An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers

1. Introduction
1.1. Background on Health Literacy in Social Contexts
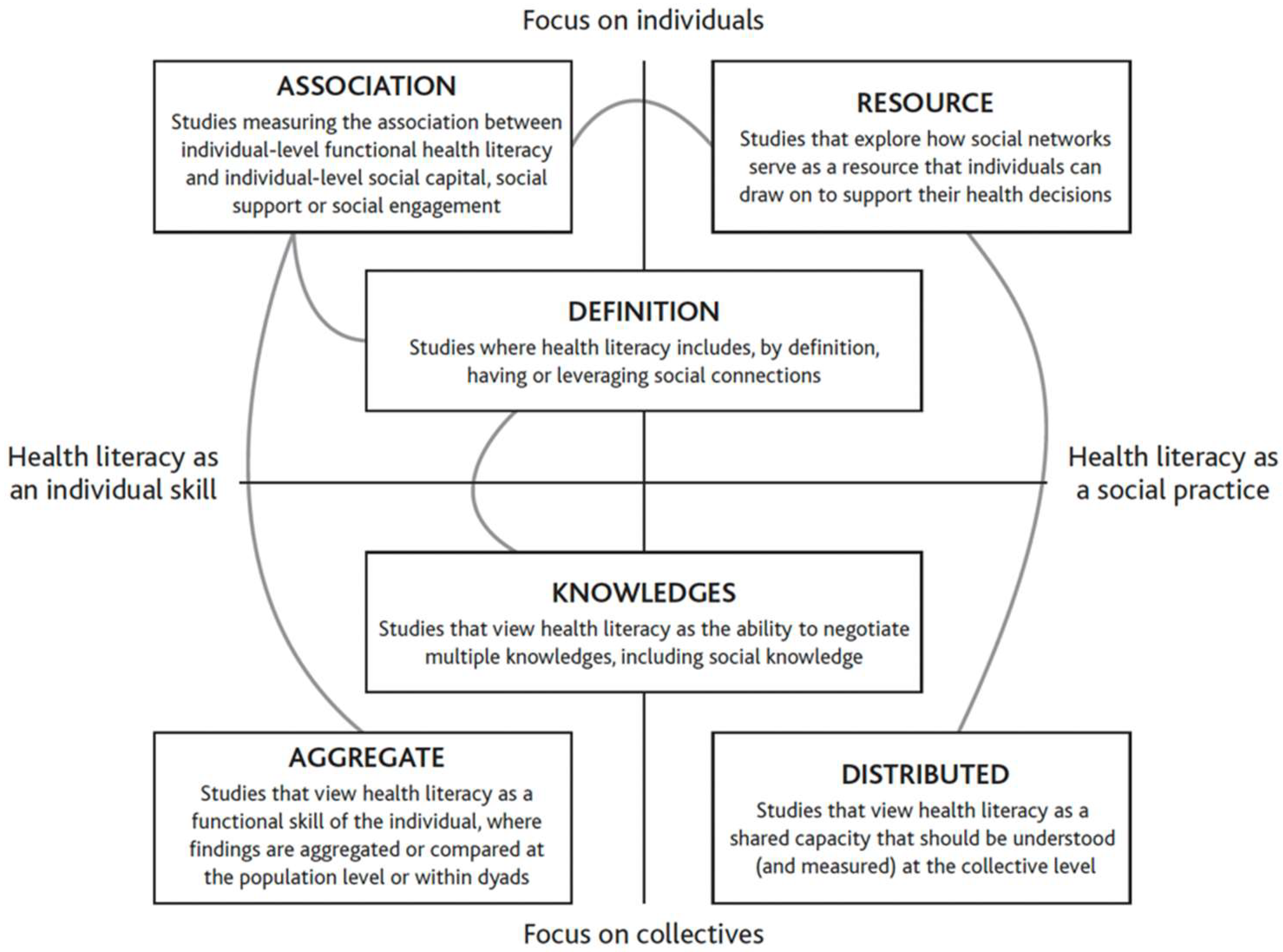
1.2. Definitions, Characteristics of Included Articles, and Conceptual Strategy
2. Health Literacy and Social Context Findings from the Special Issue
3. Practical Implications for Health Professionals and Suggestions for Future Research
3.1. Multiple Individual Factors and Levels of Social Context Intersect to Influence Health Literacy. A Comprehensive, Multi-Level Intervention Framework Could Guide Practice and Research
3.2. Social Resources and Contexts Outside the Medical Sphere Can Be Leveraged to Enhance Health Literacy in Vulnerable Populations through Meaningful Partnerships
3.3. Digital Interaction Spaces and Online Communication Are Central in Health Decision Making and Should Be a Focus of Health Literacy Interventions and Research
3.4. Health Literacy Has Bi-Directional Influences on Overall Community Health
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baker, D.W. The Meaning and the Measure of Health Literacy. J. Gen. Intern. Med. 2006, 21, 878–883. [Google Scholar] [CrossRef]
- Batterham, R.W.; Hawkins, M.; Collins, P.A.; Buchbinder, R.; Osborne, R.H. Health Literacy: Applying Current Concepts to Improve Health Services and Reduce Health Inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef]
- Ratzan, S.C.; Parker, R.M. Health Literacy. National Library of Medicine Current Bibliographies in Medicine; National Institutes of Health, US Department of Health and Human Services: Bethesda, MD, USA, 2000.
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80–93. [Google Scholar] [CrossRef]
- Abreu, L.; Arriscado Nunes, J.; Taylor, P.; Silva, S. Distributed Health Literacy among People Living with Type 2 Diabetes in Portugal: Defining Levels of Awareness and Support. Health Soc. Care Community 2018, 26, 90–101. [Google Scholar] [CrossRef]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. Distributed Health Literacy’: Longitudinal Qualitative Analysis of the Roles of Health Literacy Mediators and Social Networks of People Living with a Long-Term Health Condition. Health Expect. 2015, 18, 1180–1193. [Google Scholar] [CrossRef]
- Ellis, J.; Mullan, J.; Worsley, A.; Pai, N. The Role of Health Literacy and Social Networks in Arthritis Patients’ Health Information-Seeking Behavior: A Qualitative Study. Int. J. Fam. Med. 2012, 2012, 397039. [Google Scholar] [CrossRef]
- Kim, Y.C.; Lim, J.Y.; Park, K. Effects of Health Literacy and Social Capital on Health Information Behavior. J. Health Commun. 2015, 20, 1084–1094. [Google Scholar] [CrossRef]
