

Socioeconomic, Demographic, and Environmental Factors May Inform Malaria Intervention Prioritization in Urban Nigeria
 , ,
, ,
Abstract
:1. Introduction
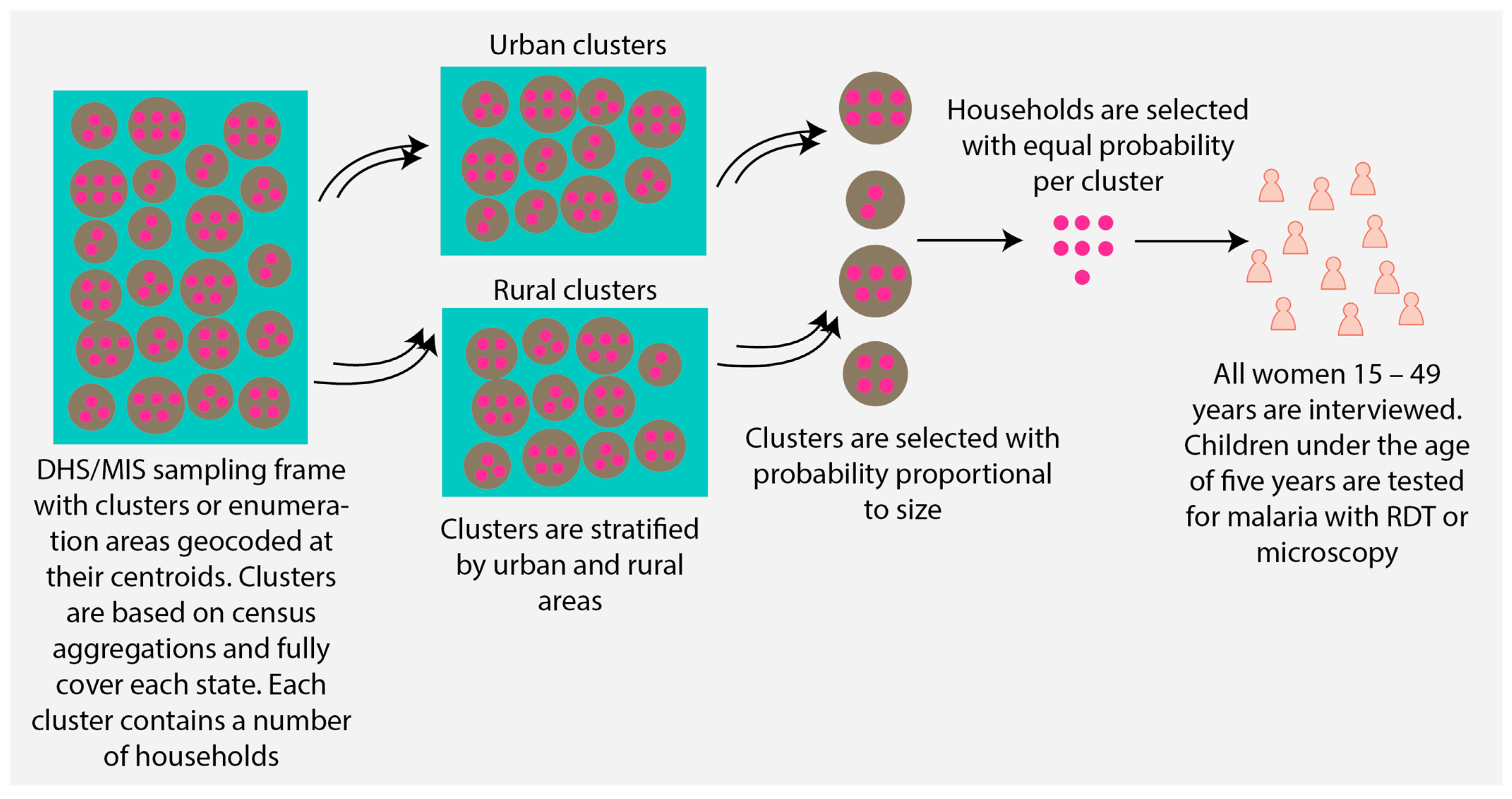
2. Materials and Methods
2.1. Data
2.2. Descriptive Analysis and Covariate Selection
2.3. Multivariable Modeling

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Name | Variable Definition | Source |
|---|---|---|
| Dependent variable | ||
| Number of U5 positive malaria tests | The number of positive malaria tests by microscopy among children 6–59 months old aggregated per cluster | MIS and DHS [23,34,35,36] |
| Explanatory variables by thematic group | ||
| Socioeconomic factors | ||
| Percentage (%) of women in each cluster with secondary or higher educational attainment | MIS and DHS [23,34,35,36] |
| % of the cluster population in the rich and richest wealth quintiles. Wealth quintiles were constructed using various indicators of household living standards [36] | MIS and DHS [23,34,35,36] |
| % of the cluster population living in homes with improved flooring (finished floors, parquet or polished wood, ceramic tiles, cement, and carpet) | MIS and DHS [23,34,35,36] |
| % of the cluster population living in homes with a metal or zinc roof | MIS and DHS [23,34,35,36] |
| % of the cluster population living in homes with an improved wall type (finished wall, cement, bricks, cement blocks, covered adobe) | MIS and DHS [23,34,35,36] |
| Predicted % of the cluster population living in improved housing in 2000. Improved housing is defined as homes with improved water and sanitation, sufficient living area, and durable construction, according to Tusting et al. [37] | Malaria Atlas Project (MAP) [38,39] |
| Predicted % of the cluster population living in improved housing in 2015 | MAP [37,40] |
| Demographic factors | ||
