
How Is Telehealth Currently Being Utilized to Help in Hypertension Management within Primary Healthcare Settings? A Scoping Review

 ,
,  ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Background
2. Method
2.1. Research Questions
- What kind of interventions are carried out in the management of hypertension in PHC settings?
- What types of technology are used in the management of hypertension in PHC settings?
2.2. Research Strategy
2.3. Eligible Criteria
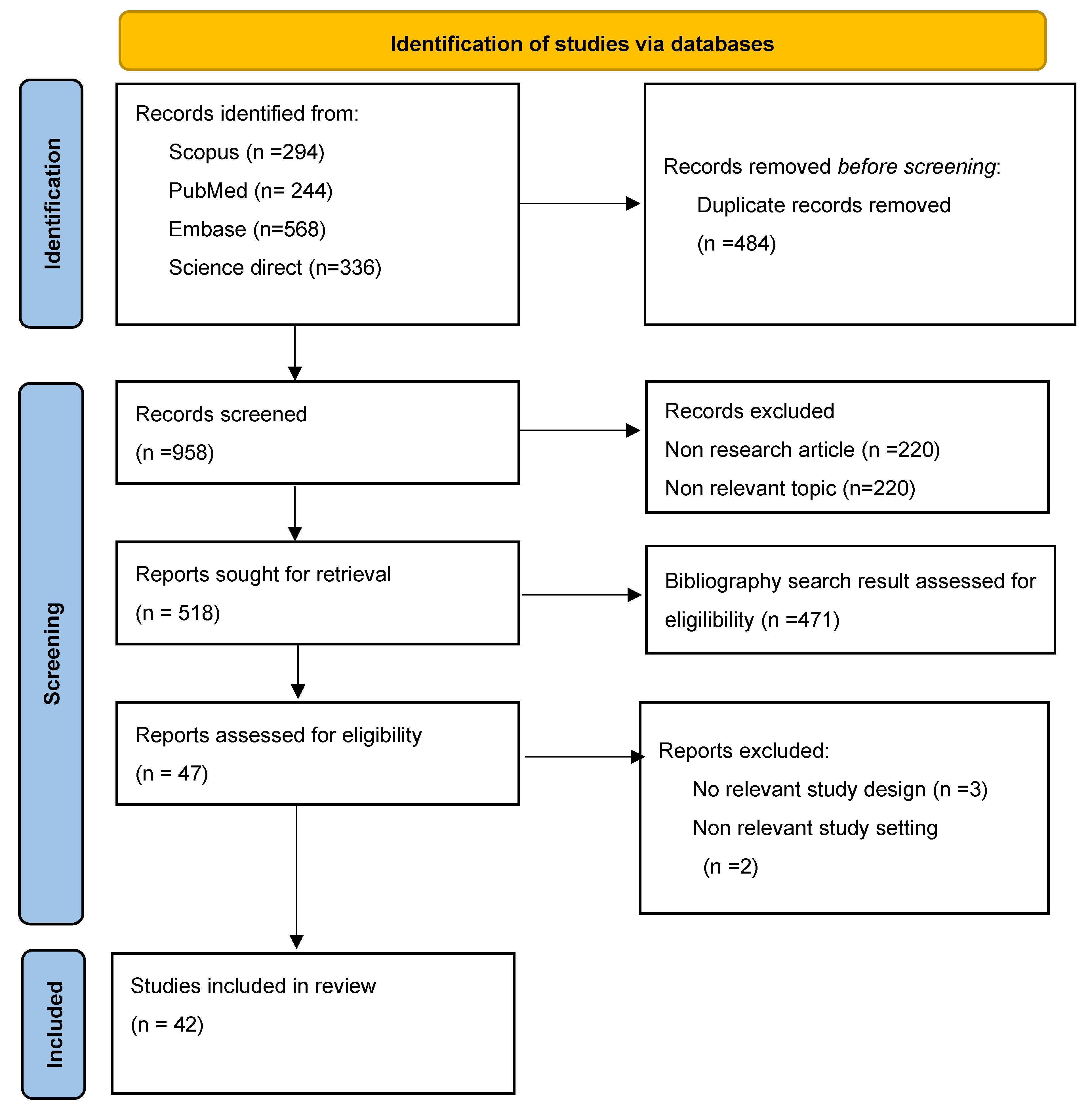
2.4. Study Selection
2.5. Data Extraction and Analysis
3. Results
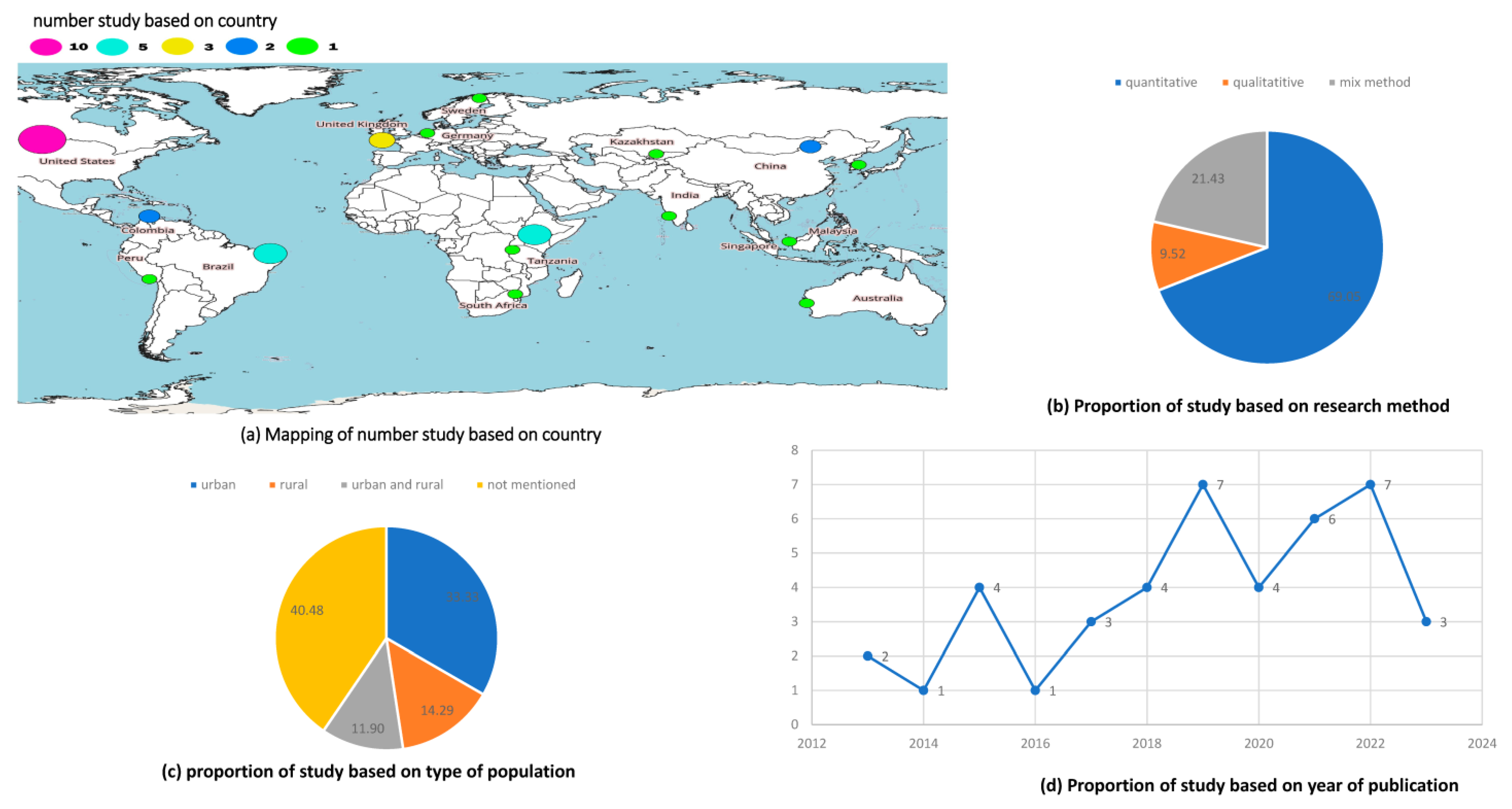
3.1. Characteristics of Study
3.2. Type of Intervention
3.3. Technology
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darvas, Z.; Moës, N.; Myachenkova, Y.; Pichler, D. The macroeconomic implications of healthcare. In Bruegel Policy Contribution; EconStor: Bruegel, Brussels, 2018. [Google Scholar]
- Hasan, A.A.; Ambrammal, S.K. The healthcare system: Policies and performance in India and ASEAN countries. Int. J. Health Sci. 2022, 6, 9960–9980. [Google Scholar] [CrossRef]
- Shin, J.-Y.J.; Man, K.; Zhou, W. International and global issues–differences in health systems, patient populations, and medical practice. In Pragmatic Randomized Clinical Trials; Elsevier: Amsterdam, The Netherlands, 2021; pp. 257–272. [Google Scholar]
- Baum, F.E. Health systems: How much difference can they make to health inequities? J. Epidemiol. Community Health 2016, 70, 635–636. [Google Scholar] [CrossRef]
- Uchimura, H. Introduction: Key Factors for Functioning Health Systems. In Making Health Services More Accessible in Developing Countries: Finance and Health Resources for Functioning Health Systems; Springer: Berlin/Heidelberg, Germany, 2009; pp. 1–21. [Google Scholar]
- Cancarevic, I.; Plichtová, L.; Malik, B.H. Healthcare systems around the world. In International Medical Graduates in the United States: A Complete Guide to Challenges and Solutions; Springer: Berlin/Heidelberg, Germany, 2021; pp. 45–79. [Google Scholar]
- Lu, W.; Yuan, J.; Liu, Z.; Su, Z.-H.; Shen, Y.-C.; Li, S.-J.; Zhang, H. Worldwide trends in mortality for hypertensive heart disease from 1990 to 2019 with projection to 2034: Data from the Global Burden of Disease 2019 study. Eur. J. Prev. Cardiol. 2023, 31, zwad262. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef] [PubMed]
- Hatano, Y.; Yano, Y.; Fujimoto, S.; Sato, Y.; Iseki, K.; Konta, T.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Narita, I.; et al. The Population-Attributable Fraction for Premature Mortality Due to Cardiovascular Disease Associated With Stage 1 and 2 Hypertension Among Japanese. Am. J. Hypertens. 2020, 34, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Mirahmadizadeh, A.; Vali, M.; Hassanzadeh, J.; Dehghani, S.P.; Razeghi, A.; Azarbakhsh, H. Mortality Rate and Years of Life Lost due to Hypertension in the South of Iran between 2004 and 2019: A Population-Based Study. Int. J. Hypertens. 2022, 2022, 7759699. [Google Scholar] [CrossRef]
- Chen, Y.; Freedman, N.D.; Albert, P.S.; Huxley, R.R.; Shiels, M.S.; Withrow, D.R.; Spillane, S.; Powell-Wiley, T.M.; de González, A.B. Association of Cardiovascular Disease with Premature Mortality in the United States. JAMA Cardiol. 2019, 4, 1230–1238. [Google Scholar] [CrossRef]
- Constant, A.; Geladari, E.V.; Geladari, C.V. The Economic Burden of Hypertension. In Hypertension and Cardiovascular Disease; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Djasri, H.; Laras, S.; Utarini, A. Quality indicators for clinical care of patients with hypertension: Scoping review protocol. BMJ Open 2019, 9, e026167. [Google Scholar] [CrossRef]
