
Comparison of Urban versus Industry Normative Values of Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT™)
Abstract
:1. Introduction
2. Materials and Methods
- Previous history of concussion (n = 53)
- Learning disability (n = 35)
- Diagnosed psychiatric disability (n = 28)
- Repeated a year in school (n = 24)
- Treatment for migraines (n = 16)
- Deemed invalid by ImPACT™ (n = 97)
3. Results
4. Discussion
4.1. Clinical Implication
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langlis, J.A.; Rutlan-Brown, W.; Wald, M.M. The epidemiology and impact of traumatic brain injury: A brief over. J. Head Trauma. Rehabil. 2006, 21, 375–378. [Google Scholar] [CrossRef]
- Zhang, A.L.; Sing, D.C.; Rugg, C.M.; Freely, B.T.; Senter, C. The rise of concussions in the adolescent population. Orthop. J. Sports Med. 2016, 4, 2325967116662458. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.W.; Grindel, S.H.; Lovell, M.R.; Dede, D.E.; Moser, D.J.; Phalin, B.R.; Nogle, S.; Wasik, M.; Cordry, D.; Daugherty, K.M.; et al. Relationship between concussion and neuropsychological performance in college football players. JAMA 1999, 282, 964–970. [Google Scholar] [CrossRef]
- Bleiberg, J.; Kane, R.L.; Reeves, D.L.; Garmoe, W.S.; Halpern, E. Factor analysis of computerized and traditional tests used in mild brain injury research. Clin. Neuropsychol. 2000, 14, 287–294. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Ross, S.E.; Marshall, S.W. Postural stability and neuropsychological deficits after concussion in collegiate athletes. J. Athl. Train. 2001, 36, 263–273. [Google Scholar]
- Valovich, T.C.; Perrin, D.H.; Gansneder, B.M. Repeat administration elicits a practice effect with the balance error scoring system but not with the standardized assessment of concussion in high school athletes. J. Athl. Train. 2003, 38, 51–56. [Google Scholar] [PubMed]
