

The Effects of Music-Based Interventions for Pain and Anxiety Management during Vaginal Labour and Caesarean Delivery: A Systematic Review and Narrative Synthesis of Randomised Controlled Trials

 , and
, and 
Abstract
:1. Introduction
1.1. Labour Pain and Anxiety
1.2. Caesarean Section and Anxiety
1.3. Music-Based Interventions for Pain and Anxiety Management
1.4. Aims and Objectives
2. Materials and Methods
2.1. Search Strategy
- Birth, labour, childbirth
- Caesarean birth, caesarean section
- Music intervention, music therapy
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- Participants were human.
- Only Randomised controlled trials were used.
- Studies were on the effect of music or music-based interventions on pain management or maternal well-being during childbirth, including vaginal birth and caesarean section.
- Music or music therapy was used as an intervention.
- Studies were published in English or German.
2.2.2. Exclusion Criteria
- Animal studies.
- Case reports.
- Review articles.
- Perspective Papers.
- Letters.
- Master or doctoral theses.
- Systematic reviews or meta-analyses
- Articles that do not report data on mothers during labour.
- No music applied.
- Meeting abstracts.
- Findings that failed to report results/clinical outcomes.
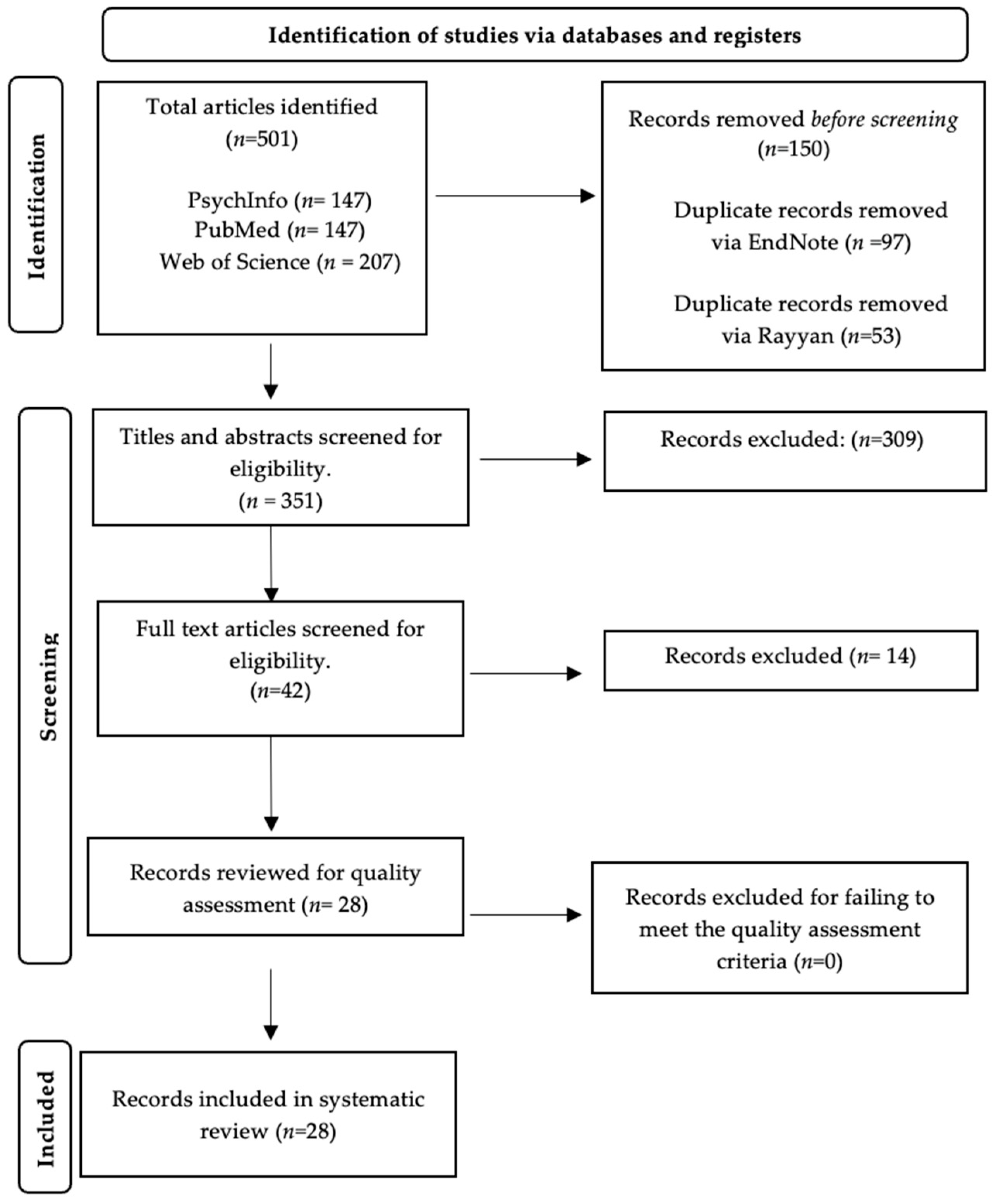
2.3. Study Selection and Risk of Bias
2.4. Analysis
3. Results
3.1. Studies Examining the Effects of Music-Based Interventions during Vaginal Labour
3.1.1. Music-Based Intervention as the Experimental Group Compared with a Control Group
3.1.2. Music-Based Interventions Compared with Other Therapies
3.1.3. Music-Based Interventions as Part of a Larger Therapy
3.2. Studies Investigating the Effects of Music-Based Interventions during Caesarean Sections
3.2.1. Studies That Used Participant-Selected Music during Caesarean Sections
3.2.2. Studies That Examined the Use of Participant-Selected Prespecified Music during Caesarean Sections
3.2.3. Studies That Used Researcher Preselected Music during Caesarean Sections
3.2.4. Studies That Used a Combination of Participant-Selected and Participant-Selected Prespecified Music during Caesarean Sections
4. Discussion
4.1. Summary of Results
4.2. Comparison with the Results of Previous Systematic Reviews
4.3. Limitations of Included Studies
4.4. Strengths and Limitations of the Current Review
4.5. Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hutchison, J.; Mahdy, H.; Hutchison, J. Stages of Labor; StatPearls Publishing LLC: San Francisco, CA, USA, 2020. [Google Scholar]
- Whitburn, L.Y.; Jones, L.; Davey, M.A.; Small, R. The meaning of labour pain: How the social environment and other contextual factors shape women’s experiences. BMC Pregnancy Childbirth 2017, 17, 157. [Google Scholar] [CrossRef]
- Phumdoung, S.; Good, M. Music reduces sensation and distress of labor pain. Pain. Manag. Nurs. 2003, 4, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Stott, D.; Papastefanou, I.; Paraschiv, D.; Clark, K.; Kametas, N.A. Longitudinal maternal hemodynamics in pregnancies affected by fetal growth restriction. Ultrasound Obstet. Gynecol. 2017, 49, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Habanananda, T. Non-pharmacological pain relief in labour. J. Med. Assoc. Thai 2004, 87, S194–S202. [Google Scholar]
- Lukasse, M.; Hovda, I.; Thommessen, S.A.O.; McAuley, S.; Morrison, M. Oxytocin and emergency caesarean section in a medium-sized hospital in Pakistan: A cross-sectional study. Eur. J. Midwifery 2020, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, M.; Aksoy, A.; Dostbil, A.; Celik, M.; Ince, I. The relationship between fear of childbirth and women’s knowledge about painless childbirth. Obstet. Gynecol. Int. 2014, 2014, 274303. [Google Scholar] [CrossRef]
- Baljon, K.J.; Romli, M.H.; Ismail, A.; Lee, K.; Chew, B.H. Effectiveness of breathing exercises, foot reflexology and massage (BRM) on maternal and newborn outcomes among primigravidae in Saudi Arabia: A randomized controlled trial. Int. J. Womens Health 2022, 14, 279–295. [Google Scholar] [CrossRef] [PubMed]
- Mostafayi, M.; Imani, B.; Zandi, S.; Rabie, S. Comparing early postoperative maternal complications in elective and emergency cesarean sections. J. Midwifery Reprod. Health 2020, 8, 2368–2375. [Google Scholar]
- Safari-Moradabadi, A.; Hassani, L.; Ghanbarnejad, A.; Madani, A.; Rajae, I.M.; Dadipoor, S. The effect of education on knowledge and preferred method of delivery in nulliparous women. J. Health Care 2014, 16, 74–83. [Google Scholar]
- Ferede, Y.A.; Bizuneh, Y.B.; Workie, M.M.; Admass, B.A. “Prevalence and associated factors of preoperative anxiety among obstetric patients who underwent cesarean section”: A cross-sectional study. Ann. Med. Surg. 2022, 74, 103272. [Google Scholar] [CrossRef]
- McQueen, K.; Coonan, T.; Ottaway, A.; Dutton, R.P.; Nuevo, F.R.; Gathuya, Z.; Wilson, I.H. Anesthesia and perioperative care. In Essential Surgery, 3rd ed.; Debas, H.T., Donkor, P., Gawande, A., Jamison, D.T., Kruk, M.E., Mock, C.N., Eds.; World Bank Group: Washington, WA, USA, 2015; Chapter 15; Volume 1, pp. 263–277. [Google Scholar]