| Estimated population density per cluster at the time of the 2010 and 2015 DHS/MIS surveys. Population density data for 2020 were extracted for the 2018 and 2021 surveys (UN World Population Prospects-Adjusted Population Density, v4.11). Unit is persons per square kilometer | Center for International Earth Science Information Network, Columbia University [39] |
| Estimated population density for children under the age of five in 2020. Unit is the number of children per square kilometer | Humanitarian Data Exchange [40] |
| % of pregnant women | MIS and DHS [23,34,35,36] |
| % of females per cluster | MIS and DHS [23,34,35,36] |
| Median household size per cluster | MIS and DHS [23,34,35,36] |
| Median age per cluster | MIS and DHS [23,34,35,36] |
| State where the cluster is located | MIS and DHS [23,34,35,36] |
| Geopolitical region where the cluster is located (there are six geopolitical regions in Nigeria: the northeast, northwest, north central, southeast, southwest, south south) | MIS and DHS [23,34,35,36] |
| Behavioral factors | ||
| % of the cluster population that slept under a treated bednet the night before the survey | MIS and DHS [23,34,35,36] |
| % of children 6–59 months tested for malaria by microscopy that slept under a treated bednet the night before the survey | MIS and DHS [23,34,35,36] |
| % of children under the age of five that received medical treatment given that they had a fever or cough in the two weeks before the survey. Medical treatment must be received in the public sector or medical private sector, except for a pharmacy | MIS and DHS [23,34,35,36] |
| % of children under the age of five that received an ACT given that they had a fever | MIS and DHS [23,34,35,36] |
| Accessibility-related factors | ||
| Predicted travel time to healthcare facility in minutes in 2019 | MAP [41] |
| Environmental factors | ||
| Estimated total precipitation during survey month and year per cluster. Units measure the depth in meters. It is measured as the depth that the water would have if it were spread evenly over a grid box | European Center for Medium-Range Weather Forecasts (ECMWF), Climate Data Store [42] |