- Field, M.; Collins, M.W.; Lovell, M.R.; Maroon, J. Does age play a role in recovery from sports-related concussion? A comparison of high school and collegiate athletes. J. Pediatr. 2003, 142, 546–553. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Guskiewicz, K.M.; Marshall, S.W.; Barr, W.; Randolph, C.; Cantu, R.C.; Onate, J.A.; Jingzhen, Y.; Kelly, J.P. Acute effects and recovery time following concussion in collegiate football players: The NCAA concussion study. JAMA 2003, 290, 2556–2563. [Google Scholar] [CrossRef]
- Hunt, T.N.; Ferrara, M.S. Age-related differences in neuropsychological testing among high school athletes. J. Athl. Train. 2009, 44, 405–409. [Google Scholar] [CrossRef]
- Collins, M.W.; Iverson, G.L.; Lovell, M.R.; McKeag, D.B.; Norwig, J.; Maroon, J. On-field predictors of neuropsychological and symptom deficit following sports-related concussion. Clin. J. Sport. Med. 2003, 13, 222–229. [Google Scholar] [CrossRef]
- Daniel, J.C.; Olesniewicz, M.H.; Reeves, D.L.; Bleiberg, J.; Thatcher, R.; Salazar, A. Repeated measures of cognitive processing efficiency in adolescent athletes: Implications for monitoring recovery from concussion. Neuropsych. Neuropsychol. Behav. Neurol. 1999, 12, 167–169. [Google Scholar]
- Guskiewicz, K.M.; Weaver, N.L.; Padua, D.A.; Garrett, W.E., Jr. Epidemiology of concussion in collegiate and high school football players. Am. J. Sports Med. 2000, 28, 643–650. [Google Scholar] [CrossRef]
- Lovell, M.R.; Collins, M.W.; Iverson, G.L.; Field, M.; Maroon, J.C.; Cantu, R.; Podell, K.; Powell, J.W.; Belza, M.; Fu, F.H. Recovery from mild concussion in high school athletes. J. Neurosurg. 