- Chowdhury, F.M.; Ayala, C.; Chang, T.E.; Dalmat, D.; Shantharam, S.; Zhang, X. Abstract 218: Effectiveness of Telehealth on Hypertension Management and Control Among Disparate Populations—A Systematic Review and Meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2018, 11, A218. [Google Scholar] [CrossRef]
- Gafane-Matemane, L.F.; Mokwatsi, G.G.; Boateng, D. Hypertension management in sub-Saharan Africa: An overview of challenges and opportunities for telemedicine. Connect. Health Telemed. 2023, 2, 9–22. [Google Scholar] [CrossRef]
- Cottrell, E.; Cox, T.; O’Connell, P.; Chambers, R. Implementation of simple telehealth to manage hypertension in general practice: A service evaluation. BMC Fam. Pract. 2015, 16, 83. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Panzeri, E.; Campolo, L. E-health in hypertension management: An insight into the current and future role of blood pressure telemonitoring. Curr. Hypertens. Rep. 2020, 22, 42. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Caserini, M.; Coronetti, C. Telemedicine and M-Health in Hypertension Management: Technologies, Applications and Clinical Evidence. High. Blood Press. Cardiovasc. Prev. 2016, 23, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Khan, S.; Khan, I.U.; Khan, S.U.; Xie, Y.; Li, X.; Zhang, G. Assessing the adoption of e-health technology in a developing country: An extension of the UTAUT model. Sage Open 2021, 11, 3. [Google Scholar] [CrossRef]
- Warr, D.; Luscombe, G.; Couch, D. Hype, evidence gaps and digital divides: Telehealth blind spots in rural Australia. Health 2023, 27, 588–606. [Google Scholar] [CrossRef] [PubMed]
- Sukkird, V.; Shirahada, K. E-health service model for Asian developing countries: A case of emergency medical service for elderly people in Thailand. In Optimizing Current Practices in E-Services and Mobile Applications; IGI Global: Hershey, PA, USA, 2018; pp. 214–232. [Google Scholar]
- Kaur, A.; Gupta, A.K. E-Health Approaches for Developing Countries. In Proceedings of the 2019 5th International Conference on Signal Processing, Computing and Control (ISPCC), Solan, India, 10–12 October 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 269–274. [Google Scholar]
- Suter, P.; Suter, W.N.; Johnston, D. Theory-Based Telehealth and Patient Empowerment. Popul. Health Manag. 2011, 14, 87–92. [Google Scholar] [CrossRef]
- Schwamm, L.H. Telehealth: Seven Strategies To Successfully Implement Disruptive Technology And Transform Health Care. Health Aff. 2014, 33, 200–206. [Google Scholar] [CrossRef]
- Wade, V.A.; Karnon, J.; Elshaug, A.G.; Hiller, J.E. A systematic review of economic analyses of telehealth services using real time video communication. BMC Health Serv. Res. 2010, 10, 233. [Google Scholar] [CrossRef]
- Hueppmeier, R.J.; Single, A.; Welte, I. Situation, motivation, implementation and results of telehealth-enabled health care. J. Telemed. Telecare 2010, 16, 187–189. [Google Scholar] [CrossRef]
- Lamothe, L.; Fortin, J.-P.; Labbé, F.; Gagnon, M.P.; Messikh, D. Impacts of telehomecare on patients, providers, and organizations. Telemed. J. e-Health 2006, 12, 363–369. [Google Scholar] [CrossRef]
- Wakefield, B.J.; Holman, J.E.; Ray, A.; Scherubel, M.; Adams, M.R.; Hillis, S.L.; Rosenthal, G.E. Effectiveness of home telehealth in comorbid diabetes and hypertension: A randomized, controlled trial. Telemed. J. e-Health 2011, 17, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Bingham, J.M.; Black, M.; Anderson, E.J.; Li, Y.; Toselli, N.; Fox, S.; Martin, J.R.; Axon, D.R.; Silva-Almodóvar, A. Impact of Telehealth Interventions on Medication Adherence for Patients With Type 2 Diabetes, Hypertension, and/or Dyslipidemia: A Systematic Review. Ann. Pharmacother. 2020, 55, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Melius, B.N.; Conwell, W.D. Impact of Telehealth on Health Economics. Sleep Med. Clin. 2020, 15, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M.G.; DiPette, D.J.; Campbell, N.R.C.; Angell, S.Y.; Ordunez, P. Developing population-based hypertension control programs. Rev. Panam. Salud Pública 2023, 46, e153. [Google Scholar] [CrossRef] [PubMed]