| Estimated temperature of air at 2 m above the surface of land, sea, or inland waters in Celsius per cluster during the survey month | ECMWF, Climate DataStore [42] |
| The average estimated depth of water present in a specific soil layer beneath the surface is measured as gravimetric soil moisture (GSM) per cluster. GSM is the mass of water compared to the mass of solid materials per unit volume of soil | Goddard Earth Sciences Data and Information Services Center [43] |
| Straight line distance to water bodies in meters | MAP (unpublished data) |
| Cluster elevation above sea level in meters | Multi-Error-Removed Improved-Terrain DEM [44] |
| Enhanced vegetation index for quantifying vegetation greenness in units of the spectral index | MAP gap filled EVI (communication with MAP) |
| Other adjustment variables | ||
| Number of children 6–59 months old tested for malaria per cluster | MIS and DHS [23,34,35,36] |
| Year the DHS survey was conducted per cluster and survey month per cluster (some clusters were surveyed over a two-month period; the first interview month was used in those cases) | MIS and DHS [23,34,35,36] |
| The longitude and latitude positions where the clusters were geolocated after displacement to protect participant confidentiality | MIS and DHS [23,34,35,36] |
3. Results
3.1. Describing Variations in Malaria Prevalence among Children under the Age of Five Years in Urban Areas
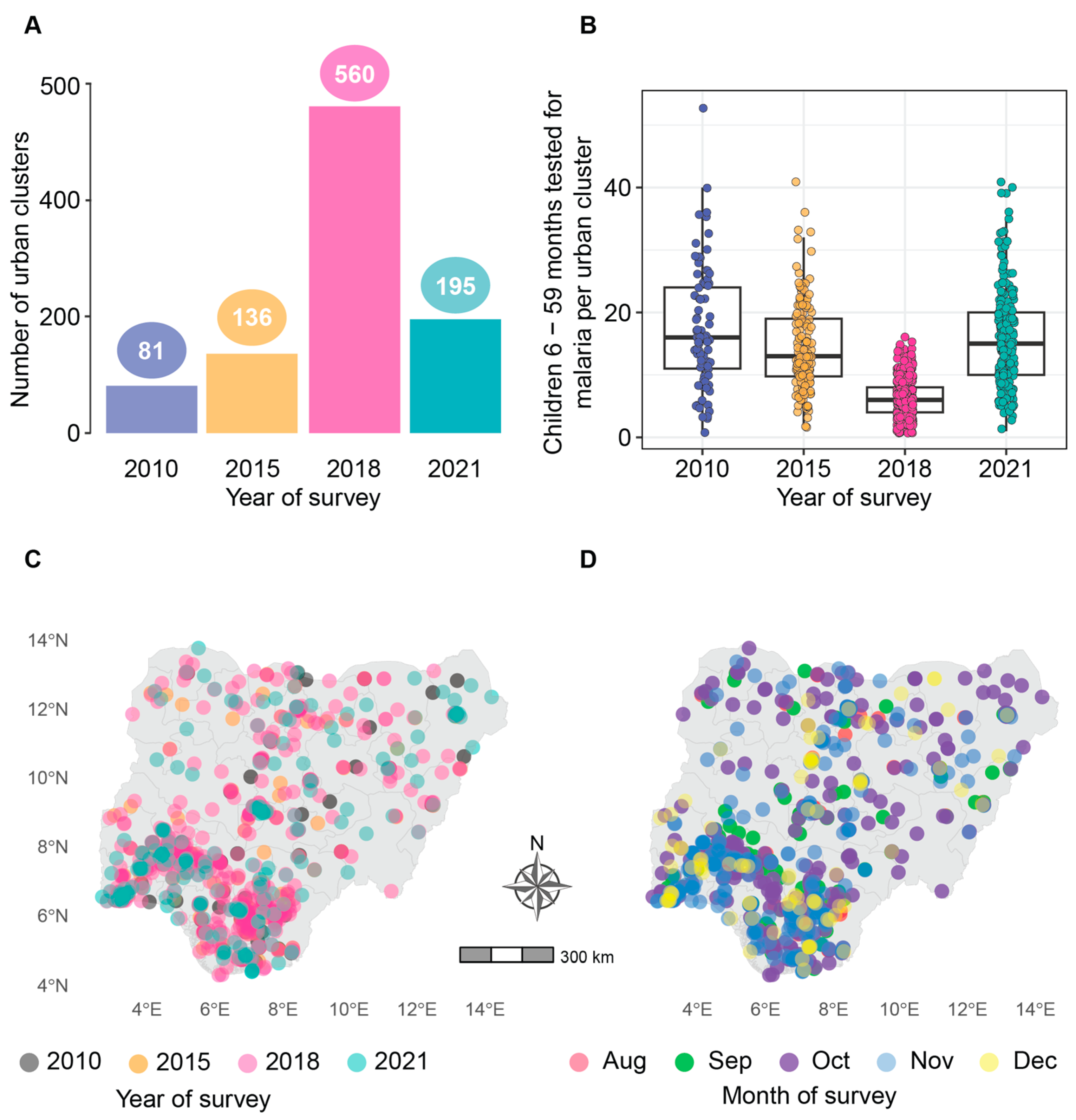
3.1.1. Sample Overview
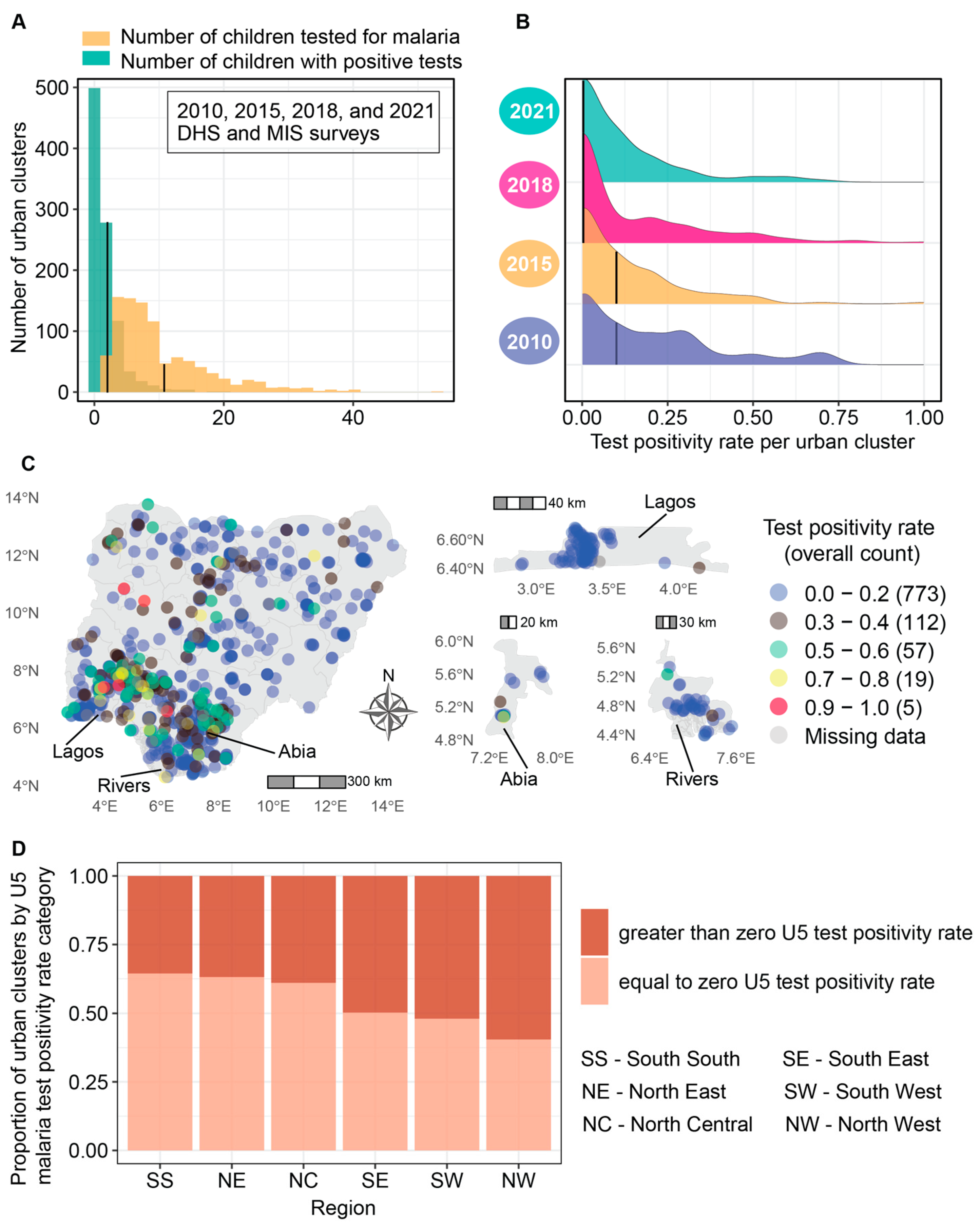
3.1.2. Low Malaria Test Positivity across the Majority of Urban Clusters
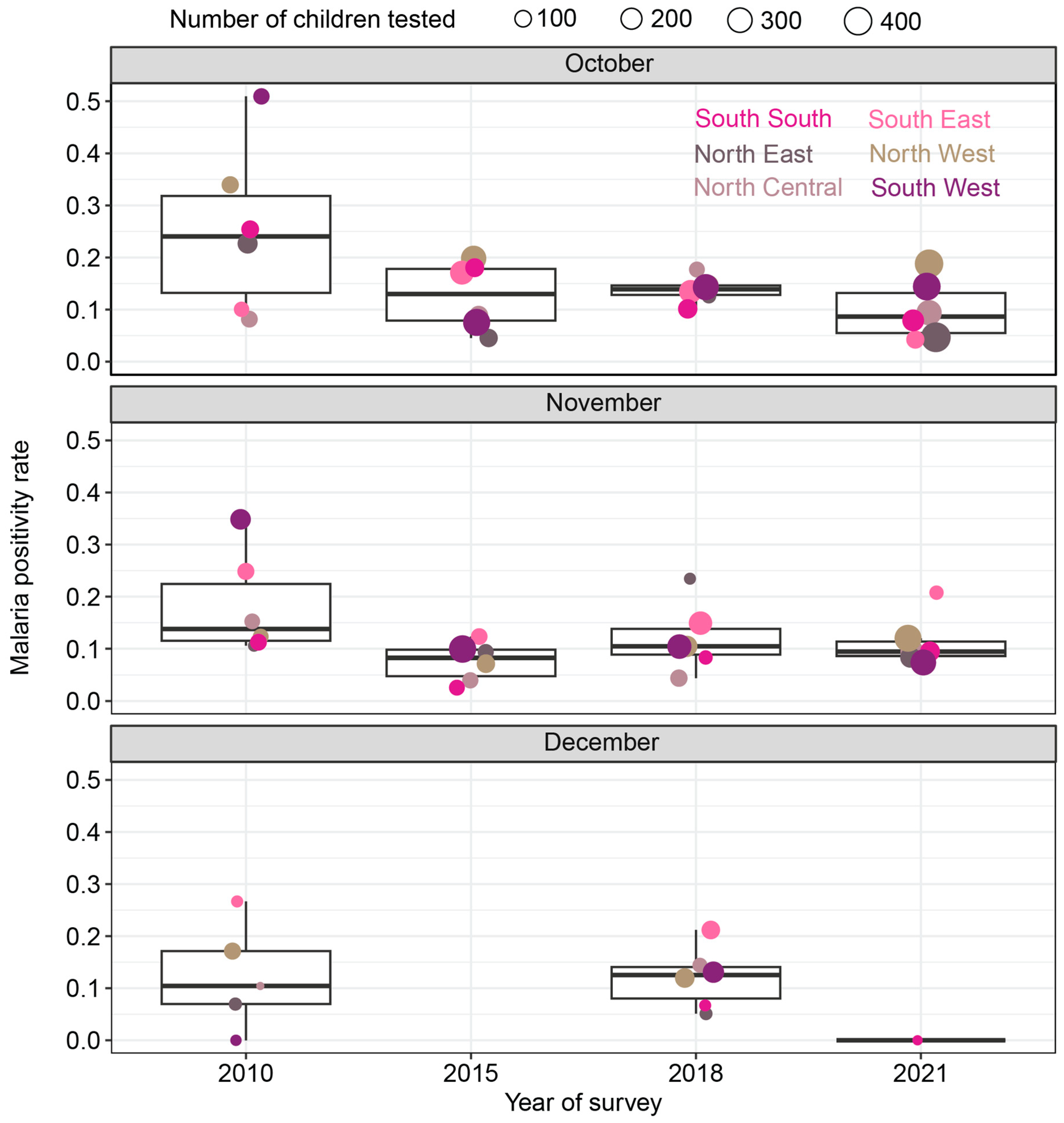
3.1.3. Test Positivity Rates in Sampled Clusters Declined over Time
3.2. Identifying Predictors of Malaria Test Positivity and Visualizing Bivariate Associations to Inform Intervention Prioritization
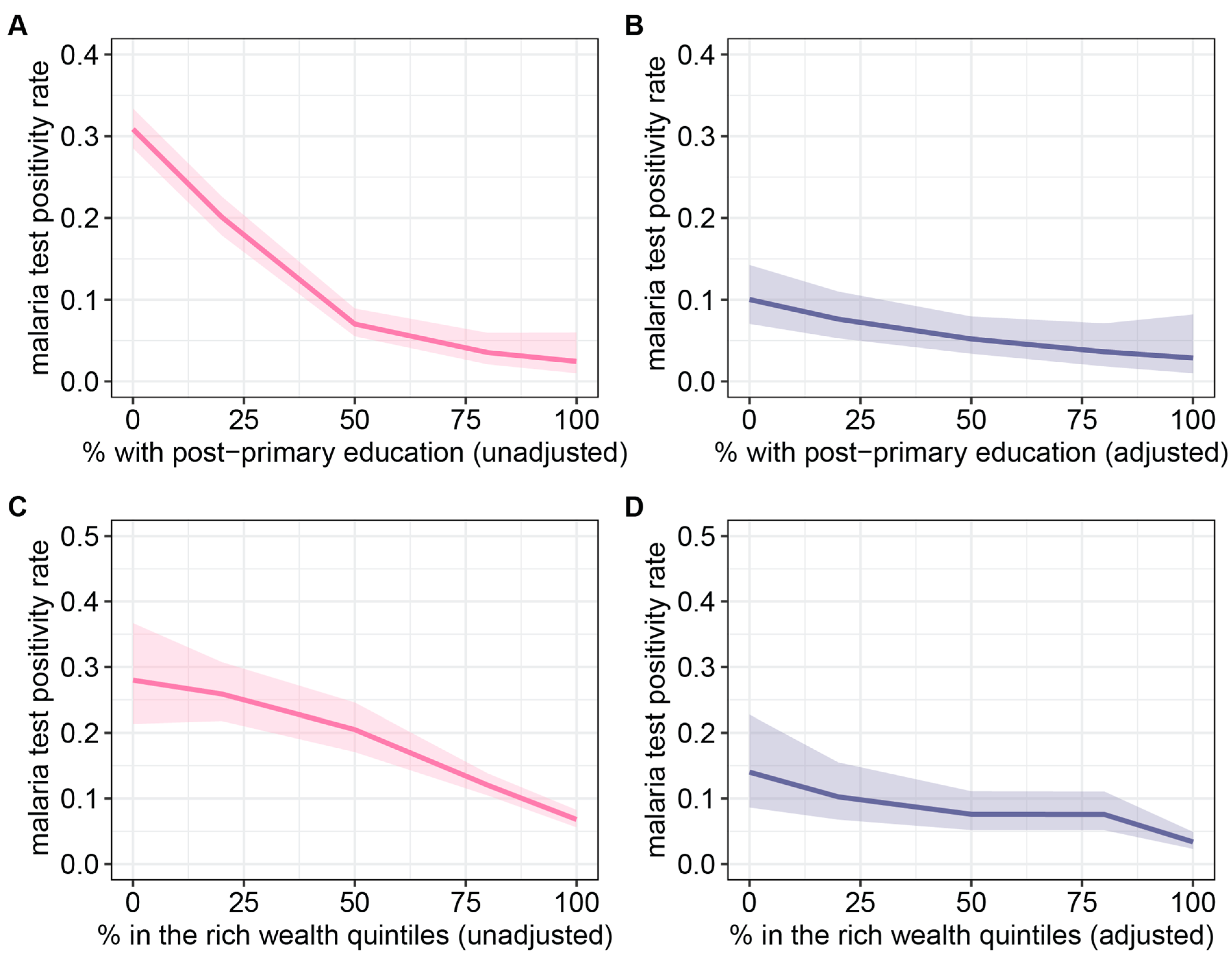