- Lee, S.Y.; Arozullah, A.M.; Cho, Y.K. Health Literacy, Social Support, and Health: A Research Agenda. Soc. Sci. Med. 2004, 58, 1309–1321. [Google Scholar] [CrossRef]
- Sentell, T.; Pitt, R.; Buchthal, O.V. Health Literacy in a Social Context: Review of Quantitative Evidence. HLRP Health Lit. Res. Pract. 2017, 1, e41–e70. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Clouston, S.A.; Manganello, J.A.; Richards, M. A life course approach to health literacy: The role of gender, educational attainment and lifetime cognitive capability. Age Ageing 2017, 46, 493–499. [Google Scholar] [CrossRef]
- Fage-Butler, A.M.; Nisbeth Jensen, M. Medical terminology in online patient-patient communication: Evidence of high health literacy? Health Expect. 2016, 19, 643–653. [Google Scholar] [CrossRef]
- Federman, A.D.; Sano, M.; Wolf, M.S.; Siu, A.L.; Halm, E.A. Health literacy and cognitive performance in older adults. J. Am. Geriatr. Soc. 2009, 57, 1475–1480. [Google Scholar] [CrossRef]
- Sentell, T.; Baker, K.K.; Onaka, A.; Braun, K. Low health literacy and poor health status in Asian Americans and Pacific Islanders in Hawai’i. J. Health Commun. 2011, 16, 279–294. [Google Scholar] [CrossRef]
- Van Der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The relationship between health, education, and health literacy: Results from the Dutch Adult Literacy and Life Skills Survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef]
- Zhou, A.Q.; Lee, H.Y.; Lee, R.M. Who Has Low Health Literacy and Does It Matter for Depression? Findings from Aggregated and Disaggregated Racial/Ethnic Groups. Cult. Divers. Ethn. Minor. Psychol. 2019, 25, 73–81. [Google Scholar] [CrossRef]
- Bourdieu, P. Ökonomisches Kapital–Kulturelles Kapital–Soziales Kapital. In Soziale Ungleichheiten; Kreckel, R., Ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 1983; p. 183. [Google Scholar]
- Liebel, A.M. What counts as literacy in health literacy: Applying the autonomous and ideological models of literacy. Lit. Compos. Stud. 2021, 8, 123. [Google Scholar] [CrossRef]
- Nutbeam, D.; Lloyd, E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42, 159–173. [Google Scholar] [CrossRef]
- Pinheiro, P. Future avenues for health literacy: Learning from literacy and literacy learning. In International Handbook of Health; Literacy Policy Press Bristol: Bristol, UK, 2019; pp. 555–572. [Google Scholar]
- Okan, O.; Pinheiro, P. Von Chicago 1958 bis Shanghai 2016: Ein Rückblick. In Health Literacy im Kindes-und Jugendalter; Bollweg, T.M., Bröder, J., Pinheiro, P., Eds.; Springer: Wiesbaden, VS, USA, 2020; pp. 11–38. [Google Scholar]