- Chu, R.Y.-K.; Dong, D.; Wong, S.Y.-S.; Lee, E.K.-P. Barriers and Determinants to the Underutilized Hypertension Screening in Primary Care Patients in Hong Kong: A Mixed-Method Study. Int. J. Environ. Res. Public Health 2023, 20, 985. [Google Scholar] [CrossRef]
- Elnaem, M.H.; Mosaad, M.; Abdelaziz, D.H.; Mansour, N.O.; Usman, A.; Elrggal, M.E.; Cheema, E. Disparities in prevalence and barriers to hypertension control: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 14571. [Google Scholar] [CrossRef]
- Abrahamowicz, A.A.; Ebinger, J.; Whelton, S.P.; Commodore-Mensah, Y.; Yang, E. Racial and Ethnic Disparities in Hypertension: Barriers and Opportunities to Improve Blood Pressure Control. Curr. Cardiol. Rep. 2023, 25, 17–27. [Google Scholar] [CrossRef]
- Benenson, I.; Prado, K. Difficult-to-Control Hypertension in a Primary Care Setting. J. Nurse Pract. 2023, 19, 104407. [Google Scholar] [CrossRef]
- Jackson, T.N.; Sreedhara, M.; Bostic, M.; Spafford, M.; Popat, S.; Beasley, K.L.; Jordan, J.; Ahn, R. Telehealth Use to Address Cardiovascular Disease and Hypertension in the United States: A Systematic Review and Meta-Analysis, 2011–2021. Telemed Rep. 2023, 4, 67–86. [Google Scholar] [CrossRef]
- Sreedhara, M.; Suvada, K.; Bostic, M.; Scott, A.; Blum, E.; Jordan, J.; Beasley, K.L. Rapid evaluations of telehealth strategies to address hypertension: A mixed-methods exploration at two US health systems during the COVID-19 pandemic. Prev. Chronic Dis. 2022, 19, E81. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.; Lewinski, A.A.; Rader, A.; Schexnayder, J.; Bosworth, H.B.; Goldstein, K.M.; Gierisch, J.; White-Clark, C.; McCant, F.; Zullig, L.L. Addressing Hypertension Outcomes Using Telehealth and Population Health Managers: Adaptations and Implementation Considerations. Curr. Hypertens. Rep. 2022, 24, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Y.; Chia, Y.; Cheng, H.; Van Minh, H.; Siddique, S.; Sogunuru, G.P.; Tay, J.C.; Teo, B.W.; Tsoi, K.; et al. Telemedicine in the management of hypertension: Evolving technological platforms for blood pressure telemonitoring. J. Clin. Hypertens. 2021, 23, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, J.; Yatabe, M.S.; Okada, R.; Ichihara, A. Efficacy of telemedicine in hypertension care through home blood pressure monitoring and videoconferencing: Randomized controlled trial. JMIR Cardio 2021, 5, e27347. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, L.; Kalankesh, L.; Doshmangir, L.; Farahbakhsh, M. Telehealth in Primary Health Care: A Scoping Review of the Literature. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9013222/ (accessed on 3 May 2023).
- Harrison, C.E. Using telehealth in the management of hypertension. Nurs. Stand. 2017, 31, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Clarke, V.; Braun, V.; Hayfield, N. Thematic analysis. In Qualitative Psychology: A Practical Guide to Research Methods; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2015; Volume 3, pp. 222–248. [Google Scholar]
- Barsky, J.; Hunter, R.; McAllister, C.; Yeates, K.; Campbell, N.; Liu, P. Analysis of the Implementation, User Perspectives, and Feedback from a Mobile Health Intervention for Individuals Living with Hypertension (DREAM-GLOBAL): Mixed Method Study. Available online: https://mhealth.jmir.org/2019/12/e12639 (accessed on 3 May 2023).
