Receptor Activator of Nuclear Factor Kappa B (RANK) and Clinicopathological Variables in Endometrial Cancer: A Study at Protein and Gene Level

 ,
,
Abstract
:1. Background
2. Results
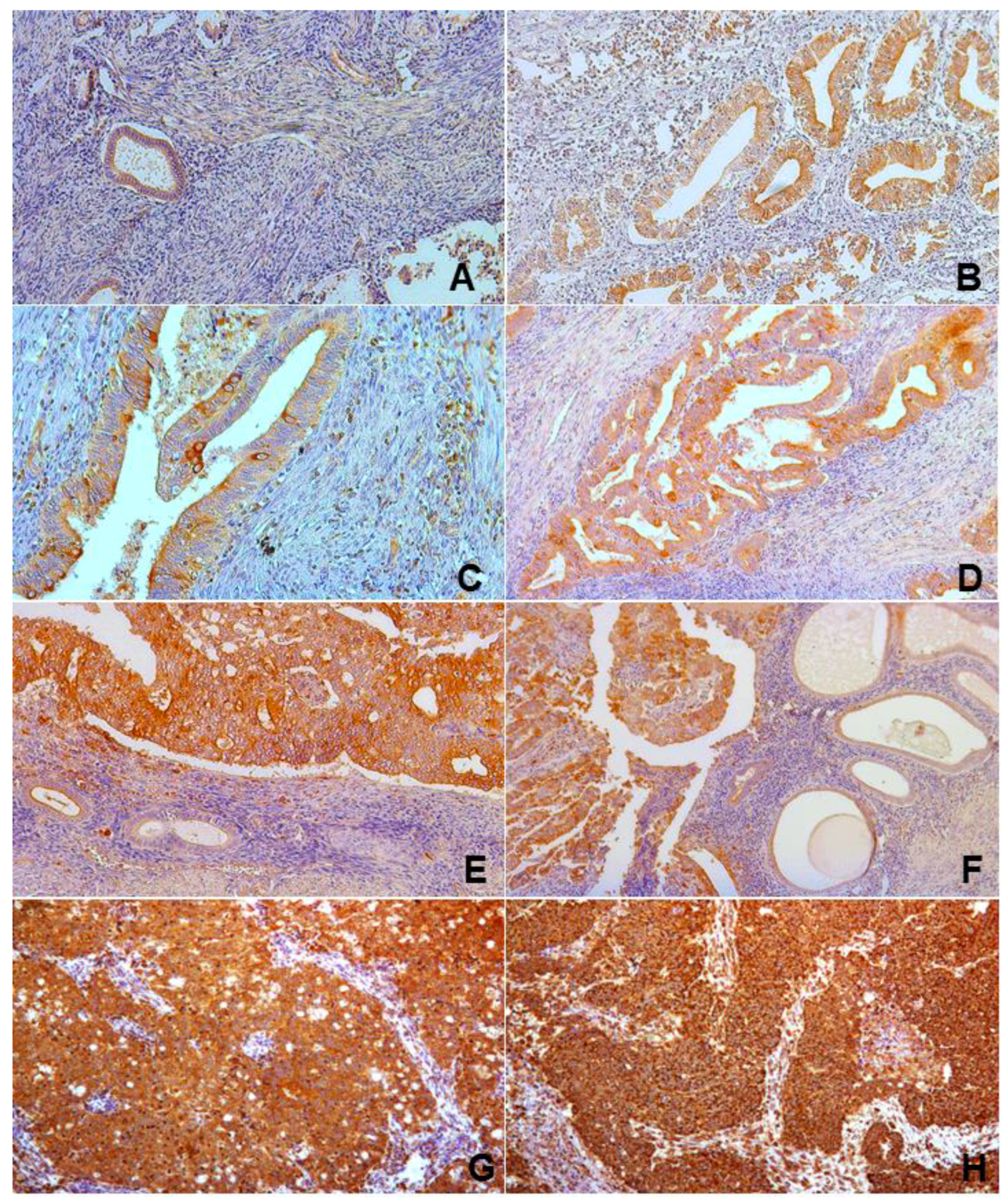
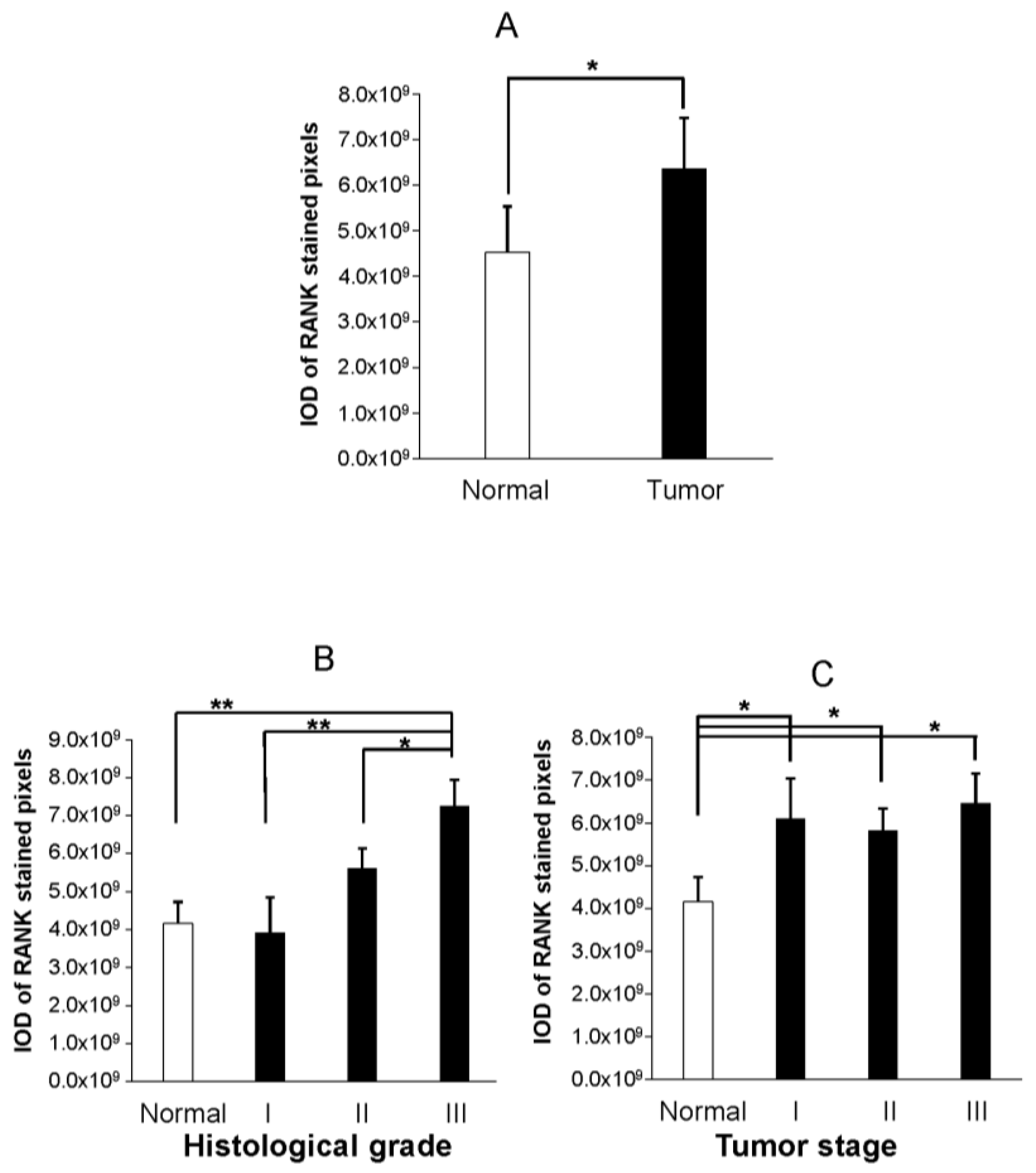
2.1. Immunohistochemical Analyses
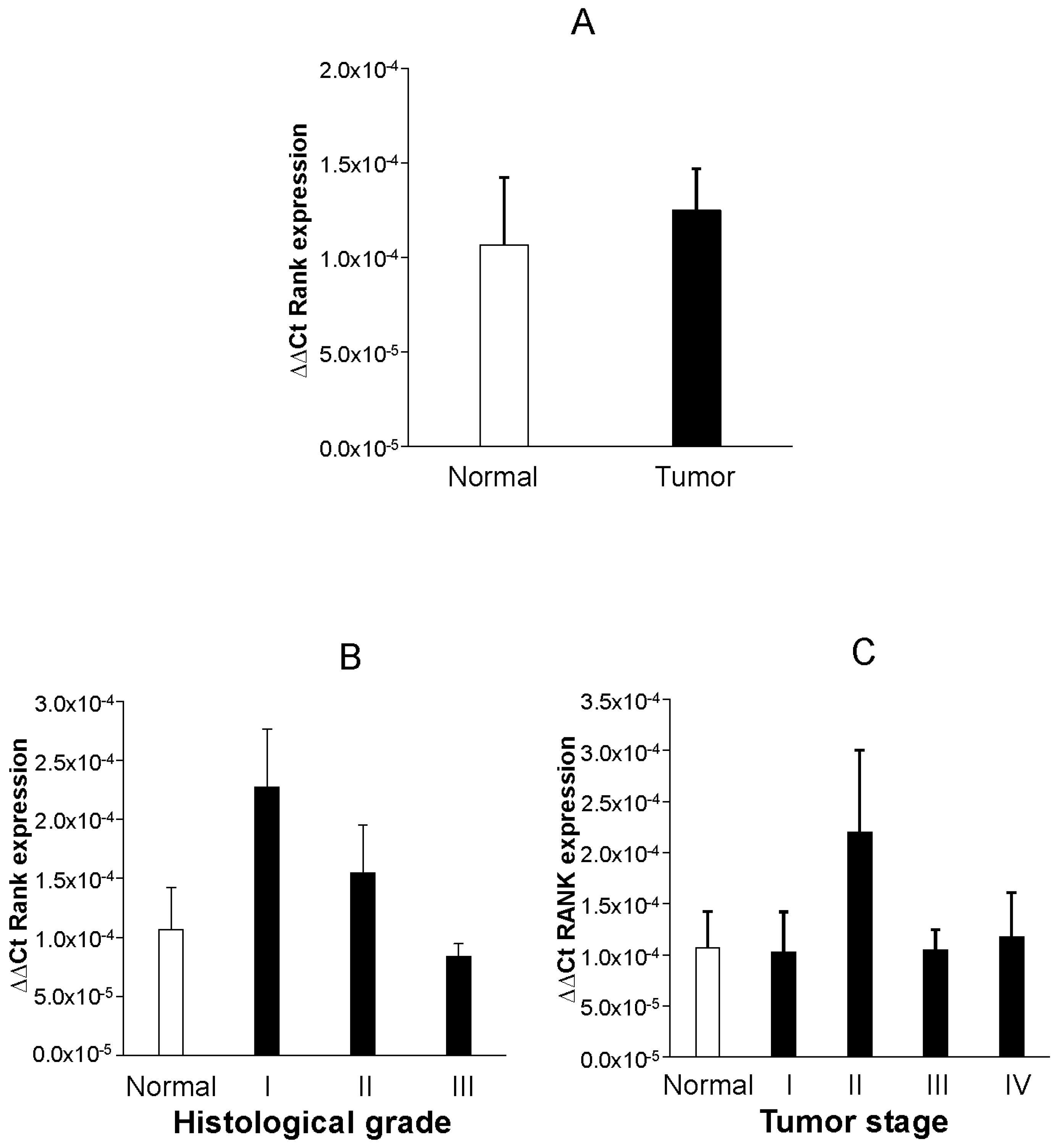
2.2. PCR Analyses
3. Discussion
4. Methods
4.1. Tissue Samples and Experimental Design
4.2. IHC Detection of RANK in TMA
4.3. Quantification of IHC RANK Signalling in TMA
4.4. QF-PCR Amplification and RANK and Quantitative Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Setiawan, V.; Yang, H.; Pike, M.; McCann, S.; Yu, H.; Xiang, Y.B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II endometrial cancers: Have they different risk factors? J. Clin. Oncol. 2013, 31, 2607–2618. [Google Scholar] [CrossRef] [PubMed]
- Brinton, L.; Trabert, B.; Anderson, G.; Falk, R.; Felix, A.; Fuhrman, B.; Gass, M.L.; Kuller, L.H.; Pfeiffer, R.M.; Rohan, T.E.; et al. Serum Estrogens and Estrogen Metabolites and Endometrial Cancer Risk among Postmenopausal Women. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.; Hankinson, S. Endogenous estrogens and the risk of breast, endometrial, and ovarian cancers. Steroids 2015, 99, 8–10. [Google Scholar] [CrossRef] [PubMed]