- Li, Y.; Dong, Y. Preoperative music intervention for patients undergoing cesarean delivery. Int. J. Gynaecol. Obstet. 2012, 119, 81–83. [Google Scholar] [CrossRef]
- Abarghoee, S.N.; Mardani, A.; Baha, R.; Aghdam, N.F.; Khajeh, M.; Eskandari, F.; Vaismoradi, M. Effects of Benson relaxation technique and music therapy on the anxiety of primiparous women prior to cesarean section: A randomized controlled trial. Anesthesiol. Res. Pract. 2022, 2022, 9986587. [Google Scholar] [CrossRef]
- Schaal, N.K.; Hepp, P.; Heil, M.; Wolf, O.T.; Hagenbeck, C.; Fleisch, M.; Fehm, T. Perioperative anxiety and length of hospital stay after caesarean section—A cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 248, 252–256. [Google Scholar] [CrossRef]
- Wyatt, S.; Jones, D.; Peach, M.J.; Gurrin, L.C. Anxiety in patients having caesarean section under regional anaesthesia: A questionnaire and pilot study. Int. J. Obstet. Anesth. 2001, 10, 278–283. [Google Scholar] [CrossRef]
- Czech, I.; Fuchs, P.; Fuchs, A.; Lorek, M.; Tobolska-Lorek, D.; Sikora, J. Pharmacological and non-pharmacological methods of labour pain relief—Establishment of effectiveness and comparison. Int. J. Environ. Res. Public. Health 2018, 15, 2792. [Google Scholar] [CrossRef] [PubMed]
- Nanji, J.A.; Carvalho, B. Pain management during labor and vaginal birth. Best. Pract. Res. Clin. Obstet. Gynaecol. 2020, 67, 100–112. [Google Scholar] [CrossRef]
- Thomson, G.; Feeley, C.; Moran, V.H.; Downe, S.; Oladapo, O.T. Women’s experiences of pharmacological and non-pharmacological pain relief methods for labour and childbirth: A qualitative systematic review. Reprod. Health 2019, 16, 71. [Google Scholar] [CrossRef]
- Henrique, A.J.; Gabrielloni, M.C.; Rodney, P.; Barbieri, M. Non-pharmacological interventions during childbirth for pain relief, anxiety, and neuroendocrine stress parameters: A randomized controlled trial. Int. J. Nurs. Pract. 2018, 24, e12642. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, K.R.M.; Stewart, L.; Glover, V. How music may support perinatal mental health: An overview. Arch. Womens Ment. Health 2021, 24, 831–839. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, R. Music, health, and well-being: A review. Int. J. Qual. Stud. Health Well-Being 2013, 8, 20635. [Google Scholar] [CrossRef]
- Situmorang, D.D.B. Dancing during labor in the midst of COVID-19 outbreak: As an alternative non-pharmacological treatment after digital interventions. J. Public Health 2022, 44, e617–e618. [Google Scholar] [CrossRef]
- John, N.; Angeline, A. Effectiveness of music therapy on anxiety and pain among mothers during first stage of labour in selected hospitals at Kollam. Int. J. Nurs. Educ. Scholarsh. 2017, 9, 24–29. [Google Scholar] [CrossRef]
- Xavier, T.; Viswanath, L. Effect of music therapy on labor pain among women in active labor admitted in tertiary care hospital Kochi. Int. J. Integr. Med. Sci. 2016, 3, 444–453. [Google Scholar] [CrossRef]
- Simkin, P.; Bolding, A. Update on nonpharmacologic approaches to relieve labor pain and prevent suffering. Midwifery Womens Health 2004, 49, 489–504. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Que, M.; Shen, J.; Nie, Q.; Chen, Y.; Huang, Q.; Jin, A. Effect of music therapy combined with free position delivery on labor pain and birth outcomes. Appl. Bionics Biomech. 2022, 2022, 8963656. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.H.; Chen, P.C.; Lee, C.S.; Chen, C.H.; Tu, Y.K.; Wu, S.C. Music intervention for pain and anxiety management of the primiparous women during labour: A systematic review and meta-analysis. J. Adv. Nurs. 2019, 75, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Santiváñez-Acosta, R.; Tapia-López, E.; Santero, M. Music therapy in pain and anxiety management during Labor: A systematic review and meta-Analysis. Medicina 2020, 56, 526. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.H.; Chang, Y.C.; Chou, H.H.; Chang, C.P.; Huang, M.Y.; Liu, S.J.; Tsai, C.H.; Lei, W.T.; Yeh, T.L. Effect of music interventions on anxiety during labor: A systematic review and meta-analysis of randomized controlled trials. PeerJ 2019, 7, e6945. [Google Scholar] [CrossRef]
- Weingarten, S.; Levy, A.T.; Berghella, V. The effect of music on anxiety in women undergoing cesarean delivery: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100435. [Google Scholar] [CrossRef]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef]
- Chang, H.C.; Yu, C.H.; Chen, S.Y.; Chen, C.H. The effects of music listening on psychosocial stress and maternal–Fetal attachment during pregnancy. Complement. Ther. Med. 2015, 23, 509–515. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Saimbert, M. Keyprinciples for searching the literature. In Comprehensive Systematic Review for Advanced Practice Nursing, 2nd ed.; Holly, C., Salmond, S.W., Saimbert, M.K., Eds.; Springer Publishing Company: New York, NY, USA, 2016; Chapter 5; pp. 77–104. [Google Scholar]