2003, 98, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Aubry, M.; Cantu, R.; Dvorak, J.; Johnston, K.; Kelly, J.; Lovell, M.; McCrory, P.; Meeuwisse, W.; Schamasch, P. Summary and agreement statement of the First International Conference on Concussion in Sport, Vienna 2001: Recommendations for the improvement of safety and health of athletes who may suffer concussive injuries. Br. J. Sports Med. 2002, 36, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Broglio, S.P.; Cantu, R.; Gioia, G.A.; Guskiewicz, K.M.; Kutcher, J.; Palm, M.; Valovich McLeod, T.C.; National Athletic Trainers’ Association. National Athletic Trainers’ Association position statement: Management of sport concussion. J. Athl. Train. 2014, 49, 245–265. [Google Scholar] [CrossRef]
- Patricious, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus Statement on concussion in sport: The 6th International conference on concussion in sport—Amsterdam 2022. Br. J. Sports Med. 2023, 57, 695–711. [Google Scholar] [CrossRef]
- Herring, S.A.; Cantu, R.C.; Guskiewicz, K.M.; Putukian, M.; Kibler, W.B.; Bergfeld, J.A.; Boyajian-O’Neill, L.A.; Franks, R.R.; Indelicato, P.A.; American College of Sports Medicine. Concussion (mild traumatic brain injury) and the team physician: A consensus statement. Med. Sci. Sports Exerc. 2006, 38, 395–399. [Google Scholar]
- Greiffenstein, M.; Baker, W.J. Premorbid clues? Pre-injury scholastic performance and present neuropsychological functioning in late postconcussion syndrome. J. Clin. Neuropsychol. 2003, 17, 561–573. [Google Scholar] [CrossRef]
- Macciocchi, S.N.; Barth, J.T.; Alves, W.; Jane, J.A. Neuropsychological functioning and recovery after mild head injury in collegiate athletes. J. Neurosurg. 1996, 39, 510–514. [Google Scholar] [CrossRef]
- Lovell, M.R.; Iverson, G.L.; Collins, M.W.; McKeag, D.; Maroon, J.C. Does loss of consciousness predict neuropsychological decrements after concussion? Clin. J. Sports Med. 1999, 9, 193–198. [Google Scholar] [CrossRef]