- Naqvi, I.; Cheung, K.; Strobino, K.; Li, J.; Schmitt, K.; Garcon, M.; Li, H. Home blood pressure telemonitoring-enhanced versus usual post-acute stroke care in an underserved setting: The telehealth after stroke care pilotrandomized clinical trial. Neurology 2022, 98, S17. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L638416316&from=export (accessed on 8 October 2023). [CrossRef]
- Vedanthan, R.; Blank, E.; Tuikong, N.; Kamano, J.; Misoi, L.; Tulienge, D. Usability and feasibility of a tablet-based Decision-Support and Integrated Record-keeping (DESIRE) tool in the nurse management of hypertension in rural western Kenya. Int. J. Med. Inform. 2015, 84, 207–219. [Google Scholar] [CrossRef]
- Dos Santos, M.V.R.; Cavalcanti De Oliveira, D.; De Araújo Novaes, M. A telehealth strategy for increasing adherence in the treatment of hypertension in primary care. Telemed. e-Health 2013, 19, 241–247. [Google Scholar] [CrossRef]
- Buis, L.R.; Roberson, D.N.; Kadri, R.; Rockey, N.G.; A Plegue, M.; Danak, S.U.; Guetterman, T.C.; Johnson, M.G.; Choe, H.M.; Richardson, C.R. Understanding the feasibility, acceptability, and efficacy of a clinical pharmacist-led mobile approach (BPTrack) to hypertension management: Mixed methods pilot study. J. Med. Internet Res. 2020, 22, e19882. [Google Scholar] [CrossRef]
- Koopman, R.J.; Wakefield, B.J.; Johanning, J.L.; Keplinger, L.E.; Kruse, R.L.; Bomar, M.; Bernt, B.; Wakefield, D.S.; Mehr, D.R. Implementing home blood glucose and blood pressure telemonitoring in primary care practices for patients with diabetes: Lessons learned. Telemed. e-Health 2014, 20, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.A.; Paterson, M.; Padfield, P.; Pinnock, H.; Hanley, J.; Hammersley, V.S.; Steventon, A.; McKinstry, B. Are self-reported telemonitored blood pressure readings affected by end-digit preference: A prospective cohort study in Scotland. BMJ Open 2018, 8, e019431. [Google Scholar] [CrossRef] [PubMed]
- Fisher, N.D.L.; Fera, L.E.; Dunning, J.R.; Desai, S.; Matta, L.; Liquori, V. Development of an entirely remote, non-physician led hypertension management program. Clin. Cardiol. 2019, 42, 285–291. [Google Scholar] [CrossRef]
- Ma, Y.; Cheng, H.Y.; Sit, J.W.H.; Chien, W.T. The effects of a smartphone-enhanced nurse-facilitated self-care intervention for Chinese hypertensive patients: A randomised controlled trial. Int. J. Nurs. Stud. 2022, 134, 104313. [Google Scholar] [CrossRef]
- Levine, D.M.; Dixon, R.F.; Linder, J.A. Association of Structured Virtual Visits for Hypertension Follow-Up in Primary Care with Blood Pressure Control and Use of Clinical Services. J. Gen. Intern. Med. 2018, 33, 1862–1867. [Google Scholar] [CrossRef] [PubMed]
- Ashjian, E.J.; Yoo, A.; Piette, J.D.; Choe, H.M.; Thompson, A.N. Implementation and barriers to uptake of interactive voice response technology aimed to improve blood pressure control at a large academic medical center. J. Am. Pharm. Assoc. 2019, 59, S104–S109.e1. [Google Scholar] [CrossRef]
- De Luca, V.; Lazic, V.; Birov, S.; Piesche, K.; Beyhan, O.; Pengo, M.F.; Melgara, M.; Sherman, M.H.; Lilja, M.; Balenovic, A.; et al. Digitally enabled health service for the integrated management of hypertension: A participatory user-centred design process. Int. J. Environ. Res. Public Health 2021, 18, 12442. [Google Scholar] [CrossRef]
- Chen, B.; Dou, Y.; Yu, X.; Ma, D. Influence of Internet-Based Health Management on Control of Clinical Parameters in Patients with Hypertension: Four-Year Longitudinal Study. J. Med. Internet Res. 2023, 25, e42896. [Google Scholar] [CrossRef]
- Jindal, D.; Gupta, P.; Jha, D.; Ajay, V.S.; Goenka, S.; Jacob, P.; Mehrotra, K.; Perel, P.; Nyong, J.; Roy, A.; et al. Development of mWellcare: An mHealth intervention for integrated management of hypertension and diabetes in low-resource settings. Glob. Health Action 2018, 11, 1517930. [Google Scholar] [CrossRef]
- Doocy, S.; Paik, K.E.; Lyles, E.; Tam, H.H.; Fahed, Z.; Winkler, E.; Kontunen, K.; Mkanna, A.; Burnham, G. Guidelines and mhealth to improve quality of hypertension and type 2 diabetes care for vulnerable populations in Lebanon: Longitudinal cohort study. JMIR mHealth uHealth 2017, 5, e158. [Google Scholar] [CrossRef]
- Leon, N.; Surender, R.; Bobrow, K.; Muller, J.; Farmer, A. Improving treatment adherence for blood pressure lowering via mobile phone SMS-messages in South Africa: A qualitative evaluation of the SMS-text Adherence SuppoRt (StAR) trial Service organization, utilization, and delivery of care. BMC Fam. Pract. 2015, 16, 80. [Google Scholar] [CrossRef]
- Buis, L.; Hirzel, L.; Dawood, R.M.; Dawood, K.L.; Nichols, L.P.; Artinian, N.T.; Schwiebert, L.; Yarandi, H.N.; Roberson, D.N.; Plegue, M.A.; et al. Text messaging to improve hypertension medication adherence in african americans from primary care and emergency department settings: Results from two randomized feasibility studies. JMIR mHealth uHealth 2017, 5, e9. [Google Scholar] [CrossRef] [PubMed]
- Ju, H.; Kang, E.; Kim, Y.; Ko, H.; Cho, B. The Effectiveness of a Mobile Health Care App and Human Coaching Program in Primary Care Clinics: Pilot Multicenter Real-World Study. JMIR mHealth uHealth 2022, 10, e34531. [Google Scholar] [CrossRef]
- Nurakysh, S.; Kurakbayev, K.; Kosherbaeva, L.; Tazhiyeva, A.; Aimakhanova, A.; Kulkaeva, G.; Asykbaeva, L.; Ainabekov, M.; Fakhradiyev, I.; Tanabayeva, S. Evaluation of the Effectiveness of the Mobile Application on Adherence of Patients With Arterial Hypertension. Acta Inform. Medica 2022, 30, 18–24. [Google Scholar] [CrossRef]
- Manusov, E.G.; Diego, V.P.; Smith, J.; Garza, J.R.; Lowdermilk, J.; Blangero, J.; Williams-Blangero, S.; Fernandez, F. UniMóvil: A Mobile Health Clinic Providing Primary Care to the Colonias of the Rio Grande Valley, South Texas. Front. Public Health 2019, 7, 215. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.S.; Anastos-Wallen, R.; Chaiyachati, K.H.; Reitz, C.; Asch, D.A.; Mehta, S.J. Clinician Decisions after Notification of Elevated Blood Pressure Measurements from Patients in a Remote Monitoring Program. JAMA Netw. Open 2022, 5, e2143590. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; Cimini, C.C.R.; Maia, J.X.; Pinto, V.S.O.A.; Sá, T.Q.V.; Amancio, K.; Coelho, L.; Ribeiro, L.B.; Cardoso, C.S.; et al. Development and Implementation of a Decision Support System to Improve Control of Hypertension and Diabetes in a Resource-Constrained Area in Brazil: Mixed Methods Study. J. Med. Internet Res. 2021, 23, e18872. [Google Scholar] [CrossRef]
- Peters, R.M.; Shivakumar, N.; Xu, R.; Javaherian, K.; Sink, E.; Patel, K.; Brown, A.; Huynh, J.; Blanchard, M.; Ross, W.; et al. Assessing the utility of a novel SMS- And phone-based system for blood pressure control in hypertensive patients: Feasibility study. JMIR Cardio 2017, 1, e2. [Google Scholar] [CrossRef]