- Harris, J.D.; Quatman, C.E.; Manring, M.M.; Siston, R.A.; Flanigan, D.C. How to write a systematic review. Am. J. Sports Med. 2013, 42, 2761–2768. [Google Scholar] [CrossRef] [PubMed]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. Prod. ESRC Methods Programme Version 2006, 1, b92. [Google Scholar]
- Liu, Y.H.; Chang, M.Y.; Chen, C.H. Effects of music therapy on labour pain and anxiety in Taiwanese first-time mothers. J. Clin. Nurs. 2010, 19, 1065–1072. [Google Scholar] [CrossRef]
- Simavli, S.; Kaygusuz, I.; Gumus, I.I.; Usluogullari, B.; Yildirim, M.; Kafali, H. Effect of music therapy during vaginal delivery on postpartum pain relief and mental health. J. Affect. Disord. 2014, 156, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Surucu, S.G.; Öztürk, M.; Vurgeç, B.A.; Alan, S.; Akbas, M. The effect of music on pain and anxiety of women during labour on first time pregnancy: A study from Turkey. Complement. Ther. Clin. Pract. 2018, 30, 96–102. [Google Scholar] [CrossRef]
- Buglione, A.; Saccone, G.; Mas, M.; Raffone, A.; Di Meglio, L.; di Meglio, L.; Toscano, P.; Travaglino, A.; Zapparella, R.; Duval, M.; et al. Effect of music on labor and delivery in nulliparous singleton pregnancies: A randomized clinical trial. Arch. Obstet. Gynaecol. 2020, 301, 693–698. [Google Scholar] [CrossRef]
- Simavli, S.; Gumus, I.I.; Kaygusuz, I.; Yildirim, M.; Usluogullari, B.; Kafali, H. Effect of music on labor pain relief, anxiety level and postpartum analgesic requirement: A randomized controlled clinical trial. Gynecol. Obstet. Invest. 2014, 78, 244–250. [Google Scholar] [CrossRef]
- García-González, J.; Ventura-Miranda, M.I.; Requena, M.; Parrón-Carreño, T.; Rodríguez, R.A. Effects of prenatal music stimulation on state/trait anxiety in full-term pregnancy and its influence on childbirth: A randomized controlled trial. J. Matern. Fetal Neonatal Med. 2017, 31, 1058–1065. [Google Scholar] [CrossRef]
- Amanak, K. The effect of the sound of the ney (reed flute) on women in labour in Bursa, Turkey. J. Pak. Med. Assoc. 2020, 70, 1934–1937. [Google Scholar] [PubMed]
- Browning, C.A. Music therapy in childbirth: Research in practice. Music. Ther. Perspects 2001, 19, 74–81. [Google Scholar] [CrossRef]
- García-González, J.; Ventura-Miranda, M.I.; Requena, M.; Parrón-Carreño, T.; Alarcón, R. State-trait anxiety levels during pregnancy and foetal parameters following intervention with music therapy. J. Affect. Disord. 2018, 232, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Kimber, L.; McNabb, M.; Court, C.; Haines, A.; Brocklehurst, P. Massage or music for pain relief in labour: A pilot randomised placebo controlled trial. Eur. J. Pain. 2008, 12, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Estrella-Juarez, F.; Requena, M.; García-González, J.; López-Villén, A.; Alarcón, R. Effect of virtual reality and music therapy on the physiologic parameters of pregnant women and fetuses and on anxiety levels: A randomized controlled trial. J. Midwifery Womens Health 2022, 68, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Taghinejad, H.; Delpisheh, A.; Suhrabi, Z. Comparison between massage and music therapies to relieve the severity of labor pain. Women’s Health 2010, 6, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Dehcheshmeh, F.S.; Rafiei, H. Complementary and alternative therapies to relieve labor pain: A comparative study between music therapy and Hoku point ice massage. Complement. Ther. Clin. Pract. 2015, 21, 229–232. [Google Scholar] [CrossRef]
- Wan, Q.; Wen, F.Y. Effects of acupressure and music therapy on reducing labor pain. Int. J. Clin. Exp. Med. 2018, 11, 898–903. [Google Scholar]
- Gönenç, İ.M.; Dikmen, H.A. Effects of dance and music on pain and fear during childbirth. J. Obstet. Gynecol. Neonatal Nurs. 2020, 49, 144–153. [Google Scholar] [CrossRef]
- Perković, R.; Dević, K.; Hrkać, A.; Šaravanja, N.; Tomić, V.; Krišto, B.; Dukić, H.; Vasilj, V. Relationship between education of pregnant women and listening to classical music with the experience of pain in childbirth and the occurrence of psychological symptoms in puerperium. Psychiatr. Danub. 2021, 33, 260–270. [Google Scholar]
- Kaur, H.; Bansal, G.L.; Sreehari, S.; Shukla, V.; Harsh, H.K.; Pareek, R. The effect of music on serum cortisol levels and anxiety in patients undergoing lower segment cesarean section under spinal anesthesia: A randomized controlled interventional study. J. Obstet. Anaesth. Crit. Care 2023, 13, 87–93. [Google Scholar]
- Eren, H.; Sahiner, N.C.; Bal, M.D.; Dişsiz, M. Effects of music during multiple cesarean section delivery. J. Coll. Physicians Surg. Pak. 2018, 28, 247–249. [Google Scholar] [CrossRef]
- Hepp, P.; Hagenbeck, C.; Gilles, J.; Wolf, O.T.; Goertz, W.; Janni, W.; Balan, P.; Fleisch, M.; Fehm, T.; Schaal, N.K. Effects of music intervention during caesarean delivery on anxiety and stress of the mother a controlled, randomised study. BMC Pregnancy Childbirth 2018, 18, 435. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Chen, C.H. Effects of music therapy on women’s physiologic measures, anxiety, and satisfaction during cesarean delivery. Res. Nurs. Health 2005, 28, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Denney, J.M.; Blackburn, K.L.; Bleach, C.C.; Martinez, A.R.; Philips, J.B.; Lanier, K.; Dean, L.; Mertz, H. The effects of music intervention on women’s anxiety before and after cesarean delivery: A randomized controlled trial. Music. Med. 2018, 10, 225–232. [Google Scholar] [CrossRef]