- Spreen, O.; Strauss, E. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Baumgartner, T.A.; Jackson, A.S.; Mahar, M.T.; Rowe, M.T.; David, A. Measurement for Evaluation; McGraw-Hill: Boston, MA, USA, 2003; pp. 96–119. [Google Scholar]
- Spreen, O.; Risser, A.; Edgell, D. Developmental Neuropsychology; Oxford University Press: New York, NY, USA, 1995; pp. 37–77. [Google Scholar]
- Segalowitz, S.J.; Brown, D. Mild head injury as a source of developmental disabilities. J. Learn. Disabil. 1991, 24, 551–559. [Google Scholar] [CrossRef]
- Beers, S.R.; Goldstein, G.; Katz, L.J. Neuropsychological differences between college students with learning disabilities and those with mild head injury. J. Learn. Disabil. 1991, 27, 315–324. [Google Scholar] [CrossRef]
- Seidman, L.J.; Biederman, J.; Monuteaux, M.C.; Weber, W.; Faraone, S.V. Neuropsychological functioning in nonreferred siblings of children with attention deficit/hyperactivity disorder. J. Abnorm. Psychol. 2000, 109, 252–265. [Google Scholar] [CrossRef]
- Slomine, B.S.; Salorio, C.F.; Grados, M.A.; Vasa, R.A.; Christensen, J.R.; Gerring, J.P. Differences in attention, executive functioning, and memory in children with and without ADHD after severe traumatic brain injury. J. Int. Neuropsychol. Soc. 2005, 11, 645–653. [Google Scholar] [CrossRef]
- Jakobson, A.; Kikas, E. Cognitive functioning in children with and without attention-deficit/Hyperactivity disorder with and without comorbid learning disabilities. J. Learn. Disabil. 2007, 40, 194–202. [Google Scholar] [CrossRef]
- Hunt, T.N.; Ferrara, M.S.; Miller, L.S.; Macchiochi, S. The effect of effort on neuropsychological test scores in high school football players. Arch. Clin. Neuropsychol. 2007, 22, 615–621. [Google Scholar] [CrossRef]
- Mueller, C.W.; Parcel, T.L. Measures of socioeconomic status: Alternatives and recommendations. Child. Dev. 1981, 52, 13–30. [Google Scholar] [CrossRef]
