Robotic Stereotactic Radiosurgery in Melanoma Patients with Brain Metastases under Simultaneous Anti-PD-1 Treatment

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient and Lesion Characteristics
2.2. Toxicity
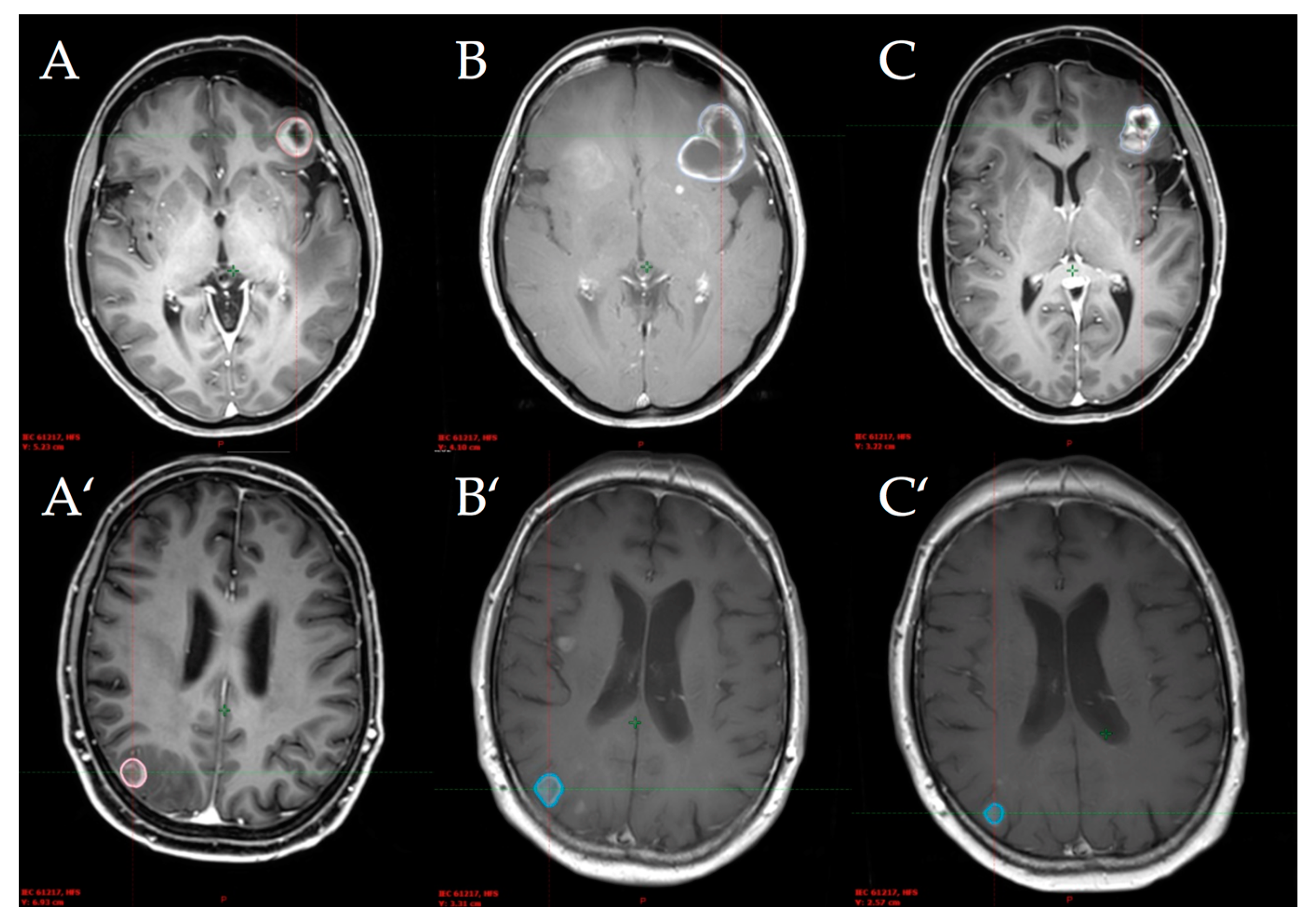
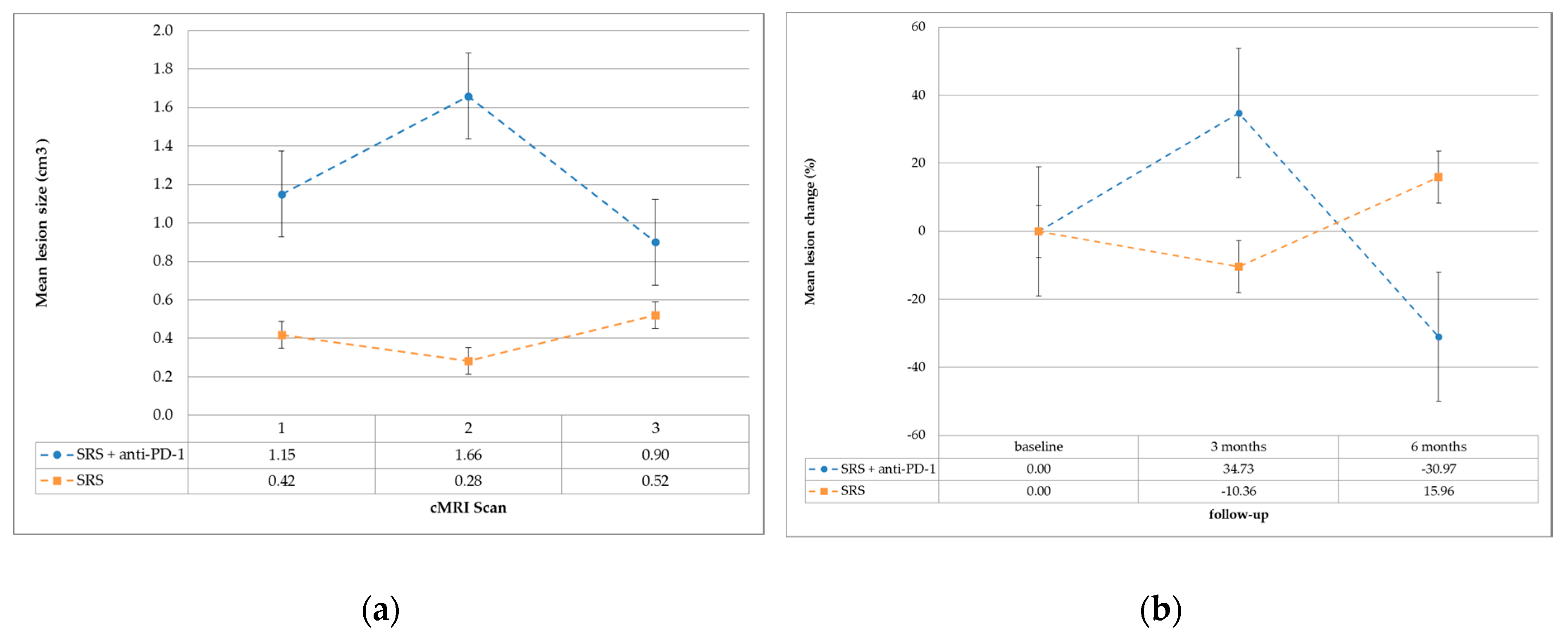
2.3. Local Tumor Control and Efficacy Analyses
3. Discussion
3.1. Response Rate
3.2. Toxicity
4. Materials and Methods
4.1. Patients
4.2. Immunotherapy
4.3. Robotic Stereotactic Radiosurgery (SRS) with Cyberknife®
4.4. Follow-Up
4.5. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SRS | stereotactic radiosurgery |
| PD-1 | programmed death 1 |
| MM | malignant melanoma |
| BM | brain metastases |
| PD-L1 | programmed death ligand 1 |
| PsP | pseudoprogression |
| ECOG | Eastern Cooperative Oncology Group performance status |
| cMRI | cranial magnetic resonance imaging |
| CTCAE | Common Terminology Criteria for Adverse Events |
| CT | computed tomography |
| GTV | gross tumor volume |
| OAR | organs at risk |
| ICP | intracranial pressure |
References
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Sloan, A.E.; Nock, C.J.; Einstein, D.B. Diagnosis and treatment of melanoma brain metastasis: A literature review. Cancer Control 2009, 16, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, J.C.; Jilaveanu, L.B.; Faries, M.; Sznol, M.; Ariyan, S.; Yu, J.B.; Knisely, J.P.S.; Chiang, V.L.; Kluger, H.M. Melanoma brain metastases: Is it time to reassess the bias? Curr. Probl. Cancer 2011, 35, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Tas, F. Metastatic behavior in melanoma: Timing, pattern, survival, and influencing factors. J. Oncol. 2012, 2012, 647684. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Atkinson, V.; Menzies, A.M.; Guminski, A.D.; Sandhu, S.K.; Brown, M.P.; Liaw, T.; Gonzalez, M.; Davison, J.; Paton, E.J.; et al. A randomized phase 2 study of nivolumab and nivolumab combined with ipilimumab in patients (pts) with melanoma brain metastases: The Anti-PD1 Brain Collaboration (ABC Study). J. Clin. Oncol. 2016, 34, TPS9591. [Google Scholar] [CrossRef]
- Tawbi, H.A.-H.; Forsyth, P.A.J.; Algazi, A.P.; Hamid, O.; Hodi, F.S.; Moschos, S.J.; Khushalani, N.I.; Gonzalez, R.; Lao, C.D.; Postow, M.A.; et al. Efficacy and safety of nivolumab (NIVO) plus ipilimumab (IPI) in patients with melanoma (MEL) metastatic to the brain: Results of the phase II study CheckMate 204. J. Clin. Oncol. 2017, 35, 9507. [Google Scholar] [CrossRef]
