
Estimation of Oral Disease Burden among Older Adults in LTC: A Scoping Review
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
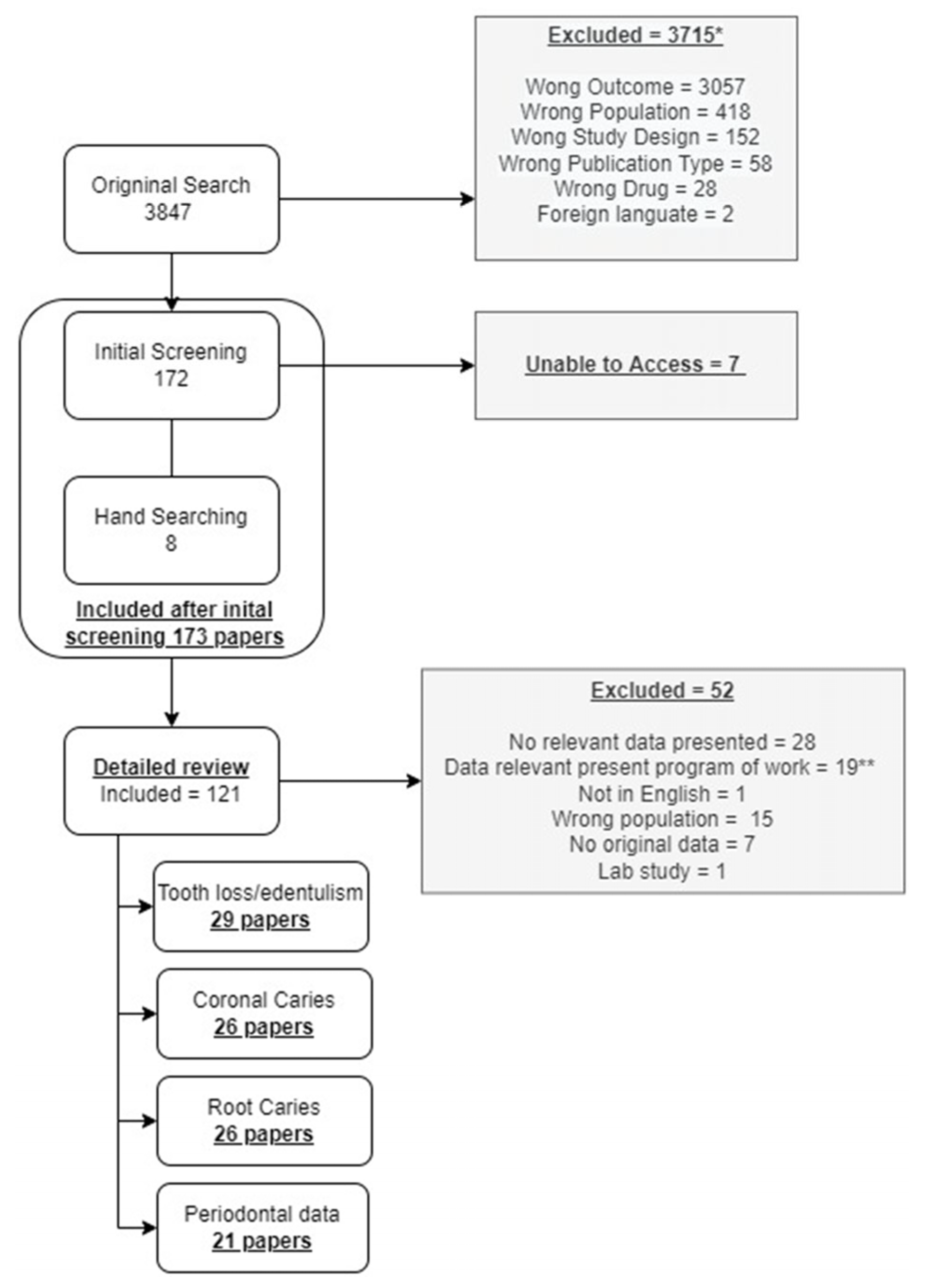
2.1. Study Selection
2.2. Data Synthesis
2.3. Calibration Process
2.4. Synthesis of Results
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, J.; Wallace, J.; Doshi, M.; Gadanya, M.; Yahya, I.B.; Roseman, J.; Srisilapanan, P. Oral health for healthy ageing. Lancet Healthy Longev. 2021, 2, e521–e527. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Griffin, P.M.; Li, C.H.; Bailey, W.D.; Brunson, D.; Jones, J.A. Changes in older adults’ oral health and disparities: 1999 to 2004 and 2011 to 2016. J. Am. Geriatr. Soc. 2019, 7, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, J.M.; Rawal, K. Demographics and Oral Health Care Utilization for Older Adults. Dent. Clin. N. Am. 2021, 65, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Brocklehurst, P.R.; Baker, S.R.; Langley, J. Context and the evidence-based paradigm: The potential for participatory research and systems thinking in oral health. Community Dent. Oral Epidemiol. 2021, 49, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Turton, B.; Henshaw, M.; Rawal, K.; Tembhe, A.; Alqunaybit, G.; Qari, A.; Calabrese, J. Prevention of Oral Disease Among Older Adults in Long Term Care. Open Science Framework. 2023. Available online: https://osf.io/6fve5/?view_only=b824a9a1881d4382b2e3bdb2e6abe610 (accessed on 8 June 2023).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A.; Chalmers, T.; Smith, H. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Gautam, N.R.; Kumar, P.M.; Kadhiresan, R.; Saxena, V.; Jain, S. Assessment of dental caries and periodontal disease status among elderly residing in old age homes of Madhya Pradesh. J. Int. Oral Health 2015, 7, 57. [Google Scholar]
- Ericson, D.; Carlsson, P.; Gabre, P.; Wårdh, I.; Zimmerman, M.; Sjögren, P. Effect of a single application of silver diamine fluoride on root caries after 12 months in institutionalised older adults—A randomised clinical trial. Gerodontology 2023, 40, 390–397. [Google Scholar] [CrossRef]
- Hunt, R.J.; Eldredge, J.B.; Beck, J.D. Effect of residence in a fluoridated community on the incidence of coronal and root caries in an older adult population. J. Public Health Dent. 1989, 49, 138–141. [Google Scholar] [CrossRef]
- Nevalainen, M.J.; Närhi, T.O.; Ainamo, A. A 5-year follow-up study on the prosthetic rehabilitation of the elderly in Helsinki, Finland. J. Oral Rehabil. 2004, 31, 647–652. [Google Scholar] [CrossRef]
- Ajwani, S.; Ainamo, A. Periodontal conditions among the old elderly: Five-year longitudinal study. Spec. Care Dent. 2001, 21, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, A.; Watanabe, R.; Hanada, N.; Miyazaki, H. A longitudinal study of the relationship between diet intake and dental caries and periodontal disease in elderly Japanese subjects. Gerodontology 2009, 26, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Aida, J.; Tsuboya, T.; Hikichi, H.; Kondo, K.; Kawachi, I.; Osaka, K. Are lowered socioeconomic circumstances causally related to tooth loss? A natural experiment involving the 2011 great East Japan earthquake. Am. J. Epidemiol. 