- Horasanlı, J.E.; Demirbaş, N. Effects of music intervention during cesarean section on the level of the mother’s anxiety: A randomized controlled study. Erciyes Med. J. 2022, 44, 257–262. [Google Scholar] [CrossRef]
- Kurdi, M.S.; Gasti, V. Intraoperative meditation music as an adjunct to subarachnoid block for the improvement of postoperative outcomes following cesarean section: A randomized placebo-controlled comparative study. Anesth. Essays Res. 2018, 12, 618. [Google Scholar]
- Halder, A.; Kumar, A.; Hariharan, U.; Manjhi, B. Effect of perioperative music therapy/medicine on postoperative pain in women undergoing elective lower segment caesarean section delivery under spinal anaesthesia: A case-control study. J. Clin. Diagn. Res. 2022, 16, 10–15. [Google Scholar] [CrossRef]
- Robb, S.L.; Carpenter, J.S.; Burns, D.S. Reporting guidelines for music-based interventions. J. Health Psychol. 2010, 16, 342–352. [Google Scholar] [CrossRef]
- Stouffer, J.W.; Shirk, B.; Polomano, R.C. Practice guidelines for music interventions with hospitalized pediatric patients. J. Pediatr. Nurs. 2007, 22, 448–456. [Google Scholar] [CrossRef]
- Krishna Priya, A.; Applewhite, B.; Au, K.; Oyeleye, O.; Walton, E.; Norton, C.; Patsalos, O.; Cardi, V.; Himmerich, H. Attitudes surrounding music of patients with anorexia nervosa: A survey-based mixed-methods analysis. Front. Psychiatry 2021, 12, 639202. [Google Scholar] [CrossRef]
- Truong, T.P.A.; Applewhite, B.; Heiderscheit, A.; Himmerich, H. A systematic review of scientific studies and case reports on music and obsessive-compulsive disorder. Int. J. Environ. Res. Public. Health 2021, 18, 11799. [Google Scholar] [CrossRef]
- Watson, K.; White, C.; Hall, H.; Hewitt, A. Women’s experiences of birth trauma: A scoping review. Women Birth. 2021, 34, 417–424. [Google Scholar] [CrossRef]


{kind=link}
| Authors/Years | Country | Sample/Group Size | Total Sample Size | Mean Age | Measures | Music Intervention | Control Group | Method of Childbirth | Type of Music | Main Outcomes and Statistical Significance |
|---|---|---|---|---|---|---|---|---|---|---|
| (1) Studies Examining the Effects of Music-based Interventions During Vaginal Labour. | ||||||||||
| (1.1) Music-based Interventions as the Experimental Group Compared with a Control Group. | ||||||||||
| Phumdoung and Good (2003) [3] | Southern Thailand |
| N = 110 | 24 | VAS | The Music group listened to soft music with earphones during the first 3 h of the active phase of labour. | Traditional labour; however, to avoid demoralization, the control group was told they would receive music at some point (once pain measurements were complete). | Vaginal delivery (active phase). | Choice of five types of Western music without lyrics: synthesizer, harp, piano, orchestra, and jazz. | Participants who listened to soft music experienced less sensation of pain (p < 0.01) and pain-related distress (p < 0.001) compared with participants in the control group. |
| Liu et al. (2010) [38] | China |
| N = 60 | 27.12 | VASP; PBI; FT; OEQ. | Participants listened to music for 30 min during the latent and active phases of labour. Participants could choose whether or not to wear headphones. | Participants received routine care post-admission. Participants were unaware of the option to listen to music. | Vaginal delivery (latent and active phases). | Participants chose either relaxing music, light music, popular music, crystal children’s, or Chinese religious music. | Mothers who listened to music during labour experienced less pain (VASP, p < 0.001) and anxiety (VASA, p < 0.001; PBI, p = 0.014) and had a higher FT (p = 0.014) compared with participants in the control group. |
| Simavli et al. [39] | Turkey |
| N = 161 | Music: 24.17 Control: 23.28 | VASA; VASP; VASS; EPDS. | During labour, participants’ selected music was played at all times, with a 20 min break after every 2 h of play. Music continued up to the end of the third phase of labour. Participants could choose whether or not to wear headphones. | Participants received standard prenatal care. | Vaginal delivery. | Six types, including classical music, light music, popular music, Turkish art music, Turkish folk music, and Turkish Sufi music. | Mothers in the music group had lower levels of postpartum pain compared with controls (p < 0.001). They also had higher satisfaction with their birthing experience at 2 h (p < 0.001), 12 h, and 24 h (p < 0.01) postpartum. |
| Surucu et al. (2018) [40] | Turkey |