- Staudt, M.; Lasithiotakis, K.; Leiter, U.; Meier, F.; Eigentler, T.; Bamberg, M.; Tatagiba, M.; Brossart, P.; Garbe, C. Determinants of survival in patients with brain metastases from cutaneous melanoma. Br. J. Cancer 2010, 102, 1213–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.-D.; Carrie, C.; et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: Results of the EORTC 22952-26001 study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs. stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Selek, U.; Chang, E.L.; Hassenbusch, S.J.; Shiu, A.S.; Lang, F.F.; Allen, P.; Weinberg, J.; Sawaya, R.; Maor, M.H. Stereotactic radiosurgical treatment in 103 patients for 153 cerebral melanoma metastases. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Theurich, S.; Rothschild, S.I.; Hoffmann, M.; Fabri, M.; Sommer, A.; Garcia-Marquez, M.; Thelen, M.; Schill, C.; Merki, R.; Schmid, T.; et al. Local Tumor Treatment in Combination with Systemic Ipilimumab Immunotherapy Prolongs Overall Survival in Patients with Advanced Malignant Melanoma. Cancer Immunol. Res. 2016, 4, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Koller, K.M.; Mackley, H.B.; Liu, J.; Wagner, H.; Talamo, G.; Schell, T.D.; Pameijer, C.; Neves, R.I.; Anderson, B.; Kokolus, K.M.; et al. Improved survival and complete response rates in patients with advanced melanoma treated with concurrent ipilimumab and radiotherapy versus ipilimumab alone. Cancer Biol. Ther. 2016, 18, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.-X. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Investig. 2014, 124, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.M.; Yu, J.B.; Kluger, H.M.; Chiang, V.L.S. Timing and type of immune checkpoint therapy affect the early radiographic response of melanoma brain metastases to stereotactic radiosurgery. Cancer 2016, 122, 3051–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, T.R.; McHugh, B.J.; Bi, W.L.; Minja, F.J.; Knisely, J.P.S.; Chiang, V.L. A Comprehensive Review of MR Imaging Changes following Radiosurgery to 500 Brain Metastases. Am. J. Neuroradiol. 2011, 32, 1885–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruzevick, J.; Kleinberg, L.; Rigamonti, D. Imaging changes following stereotactic radiosurgery for metastatic intracranial tumors: Differentiating pseudoprogression from tumor progression and its effect on clinical practice. Neurosurg. Rev. 2013, 37, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Kocher, M.; Langen, K.-J. Pseudoprogression after glioma therapy: An update. Expert Rev. Neurother. 2017, 17, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Parvez, K.; Parvez, A.; Zadeh, G. The diagnosis and treatment of pseudoprogression, radiation necrosis and brain tumor recurrence. Int. J. Mol. Sci. 2014, 15, 11832–11846. [Google Scholar] [CrossRef] [PubMed]