3.2.1. Clusters with the Lowest Educational Attainment and Wealth Were at the Highest Risk of Malaria
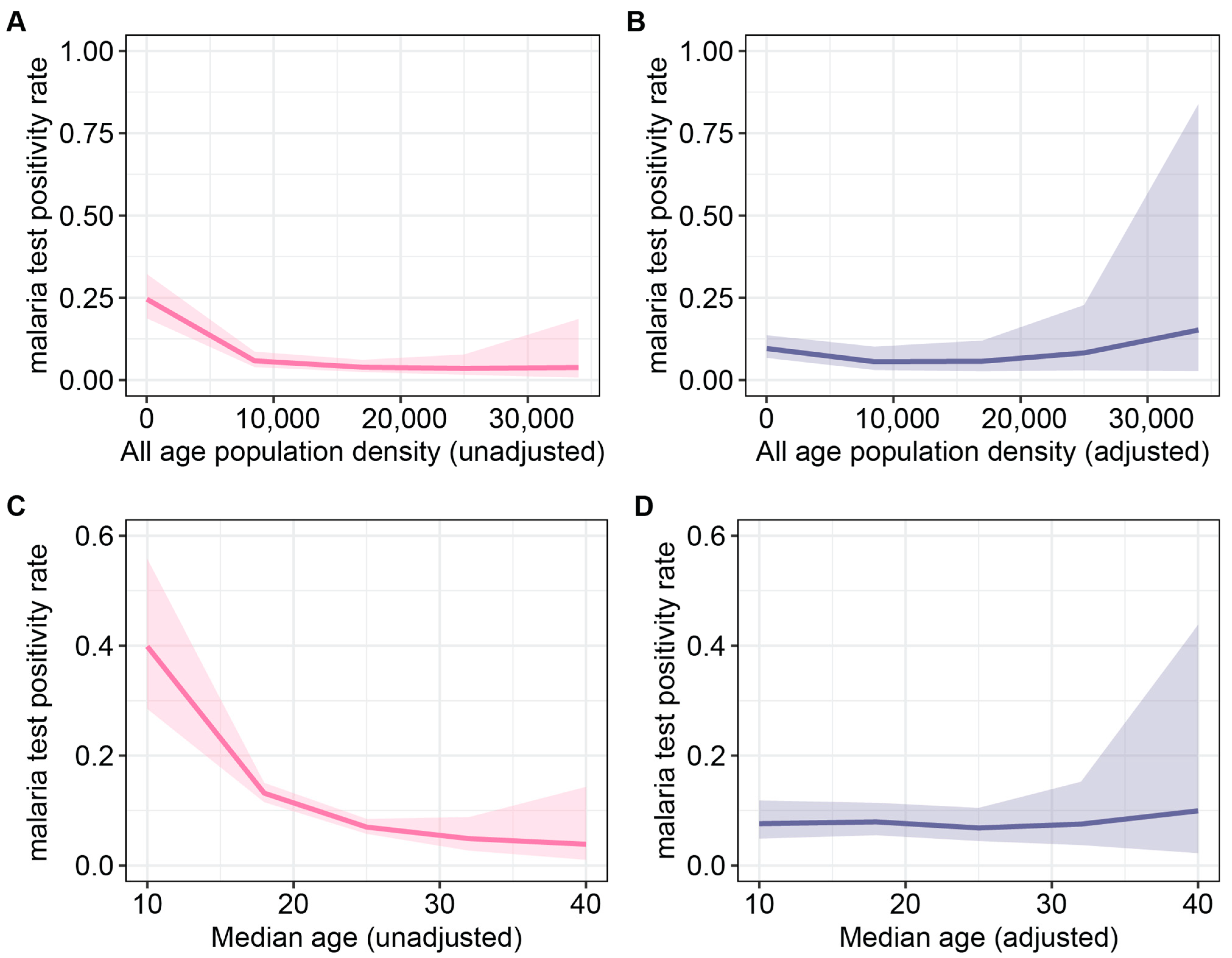
3.2.2. High Population Density and Younger Median Age Correlated with Higher Malaria Transmission Intensity
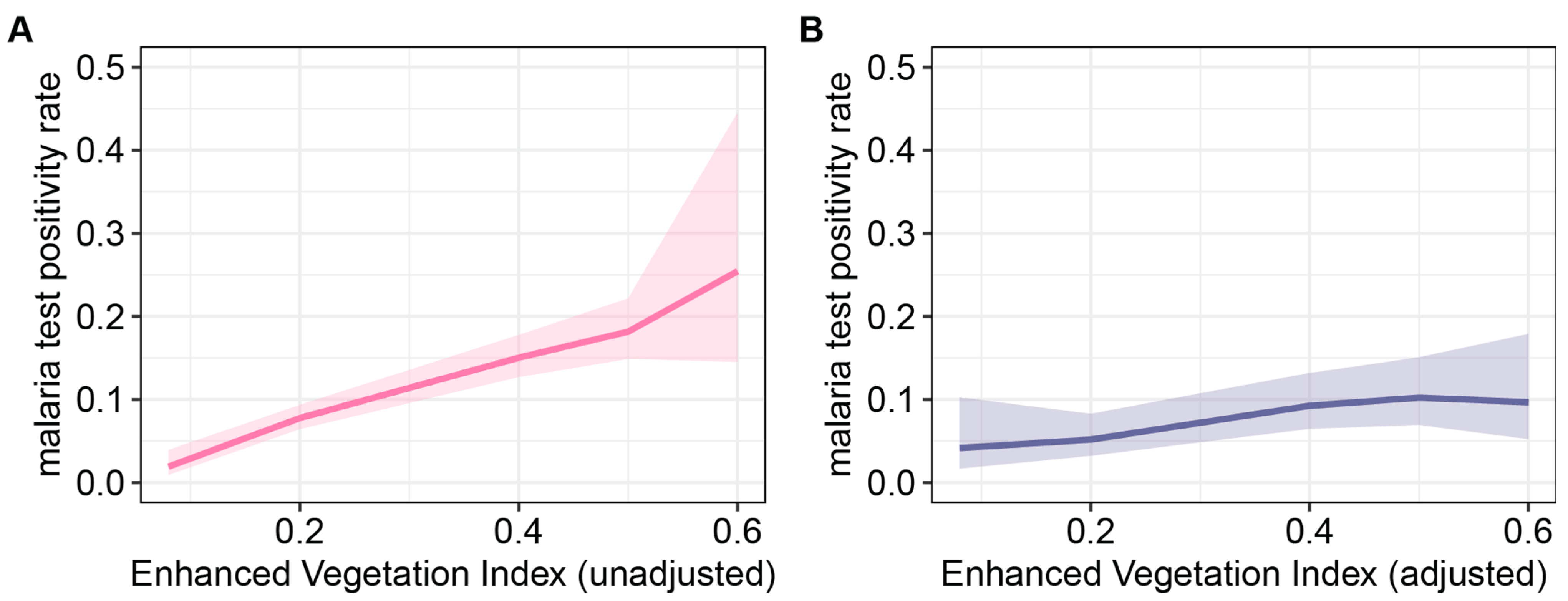
3.2.3. Higher Enhanced Vegetation Index Was Positively Associated with the U5 Malaria Test Positivity Rate
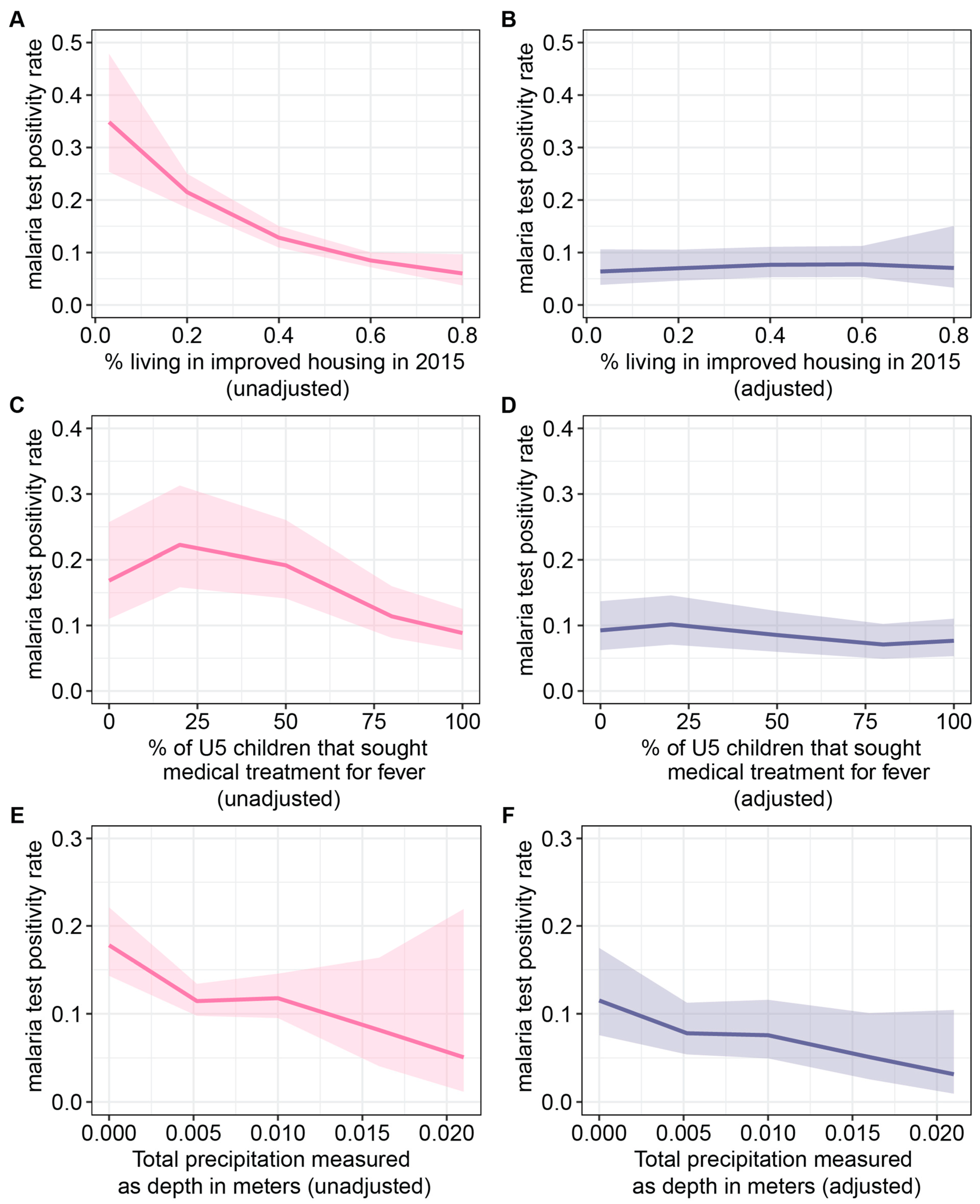
3.2.4. Effects of Housing, Care Seeking, and Precipitation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Okunlola, O.A.; Oyeyemi, O.T. Spatio-temporal analysis of association between incidence of malaria and environmental predictors of malaria transmission in Nigeria. Sci. Rep. 2019, 9, 17500. [Google Scholar] [CrossRef] [PubMed]
- National Malaria Control Programme; suMAP; World Health Organization; INFORM Project. A description of the epidemiology of malaria to guide the planning of control in Nigeria. In A Report Prepared for the Federal Ministry of Health, Nigeria, the Roll Back Malaria Partnership and the Department for International Development, UK; National Malaria Control Programme: Abuja, Nigeria, 2013. [Google Scholar]
- Jane Ugwu, C.L.; Zewotir, T. Evaluating the effects of climate and environmental factors on under-5 children malaria spatial distribution using generalized additive models (GAMs). J. Epidemiol. Glob. Health 2020, 10, 304–314. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs. World Urbanization Prospects: The 2018 Revision; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- World Health Organization. World Malaria Report 2022; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240064898 (accessed on 10 July 2023).