| N = 50 | Music: 22.08 Control: 21.04 | VAS; STAI; FAS. | When in active labour (4 cm), women listened to Acemasiran-style music through headphones for 3 h (20 min listening, 10 min not listening). | Routine procedures typically used in hospitals during labour, with no additional practices or music therapy. | Vaginal delivery (active phase). | Acemasiran. | Women in the music group experienced less pain (p < 0.05) and lower anxiety levels (p < 0.05). Labour was rated as easier by women in the music group (p < 0.05), but the contraction period was longer for women in the music group compared with controls (p < 0.05). |
| Buglione et al. (2020) [41] | Italy |
| N = 30 | Music: 28.7 Control: 31.1 | VASP; VASA. | Women listened to music via speakers throughout their labour and the birth of the baby. Women chose songs to listen to. | Participants received the same obstetrical care during labour/delivery as those in the intervention group, except they did not listen to music during labour/delivery. | Vaginal delivery (active phase). | Participants’ own choice of music. | During the active phase of labour, significantly lower levels of pain were experienced in the music group compared with the control group (p < 0.01). |
| Simavli et al. (2014) [42] | Turkey |
| N = 156 | Music: 25.06 Control: 25.09 | SBP; DBP; VASP; VASA. | Music was played during the latent phase and the first 2 h of the active phase of labour. 20 min break after every hour of music. Near the end of the active phase and during the second stage of labour, the music type and volume were changed to a more rhythmic beat for pushing. | Participants were provided with a blank CD with no music during labour. The control group only received routine obstetrical care without any additional intervention. | Vaginal delivery (latent and active phase). | Participants were advised to choose soft, relaxing music. Five types were used: classical music, Turkish art music, Turkish folk music, Turkish classical music, and pop music. | Throughout labour and postpartum, pain and anxiety were reported to be lower in the music group compared with the control group (p < 0.001). |
| Garcia-González et al. (2018) [43] | Spain |
| N = 209 | Music: 31.85 Control: 30.90 | Childbirth parameters | Prior to birth, participants listened to music via a CD player in a quiet room at home. There was a total of 14 sessions, each lasting 40 min. Music had to be listened to at the same time each day. | Participants went through the same assessment and procedures as the experimental group but without music intervention. | Vaginal labour or Caesarean section. | Instrumental piece of music called “musical journey through pregnancy” By Gabriel F. Federico. | Women in the music group had more spontaneous and less induced labour compared with women in the control group (p = 0.006). |
| Amanak (2020) [44] | Turkey |
| N = 30 | Music: 25.36 Control: 25.1 | IDF; LTF; VAS; STAI–SAI. | Post baseline data collection, participants listened to 30 min of music via a CD player followed by 30 min intermission (conducted in rounds). | The control group had standard care with no intervention. | Vaginal delivery. | Turkish music: instrumental Ney music played in the modal rhythm of Segah. | Labour duration was significantly shorter in the Ney music group compared with the control group (p ≤ 0.05). Ney music decreased anxiety and pain. |
| Browning (2001) [45] | N/A |
| N = 20 | N/A | LAS-E; MPS; TOMRI; Amount/frequency of medication requested; qualitative interviews. | Participants worked with a music therapist to choose music that was soothing/relaxing. A cassette player was used to play music during labour. Sony Walkman was provided if participants wanted to go outside of the birthing room during labour. Six 90-min tapes of recorded music were provided. | Participants in the control group had the same treatment as those in the music intervention group and had a coach but no MT before labour. | Vaginal delivery. | Selection of anxiety-relieving and rhythmic music. | The music group demonstrated a significant increase in perceptions of control according to LAE-S scores (p = 0.01). The music group showed significantly higher levels of relaxation compared with the control group (p = 0.04). |
| Garcia-Gonzalez et al. (2018) [46] | Spain |
| N = 409 | Music: 31.85 Control: 30.90 | STAI; Childbirth parameters; birth size. | Music was to be listened to in a quiet room at home over the course of 14 sessions (each session was 40 min) three times weekly at a consistent time. | Participants underwent the same procedure as the experimental group but with no music intervention. | Vaginal delivery or caesarean section. | “Musical journey through pregnancy” by Gabriel F. Federico was played on a CD. | Pregnant women who received MT experienced lower levels of anxiety compared with those in the control group (p < 0.001). The MT group also had lower anxiety levels (p < 0.001). |
| (1.2) Music-based Interventions Compared with Other Therapies. | ||||||||||
| Kimber et al. (2008) [47] | England |