- Debon, R.; Bellei, E.A.; Biduski, D.; Volpi, S.S.; Alves, A.L.S.; Portella, M.R.; De Marchi, A.C.B. Effects of using a mobile health application on the health conditions of patients with arterial hypertension: A pilot trial in the context of Brazil’s Family Health Strategy. Sci. Rep. 2020, 10, 6009. [Google Scholar] [CrossRef]
- Davoudi, A.; Lee, N.S.; Chivers, C.; Delaney, T.; Asch, E.L.; Reitz, C.; Mehta, S.J.; Chaiyachati, K.H.; Mowery, D.L. Patient interaction phenotypes with an automated remote hypertension monitoring program and their association with blood pressure control: Observational study. J. Med. Internet Res. 2020, 22, e22493. [Google Scholar] [CrossRef] [PubMed]
- McManus, R.J.; Little, P.; Stuart, B.; Morton, K.; Raftery, J.; Kelly, J.; Bradbury, K.; Zhang, J.; Zhu, S.; Murray, E.; et al. Home and Online Management and Evaluation of Blood Pressure (HOME BP) using a digital intervention in poorly controlled hypertension: Randomised controlled trial. BMJ 2021, 372, m4858. [Google Scholar] [CrossRef]
- Chew, E.; Teo, S.H.; Tang, W.E.; Ng, D.W.L.; Koh, G.C.H.; Teo, V.H.Y. Trust and Uncertainty in the Implementation of a Pilot Remote Blood Pressure Monitoring Program in Primary Care: Qualitative Study of Patient and Health Care Professional Views. JMIR Hum. Factors 2023, 10, e36072. [Google Scholar] [CrossRef] [PubMed]
- Andersson, U.; Bengtsson, U.; Ranerup, A.; Midlöv, P.; Kjellgren, K. Patients and Professionals as Partners in Hypertension Care: Qualitative Substudy of a Randomized Controlled Trial Using an Interactive Web-Based System Via Mobile Phone. J. Med. Internet Res. 2021, 23, e26143. [Google Scholar] [CrossRef] [PubMed]
- Kassavou, A.; Houghton, V.; Edwards, S.; Brimicombe, J.; Sutton, S. Development and piloting of a highly tailored digital intervention to support adherence to antihypertensive medications as an adjunct to primary care consultations. BMJ Open 2019, 9, e024121. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, E.; Cox, T.; O’Connell, P.; Chambers, R. Patient and professional user experiences of simple telehealth for hypertension, medication reminders and smoking cessation: A service evaluation. BMJ Open 2015, 5, e007270. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.; Liew, S.M.; Hanafi, N.S.; Ng, C.J.; Lai, P.S.M.; Chia, Y.C.; Kiong, L.C. What influences patients’ acceptance of a blood pressure telemonitoring service in primary care? A qualitative study. Patient Prefer. Adherence 2016, 10, 99–106. [Google Scholar] [CrossRef]
- Nau, T.; Owen, A.; Mazza, D.; Smith, B.J. Engaging primary care providers in a mobile health strategy to support lifestyle change and blood pressure management. Digit. Health 2021, 7, 205520762110667. [Google Scholar] [CrossRef]
- Ye, S.; Anstey, D.E.; Grauer, A.; Metser, G.; Moise, N.; Schwartz, J.; Kronish, I.; Abdalla, M. The Impact of Telemedicine Visits on the Controlling High Blood Pressure Quality Measure During the COVID-19 Pandemic: Retrospective Cohort Study. JMIR Form. Res. 2022, 6, e32403. [Google Scholar] [CrossRef]
- Calderón-Anyosa, R.; Tincopa, J.P.; Raza, M.; Cárcamo, C.P. Randomized Controlled Trial of Home Telemonitoring of Blood Pressure with an Adapted Tensiometer with SMS Capability. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 440–449. [Google Scholar] [CrossRef]
- Sin, D.Y.E.; Guo, X.; Yong, D.W.W.; Qiu, T.Y.; Moey, P.K.S.; Falk, M.-R.; Tan, N.C. Assessment of willingness to Tele-monitoring interventions in patients with type 2 diabetes and/or hypertension in the public primary healthcare setting. BMC Med. Inform. Decis. Mak. 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Cimini, C.C.R.; Maia, J.X.; Pires, M.C.; Ribeiro, L.B.; e Almeida, V.S.D.O.; Batchelor, J. Pandemic-Related Impairment in the Monitoring of Patients With Hypertension and Diabetes and the Development of a Digital Solution for the Community Health Worker: Quasiexperimental and Implementation Study. JMIR Med. Inform. 2022, 10, e35216. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Kaufman, M.A.; Bosworth, H.B.; Weiner, B.J.; Zullig, L.L.; Lee, S.-Y.D.; Kravetz, J.D.; Rakley, S.M.; Roumie, C.L.; E Bowen, M.; et al. Organizational factors associated with readiness to implement and translate a primary care based telemedicine behavioral program to improve blood pressure control: The HTN-IMPROVE study. Implement. Sci. 2013, 8, 106. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.; Hodgkinson, J.; Schwartz, C.; Bradburn, P.; Franssen, M.; Hobbs, F.R.; Jowett, S.; McManus, R.J.; Greenfield, S. Using mHealth for the management of hypertension in UK primary care: An embedded qualitative study of the TASMINH4 randomised controlled trial. Br. J. Gen. Pract. 2019, 69, e612–e620. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.; Farah, A.; El Arnaout, N.; Dimassi, H.; El Morr, C.; Muntaner, C. mHealth use for non-communicable diseases care in primary health: Patients’ perspective from rural settings and refugee camps. J. Public Health 2018, 40, ii52–ii63. [Google Scholar] [CrossRef] [PubMed]
- Vitório Silveira, D.; Marcolino, M.S.; Machado, E.L.; Ferreira, C.G.; Alkmim, M.B.M.; Resende, E.S.; Carvalho, B.C.; Antunes, A.P.; Ribeiro, A.L.P. Development and evaluation of a mobile decision support system for hypertension management in the primary care setting in Brazil: Mixed-methods field study on usability, feasibility, and utility. JMIR mHealth uHealth 2019, 7, e9869. [Google Scholar] [CrossRef] [PubMed]
- Teo, V.H.Y.; Teo, S.H.; Burkill, S.M.; Wang, Y.; AL Chew, E.; Ng, D.W.; Tang, W.E.; Koh, G.C. Effects of technology-enabled blood pressure monitoring in primary care: A quasi-experimental trial. J. Telemed. Telecare 2021, 30, 121–130. [Google Scholar] [CrossRef]
- Neculau, A.E.; Lăcătuș, A.M.; Mărginean, M. A Guide to Telemedicine in Primary Healthcare; UNICEF: New York, NY, USA, 2022; p. 44. [Google Scholar]
- Mechanic, O.J.; Persaud, Y.; Kimball, A.B. Telehealth Systems; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Omboni, S.; McManus, R.J.; Bosworth, H.B.; Chappell, L.C.; Green, B.B.; Kario, K. Evidence and Recommendations on the Use of Telemedicine for the Management of Arterial Hypertension: An International Expert Position Paper. Hypertension 2020, 76, 1368–1383. Available online: https://api.semanticscholar.org/CorpusID:221672050 (accessed on 8 July 2023). [CrossRef]
- Sivakumaran, D.; Earle, K.A. Telemonitoring: Use in the management of hypertension. Vasc. Health Risk Manag. 2014, 10, 217–224. [Google Scholar]
- Hammersley, V.; Parker, R.; Paterson, M.; Hanley, J.; Pinnock, H.; Padfield, P.; Stoddart, A.; Park, H.G.; Sheikh, A.; McKinstry, B. Telemonitoring at scale for hypertension in primary care: An implementation study. PLoS Med. 2020, 17, e1003124. [Google Scholar] [CrossRef]
