
Results from a Nationwide Evaluation Study of Labor Market-Integrative Health Promotion for the Unemployed: Impact of the JOBS Program Germany

Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design, Recruitment and Data Collection
2.2. Intervention
- Job-search skills training.
- Active teaching and learning methods.
- Trained trainers for program delivery.
- Supportive learning environment.
- Preparation for setbacks.
- Trainers provide continuous supportive feedback to participants and encourage appreciative, respectful interaction among the participants. They create an atmosphere of social support. Trainers also show empathy for participants’ concerns and feelings and encourage them to use appropriate coping strategies [29].
- Another training principle is the so-called “referent power”. The trainers strive to gain high esteem, trust and respect from the participants through competent teaching, self-revelation, the reduction of social distance and empathic support.
2.3. Predictor Variables and Outcome Measures
2.4. Statistical Analyses
3. Results
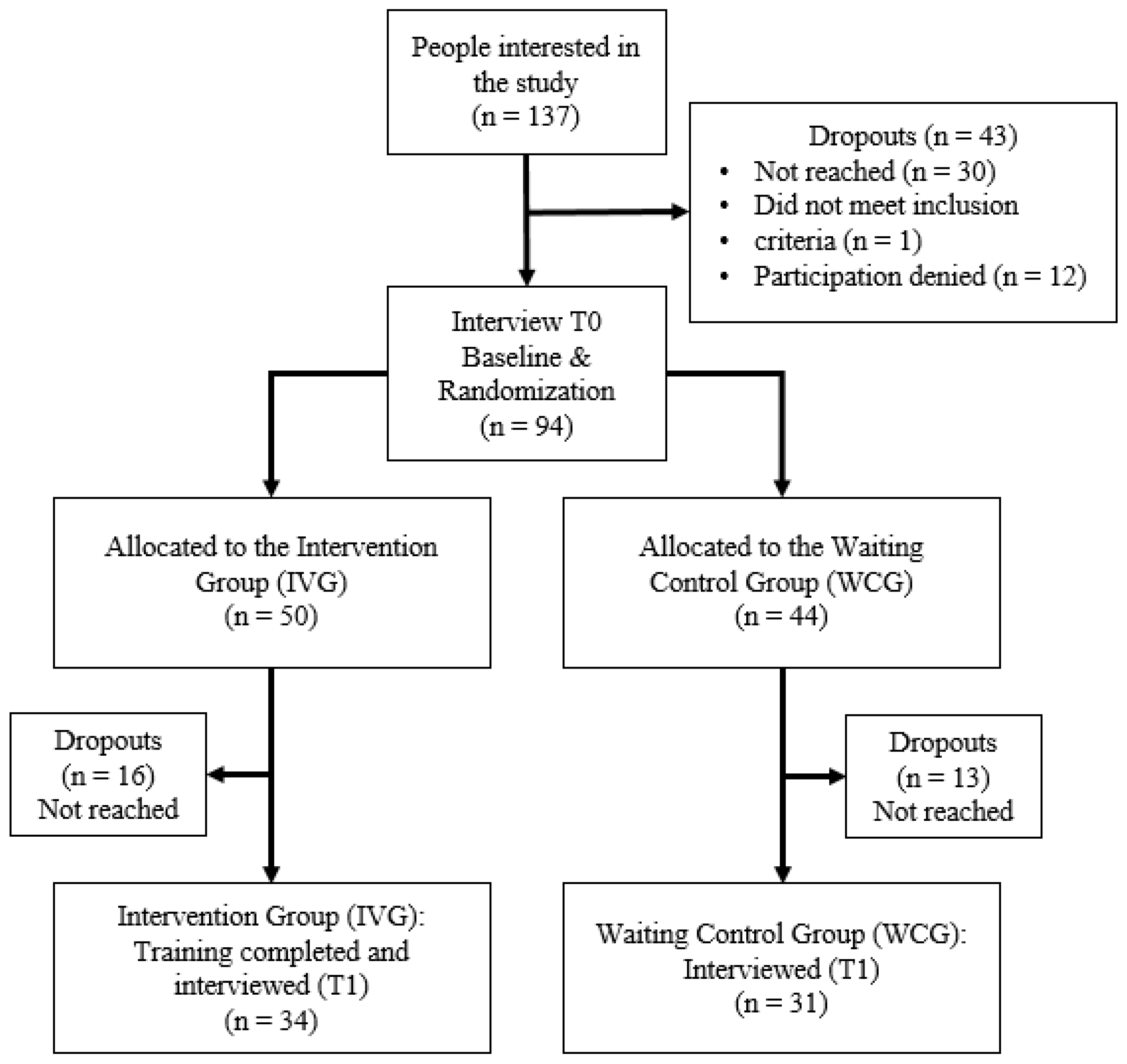
3.1. Participant Recruitment
3.2. Randomization and Dropout Analysis

{kind=link}
| IVG * | WCG * | ||||
|---|---|---|---|---|---|
| n = 50 | %/Mean | n = 44 | %/Mean | p-Value | |
| Age (Years), Mean (SD) | 50 | 44.6 (12.0) | 44 | 44.8 (11.78) | 0.964 |
| Gender 1 | |||||
| Male | 29 | 58.0 | 22 | 50.0 | |
| Female | 21 | 42.0 | 22 | 50.0 | 0.437 |
| Education | |||||
| Low Education | 19 | 38.0 | 17 | 38.6 | |
| Medium Education | 27 | 54.0 | 23 | 52.3 | |
| High Education | 4 | 8.0 | 4 | 9.1 | 0.976 |
| German citizenship | |||||
| Yes | 44 | 88 | 39 | 88.6 | |
| No | 6 | 12 | 5 | 11.4 | 0.924 |
| Duration of unemployment | |||||
| (Years), Mean (SD) | 50 | 6.27 (6.38) | 42 | 6.54 (5.84) | 0.605 |
3.3. Participant Characteristics
3.4. Bivariate Correlation Analysis
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Intervention | – | |||||||||||||
| 2. | Age (Years) | 0.044 | – | ||||||||||||
| 3. | Gender | −0.078 | −0.085 | – | |||||||||||
| 4. | Education | 0.090 | 0.363 ** | −0.113 | – | ||||||||||
| 5. | German Citizenship | 0.066 | 0.066 | −0.044 | 0.087 | – | |||||||||
| 6. | Duration of unemployment (Years) | −0.066 | 0.133 | 0.524 ** | −0.096 | 0.005 | – | ||||||||
| 7. | Job search-specific self-efficacy, T0 | −0.085 | −0.240 | −0.106 | −0.033 | 0.034 | −0.220 | – | |||||||