| N = 90 | Massage with relaxation: 30 Music with relaxation: 28 Control group: 30 | VAS; customised version of CBWS; LAS. | Participants were trained to focus on breathing and visualisation techniques. Music was used in place of massage during labour. | No music or massage intervention was used; however, participants were encouraged to attend standard antenatal classes running at the site of the trial. | Vaginal delivery. | The mother and her birthing partner picked their favourite music to play during labour. | No significant differences were observed between the massage, music, and control groups. |
| Estrella-Juarez et al. (2023) [48] | New Zealand |
| N = 343 | Music: 32.38 VR: 31.10 Control: 31.60 | Childbirth parameters. | Women in the music intervention group listened to music via iPods, with overhead headphones worn, in 20-minute intervals during the first stage of labour. | Participants received the same level of support during the initial phase of labour as the other groups; however, no MT was administered. | Vagina delivery, instrumental, or C-section. | Instrumental piece of music called “musical journey through pregnancy” By Gabriel F. Federico. | Significant reduction in the length of the first stage of labour (p = 0.008), fewer episiotomies (p = 0.04), and fewer non-reassuring FHR tracings (p = 0.004) in the music intervention group compared with the control group. |
| Taghinejad et al. (2010) [49] | Iran |
| N = 101 | Massage: 21.3 Music: 21.5 | VAS. | When the woman’s cervix was 3–4 cm dilated (early active phase of labour), mothers listened to soft traditional music without lyrics, whilst wearing headphones, for half an hour. | Participants had no MT but received standard care of pain relief during the birth. | Vaginal delivery (active phase). | Participants had five types of soft traditional music to choose from. (Exact types of music not specified). | Massage and music therapy were both effective, but massage therapy was more effective than music at reducing subjective pain (p = 0.011). |
| Dehcheshmeh and Rafiei (2015) [50] | Iran |
| N = 112 | Music intervention: 21.43 Ice massage: 22.30 Control: 22.90 | VAS. | Participants listened to music via headphones for half an hour in a selected room. | Participants received standard labour care without any additional intervention. | Vaginal delivery. | In line with participant preferences, women could listen to either piano music or wave sounds. | Participants in the music intervention group showed significant decreases in pain intensity at three time points i.e., 4 cm dilation, 6 cm dilation, and 8 cm dilation (p = 0.001). The music intervention group experienced lower pain levels at all three time points compared with the control group (p < 0.05). The average total pain intensity scores were lower in the music group. |
| Wan and Wen (2018) [51] | China |
| N = 238 | Acupressure: 26.18 Music: 25.57 Combination: 26.70 Control: 26.02 | VAS-S; VAS-P; VAS | Music was played continuously for 20 min followed by a 2 h break between sessions. | The control group completed all outcome measures but did not receive any additional interventions. | Vaginal delivery. | Participants were encouraged to choose either relaxing, soft, or regular rhythmic music. | VAS-A anxiety scores in the music group and the group that received music plus acupressure were significantly lower than in the control group (all p < 0.05). Pain scores from VAS-P in music, acupressure, and combination groups significantly decreased (all p < 0.05) compared with the control group. VAS-P scores in the acupressure group were statistically lower than those in the music group at 1, 4, and 8 h (all p < 0.05). |
| Gönenç and Dikmen (2020) [52] | Turkey |
| N = 99 | Most participants in all three groups were between 18 and 24 years. | VAS; W-DEQA; LMF. | In both the dance and music and the music-only groups, participants were asked to select three songs they liked. Music was played for 30 min via headphones once cervical dilation had reached 4–5 cm. | Participants received standard care involving monitoring of labour progression, vital signs, and foetal heart tones. | Vaginal delivery (Active phase). | A range of upbeat pop music, slow pop music, Turkish folk music, and religious music was selected in both the dance and music group and the music-only group. | Dance plus music and music only reduced labour pain and fear during the active phase of labour (both p < 0.001). |
| (1.3) Music-based Interventions as Part of a Larger Therapy. | ||||||||||
| Guo et al. (2022) [27] | China |
| N = 440 | Music/free delivery: 27.85 Traditional delivery: 27.99 | PLPQ; Apgar score; perineal score; amount of bleeding 2 h post birth. | A music therapist personalised the music therapy based on the mothers’ experiences and likings. Different types of music were played during the first, second, and third phases of labour. | Traditional therapy group: standard labour practices were implemented with no music intervention. | Vaginal delivery. | First phase of labour: relaxing/hypnotic music was played. Late stage of the first phase of labour: intense rhythmic music was played. Second/third phase of labour: parent–child music was played. | MT combined with free position during labour resulted in statistically lower levels of pain response (p < 0.01) and total pain scores in mothers (p < 0.05). |