- Chiou, V.L.; Burotto, M. Pseudoprogression and Immune-Related Response in Solid Tumors. J. Clin. Oncol. 2015, 33, 3541–3543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taube, J.M.; Anders, R.A.; Young, G.D.; Xu, H.; Sharma, R.; McMiller, T.L.; Chen, S.; Klein, A.P.; Pardoll, D.M.; Topalian, S.L.; et al. Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci. Transl. Med. 2012, 4, 127ra37. [Google Scholar] [CrossRef] [PubMed]
- Haikerwal, S.J.; Hagekyriakou, J.; MacManus, M.; Martin, O.A.; Haynes, N.M. Building immunity to cancer with radiation therapy. Cancer Lett. 2015, 368, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Dewey, W.C.; Ling, C.C.; Meyn, R.E. Radiation-induced apoptosis: Relevance to radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 781–796. [Google Scholar] [CrossRef]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Radiation therapy to convert the tumor into an in situ vaccine. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 879–880. [Google Scholar] [CrossRef] [PubMed]
- Sauter, B.; Albert, M.L.; Francisco, L.; Larsson, M.; Somersan, S.; Bhardwaj, N. Consequences of cell death: Exposure to necrotic tumor cells, but not primary tissue cells or apoptotic cells, induces the maturation of immunostimulatory dendritic cells. J. Exp. Med. 2000, 191, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Bhardwaj, N.; McBride, W.H.; Formenti, S.C. Combining radiotherapy and immunotherapy: A revived partnership. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 655–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.S.; Dong, H.; Liu, X.; Harrington, S.M.; Krco, C.J.; Grams, M.P.; Mansfield, A.S.; Furutani, K.M.; Olivier, K.R.; Kwon, E.D. PD-1 Restrains Radiotherapy-Induced Abscopal Effect. Cancer Immunol. Res. 2015, 3, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, K.A.; Abuodeh, Y.A.; Echevarria, M.I.; Arrington, J.A.; Stallworth, D.G.; Hogue, C.; Naghavi, A.O.; Kim, S.; Kim, Y.; Patel, B.G.; et al. Clinical outcomes of melanoma brain metastases treated with stereotactic radiosurgery and anti-PD-1 therapy, anti-CTLA-4 therapy, BRAF/MEK inhibitors, BRAF inhibitor, or conventional chemotherapy. Ann. Oncol. 