| 8. | Job search-specific self-efficacy, T1 | 0.139 | −0.210 | −0.258 * | 0.117 | 0.162 | −0.282 * | 0.501 ** | – | ||||||
| 9. | Life satisfaction, T0 | 0.190 | 0.077 | 0.078 | 0.053 | 0.123 | 0.111 | −0.054 | −0.015 | – | |||||
| 10. | Life satisfaction, T1 | 0.312 * | 0.087 | −0.024 | 0.007 | 0.318 ** | 0.021 | −0.139 | −0.049 | 0.606 ** | – | ||||
| 11. | General health status, T0 | 0.084 | −0.216 | −0.153 | 0.082 | 0.046 | −0.277 * | 0.174 | 0.314 * | 0.291 * | 0.350 ** | – | |||
| 12. | General health status, T1 | 0.172 | −0.138 | −0.173 | 0.236 | 0.207 | −0.244 | 0.100 | 0.248 | 0.216 | 0.307 * | 0.661 ** | – | ||
| 13. | Depressive symptoms, T0 | 0.044 | −0.006 | −0.150 | −0.020 | 0.260 * | 0.033 | 0.289 * | 0.192 | 0.368 ** | 0.422 ** | 0.327 ** | 0.350 ** | – | |
| 14. | Depressive symptoms, T1 | 0.305 * | −0.024 | −0.163 | 0.056 | 0.327 ** | −0.091 | 0.181 | 0.149 | 0.486 ** | 0.639 ** | 0.377 ** | 0.525 ** | 0.646 ** | – |
| Mean | 0.52 | 44.15 | 0.51 | 1.74 | 0.89 | 6.85 | 2.79 | 2.89 | 18.46 | 20.11 | 3.28 | 3.14 | 48.13 | 53.69 | |
| Standard Deviation | 0.50 | 11.70 | 0.50 | 0.62 | 0.31 | 6.61 | 0.95 | 0.93 | 6.18 | 6.69 | 0.96 | 1.01 | 23.74 | 26.14 | |
| Number of cases | 65 | 65 | 65 | 65 | 65 | 64 | 61 | 61 | 65 | 65 | 65 | 65 | 63 | 64 |
3.5. IVG vs. WCG Differences at T0 and T1 and Outcome Changes from T0 to T1 in Both Groups
| T0 1 | T1 2 | ∆T0 to T1 3 | |||||
|---|---|---|---|---|---|---|---|
| Outcome | IVG | WCG | p-Value | IVG | WCG | p-Value | p-Value |
| Job search-specific self-efficacy | 2.72 (n = 32) | 2.86 (n = 29) | 0.511 | 3.03 (n = 33) | 2.71 (n = 28) | 0.280 | IVG: 0.049 * (pairs: n = 31) WCG: 0.593 (pairs: n = 27) |
| Life satisfaction | 19.44 (n = 34) | 17.39 (n = 31) | 0.183 | 22.06 (n = 34) | 17.97 (n = 31) | 0.012 * | IVG: 0.017 * (pairs: n = 34) WCG: 0.545 (pairs: n = 31) |
| General health status | 3.38 (n = 34) | 3.16 (n = 31) | 0.504 | 3.29 (n = 34) | 2.97 (n = 31) | 0.170 | IVG: 0.614 (pairs: n = 34) WCG: 0.175 (pairs: n = 31) |
| Depressive symptoms | 49.21 (n = 33) | 46.93 (n = 30) | 0.730 | 61.06 (n = 34) | 45.33 (n = 30) | 0.015 * | IVG: 0.002 * (pairs: n = 33) WCG: 0.935 (pairs: n = 30) |
3.6. Intervention Effect on Job Search-Specific Self-Efficacy and Health-Related Outcomes
| Independent Variables (Baseline) | Job Search-Specific Self-Efficacy (n = 54) | Life Satisfaction (n = 61) | ||||
|---|---|---|---|---|---|---|
| M1 | M2 | M3 | M1 | M2 | M3 | |
| Intervention 1 (yes vs. no) | 0.449 * | 0.338 | 0.344 | 2.774 * | 2.736 * | 7.743 * |