- American Medical Association Ad Hoc Committee on Health Literacy for the American Council on Scientific Affairs. Health literacy: Report of the council on scientific affairs. J. Am. Med. Assoc. 1999, 281, 552–557. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 226–259. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef]
- Crondahl, K.; Eklund Karlsson, L. The Nexus Between Health Literacy and Empowerment: A Scoping Review. SAGE Open 2016, 6, 2158244016646410. [Google Scholar] [CrossRef]
- Estacio, E.V. Health Literacy and Community Empowerment: It Is More than Just Reading, Writing and Counting. J. Health Psychol. 2013, 18, 1056–1068. [Google Scholar] [CrossRef]
- Sykes, S.; Wills, J.; Rowlands, G.; Popple, K. Understanding Critical Health Literacy: A Concept Analysis. BMC Public Health 2013, 13, 150. [Google Scholar] [CrossRef]
- Chinn, D. Critical Health Literacy: A Review and Critical Analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef]
- Pelikan, J.M.; Ganahl, K.; Roethlin, F. Health literacy as a determinant, mediator and/or moderator of health: Empirical models using the European Health Literacy Survey dataset. Glob. Health Promot. 2018, 25, 57–66. [Google Scholar] [CrossRef]
- Sørensen, K.; Karuranga, S.; Denysiuk, E.; McLernon, L. Health literacy and social change: Exploring networks and interests groups shaping the rising global health literacy movement. Glob. Health Promot. 2018, 25, 89–92. [Google Scholar] [CrossRef]
- Eichler, K.; Wieser, S.; Brügger, U. The Costs of Limited Health Literacy: A Systematic Review. Int. J. Public Health 2009, 54, 313–324. [Google Scholar] [CrossRef]
- Haun, J.N.; Patel, N.R.; French, D.D.; Campbell, R.R.; Bradham, D.D.; Lapcevic, W.A. Association between Health Literacy and Medical Care Costs in an Integrated Healthcare System: A Regional Population Based Study. BMC Health Serv. Res. 2015, 15, 249. [Google Scholar] [CrossRef]
- Palumbo, R. Examining the Impacts of Health Literacy on Healthcare Costs. An Evidence Synthesis. Health Serv. Manag. Res. 2017, 30, 197–212. [Google Scholar] [CrossRef]
- WHO–World Health Organization. Shanghai declaration on promoting health in the 2030 agenda for sustainable development. Health Promot. Int. 2017, 32, 7–8. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Carter, I. Human Behavior in the Social Environment: A Social Systems Approach, 6th ed.; Routledge: New York, NY, USA, 2017; Available online: https://www.taylorfrancis.com/books/9781351514699 (accessed on 13 December 2023).
