8913. https://doi.org/10.3390/ijms21238913
Chicago/Turabian StyleHigashi, Mikito, Takeshi Yoshimura, Noriyoshi Usui, Yuichiro Kano, Akihiro Deguchi, Kazuhiro Tanabe, Youichi Uchimura, Shigeki Kuriyama, Yasuyuki Suzuki, Tsutomu Masaki, and et al. 2020. "A Potential Serum N-glycan Biomarker for Hepatitis C Virus-Related Early-Stage Hepatocellular Carcinoma with Liver Cirrhosis" International Journal of Molecular Sciences 21, no. 23: 8913. https://doi.org/10.3390/ijms21238913