2016, 27, 2288–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, K.A.; Stallworth, D.G.; Kim, Y.; Johnstone, P.A.S.; Harrison, L.B.; Caudell, J.J.; Yu, H.H.M.; Etame, A.B.; Weber, J.S.; Gibney, G.T. Clinical outcomes of melanoma brain metastases treated with stereotactic radiation and anti-PD-1 therapy. Ann. Oncol. 2016, 27, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Liniker, E.; Menzies, A.M.; Kong, B.Y.; Cooper, A.; Ramanujam, S.; Lo, S.; Kefford, R.F.; Fogarty, G.B.; Guminski, A.; Wang, T.W.; et al. Activity and safety of radiotherapy with anti-PD-1 drug therapy in patients with metastatic melanoma. Oncoimmunology 2016, 5, e1214788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, K.A.; Kim, S.; Arrington, J.; Naghavi, A.O.; Dilling, T.J.; Creelan, B.C.; Antonia, S.J.; Caudell, J.J.; Harrison, L.B.; Sahebjam, S.; et al. Outcomes targeting the PD-1/PD-L1 axis in conjunction with stereotactic radiation for patients with non-small cell lung cancer brain metastases. J. Neurooncol. 2017, 133, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, M.B.; Amsbaugh, M.J.; Burton, E.; Chesney, J.; Woo, S. Peri-SRS Administration of Immune Checkpoint Therapy for Melanoma Metastatic to the Brain: Investigating Efficacy and the Effects of Relative Treatment Timing on Lesion Response. World Neurosurg. 2017, 100, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Parakh, S.; Park, J.J.; Mendis, S.; Rai, R.; Xu, W.; Lo, S.; Drummond, M.; Rowe, C.; Wong, A.; McArthur, G.; et al. Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases. Br. J. Cancer 2017, 116, 1558–1563. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.S.; Postow, M.A.; Wolchok, J.D.; Young, R.J.; Ballangrud, Å.; Chan, T.A.; Yamada, Y.; Beal, K. Melanoma brain metastases treated with stereotactic radiosurgery and concurrent pembrolizumab display marked regression; efficacy and safety of combined treatment. J. Immunother. Cancer 2017, 5, 76. [Google Scholar] [CrossRef] [PubMed]
- Da Cruz, L.C.H.; Rodriguez, I.; Domingues, R.C.; Gasparetto, E.L.; Sorensen, A.G. Pseudoprogression and Pseudoresponse: Imaging Challenges in the Assessment of Posttreatment Glioma. Am. J. Neuroradiol. 2011, 32, 1978–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, J.; Born, D.; Chamberlain, M.C. Radiation Necrosis: Relevance with Respect to Treatment of Primary and Secondary Brain Tumors. Curr. Neurol. Neurosci. Rep. 2012, 12, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Rauch, P.J.; Park, H.S.; Knisely, J.P.S.; Chiang, V.L.; Vortmeyer, A.O. Delayed Radiation-Induced Vasculitic