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health: Discussion Paper for the Commission on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Adler, N.E.; Rehkopf, D.H. U.S. disparities in health: Descriptions, causes, and mechanisms. Annu. Rev. Public. Health 2008, 29, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.H.; Corwyn, R.F.; McAdoo, R.; Pipes, H.; García, C.C. The Home Environments of Children in the United States Part I: Variations by Age, Ethnicity, and Poverty. Child. Dev. 2002, 72, 1844–1867. [Google Scholar] [CrossRef] [PubMed]
- Alder, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health. Am. Psychol. 1994, 49, 15–24. [Google Scholar]
- Anderson, V.A.; Catroppa, C.; Dudgeon, P.; Morse, S.A.; Haritou, F.; Rosenfeld, J.V. Understanding predictors of functional recovery and outcome 30 months following early childhood head injury. Neuropsychology 2006, 20, 42–57. [Google Scholar] [CrossRef]
- Taylor, H.G.; Yeates, K.O.; Wade, S.L.; Drotar, D.; Klein, S.K.; Stancin, T. Influences on first-year recovery from traumatic brain injury in children. Neuropsychology 1999, 13, 76–89. [Google Scholar] [CrossRef]
- Ewing-Cobbs, L.; Prasad, M.R.; Landry, S.H.; Kramer, L.; DeLeon, R. Executive functions following traumatic brain injury in young children: A preliminary analysis. Dev. Neuropsychol. 2004, 26, 487–512. [Google Scholar] [CrossRef]
- Taylor, S.E.; Lerner, J.S.; Sage, R.M.; Lehman, B.J.; Seeman, T.E. Early environment, emotions, responses to stress, and health. J. Pers. 2004, 72, 1365–1393. [Google Scholar] [CrossRef] [PubMed]