- Rogers, A.T. Human Behavior in the Social Environment: Perspectives on Development, the Life Course, and Macro Contexts, 2nd ed.; Series: New directions in social work; Routledge: New York, NY, USA, 2020; Available online: https://www.taylorfrancis.com/books/9781000043778 (accessed on 13 December 2023).
- Agner, J.; Meyer, M.; Kaukau, T.M.; Liu, M.; Nakamura, L.; Botero, A.; Sentell, T. Health literacy, social networks, and health outcomes among mental health Clubhouse members in Hawai ‘i. Int. J. Environ. Res. Public Health 2023, 20, 837. [Google Scholar] [CrossRef] [PubMed]
- Achstetter, K.; Köppen, J.; Haltaufderheide, M.; Hengel, P.; Blümel, M.; Busse, R. Health literacy of people with substitutive private health insurance in Germany and their assessment of the health system performance according to Health Literacy Levels: Results from a survey. Int. J. Environ. Res. Public Health 2022, 19, 16711. [Google Scholar] [CrossRef]
- Beese, A.S.; Nicca, D.; Jaks, R.; Stuermer, N.; De Gani, S.M. How do primary care organizations rate their level of organizational health literacy? Results of a Swiss pilot-study. Int. J. Environ. Res. Public Health 2022, 19, 16139. [Google Scholar] [CrossRef] [PubMed]
- Dins, T.; Keeley, C. Recognizing basic health literacy capabilities: An explorative study on the relevance of health-related information in the support of people with profound intellectual and multiple disabilities. Int. J. Environ. Res. Public Health 2022, 19, 16874. [Google Scholar] [CrossRef]
- Jenkins, C.L.; Sykes, S.; Wills, J. Public libraries as supportive environments for children’s development of critical health literacy. Int. J. Environ. Res. Public Health 2022, 19, 11896. [Google Scholar] [CrossRef]
- Larsen, C.B.; Gilstad, H. Qualitative research studies addressing patient-practitioner communication about online health information. Int. J. Environ. Res. Public Health 2022, 19, 14004. [Google Scholar] [CrossRef]
- Li, C.; Liu, M.; Zhou, J.; Zhang, M.; Liu, H.; Wu, Y.; Deng, T. Do health information sources influence health literacy among older adults: A cross-sectional study in the urban areas of western China. Int. J. Environ. Res. Public Health 2022, 19, 13106. [Google Scholar] [CrossRef]
- Mather, C.A.; Cheng, C.; Douglas, T.; Elsworth, G.; Osborne, R. eHealth literacy of Australian undergraduate health profession students: A descriptive study. Int. J. Environ. Res. Public Health 2022, 19, 10751. [Google Scholar] [CrossRef]
- Phillips, M.M.; Weldon, R.H.; Maniar, A.; Patil, U.; Kostareva, U.; Agner, J.; Sentell, T. Social networks, health information sharing, and pandemic perceptions among young adults in Hawai’i during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 16833. [Google Scholar] [CrossRef] [PubMed]
- Stuermer, N.; De Gani, S.M.; Beese, A.S.; Giovanoli Evack, J.; Jaks, R.; Nicca, D. Health professionals’ experience with the first implementation of the Organizational Health Literacy Self-Assessment Tool for primary care (OHL Self-AsseT)—A qualitative reflexive thematic analysis. Int. J. Environ. Res. Public Health 2022, 19, 15916. [Google Scholar] [CrossRef]
- Vetter, N.S.; Ilskens, K.; Seidl, N.; Latteck, Ä.D.; Bruland, D. Health literacy of people with intellectual disabilities: How meaningful is the social context for a target group-oriented model of health literacy? Int. J. Environ. Res. Public Health 2022, 19, 16052. [Google Scholar] [CrossRef]
- Pitt, R.; Davis, T.; Manganello, J.; Massey, P.; Okan, O.; McFarlane, E.; Buchthal, O.; Davis, J.; Arnold, C.; Sentell, T. Health literacy in a social context: A meta-narrative review. In International Handbook of Health Literacy; Policy Press Bristol: Bristol, UK, 2019; pp. 665–688. [Google Scholar]