2017, 1, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Gülcan, F.; Nasir, E.; Ekbäck, G.; Ordell, S.; Åstrøm, A.N. Change in Oral Impacts on Daily Performances (OIDP) with increasing age: Testing the evaluative properties of the OIDP frequency inventory using prospective data from Norway and Sweden. BMC Oral Health 2014, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Stuck, A.E.; Chappuis, C.; Flury, H.; Lang, N.P. Dental treatment needs in an elderly population referred to a geriatric hospital in Switzerland. Community Dent. Oral Epidemiol. 1989, 17, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.M.; Carter, K.D.; Fuss, J.M.; Spencer, A.J.; Hodge, C.P. Caries experience in existing and new nursing home residents in Adelaide, Australia. Gerodontology 2002, 19, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Caries incidence and increments in community-living older adults with and without dementia. Gerodontology 2002, 19, 80–94. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Hodge, C.; Fuss, J.M.; Spencer, A.J.; Carter, K.D. The prevalence and experience of oral diseases in Adelaide nursing home residents. Aust. Dent. J. 2002, 47, 123–130. [Google Scholar] [CrossRef]
- Fure, S.; Zickert, I. Incidence of tooth loss and dental caries in 60-, 70-and 80-year-old Swedish individuals. Community Dent. Oral Epidemiol. 1997, 25, 137–142. [Google Scholar] [CrossRef]
- Wyatt, C.C.; MacEntee, M.I. Caries management for institutionalized elders using fluoride and chlorhexidine mouthrinses. Community Dent. Oral Epidemiol. 2004, 32, 322–328. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Caries incidence and increments in Adelaide nursing home residents. Spec. Care Dent. 2005, 25, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Adam, H.; Preston, A.J. The oral health of individuals with dementia in nursing homes. Gerodontology 2006, 23, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Tramini, P.; Montal, S.; Valcarcel, J. Tooth loss and associated factors in long-term institutionalized elderly patients. Gerodontology 2007, 24, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Arpin, S.; Brodeur, J.M.; Corbeil, P. Dental caries, problems perceived and use of services among institutionalized elderly in 3 regions of Quebec, Canada. J. Can. Dent. Assoc. 2008, 74, 9. [Google Scholar]
- Philip, P.; Rogers, C.; Kruger, E.; Tennant, M. Caries experience of institutionalized elderly and its association with dementia and functional status. Int. J. Dent. Hyg. 2012, 10, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Zenthöfer, A.; Rammelsberg, P.; Cabrera, T.; Schröder, J.; Hassel, A.J. Determinants of oral health-related quality of life of the institutionalized elderly. Psychogeriatrics 2014, 14, 247–254. [Google Scholar] [CrossRef] [PubMed]
- CBG Health Research. Our Older People’s Oral Health. Key Findings of the 2012 New Zealand Older People’s Oral Health Survey; CBG Health Research: Auckland, New Zealand, 2015; ISBN 978-0-473-34655-3. Available online: https://www.health.govt.nz/system/files/documents/publications/our-older-peoples-oral-health-2012-nz-older-peoples-oral-health-survey-feb16.pdf (accessed on 19 February 2024).