- Byrne, N. Urban malaria risk in sub-Saharan Africa: Where is the evidence? Travel Med. Infect. Dis. 2007, 5, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Trape, J.F.; Zoulani, A. Malaria and urbanization in Central Africa: The example of Brazzaville. Part. III: Relationships between urbanization and the intensity of malaria transmission. Trans. R. Soc. Trop. Med. Hyg. 1987, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Guerra, C.A.; Tatem, A.J.; Atkinson, P.M.; Snow, R.W. Urbanization, malaria transmission and disease burden in Africa. Nat. Rev. Microbiol. 2005, 3, 81. [Google Scholar] [CrossRef]
- Wang, S.-J.; Lengeler, C.; Smith, T.A.; Vounatsou, P.; Akogbeto, M.; Tanner, M. Rapid Urban Malaria Appraisal (RUMA) IV: Epidemiology of urban malaria in Cotonou (Benin). Malar. J. 2006, 5, 45. [Google Scholar] [CrossRef]
- Kabula, B.I.; Attah, P.K.; Wilson, M.D.; Boakye, D.A. Characterization of Anopheles gambiae s.l. and insecticide resistance profile relative to physicochemical properties of breeding habitats within Accra Metropolis, Ghana. Tanzan. J. Health Res. 2011, 13, 163–187. [Google Scholar] [CrossRef]
- Antonio-Nkondjio, C.; Fossog, B.T.; Ndo, C.; Djantio, B.M.; Togouet, S.Z.; Awono-Ambene, P.; Costantini, C.; Wondji, C.S.; Ranson, H. Anopheles gambiae distribution and insecticide resistance in the cities of Douala and Yaoundé (Cameroon): Influence of urban agriculture and pollution. Malar. J. 2011, 10, 154. [Google Scholar] [CrossRef] [PubMed]
- Azrag, R.S.; Mohammed, B.H. Anopheles arabiensis in Sudan: A noticeable tolerance to urban polluted larval habitats associated with resistance to Temephos. Malar. J. 2018, 17, 204. [Google Scholar] [CrossRef]
- Arinaitwe, E.; Mpimbaza, A.; Nankabirwa, J.I.; Kamya, V.; Asiimwe, A.; Kuule, J.K.; Kamya, M.R.; Drakeley, C.; Dorsey, G.; Rosenthal, P.J.; et al. Malaria Diagnosed in an Urban Setting Strongly Associated with Recent Overnight Travel: A Case–Control Study from Kampala, Uganda. Am. J. Trop. Med. Hyg. 2020, 103, 1517–1524. [Google Scholar] [CrossRef]
- Baragatti, M.; Fournet, F.; Henry, M.-C.; Assi, S.; Ouedraogo, H.; Rogier, C.; Salem, G. Social and environmental malaria risk factors in urban areas of Ouagadougou, Burkina Faso. Malar. J. 2009, 8, 13. [Google Scholar] [CrossRef]