- González Ricarte, M.; de Castro Pérez, A.; Tarín, J.J.; Cano, A. Progestogens and risk of breast cancer: A link between bone and breast? Gynecol. Endocrinol. 2016, 32, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Hanada, R.; Hanada, T.; Penninger, J.M. Physiology and pathophysiology of the RANKL/RANK system. Biol. Chem. 2010, 391, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- González-Suárez, E.; Sanz-Moreno, A. RANK as a therapeutic target in cancer. FEBS J. 2016, 283, 2018–2033. [Google Scholar] [CrossRef] [PubMed]
- Nolan, E.; Vaillant, F.; Branstetter, D.; Pal, B.; Giner, G.; Whitehead, L.; Lok, S.W.; Rohrbach, K.; Huang, L.Y.; Soriano, R.; et al. RANK ligand as a potential target for breast cancer prevention in BRCA1-mutation carriers. Nat. Med. 2016, 22, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Pfitzner, B.M.; Branstetter, D.; Loibl, S.; Denkert, C.; Lederer, B.; Schmitt, W.D.; Dombrowski, F.; Werner, M.; Rüdiger, T.; Dougall, W.C.; et al. RANK expression as a prognostic and predictive marker in breast cancer. Breast Cancer Res. Treat. 2014, 145, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Lee, A.; Chae, B.J.; Bae, J.S.; Song, B.J.; Jung, S.S. Expression of receptor activator of nuclear factor kappa-B as a poor prognostic marker in breast cancer. J. Surg. Oncol. 2014, 110, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, Y.; Wang, L.; Sun, X.; Wang, Y. Clinical prognostic significance and pro-metastatic activity of RANK/RANKL via the AKT pathway in endometrial cancer. Oncotarget 2016, 7, 5564–5575. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, J.; Ni, T.; Wang, L.; Wang, Y.; Sun, X. CCL20 mediates RANK/RANKL-induced epithelial-mesenchymal transition in endometrial cancer cells. Oncotarget 2016, 7, 25328–25339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Sun, X.; Zhang, H.; Wang, Y.; Li, Y. MPA influences tumour cell proliferation, migration, and invasion induced by RANKL through PRB involving the MAPK pathway in endometrial cancer. Oncol. Rep. 2015, 33, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Santini, D.; Schiavon, G.; Vincenzi, B.; Gaeta, L.; Pantano, F.; Russo, A.; Ortega, C.; Porta, C.; Galluzzo, S.; Armento, G.; et