Leukoencephalopathy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.V.; Alomari, A.K.; Vortmeyer, A.O.; Jilaveanu, L.B.; Goldberg, S.B.; Mahajan, A.; Chiang, V.L.; Kluger, H.M. Melanoma Brain Metastasis Pseudoprogression after Pembrolizumab Treatment. Cancer Immunol. Res. 2016, 4, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; Hodi, F.S.; Wolchok, J.D.; Topalian, S.L.; Schadendorf, D.; Larkin, J.; Sznol, M.; Long, G.V.; Li, H.; Waxman, I.M.; et al. Safety Profile of Nivolumab Monotherapy: A Pooled Analysis of Patients with Advanced Melanoma. J. Clin. Oncol. 2017, 35, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Daskivich, T.J.; Belldegrun, A. Re: Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer. Eur. Urol. 2015, 67, 816–817. [Google Scholar] [CrossRef] [PubMed]
- Menzies, A.M.; Johnson, D.B.; Ramanujam, S.; Atkinson, V.G.; Wong, A.N.M.; Park, J.J.; McQuade, J.L.; Shoushtari, A.N.; Tsai, K.K.; Eroglu, Z.; et al. Anti-PD-1 therapy in patients with advanced melanoma and preexisting autoimmune disorders or major toxicity with ipilimumab. Ann. Oncol. 2017, 28, 368–376. [Google Scholar] [PubMed]
- Lin, N.U.; Lee, E.Q.; Aoyama, H.; Barani, I.J.; Barboriak, D.P.; Baumert, B.G.; Bendszus, M.; Brown, P.D.; Camidge, D.R.; Chang, S.M.; et al. Response Assessment in Neuro-Oncology (RANO) group Response assessment criteria for brain metastases: Proposal from the RANO group. Lancet Oncol. 2015, 16, e270–e278. [Google Scholar] [CrossRef]
- Patel, K.R.; Shoukat, S.; Oliver, D.E.; Chowdhary, M.; Rizzo, M.; Lawson, D.H.; Khosa, F.; Liu, Y.; Khan, M.K. Ipilimumab and Stereotactic Radiosurgery Versus Stereotactic Radiosurgery Alone for Newly Diagnosed Melanoma Brain Metastases. Am. J. Clin. Oncol. 2017, 40, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Huber, P.E.; Hawighorst, H.; Fuss, M.; van Kaick, G.; Wannenmacher, M.F.; Debus, J. Transient enlargement of contrast uptake on MRI after linear accelerator (linac) stereotactic radiosurgery for brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1339–1349. [Google Scholar] [CrossRef]
- Alomari, A.; Rauch, P.J.; Orsaria, M.; Minja, F.J.; Chiang, V.L.; Vortmeyer, A.O. Radiologic and histologic consequences of radiosurgery for brain tumors. J. Neurooncol. 