- Bello, F.A.; Ayede, A.I. Prevalence of malaria parasitemia and the use of malaria prevention measures in pregnant women in Ibadan, Nigeria. Ann. Ib. Postgrad. Med. 2019, 17, 124–129. [Google Scholar]
- Olukosi, A.Y.; Olakiigbe, A.; Ajibaye, O.; Orok, B.A.; Aina, O.O.; Akindele, S.K.; Akinyele, O.O.; Onajole, A.T.; Awolola, S.T.; Arowolo, T.; et al. Socio-economic behavioural indicators of falciparum malaria parasitaemia and moderate to severe anaemia among pregnant women attending antenatal clinics in Lagos, Southwest Nigeria. Malar. J. 2020, 19, 393. [Google Scholar] [CrossRef] [PubMed]
- Adedotun, A.A.; Morenikeji, O.A.; Odaibo, A.B. Knowledge, attitudes and practices about malaria in an urban community in south-western Nigeria. J. Vector Borne Dis. 2010, 47, 155–159. [Google Scholar]
- Fana, S.A.; Bunza, M.D.A.; Anka, S.A.; Imam, A.U.; Nataala, S.U. Prevalence and risk factors associated with malaria infection among pregnant women in a semi-urban community of north-western Nigeria. Infect. Dis. Poverty 2015, 4, 24. [Google Scholar] [CrossRef]
- Awosolu, O.B.; Yahaya, Z.S.; Haziqah, M.T.F.; Simon-Oke, I.A.; Fakunle, C. A cross-sectional study of the prevalence, density, and risk factors associated with malaria transmission in urban communities of Ibadan, Southwestern Nigeria. Heliyon 2021, 7, e05975. [Google Scholar] [CrossRef] [PubMed]
- Alegana, V.A.; Okiro, E.A.; Snow, R.W. Routine data for malaria morbidity estimation in Africa: Challenges and prospects. BMC Med. 2020, 18, 121. [Google Scholar] [CrossRef]
- World Health Organization. Clinton Health Access Initiative. In Landscape Assessment of Malaria Surveillance in Nigeria; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- National Population Commission (NPC) Nigeria; ICF. Nigeria Demographic and Health Survey 2018; National Population Commission: Abuja, Nigeria; ICF: Rockville, MD, USA, 2019.