- Purcell, R.; McInnes, S.; Halcomb, E.J. Telemonitoring can assist in managing cardiovascular disease in primary care: A systematic review of systematic reviews. BMC Fam. Pract. 2014, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- AbuDagga, A.; Resnick, H.E.; Alwan, M. Impact of blood pressure telemonitoring on hypertension outcomes: A literature review. Telemed. J. e-Health Off. J. Am. Telemed. Assoc. 2010, 16, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Heizelman, R.J. Telehealth and Hypertension Management. Prim. Care Clin. Off. Pract. 2022, 49, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Carrillo de Albornoz, S.; Sia, K.-L.; Harris, A. The effectiveness of teleconsultations in primary care: Systematic review. Fam. Pract. 2022, 39, 168–182. [Google Scholar] [CrossRef]
- Dhillon, H.S.; Doermann, A.C.; Walcoff, P. Telemedicine and rural primary health care: An analysis of the impact of telecommunications technology. Socioecon. Plann Sci. 1978, 12, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Marcolino, M.S.; Pereira Afonso dos Santos, J.; Neves, D.S.; Alkmim, M.B.M. Teleconsultations to Provide Support for Primary Care Practitioners and Improve Quality of care--the Experience of a Large Scale Telehealth Service in Brazil. Stud. Health Technol. Inform. 2015, 216, 987. [Google Scholar]
- Zanaboni, P.; Scalvini, S.; Bernocchi, P.; Borghi, G.; Tridico, C.; Masella, C. Teleconsultation service to improve healthcare in rural areas: Acceptance, organizational impact and appropriateness. BMC Health Serv. Res. 2009, 9, 238. [Google Scholar] [CrossRef]
- Pandian, P.S.; Safeer, K.P.; Shakunthala, D.T.I.; Gopal, P.; Padaki, V.C. Store and Forward Applications in Telemedicine for Wireless IP Based Networks. J. Netw. 2007, 2, 58–65. [Google Scholar] [CrossRef]
- Jazayeri, D.G. TeleMedMail: A Low-Cost Store-and-Forward Telemedicine System for Use in Developing Countries. Doctoral Dissertation, Massachusetts Institute of Technology, Cambridge, MA, USA, 2002. Available online: https://api.semanticscholar.org/CorpusID:110433436 (accessed on 8 July 2023).
- Lewis, P.A.; Mccann, R.L.; Hidalgo, P.; Gorman, M. Use of store and forward technology for vascular nursing teleconsultation service. J. Vasc. Nurs. 1997, 15, 116–123. [Google Scholar] [CrossRef]
- Deshpande, A.; Khoja, S.; Lorca, J.; McKibbon, A.; Rizo, C.; Husereau, D.; Jadad, A.R. Asynchronous telehealth: A scoping review of analytic studies. Open Med. 2009, 3, e69–e91. [Google Scholar]
- Karam, S.; Drawz, P.E. Telemonitoring for Hypertension Management: The Time Is Now. Kidney360 2022, 3, 1961. [Google Scholar] [CrossRef] [PubMed]
- Dopp, J.M.; Lange, A.; Maursetter, L. Interdisciplinary telehealth team positively impacts difficult-to-control hypertension in CKD. Kidney360 2023, 4, e817–e823. [Google Scholar] [CrossRef] [PubMed]
- Papanicolas, I.; Cylus, J. Comparison of healthcare systems performance. In The Palgrave International Handbook of Healthcare Policy and Governance; Springer: Berlin/Heidelberg, Germany, 2015; pp. 116–132. [Google Scholar]
- Wang, F.; Wang, J.-D. The determinants of telehealth provision: Empirical evidence from OECD countries. Int. J. Environ. Res. Public Health 2021, 18, 8288. [Google Scholar] [CrossRef] [PubMed]
- Alverson, D. The international digital transformation of healthcare: Telehealth development in the global community. J. Int. Soc. Telemed. e-Health 2020, 8, e13. [Google Scholar] [CrossRef]
- Ramnath, V.R. Global telehealth and digital health: How to support programs and infrastructure. In Emerging Practices in Telehealth; Elsevier: Amsterdam, The Netherlands, 2023; pp. 163–182. [Google Scholar]



{kind=link}
{kind=link}
| Databases | Keywords and Query |
|---|---|
| PubMed | “Telemedicine” [Mesh] OR “Mobile health” [tw] OR mHealth [tw] OR eHealth [tw] OR “Tele-Referral” [tw] OR Tele Referral [tw] Filters: in the last 10 years “Hypertension” [Mesh] OR “hypertensi” [tw] OR “high blood pressure” [tw] Filters: in the last 10 years “Primary Health Care” [Mesh] OR “primary health care” [tw] OR “primary care” [tw] Filters: in the last 10 years |
| Scopus | (TITLE-ABS-KEY (telemedicine) or title-abs-key (“mobile health”) or title-abs-key (mhealth) or title-abs-key (ehealth) or title-abs-key (tele referral) and title-abs-key (hypertension) or title-abs-key (“high blood pressure”) and title-abs-key (“primary health care”) or title-abs-key (“primary care”)) and pubyear > 2012 and pubyear > 2012 |
| Science direct | “high blood pressure” AND telemedicine OR “mobile health” OR “eHealth” AND “primary health care” |
| Embase | ((‘high blood pressure’/exp OR ‘high blood pressure’ OR ‘hypertension’/exp OR hypertension) AND (‘telemedicine’/exp OR telemedicine) OR ‘mobile health’/exp OR ‘mobile health’ OR ‘ehealth’/exp OR ehealth) AND (‘primary health care’/exp OR ‘primary health care’) AND ((controlled clinical trial)/lim OR (randomized controlled trial)/lim) AND (2013–2023)/py |
| Author | Year | Participant Subject | Intervention | Population Type | Type of Technology | Purpose of Telehealth | Type of Study | Number Primary Healthcare | Country | Tool of Hardware/Software | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Barsky et al. [47] | 2019 | Canadian Aboriginal and Tanzanian communities | SMS-text-messaging-based system for blood pressure measurement and hypertension management | rural | Mobile health (SMS text messaging) | Monitoring blood pressure | mixed methods | n/a | Canada and East Africa | wireless, Bluetooth |
|
| Naqvi et al. [48] | 2022 | Acute stroke patients with hypertension | TASC (Telehealth After Stroke Care) | Urban | home blood pressure telemonitoring | Monitoring blood pressure | Pilot randomized trial | n/a | Northern Manhattan | Tablet and monitor |
|
| Vedanthan et al. [49] | 2015 | nurses | Tablet-based Decision Support and Integrated Record keeping (DESIRE) tool | rural | Mobile health (mHealth) | management of hypertension | investigative study | n/a | Rural Western Kenya | tablet |
|
| Dos Santos et al. [50] | 2013 | professionals and hypertensive patients | Education program | rural | Web conference | Increase the adherence to the treatment of hypertension. | before–after study | 2 | Brazil | n/a |
|
| Buis et al. [51] | 2020 | people with hypertension, medical assistants, physicians, a nurse, and the current and former director of the Family Medicine clinic | BPTrack | urban and rural | Mobile health (mHealth) | Home blood pressure monitoring | pre-post pilot study | 1 | USA | mobile applications |
|
| Koopman et al. [52] | 2014 | patients, nurses, and physicians | Home blood pressure telemonitoring | n/a | Electronic medical record and home blood pressure telemonitoring | blood pressure monitoring | qualitative study | 6 | South America | USB computer connection, dedicated telemonitoring device with an analog phone line |
|
| Parker et al. [53] | 2018 | hypertension patients | text based telemonitoring system | n/a | Home blood pressure telemonitoring | blood pressure monitoring | prospective cohort study | 37 | South-East Scotland | automatic-transmission system |