- Pham, T.A.; Nguyen, T.Q. Dental and periodontal problems of elderly people in Vietnamese nursing homes. Gerodontology 2018, 35, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Saarela, R.K.; Savikko, N.M.; Soini, H.; Muurinen, S.; Suominen, M.H.; Kautiainen, H.; Pitkala, K.H. Burden of oral symptoms and health-related quality of life in long-term care settings in Helsinki, Finland. J. Nutr Health Aging 2019, 23, 1021–1025. [Google Scholar] [CrossRef]
- Chiesi, F.; Grazzini, M.; Innocenti, M.; Giammarco, B.; Simoncini, E.; Garamella, G.; Zanobini, P.; Perra, C.; Baggiani, L.; Lorini, C.; et al. Older people living in nursing homes: An oral health screening survey in Florence, Italy. Int. J. Environ. Res. Public Health 2019, 16, 3492. [Google Scholar] [CrossRef]
- Girestam Croonquist, C.; Dalum, J.; Skott, P.; Sjögren, P.; Wårdh, I.; Morén, E. Effects of domiciliary professional oral care for care-dependent elderly in nursing homes–oral hygiene, gingival bleeding, root caries and nursing staff’s oral health knowledge and attitudes. Clin. Interv. Aging 2020, 6, 1305–1315. [Google Scholar] [CrossRef]
- Tanji, F.; Komiyama, T.; Ohi, T.; Hattori, Y.; Watanabe, M.; Lu, Y.; Tsuji, I. The association between number of remaining teeth and maintenance of successful aging in Japanese older people: A 9-year longitudinal study. Tohoku J. Exp. Med. 2020, 252, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Mazzea, S.; Fortunato, L.; Giudice, A.; Papadopoli, R.; Nobile, C.G.; Pavia, M. Oral health status and the impact on oral health-related quality of life among the institutionalized elderly population: A cross-sectional study in an area of southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 2175. [Google Scholar] [CrossRef] [PubMed]
- Tokumoto, K.; Kimura-Ono, A.; Mino, T.; Osaka, S.; Numoto, K.; Koyama, E.; Kurosaki, Y.; Nakagawa, S.; Amano, Y.; Nguyen, H.T.; et al. Risk factors for root caries annual incidence and progression among older people requiring nursing care: A one-year prospective cohort study. J. Prosthodont. Res. 2022, 66, 250–257. [Google Scholar] [CrossRef]
- MacEntee, M.I.; Silver, J.G.; Gibson, G.; Weiss, R. Oral health in a long-term care institution equipped with a dental service. Community Dent. Oral Epidemol. 1985, 13, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Vigild, M. Dental caries and the need for treatment among institutionalized elderly. Community Dent. Oral Epidemiol. 1989, 17, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.A.; Lavallee, N.; Alman, J.; Sinclair, C.; Garcia, R.I. Caries incidence in patients with dementia. Gerodontology 1993, 10, 76–82. [Google Scholar] [CrossRef] [PubMed]
- MacEntee, M.I.; Clark, D.C.; Glick, N. Predictors of caries in old age. Gerodontology 1993, 10, 90–97. [Google Scholar] [CrossRef]
- Wyatt, C.C. Elderly Canadians residing in long-term care hospitals: Part II. Dental caries status. J. Can. Dent. Assoc. 2002, 1, 359–363. [Google Scholar]
- McMillan, A.S.; Wong, M.C.; Lo, E.C.; Allen, P.F. The impact of oral disease among the institutionalized and non-institutionalized elderly in Hong Kong. J. Oral Rehabil. 2003, 30, 46–54. [Google Scholar] [CrossRef]
- Vilstrup, L.; Holm-Pedersen, P.; Mortensen, E.L.; Avlund, K. Dental status and dental caries in 85-year-old Danes. Gerodontology 2007, 24, 3–13. [Google Scholar] [CrossRef]
- Gluhak, C.; Arnetzl, G.V.; Kirmeier, R.; Jakse, N.; Arnetzl, G. Oral status among seniors in nine nursing homes in Styria, Austria. Gerodontology 2010, 27, 47–52. [Google Scholar] [CrossRef]
- Chen, X.; Shuman, S.K.; Hodges, J.S.; Gatewood, L.C.; Xu, J. Patterns of tooth loss in older adults with and without dementia: A retrospective study based on a Minnesota cohort. J. Am. Geriatr. Soc. 2010, 58, 2300–2307. [Google Scholar] [CrossRef]