- Carneiro, I.; Roca-Feltrer, A.; Griffin, J.T.; Smith, L.; Tanner, M.; Schellenberg, J.A.; Greenwood, B.; Schellenberg, D. Age-Patterns of Malaria Vary with Severity, Transmission Intensity and Seasonality in Sub-Saharan Africa: A Systematic Review and Pooled Analysis. PLoS ONE 2010, 5, e8988. [Google Scholar] [CrossRef] [PubMed]
- Burgert-Brucker, C.R.; Colston, J.; Roy, T.; Zachary, B. Geographic Displacement Procedure and Georeferenced Data Release Policy for the Demographic and Health Surveys; DHS Spatial Analysis Reports No. 7; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Anyanwu, P.E.; Fulton, J.; Evans, E.; Paget, T. Exploring the role of socioeconomic factors in the development and spread of anti-malarial drug resistance: A qualitative study. Malar. J. 2017, 16, 203. [Google Scholar] [CrossRef] [PubMed]
- Dawaki, S.; Al-Mekhlafi, H.M.; Ithoi, I.; Ibrahim, J.; Atroosh, W.M.; Abdulsalam, A.M.; Sady, H.; Elyana, F.N.; Adamu, A.U.; Yelwa, S.I.; et al. Is Nigeria winning the battle against malaria? Prevalence, risk factors and KAP assessment among Hausa communities in Kano State. Malar. J. 2016, 15, 351. [Google Scholar] [CrossRef] [PubMed]
- Johansen, I.C.; Rodrigues, P.T.; Ferreira, M.U. Human mobility and urban malaria risk in the main transmission hotspot of Amazonian Brazil. PLoS ONE 2020, 15, e0242357. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.J.; Mappin, B.; Dalrymple, U.; Bhatt, S.; Cameron, E.; Hay, S.I.; Gething, P.W. Re-examining environmental correlates of Plasmodium falciparum Malaria endemicity: A data-intensive variable selection approach. Malar. J. 2015, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- Hadley, W. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Brooks, M.E.; Kristensen, K.; van Benthem, K.J.; Magnusson, A.; Berg, C.W.; Nielsen, A.; Skaug, H.J.; Machler, M.; Bolker, B.M. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. R J. 2017, 9, 378–400. [Google Scholar] [CrossRef]
- Bates, D.; Venables, W.N. Splines-Package: Regression Spline Functions and Classes. Available online: https://rdrr.io/r/splines/splines-package.html (accessed on 3 January 2022).
- Hartig, F. DHARMa: Residual Diagnostics for Hierarchical (Multi-Level/Mixed) Regression Models. The Comprehensive R Archive Network. 2021. Available online: https://cran.r-project.org/web/packages/DHARMa/vignettes/DHARMa.html (accessed on 12 December 2022).
- National Population Commission (NPC); National Malaria Control Programme (NMCP); ICF International. Nigeria Malaria Indicator Survey 2010; National Population Commission: Abuja, Nigeria, 2012.
- National Malaria Elimination Programme (NMEP); National Population Commission (NPopC); National Bureau of Statistics (NBS); ICF International. Nigeria Malaria Indicator Survey 2015; National Population Commission: Abuja, Nigeria; ICF International: Rockville, MD, USA,, 2016.
- National Malaria Elimination Programme National (NMEP) Nigeria; National Population Commission (NPC) Nigeria; ICF. Nigeria Malaria Indicator Survey 2021 Final Report; NMEP: Abuja, Nigeria; NPC: Abuja, Nigeria; ICF: Rockville, MD, USA, 2022. Available online: https://www.dhsprogram.com/pubs/pdf/MIS41/MIS41.pdf (accessed on 12 September 2023).
- Tusting, L.S.; Bisanzio, D.; Alabaster, G.; Cameron, E.; Cibulskis, R.; Davies, M.; Flaxman, S.; Gibson, H.S.; Knudsen, J.; Mbogo, C.; et al. Mapping changes in housing in sub-Saharan Africa from 2000 to 2015. Nature 2019, 568, 391–394. [Google Scholar] [CrossRef]
- Center for International Earth Science Information Network—CIESIN—Columbia University. Gridded Population of the World; Version 4 (GPWv4): Population Density Adjusted to Match 2015 Revision UN WPP Country Totals, Revision 11; NASA Socioeconomic Data and Applications Center (SEDAC): Palisades, NY, USA, 2018. Available online: https://doi.org/10.7927/H4F47M65 (accessed on 3 March 2021). [CrossRef]
- The Centre for Humanitarian Data. Welcome—Humanitarian Data Exchange. Available online: https://data.humdata.org/ (accessed on 16 September 2021).
- The Malaria Atlas Project. The Malaria Atlas Project Website. Available online: https://malariaatlas.org/ (accessed on 27 May 2020).
- Weiss, D.J.; Nelson, A.; Vargas-Ruiz, C.A.; Gligorić, K.; Bavadekar, S.; Gabrilovich, E.; Bertozzi-Villa, A.; Rozier, J.; Gibson, H.S.; Shekel, T.; et al. Global maps of travel time to healthcare facilities. Nat. Med. 2020, 26, 1835–1838. [Google Scholar] [CrossRef]
- European Center for Medium Range Weather Forecasts (ECMWF) Climate Data Store. ERA5-Land Monthly Averaged Data from 1981 to Present. Available online: https://doi.org/10.24381/cds.68d2bb30 (accessed on 2 September 2021). [CrossRef]
- Global Modeling and Assimilation Office. MERRA-2 tavgM_2d_lnd_Nx: 2d Monthly Mean Time-Averaged Single-Level Assimilation Land Surface Diagnostics V5.12.4; Goddard Earth Sciences Data and Information Services Center (GES DISC): Greenbelt, MD, USA, 2015.