2014, 117, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Dunkl, V.; Stoffels, G.; Hutterer, M.; Rapp, M.; Sabel, M.; Reifenberger, G.; Kebir, S.; Dorn, F.; Blau, T.; et al. Diagnosis of pseudoprogression in patients with glioblastoma using O-(2-[18F]fluoroethyl)-l-tyrosine PET. Eur. J. Nucl. Med. Mol. Imaging 2014, 42, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Stoffels, G.; Filss, C.; Rapp, M.; Blau, T.; Tscherpel, C.; Ceccon, G.; Dunkl, V.; Weinzierl, M.; Stoffel, M.; et al. The use of dynamic O-(2-18F-fluoroethyl)-l-tyrosine PET in the diagnosis of patients with progressive and recurrent glioma. Neuro Oncol. 2015, 17, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | All Patients | SRS + Anti-PD-1 | SRS | p-Value | |
|---|---|---|---|---|---|
| Patients n | 26 | 13 | 13 | ||
| Age (y) at SRS-treatment | median (IQR) | 57 (32.5) | 52 (27) | 64 (31) | 0.314 |
| range | 33–84 | 36–81 | 33–84 | ||
| Gender | male (% of pts.) | 14 (54) | 6 (46) | 8 (62) | 0.431 |
| female (% of pts.) | 12 (46) | 7 (54) | 5 (38) | ||
| ECOG | 0 (% of pts.) | 4 (15) | 2 (15) | 2 (15) | 0.18 |
| 1 (% of pts.) | 18 (69) | 7 (54) | 11 (85) | ||
| 2 (% of pts.) | 4 (15) | 4 (31) | 0 | ||
| Mutations | BRAF (% of pts.) | 18 (69) | 8 (62) | 10 (77) | 0.317 |
| NRAS (% of pts.) | 6 (23) | 5 (38) | 1 (8) | 0.155 | |
| c-KIT (% of pts.) | 2 (8) | 1 (8) | 1 (8) | 1 | |
| Metastases | 1 other location than brain (% of pts.) | 5 (19) | 2 (15) | 3 (23) | |
| 2 other locations than brain (% of pts.) | 13 (50) | 8 (62) | 5 (38) | 0.584 | |
| >2 other locations than brain (% of pts.) | 8 (31) | 3 (23) | 5 (38) | ||
| Prior systemic therapy | B-Raf inhibitor | 11 | 3 | 8 | |
| MEK inhibitor | 5 | 3 | 2 | ||
| TK-/RTK-inhibitor | 2 | 0 | 2 | ||
| chemotherapy | 10 | 4 | 6 | ||
| interferon | 2 | 2 | 0 | ||
| ipilimumab | 10 | 6 | 4 | ||
| none | 9 | 5 | 4 | ||
| Type of PD-1 inhibitor | pembrolizumab (% of pts.) | 10 (38) | 10 (77) | - | |
| nivolumab (% of pts.) | 2(12) | 3 (23) | - | ||
| Interval Diagnosis SRS (m) | median (IQR) | 33.5 (33.3) | 29 (29) | 45 (45) | 0.724 |
| range | 1–204 | 1–129 | 4–204 | ||
| Characteristic | All Patients | SRS + Anti-PD-1 | SRS | p-Value | |
|---|---|---|---|---|---|
| Patients n (%) | 26 | 13 (50) | 13 (50) | ||
| Lesions n (%) | 48 | 28 (58) | 20 (42) | ||
| Lesions treated per patient | median (IQR) | 1.5 (2) | 2 (2) | 1 (1) | 0.555 |
| range | 1–5 | 1–5 | 1–3 | ||
| GTV in cm3—baseline | median (IQR) | 0.3 (0.95) | 0.55 (1.23) | 0.1 (0.38) | 0.033 |
| range | 0.01–7.4 | 0.01–7.4 | 0.01–2.7 | ||
| Dose in Gy, 65% isodose level | range | 18–22 | 18–20 | 18–22 | 1 |
| Outcome | |||||
| GTV in cm3—1st follow-up | median (IQR) | 0.2 (0.57) | 0.2 (1.14) | 0.2 (0.34) | 0.561 |
| range | 0.0–17.8 | 0.0–17.8 | 0.0–1.5 | ||
| 1st follow-up vs. baseline | regression (% of les.) | 16 (33) | 12 (43) | 4 (20) | 0.028 |