- Anderson, V.; Brown, S.; Newitt, H.; Hoile, H. Long-term outcome from childhood traumatic brain injury: Intellectual ability, personality and quality of life. Neuropsychology 2011, 25, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Haines, K.L.; Nguyen, B.P.; Vatsaas, C.; Alger, A.; Brooks, K.; Agarwal, S.K. Socioeconomic status affects outcomes after severity-stratified traumatic brain injury. J. Surg. Res. 2019, 235, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Shavers, V.L. Measurement of socioeconomic status in health disparities research. J. Natl. Med. Assoc. 2007, 99, 1013–1023. [Google Scholar]
- Houck, Z.; Asken, B.; Clugston, J.; Perlstein, W.; Bauer, R. Socioeconomic status and race outperform concussion history and sport participation in predicting collegiate athlete baseline neurocognitive scores. J. Int. Neuropsychol. Soc. 2018, 24, 1–10. [Google Scholar] [CrossRef]
- Zuckerman, S.L.; Zalneraitis, B.H.; Totten, D.J.; Rubel, K.E.; Kuhn, A.W.; Yengo-Kahn, A.M.; Bonfield, C.M.; Sills, A.K.; Solomon, G.S. Socioeconomic status and outcomes after sport-related concussion: A preliminary investigation. J. Neurosurg. Peds. 2007, 19, 652–661. [Google Scholar] [CrossRef]
- McLoyd, V.C. Socioeconomic disadvantage and child development. Am. Psychol. 1998, 53, 185–204. [Google Scholar] [CrossRef]
- Lovell, M. ImPACT Version 2.0 Clinical User’s Manual; ImPACT Applications Inc.: Coralville, IA, USA, 2004. [Google Scholar]
- Schatz, P.; Pardini, J.E.; Lovell, M.R.; Collins, M.W.; Podell, K. Sensitivity and specificity of the ImPACT™ test battery for concussion in athletes. Arch. Clin. Neuropsychol. 2006, 21, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; English, K. The environment of poverty; multiple stressor exposure, psychophysiological stress, and socioemotional adjustment. Child. Dev. 2002, 73, 1238–1248. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Gonnella, C.; Marcynyszyn, L.A.; Gentile, L.; Salpekar, N. The role of chaos in poverty and children’s socioemotional adjustment. Psychol. Sci. 2005, 16, 560–565. [Google Scholar] [CrossRef]