- Ellefsen, B.S.; Morse, D.E.; Waldemar, G.; Holm-Pedersen, P. Indicators for root caries in Danish persons with recently diagnosed Alzheimer’s disease. Gerodontology 2012, 29, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Hopcraft, M.; Morgan, M. Dental caries in Victorian nursing homes. Aust. Dent. J. 2014, 59, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Bilder, L.; Yavnai, N.; Zini, A. Oral health status among long-term hospitalized adults: A cross-sectional study. PeerJ 2014, 10, e423. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, J.S.; Kohanchi, D.; Biren-Fetz, J.; Fontana, M.; Ramchandani, M.; Osann, K.; Hallajian, L.; Mansour, S.; Nabelsi, T.; Chung, N.E.; et al. Detection and proportion of very early dental caries in independent living older adults. Lasers Surg. Med. 2015, 47, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; McGrath, C.; Lo, E.C.; Li, J.Y. Silver diamine fluoride and education to prevent and arrest root caries among community-dwelling elders. Caries Res. 2013, 1, 284–290. [Google Scholar] [CrossRef]
- Berg, R.; Berkey, D.; Tang, J.M.; Baine, C.; Altman, D.S. Oral health status of older adults in Arizona: Results from the Arizona Elder Study. Spec. Care Dent. 2000, 20, 226–233. [Google Scholar] [CrossRef]
- Tan, H.P.; Lo, E.C.; Dyson, J.E.; Luo, Y.; Corbet, E.F. A randomized trial on root caries prevention in elders. J. Dent. Res. 2010, 89, 1086–1090. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Poulsen, J.E.; Hede, B.; Twetman, S.; Qvist, V.; Ellwood, R.P. A randomized clinical trial of the anti-caries efficacy of 5000 compared to 1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013, 47, 391–398. [Google Scholar] [CrossRef]
- Zhang, J.; Leung, K.C.; Chu, C.H.; Lo, E.C. Risk indicators for root caries in older adults using long-term social care facilities in Hong Kong. Community Dent. Oral Epidemiol. 2020, 48, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Fitzgerald, R.; Warburton, F.; Robertson, C.; Pitts, N.B.; Gallagher, J.E. Refocusing dental care: A risk-based preventative oral health program for dentate older people in UK care homes. Gerodontology 2022, 39, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.D.; Koch, G.G.; Offenbacher, S. Incidence of attachment loss over 3 years in older adults—New and progressing lesions. Community Dent. Oral Epidemiol. 1995, 23, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Qian, F.; Levy, S.M.; Warren, J.J.; Hand, J.S. Incidence of periodontal attachment loss over 8 to 10 years among Iowa elders aged 71+ at baseline. J. Public Health Dent. 2007, 67, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Yoshihara, A.; Hirotomi, T.; Ando, Y.; Miyazaki, H. Risk factors for periodontal disease progression among elderly people. J. Clin. Periodontol. 2002, 29, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.M.; Warren, J.J.; Chowdhury, J.; DeBus, B.; Watkins, C.A.; Cowen, H.J.; Kirchner, H.L.; Hand, J.S. The prevalence of periodontal disease measures in elderly adults, aged 79 and older. Spec. Care Dent. 2003, 23, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Mack, F.; Mojon, P.; Budtz-Jørgensen, E.; Kocher, T.; Splieth, C.; Schwahn, C.; Bernhardt, O.; Gesch, D.; Kordaß, B.; John, U.; et al. Caries and periodontal disease of the elderly in Pomerania, Germany: Results of the Study of Health in Pomerania. Gerodontology 2004, 21, 27–36. [Google Scholar] [CrossRef]
- Orwoll, E.S.; Chan, B.K.; Lambert, L.C.; Marshall, L.M.; Lewis, C.; Phipps, K.R. Sex steroids, periodontal health, and tooth loss in older men. J. Dent. Res. 2009, 88, 704–708. [Google Scholar] [CrossRef]
- Siukosaari, P.; Ajwani, S.; Ainamo, A.; Wolf, J.; Närhi, T. Periodontal health status in the elderly with different levels of education: A 5-year follow-up study. Gerodontology 2012, 29, e170–e178. [Google Scholar] [CrossRef]