| stable (% of les.) | 25 (52) | 10 (36) | 15 (75) | ||
| progression (% of les.) | 7 (15) | 6 (21) | 1 (5) | ||
| GTV in cm3—2nd follow-up | median (IQR) | 0.06 (0.4) | 0.06 (0.37) | 0.06 (0.93) | 0.551 |
| range | 0.0–6.4 | 0.0–6.4 | 0.0–2.4 | ||
| 2nd follow-up vs. baseline | regression (% of les.) | 20 (42) | 17 (61) | 3 (15) | 0.005 |
| stable (% of les.) | 20 (42) | 7 (25) | 13 (65) | ||
| progression (% of les.) | 8 (17) | 4 (14) | 4 (20) | ||
| 2nd follow-up | pseudoprogression (% of les.) | 4 (8) | 4 (14) | 0 | 0.13 |
| Characteristic | SRS + Anti-PD1 (n = 13) | SRS (n = 13) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Grade 0–1 | Grade 2 | All Grades | Grade 0–1 | Grade 2 | All Grades | |||
| Any Toxicity (pts.) | 10 | 7 | 0.411 | |||||
| Symptoms of ICP (pts.) | 8 | 5 | 0.239 | |||||
| headache | 4 | 2 | (6) | 3 | 0 | (3) | 0.352 | |
| nausea | 1 | 1 | (2) | 1 | 0 | (1) | 1 | |
| vertigo | 3 | 1 | (4) | 2 | 0 | (2) | 0.645 | |
| Fatigue (pts.) | 3 | 1 | (4) | 2 | 1 | (3) | 1 | |
| Thyroid disorder (pts.) | 6 | 3 | 0.411 | |||||
| new | 2 | 2 | (4) | 0 | 0 | (0) | 0.096 | |
| known | 0 | 2 | (2) | 2 | 1 | (3) | 0.593 | |
| Gastroenterological symptoms (pts.) | 2 | 3 | 1 | |||||
| colitis | 0 | 2 | (2) | 0 | 0 | (0) | 0.48 | |
| unspecific | 0 | 0 | (0) | 3 | 0 | (3) | 0.22 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trommer-Nestler, M.; Marnitz, S.; Kocher, M.; Rueß, D.; Schlaak, M.; Theurich, S.; Von Bergwelt-Baildon, M.; Morgenthaler, J.; Jablonska, K.; Celik, E.; et al. Robotic Stereotactic Radiosurgery in Melanoma Patients with Brain Metastases under Simultaneous Anti-PD-1 Treatment. Int. J. Mol. Sci. 2018, 19, 2653. https://doi.org/10.3390/ijms19092653
Trommer-Nestler M, Marnitz S, Kocher M, Rueß D, Schlaak M, Theurich S, Von Bergwelt-Baildon M, Morgenthaler J, Jablonska K, Celik E, et al. Robotic Stereotactic Radiosurgery in Melanoma Patients with Brain Metastases under Simultaneous Anti-PD-1 Treatment. International Journal of Molecular Sciences. 2018; 19(9):2653. https://doi.org/10.3390/ijms19092653
Chicago/Turabian StyleTrommer-Nestler, Maike, Simone Marnitz, Martin Kocher, Daniel Rueß, Max Schlaak, Sebastian Theurich, Michael Von Bergwelt-Baildon, Janis Morgenthaler, Karolina Jablonska, Eren Celik, and et al. 2018. "Robotic Stereotactic Radiosurgery in Melanoma Patients with Brain Metastases under Simultaneous Anti-PD-1 Treatment" International Journal of Molecular Sciences 19, no. 9: 2653. https://doi.org/10.3390/ijms19092653