- Evans, G.W. Child development and the physical environment. Annu. Rev. Psychol. 2006, 57, 423–451. [Google Scholar] [CrossRef]
- Sarsour, K.; Sheridan, M.; Jutte, D.; Nuru-Jeter, A.; Hinshaw, S.; Boyce, W.T. Family Socioeconomic Status and Child Executive Functions: The Roles of Language, Home Environment, and Single Parenthood. J. Int. Neuropsychol. Soc. 2011, 17, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Kennepohl, S.; Shore, D.; Nabors, N.; Hanks, R. African American acculturation and neuropsychological test performance following traumatic brain injury. J. Int. Neuropsychol. Soc. 2004, 10, 566–577. [Google Scholar] [CrossRef] [PubMed]
- Hackman, D.A.; Farah, M.J. Socioeconomic status and the developing brain. Trends Cogn. Sci. 2009, 13, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Farah, M.J.; Shera, D.M.; Savage, J.H.; Betancourt, L.; Giannetta, J.M.; Brodsky, N.L.; Malmud, E.K.; Hurt, H. Childhood poverty: Specific associations with neurocognitive development. Brain Res. 2006, 1110, 166–174. [Google Scholar] [CrossRef]
- Baxendale, S.; Heaney, D. Socioeconomic Status, cognition and hippocampal sclerosis. Epilepsy Behav. 2011, 20, 64–67. [Google Scholar] [CrossRef]
- Ip, E.Y.; Giza, C.C.; Griesbach, G.S.; Hovda, D.A. Effects of enriched environment and fluid percussion injury on dendritic arborization within the cerebral cortex of the developing rat. J. Neurotrauma. 2002, 19, 573–585. [Google Scholar] [CrossRef]
- Mormile, M.E.E.; Langdon, J.L.; Hunt, T.N. The role of gender in neuropsychological assessment in healthy adolescents. J. Sport Rehab. 2018, 27, 16–21. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Height | Weight | Ethnicity | % Free and Reduced Lunch | |
|---|---|---|---|---|---|
| (Years ± S.D) | (in. ± S.D) | (lbs) | %White | ||