al. Receptor activator of NF-Kb (RANK) expression in primary tumours associates with bone metastasis occurrence in breast cancer patients. PLoS ONE 2011, 6, e19234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, S.; Ye, L.; Sanders, A.J.; Mason, M.D.; Jiang, W.G. Expression profile of receptor activator of nuclear-κB (RANK), RANK ligand (RANKL) and osteoprotegerin (OPG) in breast cancer. Anticancer Res. 2013, 33, 199–206. [Google Scholar] [PubMed]
- Yoldi, G.; Pellegrini, P.; Trinidad, E.M.; Cordero, A.; Gomez-Miragaya, J.; Serra-Musach, J.; Dougall, W.C.; Muñoz, P.; Pujana, M.A.; Planelles, L.; et al. RANK Signaling Blockade Reduces Breast Cancer Recurrence by Inducing Tumour Cell Differentiation. Cancer Res. 2016, 76, 5857–5869. [Google Scholar] [CrossRef] [PubMed]
- Sigl, V.; Jones, L.P.; Penninger, J.M. RANKL/RANK: From bone loss to the prevention of breast cancer. Open Biol. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Study of Denosumab as Adjuvant Treatment for Women with High Risk Early Breast Cancer Receiving Neoadjuvant or Adjuvant Therapy (D-CARE). Available online: http://clinicaltrials.gov/show/NCT01077154 (accessed on 16 March 2018).