| Perkovic et al. (2021) [53] | Bosnia |
| N = 175 | Music: 31.4 Control: 30.9 | VAS; SCL-90. | Music was part of a group education intervention. It involved participants listening to their choice of classical music for 15 min before bedtime. | Participants received routine prenatal care and usual obstetric practices exclusive of additional interventions | Vaginal delivery. | Classical music | Women who took midwifery education classes and listened to classical music during pregnancy described pain as moderate compared with those in the control group, who rated their pain as severe. |
| (2) Studies Investigating the Effect of Music-based Interventions During Caesarean Section. | ||||||||||
| (2.1) Studies That Used Participant-selected Music During Caesarean Section. | ||||||||||
| Kaur et al. (2023) [54] | N/A |
| N = 60 | Music: 26.63 Control: 26.17 | VAS-A; serum cortisol levels; hemodynamic parameter. | Participants listened to music via headphones for the duration of the C-section under spinal anaesthesia. | No music was played but headphones were still worn. | Caesarean section. | Patient-chosen music (folk, Hindi film music, or religious songs). | In the music group, the levels of serum cortisol post-surgery did not differ from the pre-C-section levels (p = 0.583). Anxiety scores in the music group decreased significantly (p < 0.001) pre-and-post-surgery. Post-surgery differences in anxiety scores in the music and control groups were statistically significant (p = 0.0001). |
| Eren et al. (2018) [55] | Turkey |
| N = 60 | Music: 30.63 Control: 30.03 | VAS; vital findings. | Songs were played via stereo speaker throughout the C-sections. | Standard care was given to participants without MT. | Planned caesarean section. | Participants’ favourite songs. | Statistically significant reductions in body temperature (p = 0.00), anxiety score (p = 0.022), SBP (p = 0.003), and DBP (p = 0.011) in both pre-and post-C-section and an increase in OSL (p = 0.017) in participants in the music group. |
| (2.2)Studies That Used Participant-selected Prespecified Music During Caesarean Section. | ||||||||||
| Hepp et al. (2018) [56] | Germany |
| N = 305 | 33.6 | STAI; VAS-A; Salvia samples. | Music was played via CD player as soon as participants entered the operating theatre. | Participants received standard treatment with no music intervention. | Caesarean section. | Women selected their preferred music genre from either classical, jazz, lounge, or meditation music. | The music group displayed significantly less anxiety than the control group (p = 0.004). At skin incision, the music group had significantly lower SBP (p = 0.002) and HR (p = 0.049) compared with controls. |
| Chang and Chen (2005) [57] | Taiwan |
| N = 64 | Music: 30.31 Control: 32.31 | VASA; Physiological indexes; SCDS | Music was delivered from a portable compact disk player via headphones from the beginning of anaesthesia administration and throughout the C-section. | Participants were unaware of a music option but received standard nursing care and regular communication with the researchers. | Caesarean section. | Participants chose one of the following anxiety-relieving music types: western classical, new-age, or Chinese religious. | Women in the music group experienced less anxiety than women in the control group at the end of maternal contact with the baby during the intraoperative period and post-skin-suture (p < 0.01). Participants in the music group also had higher SCDS scores, demonstrating increased satisfaction with the C-section (p < 0.01). |
| Denney et al. (2018) [58] | USA |
| N = 50 | Music: 29.9 Control: 31.2 | STAI; Physiological measures; qualitative questionnaire. | Music was played via a portable MP3 player whilst mothers were in the preoperative waiting area and postoperative recovery room. | Participants received standard preoperative care prior to the C-section without any music intervention. | Caesarean section. | Mothers in the music group had to choose a playlist from the following genres: classical, pop/top 40, R&B, country, soft rock, or gospel. | There was no statistically significant difference in state-anxiety scores between the music and control groups. When comparing the music group with the control group, participants talked about their deliveries in more positive ways relative to their previous delivery experiences (p = 0.046). |
| Li and Dong. (2012) [13] | China |
| N = 60 | N/A | SAS; HRV; VAS. | Participants listened to music for half an hour before undergoing surgery and continued to listen to music during the C-Section. | Participants did not receive music intervention; however, they were told to relax for 30 min in a quiet room before having the surgery. | Caesarean section. | Participants chose a piece of classical Chinese music. | Anxiety was significantly decreased after music intervention but not in the control group (p < 0.01). |
| Horasanlı and Demirbas (2022) [59] | Turkey |