| Total | 15.6 ± 2.5 | 69.3 ± 3.35 | 180.4 ± 48.31 | 19% | 81% |
| 13–15 | 14.2 ± 1.1 | 67.6 ± 3.77 | 170.6 ± 46.87 | 20% | 81% |
| 16–18 | 16.9 ± 1.2 | 70.6 ± 3.43 | 190.7 ± 50.11 | 19% | 81% |
| Age | Test | Urban | Published Norm | T | p | 95% Confident Interval |
|---|---|---|---|---|---|---|
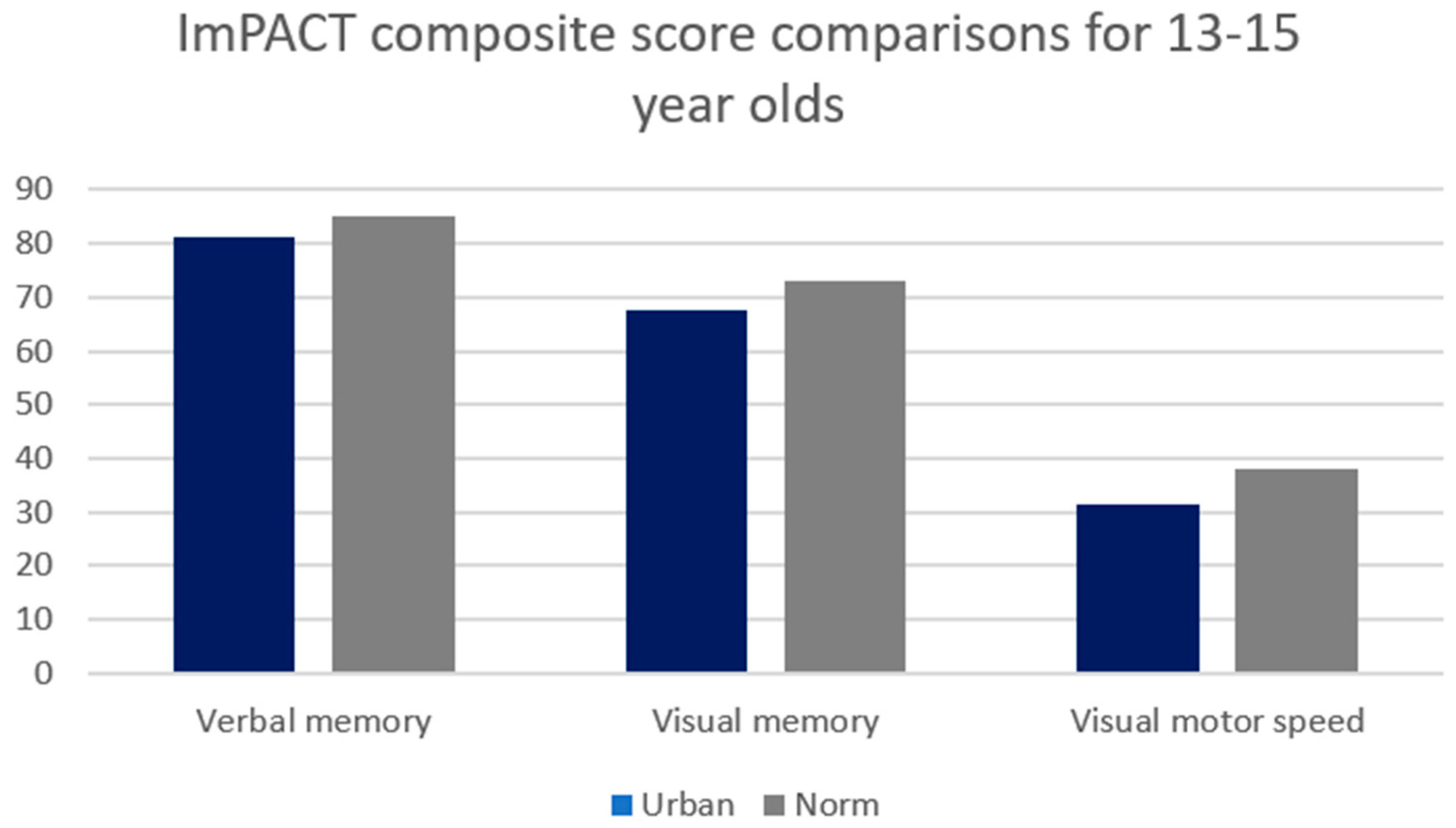
| 13–15 years old (n = 300) | Verbal | 81.3 (9.8) | 85 | −6.7 | <0.001 | 80.2–82.4 |
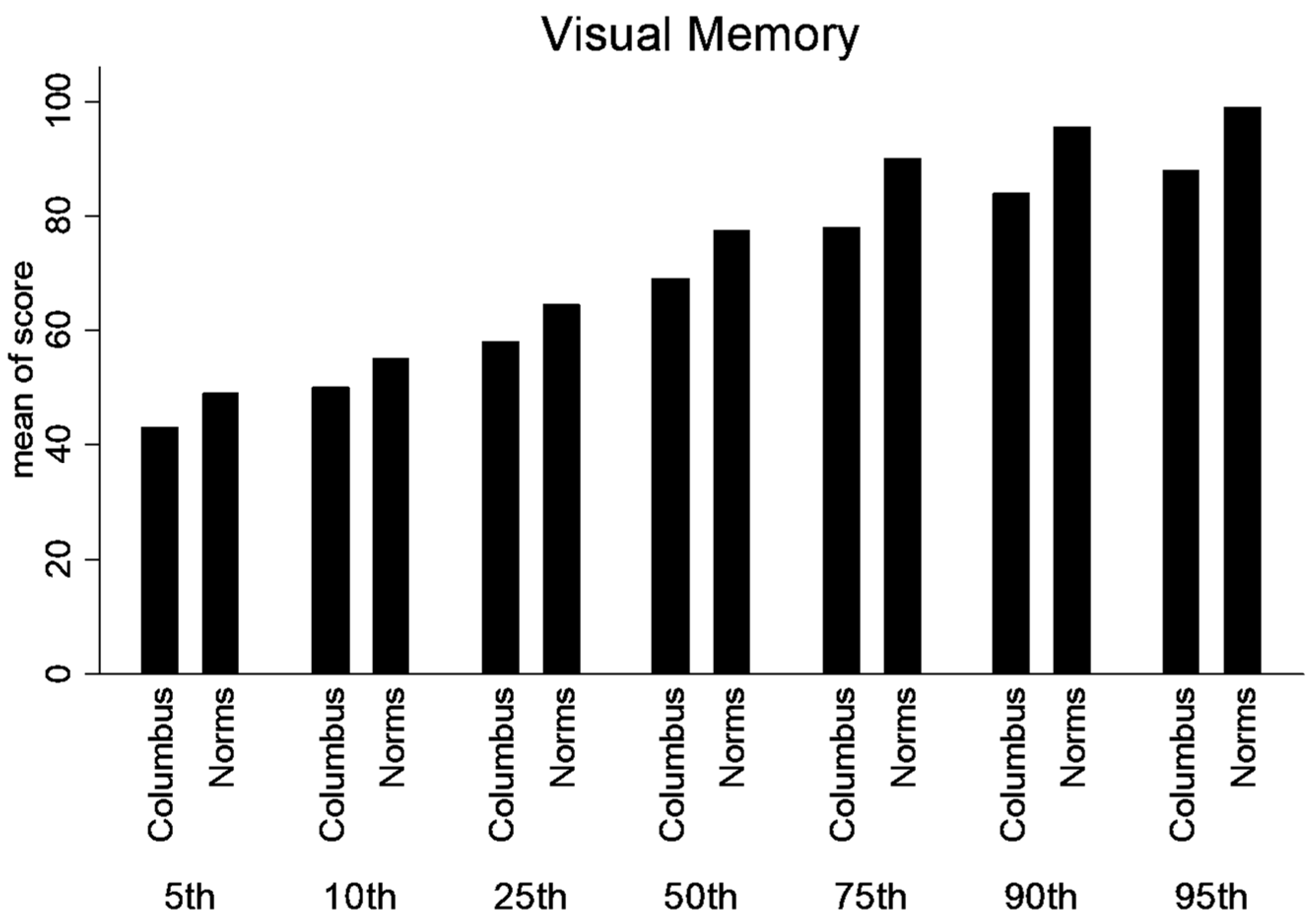
| Visual | 67.5 (13.1) | 73 | −6.9 | <0.001 | 65.9–69.1 | |
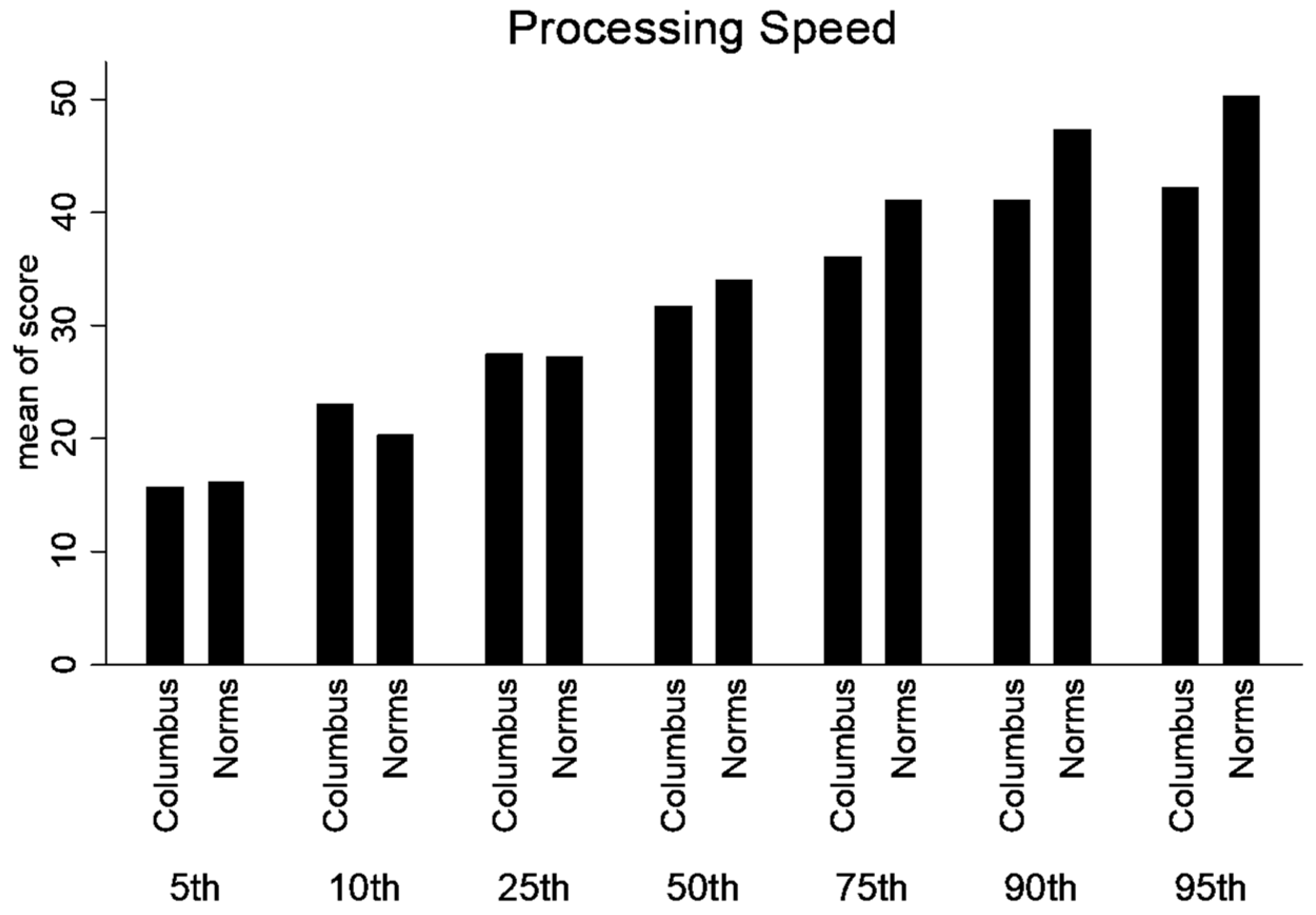
| Visual Motor Speed | 31.5 (7.4) | 38 | −15.9 | <0.001 | 30.6–32.3 | |
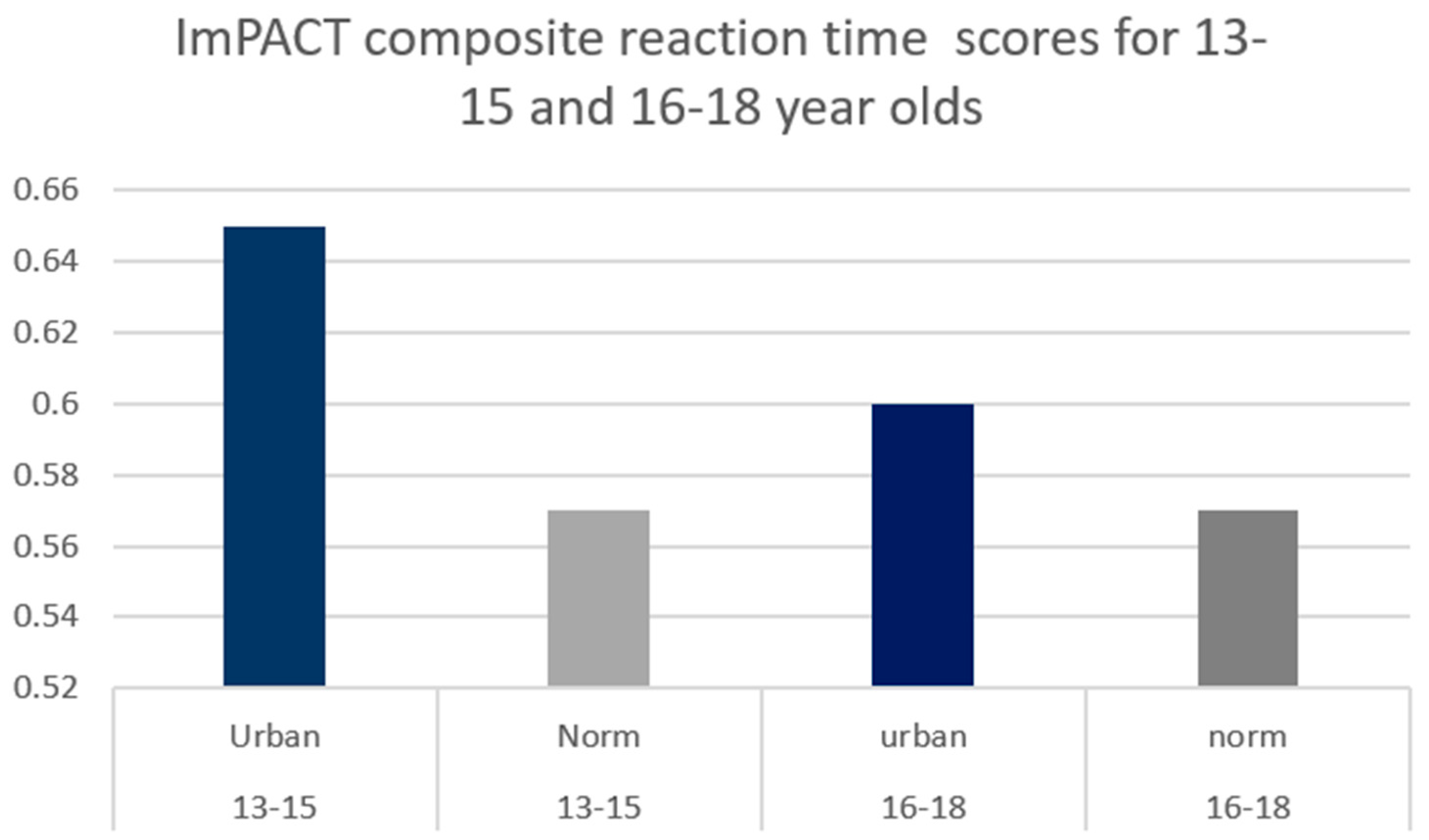
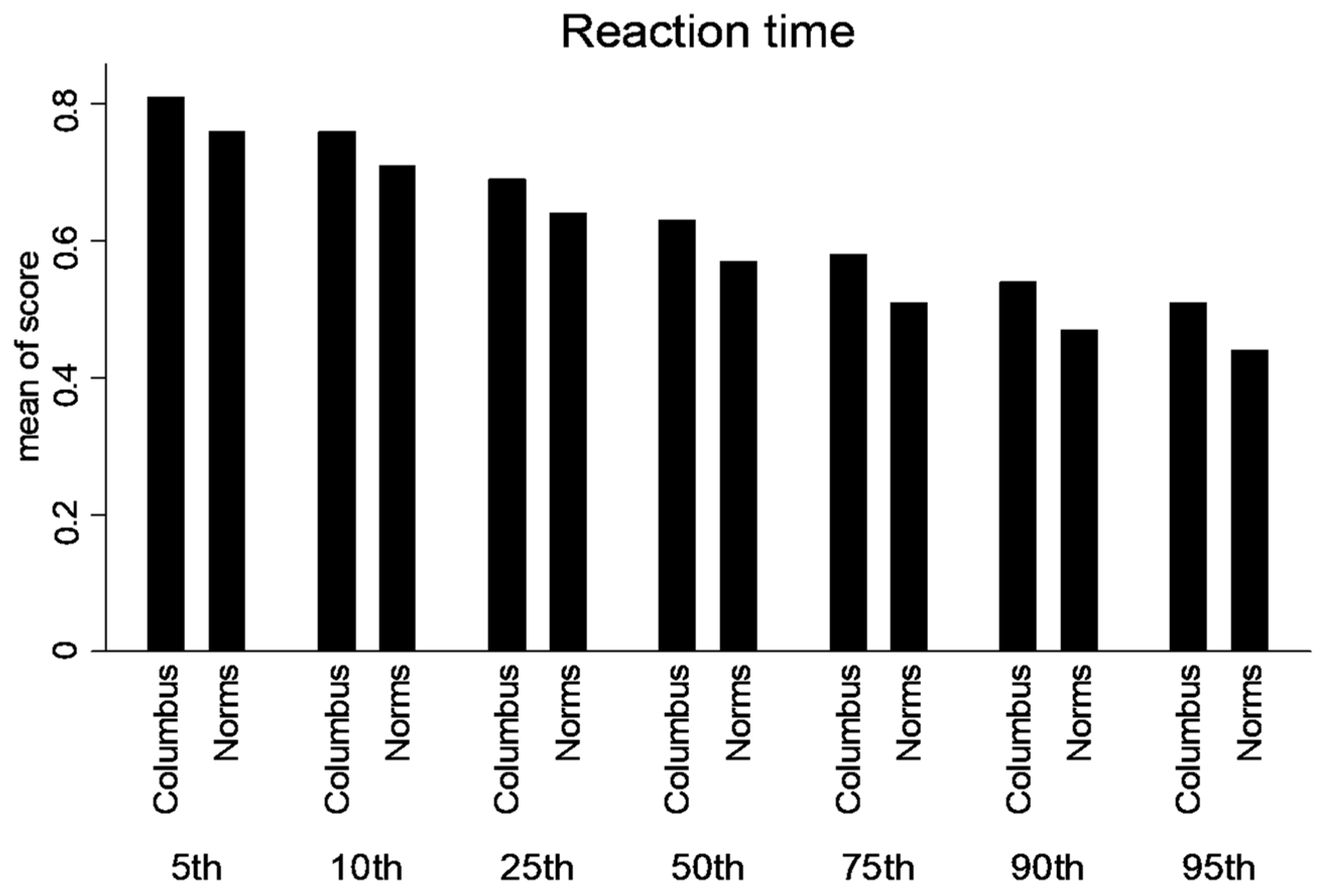
| Reaction Time | 0.65 (0.1) | 0.57 | 11.8 | <0.001 | 0.63–0.66 | |
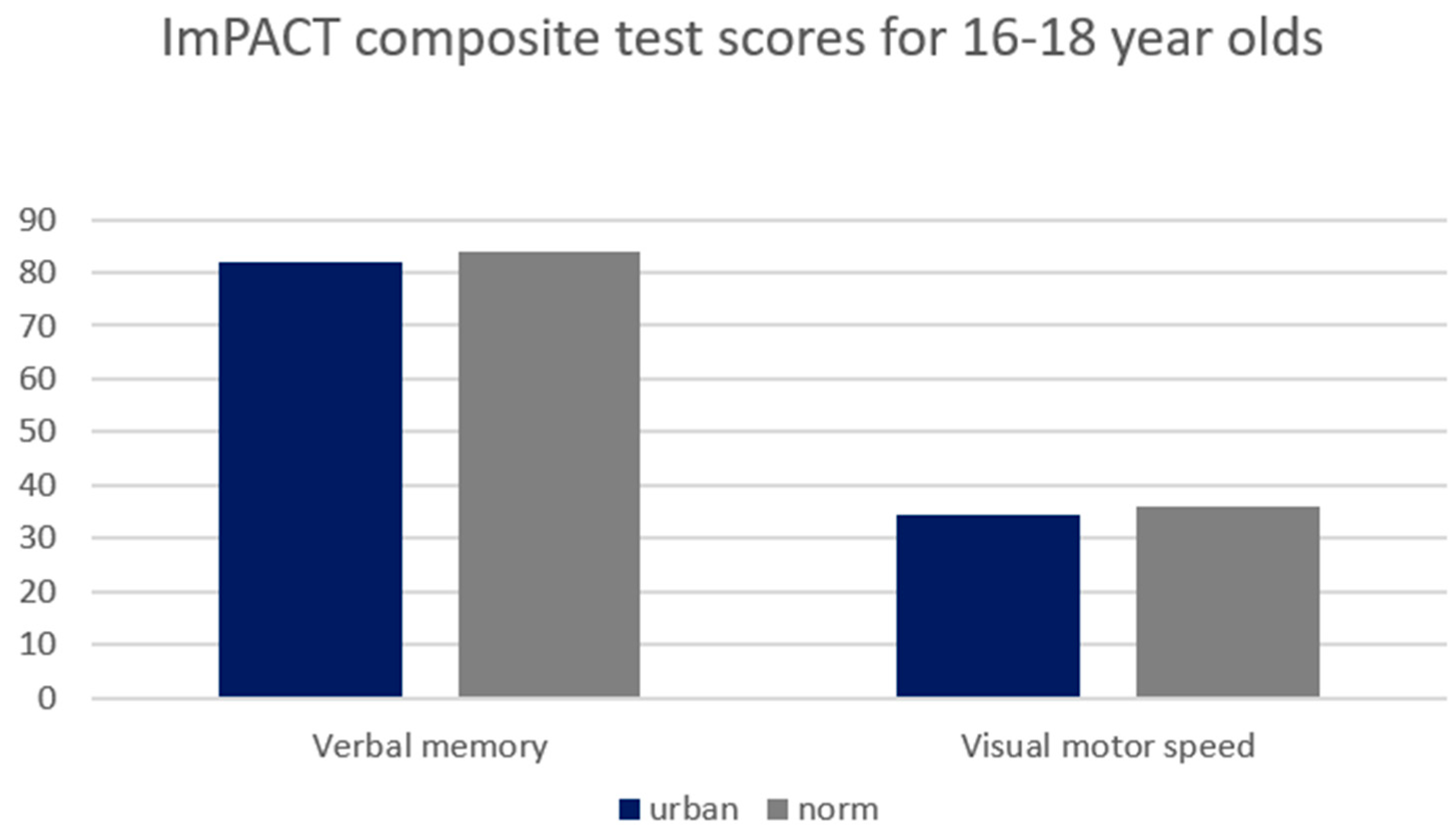
| 16–18 years old (n = 331) | Verbal | 81.9 (9.9) | 84 | −4.1 | <0.001 | 80.9–82.9 |
| Visual Motor Speed | 34.3 (7.3) | 36 | −5.7 | <0.001 | 33.4–35.1 | |
| Reaction Time | 0.6 (0.09) | 0.53 | 6.9 | <0.001 | 0.59–0.62 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hunt, T.N.; Byrd, M. Comparison of Urban versus Industry Normative Values of Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT™). Int. J. Environ. Res. Public Health 2024, 21, 247. https://doi.org/10.3390/ijerph21030247
Hunt TN, Byrd M. Comparison of Urban versus Industry Normative Values of Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT™). International Journal of Environmental Research and Public Health. 2024; 21(3):247. https://doi.org/10.3390/ijerph21030247
Chicago/Turabian StyleHunt, Tamerah N., and Megan Byrd. 2024. "Comparison of Urban versus Industry Normative Values of Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT™)" International Journal of Environmental Research and Public Health 21, no. 3: 247. https://doi.org/10.3390/ijerph21030247