- Clausen, W.; Watanabe-Galloway, S.; Bill Baerentzen, M.; Britigan, D.H. Health Literacy Among People with Serious Mental Illness. Community Ment. Health J. 2016, 52, 399–405. [Google Scholar] [CrossRef]
- Krishan, S.; von Esenwein, S.A.; Druss, B.G. The Health Literacy of Adults with Severe Mental Illness. Psychiatr. Serv. 2012, 63, 397. [Google Scholar] [CrossRef]
- Albert, M.; Becker, T.; Mccrone, P.; Thornicroft, G. Social networks and mental health service utilization—A literature review. Intern. J. Soc. Psychiatry 1998, 44, 248–266. [Google Scholar] [CrossRef]
- Meyer, M.S.; Agner, J.; Botero, A.; Cha, T. Mapping community: A scoping review of clubhouse members’ social networks and their impact on recovery in mental illness. Psychiatr. Rehabil. J. 2023, 46, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Agner, J.; Barile, J.P.; Botero, A.; Cha, T.; Herrera, N.; Kaukau, T.M.; Nakamura, L.; Inada, M.; Coalition, H.C. Understanding the Role of Mental Health Clubhouses in Promoting Wellness and Health Equity Using Pilinahā—An Indigenous Framework for Health. Am. J. Community Psychol. 2020, 66, 290–301. [Google Scholar] [CrossRef]
- McKay, C.; Nugent, K.L.; Johnsen, M.; Eaton, W.W.; Lidz, C.W. A Systematic Review of Evidence for the Clubhouse Model of Psychosocial Rehabilitation. Adm. Policy Ment. Health 2018, 45, 28–47. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. On Intersectionality: Essential Writings; New Press: New York, NY, USA, 2019. [Google Scholar]
- Bauer, G.R.; Churchill, S.M.; Mahendran, M.; Walwyn, C.; Lizotte, D.; Villa-Rueda, A.A. Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods. SSM-Popul. Health 2021, 14, 100798. [Google Scholar] [CrossRef] [PubMed]
- Harari, L.; Lee, C. Intersectionality in quantitative health disparities research: A systematic review of challenges and limitations in empirical studies. Soc. Sci. Med. 2021, 277, 113876. [Google Scholar] [CrossRef]
- Gornick, M.E. Disparities in Medicare services: Potential causes, plausible explanations, and recommendations. Health Care Financ. Rev. 2000, 21, 23–43. [Google Scholar]
- Terraneo, M. Inequities in health care utilization by people aged 50+: Evidence from 12 European countries. Soc. Sci. Med. 2015, 126, 154–163. [Google Scholar] [CrossRef]
- Tessema, Z.T.; Yazachew, L.; Tesema, G.A.; Teshale, A.B. Determinants of postnatal care utilization in sub-Saharan Africa: A meta and multilevel analysis of data from 36 sub-Saharan countries. Ital. J. Pediatr. 2020, 46, 175. [Google Scholar] [CrossRef]
- Diviani, N.; van den Putte, B.; Giani, S.; van Weert, J.C.M. Low Health Literacy and Evaluation of Online Health Information: A Systematic Review of the Literature. J. Med. Internet Res. 2015, 17, e4018. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 2, e9. [Google Scholar] [CrossRef]
- Chaiken, S.R.; Han, L.; Darney, B.G.; Han, L. Factors associated with perceived trust of false abortion websites: Cross-sectional online survey. J. Med. Internet Res. 2021, 23, e25323. [Google Scholar] [CrossRef] [PubMed]
- McMullan, M. Patients Using the Internet to Obtain Health Information: How This Affects the Patient–Health Professional Relationship. Patient Educ. Couns. 2006, 63, 24–28. [Google Scholar] [CrossRef]
- Murray, E.; Lo, B.; Pollack, L.; Donelan, K.; Catania, J.; White, M.; Zapert, K.; Turner, R. The Impact of Health Information on the Internet on the Physician-Patient Relationship: Patient Perceptions. Arch. Intern. Med. 2003, 163, 1727–1734. [Google Scholar] [CrossRef]
- Pomputius, A. Putting misinformation under a microscope: Exploring technologies to address predatory false information online. Med. Ref. Serv. Q. 2019, 38, 369–375. [Google Scholar] [CrossRef]
- WHO–World Health Organization. Health Promotion Glossary. 1998. Available online: https://iris.who.int/bitstream/handle/10665/64546/WHO_HPR_HEP_98.1.pdf?sequence=1 (accessed on 20 October 2023).