| Baseline control of outcome | 0.525 *** | 0.451 ** | 0.512 ** | 0.613 *** | 0.493 *** | 0.488 *** |
| Age | −0.014 | −0.017 | 0.029 | 0.023 | ||
| Gender (female vs. male) 2 | −0.332 | −0.351 | −0.415 | 0.603 | ||
| Education | ||||||
| low vs. high | −0.768 | −0.778 | 2.645 | 2.703 | ||
| medium vs. high | −0.672 | −0.642 | 2.865 | 3.071 | ||
| Citizenship (yes vs. no) | 0.488 | 0.560 | 4.544 * | 4.930 * | ||
| Duration of unemployment 3 | −0.004 | −0.025 | 0.012 | 0.028 | ||
| Depressive Symptoms | 0.001 | 0.004 | 0.058 | 0.103 * | ||
| Interactions | ||||||
| Intervention × Dur_Unempl 4 | 0.047 | −0.110 | ||||
| Intervention × Depression 5 | −0.007 | −0.088 | ||||
| R2 | 0.314 | 0.449 | 0.473 | 0.408 | 0.510 | 0.531 |
| adjusted R2 | 0.288 | 0.339 | 0.338 | 0.388 | 0.425 | 0.428 |
| Significant change in F? (y/n) 6 | y | n | n | y | n | n |
| Independent Variables (Baseline) | General Health Status (n = 59) | Depressive Symptoms (n = 61) | ||||
|---|---|---|---|---|---|---|
| M1 | M2 | M3 | M1 | M2 | M3 | |
| Intervention 1 (yes vs. no) | 0.378 * | 0.337 * | 0.847 * | 15.073 ** | 14.524 ** | 30.341 * |
| Baseline control of outcome | 0.709 *** | 0.631 *** | 0.593 *** | 0.713 *** | 0.704 *** | 0.849 *** |
| Age | −0.007 | −0.012 | 0.091 | 0.064 | ||
| Gender (female vs. male) 2 | −0.093 | −0.016 | 2.592 | 5.744 | ||
| Education | ||||||
| low vs. high | −0.440 | −0.468 | 4.591 | 4.732 | ||
| medium vs. high | −0.106 | −0.090 | 9.729 | 10.388 | ||
| Citizenship (yes vs. no) | 0.271 | 0.322 | 13.174 | 14.511 | ||
| Duration of unemployment 3 | −0.007 | −0.021 | −0.434 | −0.424 | ||
| Depressive Symptoms | 0.001 | 0.008 | ― 7 | ― 7 | ||
| Interactions | ||||||
| Intervention × Dur_Unempl 4 | 0.021 | −0.259 | ||||
| Intervention × Depression 5 | −0.013 | −0.291 | ||||
| R2 | 0.582 | 0.627 | 0.651 | 0.524 | 0.573 | 0.588 |
| adjusted R2 | 0.568 | 0.559 | 0.571 | 0.508 | 0.509 | 0.508 |
| Significant change in F? 6 (y/n) | y | n | n | y | n | n |
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- BA. Statistik der Bundesagentur für Arbeit: Berichte: Blickpunkt Arbeitsmarkt—Monatsbericht zum Arbeits—Und Ausbildungsmarkt, Nürnberg, August 2023; Berichte: Blickpunkt Arbeitsmarkt, Nürnberg, 2023; Available online: https://statistik.arbeitsagentur.de/Statistikdaten/Detail/202308/arbeitsmarktberichte/monatsbericht-monatsbericht/monatsbericht-d-0-202308-pdf.pdf?__blob=publicationFile&v=3 (accessed on 9 September 2023).