|
| Fisher et al. [54] | 2019 | hypertension patients | A home-based BP control program | n/a | telemonitoring | blood pressure monitoring | prospective cohort implementation | n/a | USA | home monitors |
|
| Ma et al. [55] | 2022 | Chinese hypertensive patients | Smartphone-enhanced nurse-facilitated self-care intervention | urban | mobile health | hypertension management | Randomized controlled trial with a repeated-measures design | 2 | China | smartphone |
|
| Levine et al. [56] | 2018 | primary care patients with hypertension | virtual visits | n/a | asynchronous online | hypertension management | propensity-score-matched, retrospective cohort study with adjustment by difference in differences | n/a | USA | n/a |
|
| Ashjian et al. [57] | 2019 | hypertensive patients | an interactive voice response (IVR) | n/a | Electronic health record | home blood pressure monitoring | observational study | 14 | USA | Aspect Patient Engagement Solution and Microsoft Dynamics 365 platforms |
|
| De Luca et al. [58] | 2021 | patients diagnosed with hypertension and professionals | integrated management hypertension | n/a | digitally enabled integrated approach (HER), smartphone, computer | hypertension management | user-centered approach | n/a | Europe | n/a |
|
| Chen et al. [59] | 2023 | individual | online health management | urban | internet based | hypertension management | longitudinal study | n/a | China | n/a |
|
| Jindal et al. [60] | 2018 | people with hypertension and diabetes along with comorbid conditions | Smartphone application (mWellcare) | rural | mobile health | integrated management of hypertension | n/a | 5 | India | tablet-computer-based application |
|
| Doocy et al. [61] | 2017 | people aged 40 years or older with hypertension | Mobile health app | urban | mobile health | improve adherence to guidelines and quality of care | a longitudinal cohort study | 10 | Lebanon | tablets |
|
| Leon et al. [62] | 2015 | female and male participants in South Africa aged 36 to 78 years old | SMS texts | n/a | mobile health | improve adherence to clinic visits and treatment | an individually randomized controlled trial | 1 | South Africa | Mobile phone |
|
| Buis et al. [63] | 2017 | African American patients with uncontrolled hypertension | automated text message | urban | mobile health | improve medication adherence among African Americans with uncontrolled HTN | unblinded randomized controlled pilot trials | 2 | USA | n/a |
|
| Cottrell et al. [17] | 2015 | patients and clinicians in a national primary care population in England | Text messaging (‘Florence’) | n/a | mobile health | for diagnosis and management hypertension | evaluation study | n/a | UK | Mobile phone |
|
| Ju et al. [64] | 2022 | Patients aged ≥19 years were diagnosed with hypertension, diabetes, dyslipidemia, or metabolic syndrome | mobile self-management healthcare app | n/a | Mobile health | management of chronic conditions | pilot multicenter real world study | 17 | Republic of Korea | mobile app |
|
| Nurakysh et al. [65] | 2022 | patients with diagnosed arterial hypertension | Mobile application “MyTherapy” | n/a | mobile health | evaluation of the degree of adherence of patients determined to have hypertension to treatment | a multicenter randomized controlled study | 1 | Kazakhstan | mobile phone app |
|
| Manusov et al. [66] | 2019 | people with chronic illness, obesity, hypertension, hypercholesterolemia, hypertriglyceridemia, and depression | UniMóvil, a mobile health clinic | rural | mobile health | improve poor healthcare access delivery | a retrospective review of the cohort | 1 | USA | n/a |
|
| Lee et al. [67] | 2022 | people aged 18 to 75 years, predominantly female, within the University of Pennsylvania Health Systems | remote blood pressure monitoring | urban | Electronic health record | remote blood pressure monitoring | cohort study | n/a | USA | n/a |
|
| Marcolinoet al. [68] | 2021 | people in Brazil, 71% of which were female, consisting of physicians and nurses | teleconsultation | urban and rural | Asynchronous | hypertension management | mixed methods | 34 | Brazil | Web-based |
|
| Peters et al. [69] | 2017 | hypertensive patients aged above 18 years | phone call and short-message-service text messaging | n/a | mobile health | blood pressure control | quality improvement study | 1 | USA | Mobile phone |
|
| Debon et al. [70] | 2020 | female humans in Brazil with arterial hypertension who were workers or retirees | use of a mobile health app | n/a | mobile health | monitoring patients with arterial hypertension (AH) | a non-randomized, controlled, non-blind trial | n/a | Brazil | smartphone |
|
| Davoudi et al. [71] | 2020 | adults with poorly controlled hypertension | an automated text messaging | n/a | mobile health | hypertension management | secondary analysis of data from a randomized controlled trial | 1 | USA | n/a |
|
| McManuset al. [72] | 2021 | people with treated but poorly controlled hypertension (>140/90 mm Hg) and access to the internet | Home and Online Management | n/a | Home blood pressure telemonitoring | hypertension management | randomized controlled trial | 76 | UK | Omron |
|
| Chew et al. [73] | 2023 | patients and clinical staff | a remote blood pressure monitoring program | urban | Home blood pressure telemonitoring | blood pressure monitoring | a secondary qualitative study | n/a | Singapura | a Bluetooth-enabled device |
|
| Anderssonet al. [74] | 2021 | patients and 15 professionals | interactive web-based system | Urban and rural | mobile health | strengthening patients’ potential for self-management | qualitative substudy of a randomized controlled trial | n/a | Sweden | Mobile phone |
|
| Kassavou et al. [75] | 2019 | healthcare providers, commissioners, and patients with either hypertension or both hypertension and type 2 diabetes | highly tailored text and voice message | n/a | mobile health | to increase adherence to medication in primary care | descriptive and interventional study | n/a | UK—England | Mobile phone |
|
| Cottrell et al. [76] | 2015 | patients and professional users in England with hypertension, CKD, and diabetes | text messages | n/a | mobile health | support self-management and education using technology with which patients are already familiar | evaluation study | 425 | UK | Mobile phone |
|
| Abdullah et al. [77] | 2016 | patients with hypertension and comorbidities | a blood pressure telemonitoring service | urban | home BP telemonitoring | blood pressure monitoring | a qualitative study design | n/a | Malaysia | MediHome Digital Blood Pressure and Pulse Oximeter 2-in-1 Monitor |
|
| Nau et al. [78] | 2021 | patients aged 40–70 years | videos, web-based education, and text message | urban | mobile health | To support patients with improving lifestyle behaviors for high blood pressure | pilot study | n/a | Australia | Mobile phone |