- WHO–World Health Organization. Improving Health Literacy. 2023. Available online: https://www.who.int/health-promotion/enhanced-wellbeing/improving-health-literay (accessed on 20 October 2023).
- Paakkari, L.; Paakkari, O. Health literacy as a learning outcome in schools. Health Educ. 2012, 112, 133–152. [Google Scholar] [CrossRef]
- Brach, C.; Keller, D.; Hernandez, L.M.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D. Ten Attributes of Health Literate Health Care Organizations. In NAM Perspectives; Discussion Paper; National Academy of Medicine: Washington, DC, USA, 2012. [Google Scholar] [CrossRef]
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Community Health 2003, 57, 254–258. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Citation | N | Country | Population | Setting | Aim/Purpose |
|---|---|---|---|---|---|
| [39] | 163 | USA | People with serious mental illnesses attending Clubhouses | Mental health center | Examines the relationship between health literacy, social networks, self-efficacy, self-rated health, and stigma among people with serious mental illness in Hawai’i |
| [40] | 3601 | Germany | People with private health insurance | Healthcare | Examines “the health literacy of private health insurance insureds in Germany and analyze their assessment of the health system according to their health literacy level” (p. 1) |
| [41] | 74 | Switzerland | Primary care teams and healthcare professionals | Healthcare | “Assess organizational health literacy (OHL) in Swiss primary care organizations” (p. 1) |
| [42] | 125 | Germany | Disability care professionals and people with profound intellectual disabilities | Intellectual disabilities | Addresses the gap in approaches to communicate health-related needs and questions for people with profound intellectual disabilities |
| [43] | 32 | England | Children and public library staff | Public library | “Analyzes the potential of public libraries in England to be supportive environments for children’s development of critical health literacy” (p. 1) |
| [44] | 21 | Norway | Patients and providers | Healthcare | Summarizes existing studies examining patient and provider communication about online health information |
| [45] | 812 | China | Urban citizens aged 60 and older | Community | Explores “the link between health information sources and health literacy” among older adults (p. 1) |
| [46] | 610 | Australia | Undergraduate health profession students | University | Analyzes the online health literacy of Australian “health profession students to inform undergraduate curriculum development and promote work-readiness” (p. 1) |
| [47] | 324 | USA | Residents of Hawai’i aged 18–35 | Community | Explores “social network variation & health information sharing during COVID-19, especially for Native Hawaiians, other Pacific Islanders, and Filipinos who experienced COVID-19 inequities” (p. 1) |
| [48] | 19 | Switzerland | Primary care teams and healthcare professionals | Healthcare | Explores how an organizational health literacy assessment tool (OHL Self-AsseT) was implemented by primary care teams in Switzerland |
| [49] | 38 | Germany | People with mild to moderate intellectual disabilities | Community | Explores which dimensions influence the health literacy of people with intellectual disabilities |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agner, J.; Bau, K.E.; Bruland, D. An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers. Int. J. Environ. Res. Public Health 2024, 21, 240. https://doi.org/10.3390/ijerph21020240
Agner J, Bau KE, Bruland D. An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers. International Journal of Environmental Research and Public Health. 2024; 21(2):240. https://doi.org/10.3390/ijerph21020240
Chicago/Turabian StyleAgner, Joy, Katharine Elizabeth Bau, and Dirk Bruland. 2024. "An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers" International Journal of Environmental Research and Public Health 21, no. 2: 240. https://doi.org/10.3390/ijerph21020240