- Kroll, L.E.; Müters, S.; Lampert, T. Unemployment and Health: An overview of current research results and data from the 2010 and 2012 German Health Update. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2016, 59, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Michalski, N.; Müters, S.; Wachtler Hoebel, J. Kap. 9.2 Gesundheitliche Ungleichheit. In Datenreport 2021: Ein Sozialbericht für die Bundesrepublik Deutschland; Statistisches Bundesamt (Destatis), Wissenschaftszentrum Berlin für Sozialforschung (WZB), Bundesinstitut für Bevölkerungsforschung (BiB), Eds.; Bundeszentrale für politische Bildung, publisher: Bonn, Germany, 2021; pp. 334–345. [Google Scholar]
- Roelfs, D.J.; Shor, E.; Davidson, K.W.; Schwartz, J.E. Losing life and livelihood: A systematic review and meta-analysis of unemployment and all-cause mortality. Soc. Sci. Med. 2011, 72, 840–854. [Google Scholar] [CrossRef] [PubMed]
- Garcy, A.M.; Vågerö, D. The length of unemployment predicts mortality, differently in men and women, and by cause of death: A six year mortality follow-up of the Swedish 1992–1996 recession. Soc. Sci. Med. 2012, 74, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Page, A.; Lamontagne, A.D. Cause and effect in studies on unemployment, mental health and suicide: A meta-analytic and conceptual review. Psychol. Med. 2014, 44, 909. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, S.; Treloar, A.; Hawgood, J.; Ross, V.; Kõlves, K. The Role of Unemployment, Financial Hardship, and Economic Recession on Suicidal Behaviors and Interventions to Mitigate Their Impact: A Review. Front. Public Health 2022, 10, 907052. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- Nolte-Troha, C.; Roser, P.; Henkel, D.; Scherbaum, N.; Koller, G.; Franke, A.G. Unemployment and Substance Use: An Updated Review of Studies from North America and Europe. Healthcare 2023, 11, 1182. [Google Scholar] [CrossRef]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Kim, T.J.; von dem Knesebeck, O. Perceived job insecurity, unemployment and depressive symptoms: A systematic review and meta-analysis of prospective observational studies. Int. Arch. Occup. Environ. Health 2016, 89, 561–573. [Google Scholar] [CrossRef]
- McKee-Ryan, F.; Song, Z.; Wanberg, C.R.; Kinicki, A.J. Psychological and physical well-being during unemployment: A meta-analytic study. J. Appl. Psychol. 2005, 90, 53–76. [Google Scholar] [CrossRef]
- Lamberg, T.; Virtanen, P.; Vahtera, J.; Luukkaala, T.; Koskenvuo, M. Unemployment, depressiveness and disability retirement: A follow-up study of the Finnish HeSSup population sample. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.I.; Scholl, H.; Moser, K.; Zechmann, A.; Batinic, B. Employment status, psychological needs, and mental health: Meta-analytic findings concerning the latent deprivation model. Front. Psychol. 2023, 14, 1017358. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Lorgelly, P.; Jasim, S.; Morris, T.; Gomes, M. Does a working day keep the doctor away? A critical review of the impact of unemployment and job insecurity on health and social care utilisation. Eur. J. Health Econ. 2022, 24, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Virgolino, A.; Costa, J.; Santos, O.; Pereira, M.E.; Antunes, R.; Ambrósio, S.; Heitor, M.J.; Vaz Carneiro, A. Lost in transition: A systematic review of the association between unemployment and mental health. J. Ment. Health 2022, 31, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S. Unemployment associated with major depression disorder and depressive symptoms: A systematic review and meta-analysis. Int. J. Occup. Saf. Ergon. 2021, 28, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Hollederer, A. Gesundheit und Krankheit von Arbeitslosen sowie Chancen und Grenzen arbeitsmarktintegrativer Gesundheitsförderung. In Gesundheitsförderung bei Arbeitslosen, 1st ed.; Hollederer, A., Ed.; Fachhochschulverlag: Frankfurt am Main, Germany, 2021; pp. 12–35. ISBN 978-3-947273-39-3. [Google Scholar]