- Sánchez-García, S.; Reyes-Morales, H.; Juárez-Cedillo, T.; Espinel-Bermúdez, C.; Solórzano-Santos, F.; García-Peña, C. A prediction model for root caries in an elderly population. Community Dent. Oral Epidemiol. 2011, 39, 44–52. [Google Scholar] [CrossRef]
- Syrjälä, A.M.; Ylöstalo, P.; Ruoppi, P.; Komulainen, K.; Hartikainen, S.; Sulkava, R.; Knuuttila, M. Dementia and oral health among subjects aged 75 years or older. Gerodontology 2012, 29, 36–42. [Google Scholar] [CrossRef]
- Gaio, E.J.; Haas, A.N.; Carrard, V.C.; Oppermann, R.V.; Albandar, J.; Susin, C. Oral health status in elders from South Brazil: A population-based study. Gerodontology 2012, 29, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Kimble, R.; McLellan, G.; Lennon, L.T.; Papacosta, A.O.; Weyant, R.J.; Kapila, Y.; Mathers, J.C.; Wannamathee, S.G.; Whincup, P.H.; Ramsay, S.E. Association between oral health markers and decline in muscle strength and physical performance in later life: Longitudinal analyses of two prospective cohorts from the UK and the USA. Lancet Healthy Longev. 2022, 3, e777–e788. [Google Scholar] [CrossRef] [PubMed]
- Kotronia, E.; Brown, H.; Papacosta, O.; Lennon, L.T.; Weyant, R.J.; Whincup, P.H.; Wannamethee, S.G.; Ramsay, S.E. Oral health problems and risk of incident disability in two studies of older adults in the United Kingdom and the United States. J. Am. Geriatr. Soc. 2022, 70, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe tooth loss: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 20S–28S. [Google Scholar] [CrossRef]
- Lee, H.; Kim, D.; Jung, A.; Chae, W. Ethnicity, social, and clinical risk factors to tooth loss among older adults in the US, NHANES 2011–2018. Int. J. Environ. Res. Public Health 2022, 19, 2382. [Google Scholar] [CrossRef]
- Walgama, K.; Wides, C.; Kottek, A.; Mertz, E. The Impact of Federal and State Policy on Oral Health Care Delivery in Long-Term Care Settings. J. Health Care Poor Underserved 2018, 29, 1570–1586. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D.; Morford, L.A.; Huja, P.E.; Hartsfield, J.K., Jr.; Huja, S.S.; Pandruvada, S.; Wallet, S.M. Aging, inflammation, immunity and periodontal disease. Periodontology 2016, 72, 54–75. [Google Scholar] [CrossRef]
- Coker, E.; Ploeg, J.; Kaasalainen, S. The effect of programs to improve oral hygiene outcomes for older residents in long-term care: A systematic review. Res. Gerontol. Nurs. 2014, 7, 87–100. [Google Scholar] [CrossRef]
- Weening-Verbree, L.; Huisman-de Waal, G.; Van Dusseldorp, L.; van Achterberg, T.; Schoonhoven, L. Oral health care in older people in long term care facilities: A systematic review of implementation strategies. Int. J. Nurs. Stud. 2013, 50, 569–582. [Google Scholar] [CrossRef]
- Willumsen, T.; Karlsen, L.; Næss, R.; Bjørntvedt, S. Are the barriers to good oral hygiene in nursing homes within the nurses or the patients? Gerodontology 2012, 29, e748–e755. [Google Scholar] [CrossRef]
- Baker, S.R. Editorial ‘No simple solutions, no single ingredient’: Systems orientated approaches for addressing Wicked Problems in population oral health. Community Dent. Health 2019, 36, 3–4. [Google Scholar]
- Gibson, L.B.; Blake, M.; Baker, S. Inequalities in oral health: The role of sociology. Community Dent. Health 2016, 33, 156–160. [Google Scholar]
- Niesten, D.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Oral health care behavior and frailty-related factors in a care-dependent older population. J. Dent. 2017, 61, 39–47. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Older adults in long-term care facilities and community settings and in any country. | Younger population age groups (<65 years old) |
| Language | English | Non-English language papers |
| Interventions | Those include, but are not limited to, Fluoride Varnish, Mouth rinses, Silver Diamine fluoride, high fluoride toothpaste | Interventions occurring with the wrong population. |