|
| Ye et al. [79] | 2022 | patients with hypertension aged between 18 and 85 years | video and telephone | urban | telemedicine visit | controlling high blood pressure | retrospective cohort study | n/a | South America | n/a |
|
| Calderón et al. [80] | 2023 | patient with hypertension | SMS-based home BP telemonitoring system | urban | home bp telemonitoring | helps improve adherence to treatment, also improving disease awareness | randomized controlled trial | 1 | Peru | omron |
|
| Sin et al. [81] | 2020 | People aged 21–70 years old in Singapore with Type 2 DM and/or hypertension | Telemonitoring | urban | telemonitoring | diabetes and hypertension management | cross-sectional survey | 2 | Singapura | n/a |
|
| Cimini et al. [82] | 2022 | primary care physicians, one nurse, one pharmacist, and one community health worker | a digital solution with a decision support system (DSS) for community health workers (CHWs) | n/a | telemedicine with video consultations | To address and identify at risk patients with uncontrolled hypertension or diabetes mellitus (DM) | multimethodological | 34 | Brazil | video consultation |
|
| Shaw et al. [83] | 2013 | US stakeholders including physicians, nurses, non-physician providers, administrators, and an IT professional with hypertension | nurse-delivered self-management phone | urban and rural | telephone counselling | initiating and maintaining specific health behaviors related to hypertension | mixed methods approach | 3 | USA | n/a |
|
| Grant et al. [84] | 2019 | people in the West Midlands, UK with hypertension, including patients, healthcare professionals, and patient caregivers | Text message | urban and rural | mobile health | blood pressure monitoring | randomized controlled trial | n/a | UK | mobile platform |
|
| Saleh et al. [85] | 2018 | Lebanese hypertensive | Short message service (SMS) | rural | mobile health | enhance access among underserved rural and refugee populations to health services specific to hypertension and/or diabetes. | mixed methods | n/a | Lebanon | Mobile phone |
|
| Vitório et al. [86] | 2019 | hypertensive patients | TeleHAS (tele-hipertensão arterial sistêmica, or arterial hypertension system) | urban | computerized clinical decision support system (CDSS) | hypertension management | Mixed methods | 88 | Brazil | n/a |
|
| Teo et al. [87] | 2021 | middle-aged people in Asia with hypertension | Home blood pressure monitoring | urban | Home blood pressure monitoring, teleconsultation | hypertension management | a mixed-methods field study | n/a | Singapura | Bluetooth |
|
| Key Themes | References |
|---|---|
| Tele-consultation | Dos et al. [50], Fisher et al. [54], Ma et al. [55], De Luca et al. [58], Chen et al. [59], Jindal et al. [60], Leon et al. [62], Buis et al. [63], Ju et al. [64], Nurakysh et al. [65], Manusov et al. [66], Marcolino et al. [68], Chew et al. [73], Andersson et al. [74], Kassavou et al. [75], Shaw et al. [83], Vitório et al. [86], Teo et al. [87] |
| Tele-monitoring | Barsky et al. [47], Naqvi et al. [48], Vedanthan et al. [49], Buis et al. [51], Koopman et al. [52], Parker et al. [53], Fisher et al. [54], Levine et al. [56], Ashjian et al. [57], De et al. [58], Doocy et al. [61], Ju et al. [64], Nurakysh et al. [65], Lee et al. [67], Marcolino et al. [68], Peters et al. [69], Debon et al. [70], Davoudi et al. [71], McManus et al. [72], Chew et al. [73], Andersson et al. [74], Cottrell et al. [76], Abdullah et al. [77], Ye et al. [79], Calderón et al. [80], Sin et al. [81], Cimini et al. [82], Grant et al. [84], Vitório et al. [86] |
| Tele-expertise | Fisher [54], Jindal [60], Marcolino [68], Vitório [86] |
| Tele-assistance | Dos et al. [50] |
| Others: tele-education | Dos et al. [50], Ma et al. [55], De et al. [58], Manusov et al. [66], Marcolino et al. [68], Cottrell et al. [76], Nau et al. [78], Shaw et al. [83], Saleh et al. [85], Vitório et al. [86] |
| Key Themes | References |
|---|---|
| Asynchronous: SMS text messaging, Tablet-based Decision Support and Integrated Record keeping (DESIRE) tool (mobile health), mobile health app, smartphone, patient-texted system, SMS and IVR messages, internet-based health management, mobile health clinic, mobile health, clinical decision support system, clinical decision support system, web conference | Cottrell et al. [17], Barsky et al. [47], Vedanthan et al. [49], Dos et al. [50], Buis et al. [51], Parke et al. [53], Ma et al. [55], Chen et al. [59], Jindal et al. [60], Doocy et al. [61], Leon et al. [62], Buis et al. [63], Ju et al. [64], Manusov et al. [66], Marcolino et al. [68], Peters et al. [69], Debon et al. [70], Davoudi et al. [71], Kassavou et al. [75], Cottrell et al. [76], Nau et al. [78], Grant et al. [84], Saleh et al. [85], Vitório et al. [86] |
| Synchronous: Virtual visit, teleconsultation online, interactive voice response (IVR), Home and Online Management and Evaluation of Blood Pressure, web-based system, telemedicine visit, telephone, app with decision support system | Naqvi et al. [48], Levine et al. [56], Ashjian et al. [57], McManus et al. [72], Andersson et al. [74], Ye et al. [79], Cimini et al. [82], Shaw et al. [83] |
| Remote patient monitoring: Blood Pressure Remote Patient Monitoring (RPM), monitoring hypertension, telemonitoring, home BP telemonitoring system | Koopman et al. [52], Fisher et al. [54], De Luca et al. [58], Lee et al. [67], Chew et al. [73], Abdullah et al. [77], Calderón et al. [80], Sin et al. [81], Teo et al. [87] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idris, H.; Nugraheni, W.P.; Rachmawati, T.; Kusnali, A.; Yulianti, A.; Purwatiningsih, Y.; Nuraini, S.; Susianti, N.; Faisal, D.R.; Arifin, H.; et al. How Is Telehealth Currently Being Utilized to Help in Hypertension Management within Primary Healthcare Settings? A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 90. https://doi.org/10.3390/ijerph21010090
Idris H, Nugraheni WP, Rachmawati T, Kusnali A, Yulianti A, Purwatiningsih Y, Nuraini S, Susianti N, Faisal DR, Arifin H, et al. How Is Telehealth Currently Being Utilized to Help in Hypertension Management within Primary Healthcare Settings? A Scoping Review. International Journal of Environmental Research and Public Health. 2024; 21(1):90. https://doi.org/10.3390/ijerph21010090
Chicago/Turabian StyleIdris, Haerawati, Wahyu Pudji Nugraheni, Tety Rachmawati, Asep Kusnali, Anni Yulianti, Yuni Purwatiningsih, Syarifah Nuraini, Novia Susianti, Debri Rizki Faisal, Hidayat Arifin, and et al. 2024. "How Is Telehealth Currently Being Utilized to Help in Hypertension Management within Primary Healthcare Settings? A Scoping Review" International Journal of Environmental Research and Public Health 21, no. 1: 90. https://doi.org/10.3390/ijerph21010090