- Paul, K.I. The Negative Mental Health Effect of Unemployment: Meta-Analyses of Cross-Sectional and Longitudinal Data. Doctoral Dissertation, Friedrich-Alexander-Universität Erlangen-Nürnberg, Nürnberg, Germany, 2005. [Google Scholar]
- Jahoda, M. Wieviel Arbeit Braucht der Mensch?: Arbeit und Arbeitslosigkeit im 20. Jahrhundert; Beltz: Weinheim, Germany, 1983; ISBN 3407850336. [Google Scholar]
- Warr, P. A conceptual framework for the study of work and mental health. Work Stress 1994, 8, 84–97. [Google Scholar] [CrossRef]
- Warr, P. Work, Unemployment and Mental Health; Oxford University Press: Oxford, UK; Clarendon Press: Oxford, UK, 1987; ISBN 0198521588. [Google Scholar]
- Warr, P. Jobs and job-holders: Two sources of happiness and unhappiness. In Oxford Handbook of Happiness; Boniwell, I., David, S.A., Ayers, A.C., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 733–750. ISBN 9780199557257. [Google Scholar]
- Fryer, D. Employment deprivation and personal agency during unemployment: A critical discussion of Jahoda’s explanation of the psychological effects of unemployment. Soc. Behav. 1986, 1, 3–23. [Google Scholar]
- Paul, K.I.; Hollederer, A. The Effectiveness of Health-Oriented Interventions and Health Promotion for Unemployed People—A Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6028. [Google Scholar] [CrossRef]
- Hollederer, A. Health promotion and prevention among the unemployed: A systematic review. Health Promot. Int. 2019, 34, 1078–1096. [Google Scholar] [CrossRef] [PubMed]
- Hult, M.; Lappalainen, K.; Saaranen, T.K.; Räsänen, K.; Vanroelen, C.; Burdorf, A. Health-improving interventions for obtaining employment in unemployed job seekers. Cochrane Database Syst. Rev. 2020, 1, 1465–1858. [Google Scholar] [CrossRef] [PubMed]
- Arena, A.F.; Mobbs, S.; Sanatkar, S.; Williams, D.; Collins, D.; Harris, M.; Harvey, S.B.; Deady, M. Mental health and unemployment: A systematic review and meta-analysis of interventions to improve depression and anxiety outcomes. J. Affect. Disord. 2023, 335, 450–472. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.; Wishart, P.; Gingrich, J. JOBS: A Manual for Teaching People Successful Job Search Strategies: JOBS Implementation Manual, 2nd ed.; Michigan Prevention Research Center (MPRC), Institute for Social Research, University of Michigan, Eds.; University of Michigan Regents: Ann Arbor, MI, USA, 1999. [Google Scholar]
- Caplan, R.D.; Vinokur, A.D.; Price, R.H.; van Ryn, M. Job seeking, reemployment, and mental health: A randomized field experiment in coping with job loss. J. Appl. Psychol. 1989, 74, 759–769. [Google Scholar] [CrossRef]
- Vinokur, A.D.; Price, R.H.; Schul, Y. Impact of the JOBS Intervention on Unemployed Workers Varying in Risk for Depression. Am. J. Community Psychol. 1995, 23, 39–74. [Google Scholar] [CrossRef] [PubMed]
- van Ryn, M.; Vinokur, A.D. How did it work? An examination of the mechanisms through which an intervention for the unemployed promoted job-search behavior. Am. J. Community Psychol. 1992, 20, 577–597. [Google Scholar] [CrossRef]
- Vinokur, A.D.; van Ryn, M.; Gramlich, E.M.; Price, R.H. Long-term follow-up and benefit-cost analysis of the Jobs Program: A preventive intervention for the unemployed. J. Appl. Psychol. 1991, 76, 213–219. [Google Scholar] [CrossRef]