| N = 49 | Music: 31.25 Control: 29.64 | STAI Vital signs: DBP, SBP, HR, RR, and OSL | Music was played via an earpiece prior to the administration of spinal anaesthesia. Music was played throughout the operation. | Participants did not receive music intervention but did listen to regular atmospheric white noise. | Caesarean section. | Sufi music with a steady rhythm. | Anxiety scores after C-section were significantly lower in the music group than in the control group (p < 0.001). No difference in anxiety before and after C-section in the control group (p < 0.001). |
| Kurdi and Gasti (2018) [60] | N/A |
| N = 189 | Group M: 25.4 Group B: 24.6 Group C: 24.5 | VAS-A; VAS-P; PONV; psychological wellbeing questionnaire. | Meditation music was played from an MP3 player via bilateral headphones covering the entire ear, ensuring that any noise interference from the operating theatre was kept to a minimum. | The control group listened to a blank MP3 player via headphones concealing the ear. | Caesarean section. | Group M: calming and soothing meditation music. Group B: Binaural beat meditation music. | Calming/soothing and beat meditation music were effective at reducing postoperative pain and anxiety in comparison to the control group at 6 h (both groups, p < 0.05) and 24 h (both groups, p < 0.05). However, participants in the music groups required pain-alleviating medication earlier than participants in the control group (both p < 0.05). |
| Abarghoee et al. (2022) [14] | Iran |
| N = 105 | BRT: 26.97 Music: 29.97 Control: 29.34 | SAI | Women were taken into a private room on their own and Music was played through an MP3 player for 20 min prior to the C-section. | Participants received only standard nursing care that sought to give in-depth explanations of the surgery procedure and recovery. | Caesarean section | The song “Weightless” by Macaroni Union was played as the nonverbal music for the Music group. | Significant reduction in anxiety after both the BRT (p < 0.001) and the music intervention compared with the control condition (p < 0.001). |
| (2.3) Studies That Used a Combination of Participant-selected and Participant-selected Prespecified Music During Caesarean Sections. | ||||||||||
| Halder et al. (2022) [61] | India |
| N = 60 | Music: 28.4 4 Control: 27.2 4 | VAS; VRS; NRS | Participants’ chosen music was played (for 20 min durations) via headphones during the preoperative, intraoperative, and postoperative stages. | Participants in the control group followed the same procedure as those in the experimental group but had no music intervention. | Caesarean section | Participants chose their preferred genre. If participants had no preference, they were asked to choose from vocal i.e., Indian classical, semi-classical, folk, light music, or instrumental i.e., single or multiple musical instruments. | VAS scores of postoperative pain were significantly lower in the music group at 1, 2, and 3 h post-surgery compared with the control group (p = 0.0003; p = 0.002; p = 0.02). Patients in the music group took, on average, 29 min longer than the control group before needing further pain-reducing medication (p = 0.017). |
| Category of Study | Main Relevant Findings |
|---|---|
| Music-based interventions as the experimental group compared with a control group. |
|
| Music-based interventions compared with other therapies. |
|
| Music-based interventions as part of a larger therapy. |
|
| Studies that used participant-selected music during caesarean sections. |
|
| Studies that examined participant-selected prespecified music during caesarean sections. |
|
| Studies that used researcher-pre-selected music during caesarean sections. |
|
| Studies that used a combination of participant-selected and participant-selected prespecified music during caesarean sections. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hunter, A.R.; Heiderscheit, A.; Galbally, M.; Gravina, D.; Mutwalli, H.; Himmerich, H. The Effects of Music-Based Interventions for Pain and Anxiety Management during Vaginal Labour and Caesarean Delivery: A Systematic Review and Narrative Synthesis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2023, 20, 7120. https://doi.org/10.3390/ijerph20237120
Hunter AR, Heiderscheit A, Galbally M, Gravina D, Mutwalli H, Himmerich H. The Effects of Music-Based Interventions for Pain and Anxiety Management during Vaginal Labour and Caesarean Delivery: A Systematic Review and Narrative Synthesis of Randomised Controlled Trials. International Journal of Environmental Research and Public Health. 2023; 20(23):7120. https://doi.org/10.3390/ijerph20237120
Chicago/Turabian StyleHunter, Amy Rose, Annie Heiderscheit, Megan Galbally, Davide Gravina, Hiba Mutwalli, and Hubertus Himmerich. 2023. "The Effects of Music-Based Interventions for Pain and Anxiety Management during Vaginal Labour and Caesarean Delivery: A Systematic Review and Narrative Synthesis of Randomised Controlled Trials" International Journal of Environmental Research and Public Health 20, no. 23: 7120. https://doi.org/10.3390/ijerph20237120