- Yamazaki, D.; Ikeshima, D.; Tawatari, R.; Yamaguchi, T.; O’loughlin, F.; Neal, J.C.; Sampson, C.C.; Kanae, S.; Bates, P.D. A high-accuracy map of global terrain elevations. Geophys. Res. Lett. 2017, 44, 5844–5853. [Google Scholar] [CrossRef]
- Agomo, C.O.; Oyibo, W.A. Factors associated with risk of malaria infection among pregnant women in lagos, nigeria. Infect. Dis. Poverty 2013, 2, 19. [Google Scholar] [CrossRef]
- Brieger, W.R.; Sesay, H.R.; Adesina, H.; Mosanya, M.E.; Ogunlade, P.B.; Ayodele, J.O.; Orisasona, S.A. Urban malaria treatment behaviour in the context of low levels of malaria transmission in Lagos, Nigeria. Afr. J. Med. Med. Sci. 2001, 30, 7–15. [Google Scholar]
- Oladosu, O.O.; Oyibo, W.A. Overdiagnosis and Overtreatment of Malaria in Children That Presented with Fever in Lagos, Nigeria. ISRN Infect. Dis. 2013, 2013, 914675. [Google Scholar] [CrossRef]
- Oyibo, W.; Latham, V.; Oladipo, O.; Ntadom, G.; Uhomoibhi, P.; Ogbulafor, N.; Okoronkwo, C.; Okoh, F.; Mahmoud, A.; Shekarau, E.; et al. Malaria parasite density and detailed qualitative microscopy enhances large-scale profiling of infection endemicity in Nigeria. Sci. Rep. 2023, 13, 1599. [Google Scholar] [CrossRef]
- Noland, G.S.; Graves, P.M.; Sallau, A.; Eigege, A.; Emukah, E.; Patterson, A.E.; Ajiji, J.; Okorofor, I.; Oji, O.U.; Umar, M.; et al. Malaria prevalence, anemia and baseline intervention coverage prior to mass net distributions in Abia and Plateau States, Nigeria. BMC Infect. Dis. 2014, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Nzeako, S.O.; Nduka, F.O.; Origie, O.A. Prevalence of Malaria in Pregnant Women Attending Ante Natal Care at University of Port Harcourt Primary Health Care Centre Aluu, Port Harcourt, Rivers State, Nigeria. Int. J. Sci. Res. Environ. Sci. 2013, 1, 268–272. [Google Scholar] [CrossRef]
- Onoja, H.; Nduka, F.O.; Abah, A.E. Effectiveness and compliance to the use of sulphadoxine-pyrimethamine as a prophylaxis for malaria among pregnant women in Port Harcourt, Rivers State, Nigeria. Afr. Health Sci. 2022, 22, 187. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.M.; Marshall, J.M. Factors Contributing to Urban Malaria Transmission in Sub-Saharan Africa: A Systematic Review. J. Trop. Med. 2012, 2012, 819563. [Google Scholar] [CrossRef] [PubMed]
- National Malaria Elimination Programme. National Malaria Strategic Plan, 2021–2025. 2020. Available online: https://www.dropbox.com/s/cw9qvzdb2uwy4w1/NATIONALMALARIASTRATEGICPLAN2021–2025–FinalDraft2.0forprintingXXX.pdf?dl=0 (accessed on 12 August 2021).
- Fox, T.; Furnival-Adams, J.; Chaplin, M.; Napier, M.; Olanga, E.A. House modifications for preventing malaria. Cochrane Database Syst. Rev. 2022, 2022, CD013398. [Google Scholar] [CrossRef]
- Martello, E.; Yogeswaran, G.; Reithinger, R.; Leonardi-Bee, J. Mosquito aquatic habitat modification and manipulation interventions to control malaria. Cochrane Database Syst. Rev. 2022, 2022, CD008923. [Google Scholar] [CrossRef]
- Young, A.J.; Eaton, W.; Worges, M.; Hiruy, H.; Maxwell, K.; Audu, B.M.; Marasciulo, M.; Nelson, C.; Tibenderana, J.; Abeku, T.A. A practical approach for geographic prioritization and targeting of insecticide-treated net distribution campaigns during public health emergencies and in resource-limited settings. Malar. J. 2022, 21, 10. [Google Scholar] [CrossRef]
- Gracie, R.; Barcellos, C.; Magalhães, M.; Souza-Santos, R.; Guimarães Barrocas, P.R. Geographical scale effects on the analysis of leptospirosis determinants. Int. J. Environ. Res. Public Health 2014, 11, 10366. [Google Scholar] [CrossRef]
- Gyimah-Brempong, K.; Paddison, O.; Mitiku, W. Higher education and economic growth in Africa. J. Dev. Stud. 2006, 42, 509–529. [Google Scholar] [CrossRef]
- Bloom, D.; Canning, D.; Chan, K. Higher Education and Economic Development in Africa; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- WHO. Global Framework for the Response to Malaria in Urban Areas; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240061781 (accessed on 15 September 2023).
- National Malaria Elimination Programme. National Malaria Strategic Plan 2014–2020. 2013. Available online: https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/nigeria/nigeria_national_malaria_strategic_plan.pdf (accessed on 12 December 2020).
- Akpan, G.E.; Adepoju, K.A.; Oladosu, O.R.; Adelabu, S.A. Dominant malaria vector species in Nigeria: Modelling potential distribution of Anopheles gambiae sensu lato and its siblings with MaxEnt. PLoS ONE 2018, 13, e0204233. [Google Scholar] [CrossRef]
- Kaufmann, C.; Briegel, H. Flight performance of the malaria vectors Anopheles gambiae and Anopheles atroparvus. J. Vector Ecol. 2004, 29, 140–153. [Google Scholar] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiziba, C.; Mercer, L.D.; Diallo, O.; Bertozzi-Villa, A.; Weiss, D.J.; Gerardin, J.; Ozodiegwu, I.D. Socioeconomic, Demographic, and Environmental Factors May Inform Malaria Intervention Prioritization in Urban Nigeria. Int. J. Environ. Res. Public Health 2024, 21, 78. https://doi.org/10.3390/ijerph21010078
Chiziba C, Mercer LD, Diallo O, Bertozzi-Villa A, Weiss DJ, Gerardin J, Ozodiegwu ID. Socioeconomic, Demographic, and Environmental Factors May Inform Malaria Intervention Prioritization in Urban Nigeria. International Journal of Environmental Research and Public Health. 2024; 21(1):78. https://doi.org/10.3390/ijerph21010078
Chicago/Turabian StyleChiziba, Chilochibi, Laina D. Mercer, Ousmane Diallo, Amelia Bertozzi-Villa, Daniel J. Weiss, Jaline Gerardin, and Ifeoma D. Ozodiegwu. 2024. "Socioeconomic, Demographic, and Environmental Factors May Inform Malaria Intervention Prioritization in Urban Nigeria" International Journal of Environmental Research and Public Health 21, no. 1: 78. https://doi.org/10.3390/ijerph21010078