- Price, R.H.; van Ryn, M.; Vinokur, A.D. Impact of a preventive job search intervention on the likelihood of depression among the unemployed. J. Health Soc. Behav. 1992, 33, 158–167. [Google Scholar] [CrossRef]
- Vuori, J.; Silvonen, J.; Vinokur, A.D.; Price, R.H. The Työhön Job Search Program in Finland: Benefits for the unemployed with risk of depression or discouragement. J. Occup. Health Psychol. 2002, 7, 5–19. [Google Scholar] [CrossRef]
- Vuori, J.; Silvonen, J. The benefits of a preventive job search program on re-employment and mental health at 2-year follow-up. J. Occup. Organ. Psychol. 2005, 78, 43–52. [Google Scholar] [CrossRef]
- Shirom, A.; Vinokur, A.; Price, R.H. Self-Efficacy as a Moderator of the Effects of Job-Search Workshops on Re-Employment: A Field Experiment1. J. Appl. Soc. Psychol. 2008, 38, 1778–1804. [Google Scholar] [CrossRef]
- Reynolds, C.; Barry, M.M.; Nic Gabhainn, S. Evaluating the impact of the winning new jobs programme on the re-employment and mental health of a mixed profile of unemployed people. Int. J. Ment. Health Promot. 2010, 12, 32–41. [Google Scholar] [CrossRef]
- Brenninkmeijer, V.; Blonk, R.W.B. The effectiveness of the JOBS program among the long-term unemployed: A randomized experiment in the Netherlands. Health Promot. Int. 2012, 27, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Price, R.H.; Vinokur, A.D. The JOBS program: Impact on job seeker motivation reemployment, and mental health. In Oxford Handbook of Job Loss and Job Search; Oxford University Press: Oxford, UK, 2014; pp. 575–590. [Google Scholar]
- Paver, R.; de Witte, H.; Rothmann, S.; van den Broeck, A.; Blonk, R.W.B. The implementation and evaluation of the South African adaptation of the JOBS program. Front. Psychol. 2020, 11, 1418. [Google Scholar] [CrossRef] [PubMed]
- Vinokur, A.D.; Schul, Y.; Vuori, J.; Price, R.H. Two years after a job loss: Long-term impact of the JOBS program on reemployment and mental health. J. Occup. Health Psychol. 2000, 5, 32–47. [Google Scholar] [CrossRef]
- Hollederer, A.; Jahn, H.J.; Klein, D. JOBS Program Germany for health promotion among the unemployed in the community setting with institutions for employment promotion (JobsProgramDtl): Study protocol for a randomized controlled trial. BMC Public Health 2021, 21, 261. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Learning Theory; Prentice-Hall: Oxford, UK, 1977; ISBN 0138167516. [Google Scholar]
- Bandura, A.; Stanford, U. Social cognitive theory of personality. In Handbook of Personality—Theory and Research, 2nd ed.; Pervin, L.A., John, O.J., Eds.; Guilford Press: New York, NY, USA, 1999; pp. 154–196. ISBN 1-57230-483-9. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of Thought and Action; Prentice Hall: Englewood Cliffs, NJ, USA, 1986; Volume 1986, pp. 23–28. [Google Scholar]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- BZgA. GKV-Spitzenverband. In Mit Selbstvertrauen in die Jobsuche—JOBS Program: Trainingsmanual zur Erprobung; Adaptierte und übersetzte Fassung des Original-Trainingmanuals “JOBS: A Manual for Teaching People Successful job Search Strategies—JOBS implementation manual”; GKV-Spitzenverband: Berlin, Germany, 2021. [Google Scholar]
- Bohlinger, S. Internationale Standardklassifikation im Bildungswesen. BWB 2012, 41, 16–19. [Google Scholar]
- Eurostat. Glossary: International Standard Classification of Education (ISCED). Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:International_standard_classification_of_education_(ISCED) (accessed on 24 April 2023).