- Gómez, R.; Abad, A.; Delgado, F.; Tamarit, S.; Simón, C.; Pellicer, A. Effects of hyperprolactinemia treatment with the dopamine agonist quinagolide on endometriotic lesions in patients with endometriosis-associated hyperprolactinemia. Fertil. Steril. 2011, 95, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Gómez, R.; Simón, C.; Remohí, J.; Pellicer, A. Vascular endothelial growth factor receptor-2 activation induces vascular permeability in hyperstimulated rats, and this effect is prevented by receptor blockade. Endocrinology 2002, 143, 4339–4348. [Google Scholar] [CrossRef] [PubMed]
- Papanastasiou, A.D.; Sirinian, C.; Kalofonos, H.P. Identification of novel human receptor activator of nuclear factor-kB isoforms generated through alternative splicing: Implications in breast cancer cell survival and migration. Breast Cancer Res. 2012, 14, R112. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Variable | N | % |
|---|---|---|---|
| Age | <50 | 14 | 38.88 |
| ≥50 | 22 | 61.12 | |
| Grade | I | 4 | 11.11 |
| II | 17 | 47.22 | |
| III | 13 | 36.11 | |
| Unreported | 2 | 5.56 | |
| Stage | I | 23 | 63.89 |
| II | 9 | 25.00 | |
| III | 3 | 8.33 | |
| Unreported | 1 | 2.78 |
| Parameter | Variable | N | % |
|---|---|---|---|
| Age | <50 | 5 | 12.50 |
| ≥50 | 35 | 87.50 | |
| Grade | I | 2 | 5.00 |
| II | 21 | 52.50 | |
| III | 17 | 42.50 | |
| Stage | I | 12 | 30.00 |
| II | 7 | 17.50 | |
| III | 13 | 32.50 | |
| IV | 8 | 20.00 | |
| M-Stage * | M1 | 7 | 17.50 |
| MX | 33 | 82.50 | |
| N-Stage ** | N0 | 19 | 47.50 |
| N1 | 11 | 27.50 | |
| Nx | 10 | 25.00 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez, R.; Castro, A.; Martínez, J.; Rodríguez-García, V.; Burgués, O.; Tarín, J.J.; Cano, A. Receptor Activator of Nuclear Factor Kappa B (RANK) and Clinicopathological Variables in Endometrial Cancer: A Study at Protein and Gene Level. Int. J. Mol. Sci. 2018, 19, 1848. https://doi.org/10.3390/ijms19071848
Gómez R, Castro A, Martínez J, Rodríguez-García V, Burgués O, Tarín JJ, Cano A. Receptor Activator of Nuclear Factor Kappa B (RANK) and Clinicopathological Variables in Endometrial Cancer: A Study at Protein and Gene Level. International Journal of Molecular Sciences. 2018; 19(7):1848. https://doi.org/10.3390/ijms19071848
Chicago/Turabian StyleGómez, Raúl, Ana Castro, Jessica Martínez, Víctor Rodríguez-García, Octavio Burgués, Juan J. Tarín, and Antonio Cano. 2018. "Receptor Activator of Nuclear Factor Kappa B (RANK) and Clinicopathological Variables in Endometrial Cancer: A Study at Protein and Gene Level" International Journal of Molecular Sciences 19, no. 7: 1848. https://doi.org/10.3390/ijms19071848