| Publication status | Published literature searchable by PubMed, Embase, or Dentistry and oral sciences sources. | Not available online using search engines or hand searches |
| Study designs | Cross-sectional surveys, cohort studies, experimental studies | Qualitative studies, review articles, articles without original data |
| Outcome measures | Caries incidence, incidence of tooth loss (incidence), periodontal disease incidence, oral symptoms, periodontal diseases | If there is an absence of clinical measures on caries, periodontal disease, tooth loss, or oral symptoms. Studies where the clinical outcome is the plaque score and there are no other clinical outcome measures meeting our criteria will be excluded. |
| Dates | Any date if the electronic version of the paper is available | All dates included |
| Author | Country | Prevalence of Edentulism | Mean Number of Missing Teeth | Proportion with >20 Teeth | Incidence of Tooth Loss |
|---|---|---|---|---|---|
| Stuck et al., 1989 [16] | Switzerland | 58.90% | |||
| Hunt et al., 1995 [10] * | USA | 0.7 (SD2.0) over 18 m; 0.5/year | |||
| Chalmers et al., 2002 [17] | Australia | 66% | 18.9 (no SD) | ||
| Chalmers et al., 2002 [18] | Australia | 19.3 (SD 7.4) | |||
| Chalmers et al., 2002 [19] | Australia | excluded | 10.4 (No SD) | 0.4/year | |
| Fure, 2003 [20] * | Sweden | 27% | 21.2 (SD 6.6) | 2.5 (SD 3.4) over 5 years; 0.5/year | |
| Wyatt & MacEntee, 2004 [21] | Canada | 14.9 (SD 6.9) | 0.1 teeth per year | ||
| Nevalainen et al., 2004 [11] * | Finland | 31% | 16.2 (SD 8.0) | 1% year became edentulous | |
| Ajwani & Ainamo, 2004 [12] * | Finland | 12.2 (SD 7.7) | 0.9 teeth over 5 years; 0.2 teeth per year | ||
| Chalmers et al., 2005 [22] | Australia | 63.10% | |||
| Adam et al., 2006 [23] | UK | 65.90% | 27.8 (SD 7.0) | ||
| Tramini et al., 2007 [24] | France | 26.90% | 33.6% | ||
| Arpin S et al., 2008 [25] | Canada | 19.1 (SD 7.8) | |||
| Yoshihara et al., 2008 [13] * | Japan | 19.3 (SD 8.6) | 1.7 (SD 2.2) over 6 years; 0.3 teeth lost per year | ||
| Philip P et al., 2012 [26] | Australia | 17.7 (SD 7.2) | |||
| Zenthöfer et al., 2014 [27] | Germany | 39.40% | 20.3 (SD 8.9) | ||
| Agrawal et al., 2015 [8] | India | 37.90% | 6.7 (SD 5.2) | ||
| Tompson et. al., 2015 [28] | NZ | 56.6% | 15.6 (SD 14.7) ** | 35.1% ** | |
| Matsuyama et al., 2016 [14] * | Japan | 8% | 8.2% lost ≥ 1 tooth over 3 years (2.7%/year) | ||
| Gülcan et al., 2017 [15] * | Norway and Sweden | 5.5% lost one or more teeth over 5 years (1.1%/year) | |||
| Pham and Nguyen, 2018 [29] | Vietnam | 9.90% | 13.8 (SD 7.4) ** | 52.1% | |
| Saarela et al., 2019 [30] | Finland | 13% *** | |||
| Chiesi and Grazzini et al., 2019 [31] | Italy | 39.8% | 21% | ||
| Girestam Croonquist et al., 2019 [32] | Sweden | 7.8 (SD 3.0) ** | |||
| Tanji et al., 2020 [33] | Japan | 32% <10 teeth | 44.4% | ||
| Bianco A et al., 2021 [34] | Italy | 31.90% | 17% | ||
| Ericson et al., 2022 [9] | Sweden | 8.0 (SD 5.9) ** | |||
| Tokumoto et al., 2022 [35] | Japan | 14.7 (SD 8.0) |
| Author | Country | Caries Severity | Untreated Caries Severity and Prevalence | Caries Increment/Prevalence of New Lesions (DS/DT) |
|---|---|---|---|---|
| MacEntee et. al., 1985 [36] | Canada | 78% | ||
| Vigild et al., [37] | Denmark | DT = 9.6 | ||
| Jones et al., 1993 [38] | USA | FS = 9.5 (SD 5.7) | DT = 1.0 (SD 1.5) | |
| MacEntee et al., 1993 [39] | Canada | DMFT = 24.1 | DT = 3.4 (SD 4.4) DS = 7.4 (SD 12.1) | DS/year = 0.9 (SD 1.5) FS/year = 0.5 (SD 1.3) |
| Wyatt, 2002 [40] | Canada | DMFS = 112.3 (SD 26.6) | DS = 3.8 (SD 4.2) | |
| Chalmers et al., 2002 [17] | Australia | DMFT = 23.7 | ||
| Chalmers et al., 2002 [18] | Australia | DMFT = 24.4 (SD 4.5) | DT = 1.7 (SD 2.5) | 17.7% (SE11.7%) ** |
| McMillan et al., 2003 [41] | Hong Kong | DMFT = 21.4 (SD 0.6) | DT = 2.1 (SD 0.2) | |
| Wyatt and MacEntee., 2004 [21] | Canada | DMFS = 112.3 (SD 26.6) | DT/year = 2.3 (SD not presented) | |
| Chalmers et al., 2005 [22] | Australia | DT/year 2.2 (SD 3.9)/year | ||
| Adam et al., 2006 [23] | UK | DMFT = 29.7 (SD 11.7) | DT = 0.9 | |
| Vilstrup et al., 2007 [42] | Denmark | FS = 11.8 | DS = 3.0 (SD 3.4); 57.60% | |
| Arpin et al., 2008 [25] | Canada | DMFT = 24.9 | ||
| Gluhak et al., 2010 [43] | Austria | DMFT = 25.6 (SD 4.2) | ||
| Chen et al., 2010 [44] | United States | DMFT = 23.2 | DT = 3.3 (SD 4.0) | |
| Ellefsen et al., 2012 [45] | Denmark | FS = 32.4 (SD 21.4) | DS = 2.9 (SD 3.6) | |
| Philip P et al., 2012 [26] | Australia | DMFT = 26.0 (SD 4.3) * | DT = 3.0 (SD 3.5) | |
| Silva et al., 2014 [46] | Australia | DMFT = 21.7 (SD 0.3) | DT = 2.7 (SD 0.2) | |
| Bilder et al., 2014 [47] | Israel | DT = 4.2 (SD 4.5) | ||
| Agrawal et al., 2015 [8] | India | DFT—8.3 * | DT = 1.5 (no SD reported) | |
| Tompson et. al., 2015 [28] | NZ | DMFT = 24.2 (CI 23.5, 25.0) | DT = 2.2 (CI 1.8, 2.5) 61.3%; DT among those with caries = 3.5 (CI 3.1, 4.0) | |
| Holtzman et al., 2015 [48] | USA | DT = 0.50 (26.0%) | ||
| Pham & Nguyen, 2018 [29] | Vietnam | DMFT = 20.0 | DT = 5.8 (SD 4.0) | |
| Zhang et al., 2019 [49] | Hongkong, China | DMFT = 10.1 (SD not reported) | DT = 0.8 (SD 1.6) | |
| Bianco et al., 2021 [34] | Italy | DMFT = 26.4 (SD 7.5) | DT—3.5 (SD 4.6); 70.8% | |
| Ericson et al., 2022 [9] | Sweden | DT—2.0 (SD 6.7) |
| Citation | Country | Root Caries Definition ** | Severity/Prevalence of Root Caries ** | Incidence and Increment *** |
|---|---|---|---|---|
| Jones et al., 1993 [38] | USA | NIDCR definition | T-DRS = 2.8 (SD 4.3) T-DRS = 4.6 (SD 4.7) | T-DRS/year = 1.0 (SD 3.3) |
| MacEntee et al., 1993 [39] | Canada | NS | T-DRS/year = 1.6 (SD 3.1) Filled root surfaces = 0.8 (SD 2.3)/year | |
| Berg et al., 2000 [50] | USA | NIDCR diagnostic criteria. | DRS = 4.1 (SD 8.9) FRS = 21.1 (SD 18.5) | |
| Wyatt et al., 2012 [40] | Canada | The Root Caries Index | DFRS = 30.3 (SD 26.1) | |
| Chalmers et al., 2002 [17] | Australia | The Root Caries Index | T-DRS = 1.5; T-FRS = 1.1 | |
| Chalmers et al., 2002 [18] | Australia | The Root Caries Index | T-DRS = 2.6 (SD 3.9) T-DFRS = 1.3 (SD 3.3) | |
| McMillan et al., 2003 [41] | Hong Kong | NS | T-DRS = 1.3 (SD 0.2) teeth | |
| Wyatt and MacEntee, 2004 [21] | Canada | The Root Caries Index | T-DRS= 4.6 (SD 6.8); 68% of people | 1.8 (SD 1.6) |
| Chalmers et al., 2005 [22] | Australia | NIDCR definition | 0.8/year | |
| Tan et al., 2010 [51] | Hongkong | Lesions “easily penetrable with a sharp sickle probe” | DRS = 1.3 (SD 0.1); FRS = 0.8 (SD 0.1) 10.7% of exposed root surfaces | 1.3 (SD 0.2) or 0.4/year |
| Ellefsen et al., 2012 [45] | Denmark | NIDCR criteria | DRS = 4.9 (SD 6.1); FRS = 5.4 (SD 4.8) | |
| Philip P et al., 2012 [26] | Australia | The Root Caries Index | 0.1 (SD 0.4) | |
| Ekstrandet al., 2013 [52] | Denmark | NS | 3.3 (SD 3.0) * | |
| Zhang et al., 2013 [49] | China | NS | T-DRS = 0.2 (0.1) | 1.0 (SD 0.1)/year |
| Silva et al., 2014 [46] | Australia | ICDAS II ≥ Code 2 | T-DRS = 3.4 (0.3) | |
| Tompson et al., 2015 [28] | NZ | A lesion on the root surface that was soft to exploration using a periodontal probe | T-DRS = 0.8 (CI 0.6, 1.0); 33.7%—among those with >1 lesion TDRS = 2.4 (CI 2.0, 2.7) | |
| Pham and Nguyen, 2018 [29] | Vietnam | NS | T-DRS = 6.0 (SD 4.2) | |
| Zhang et al., 2020 [53] | Hongkong, China | Visual inspection (NS) | T- DR = 0.7 (±1.7); T-DFS = 1.3 (SD 2.1); 43.10% of people | |
| Patel et al., 2022 [54] | UK | NS | T-DFRS = 3.1; 69.20% of people | |
| Ericson et al., 2022 [9] | Sweden | Nyvad modified criteria | 11.4% of lesions progressed | |
| Tokumoto et al., 2022 [35] | Japan | Fejerskov et al. | 16% of teeth | T-DRS = 14.6% of teeth/year and 22.5% of existing lesions progressed across one-year |
| Author | Country | Disease Descriptor | Perio Status/Incidence of Disease |
|---|---|---|---|
| MacEntee et al., 1985 [36] | Canada | CPITN | CPI > 3 = 29% |
| Beck et al., 1995 [55] | USA ** | Incidence = % of people with 1+ sites of AL of 3+ mm over 3 years Affected = mean number of sites with AL in people with AL. | One or more new sites of attachment loss = 27.5% of people. Progression of existing sites with attachment loss = 11.1% of people Overall (either new or progressing sites) = 20.1% The mean number of sites progressing = 4.5 sites (SD 0.5) |
| Ogawa H et al., 2002 [57] | Japan * | Worst CAL | <4 mm = 3.5%; 4–6 mm = 32.5%; >6 mm = 64% |
| Levy et al., 2003 [58] | USA ** | Worst attachment loss | For those who had their most severe CAL at 4 mm, the mean number of sites involved was 11.38 (±12.47); 6 mm = 1.93 ± 5.05; 8 mm = 0.44 (1.62) |
| McMillan et al., 2003 [41] | Hong Kong ** | The most severe CPITN score | CPI 0 = 0.0%; CPI 1 = 0.5%; CPI 2 = 40.1%; CPI 3 = 39.6%; CPI 4 = 19.8% |
| Mack et al., 2004 [59] | Germany * | Presence of pockets >4 mm and >6 mm | ≥4 mm pockets = 49.1%; ≥6 mm pockets = 21.7% |
| Ajwani and Ainamo, 2004 [12] | Finland ** | One or more sextants with > Code 3 CPITN | CPI ≥ 3 = 43% |
| Qian et al., 2007 [56] | USA * | CAL, Incidence of ALOSS (>2 mm difference). | Mean CAL = 1.6 mm (SD 0.6); 16.1% of sites with >2 mm progression/10 years. |
| Yoshihara et al., 2008 [13] | Japan * | Presence of site with >3 mm difference in periodontal readings across one-year | Sites per year = 9.8 (SD 6.5) |
| Orwoll et al., 2009 [60] | USA * | Gingival index, Gingival bleeding, CAL | Mean gingival index = 1.2 + 0.5; Prevalence of gingival bleeding = 53%; Mean CAL = 3.0 (SD 0.8) |
| Chen et al., 2010 [44] | USA * | Presence of calculus, plaque and gingival bleeding; | none= 1.2%; mild to moderate = 81.3%; High = 17.7% |
| Gluhak et al., 2010 [43] | Austria | CPITN | CPI ≥ 2 = 84.1% |
| Siukosaari et al., 2010 [61] | Finland ** | Most severe CPITN | CPI ≥ 3 = 44.7 |
| Sánchez-García et al., 2011 [62] | Mexico * | % of those with CPI code >2 | CPI > 2 = 36.1% |
| Syrjälä et al., 2012 [63] | Finland * | Number of teeth with pocket depth >4 mm | Mean of 2.9 teeth (SD3.7) |
| Gaio et al., 2012 [64] | Brazil * | Worst CAL (person level) | W-CAL ≥ 3 mm = 94%; W-CAL ≥ 5 mm = 60% of teeth |
| Tompson et al., 2015 [28] | NZ | CPI code on index teeth | CPI ≥ 3 = 11.2% (CI 7.9, 14.5) CPI > 4 = 2.1% |
| Agrawal et al., 2015 [8] | India | CPITN by sextant | 0.5 sextants/person (SD 0.9); |
| Pham and Nguyen, 2018 [29] | Vietnam | Worst pocket depth | ≤3 mm = 526 (73.8%); 4–6 mm = 116 (16.7%); ≥7 mm = 68 (9.5%) |
| Kimble et al., 2022 [65] | US/UK * | Percentage people with 20% of sites having >3.5 mm CAL | UK sample—>20% with >3.5 mm pockets = 20.1% US sample—>20% with >3.5 mm pockets = 52.9% |
| Kotronia et al., 2022 [66] | UK/US * | >20% sites with LOA >3.5 mm and >5.5 mm | UK sample—20% >3.5 mm = 53%; 20% > 5.5 mm = 29% US sample—>20% >3.5 mm = 64%; >20% > 5.5 mm = 31% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turton, B.; Alqunaybit, G.; Tembhe, A.; Qari, A.; Rawal, K.; Mandel, E.; Calabrese, J.; Henshaw, M. Estimation of Oral Disease Burden among Older Adults in LTC: A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 248. https://doi.org/10.3390/ijerph21030248
Turton B, Alqunaybit G, Tembhe A, Qari A, Rawal K, Mandel E, Calabrese J, Henshaw M. Estimation of Oral Disease Burden among Older Adults in LTC: A Scoping Review. International Journal of Environmental Research and Public Health. 2024; 21(3):248. https://doi.org/10.3390/ijerph21030248
Chicago/Turabian StyleTurton, Bathsheba, Gheed Alqunaybit, Amrita Tembhe, Alaa Qari, Kadambari Rawal, Ernest Mandel, Joseph Calabrese, and Michelle Henshaw. 2024. "Estimation of Oral Disease Burden among Older Adults in LTC: A Scoping Review" International Journal of Environmental Research and Public Health 21, no. 3: 248. https://doi.org/10.3390/ijerph21030248