- Janke, S.; Glöckner-Rist, A. Deutsche Version der Satisfaction with Life Scale (SWLS): Zusammenstellung Sozialwissenschaftlicher Items und Skalen (ZIS); GESIS—Leibniz-Institut für Sozialwissenschaften: Mannheim, Germany, 2012. [Google Scholar] [CrossRef]
- EHEMU. The Minimum European Health Module: EHEMU Technical Report 2010_4.6. 2010. Available online: www.eurohex.eu/pdf/Reports_2010/2010TR4.6_Health%20Module.pdf (accessed on 24 April 2023).
- WHO. WHO (Five) Well-Being Index (1998 Version). 1998. Available online: https://www.psykiatri-regionh.dk/who-5/Documents/WHO-5%20questionaire%20-%20English.pdf (accessed on 24 April 2023).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother Psychosom 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE: Los Angeles, CA, USA, 2018; ISBN 9781526419521. [Google Scholar]
- Urban, D.; Mayerl, J. Angewandte Regressionsanalyse: Theorie, Technik und Praxis; Springer VS: Wiesbaden, Germany, 2018; ISBN 3658019158. [Google Scholar]
- Wan, F. Statistical analysis of two arm randomized pre-post designs with one post-treatment measurement. BMC Med. Res. Methodol. 2021, 21, 150. [Google Scholar] [CrossRef]
- van Breukelen, G.J.P. ANCOVA versus change from baseline: More power in randomized studies, more bias in nonrandomized studies corrected. J. Clin. Epidemiol. 2006, 59, 920–925. [Google Scholar] [CrossRef]
- McCoy, C.E. Understanding the Intention-to-treat Principle in Randomized Controlled Trials. West. J. Emerg. Med. 2017, 18, 1075–1078. [Google Scholar] [CrossRef] [PubMed]
- Brambor, T.; Clark, W.R.; Golder, M. Understanding Interaction Models: Improving Empirical Analyses. Polit. Anal. 2006, 14, 63–82. [Google Scholar] [CrossRef]
- Stoetzer, M.-W. Regressionsanalyse in der Empirischen Wirtschafts- und Sozialforschung Band 1; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 978-3-662-53823-4. [Google Scholar]
- Liu, S.; Huang, J.L.; Wang, M. Effectiveness of job search interventions: A meta-analytic review. Psychol. Bull. 2014, 140, 1009–1041. [Google Scholar] [CrossRef] [PubMed]
- Vinokur, A.D.; Price, R.H.; Caplan, R.D. From field experiments to program implementation: Assessing the potential outcomes of an experimental intervention program for unemployed persons. Am. J. Community Psychol. 1991, 19, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Barry, M.; Reynolds, C.; Sheridan, A.; Egenton, R. Implementation of the JOBS programme in Ireland. J. Public Ment. Health 2006, 5, 10–25. [Google Scholar] [CrossRef]
- Paver, R.; de Witte, H.; Rothmann, S.; van den Broeck, A.; Blonk, R. A systematic literature review of the implementation and evaluation of the JOBS programme: A suggested framework for South Africa. South Afr. J. Econ. Manag. Sci. 2020, 23, 1–13. [Google Scholar] [CrossRef]
- Choi, J.N.; Price, R.H.; Vinokur, A.D. Self-efficacy changes in groups: Effects of diversity, leadership, and group climate. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2003, 24, 357–372. [Google Scholar] [CrossRef]
- Vuori, J.; Vinokur, A.D. Job-search preparedness as a mediator of the effects of the Työhön Job Search Intervention on re-employment and mental health. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2005, 26, 275–291. [Google Scholar] [CrossRef]
- Proudfoot, J.; Guest, D.; Carson, J.; Dunn, G.; Gray, J. Effect of cognitive-behavioural training on job-finding among long-term unemployed people. Lancet 1997, 350, 96–100. [Google Scholar] [CrossRef]
- Brähler, E.; Mühlan, H.; Albani, C.; Schmidt, S. Teststatistische Prüfung und Normierung der deutschen Versionen des EUROHIS-QOL Lebensqualität-Index und des WHO-5 Wohlbefindens-Index. Diagnostica 2007, 53, 83–96. [Google Scholar] [CrossRef]
- Ware, J.E.; Davies, A.R. Monitoring Health Outcomes from the Patients’ Point of View: A Primer; Integrated Therapeutics Group, Incorporated: Kenilwork, NJ, USA, 1995. [Google Scholar]
- Hollederer, A.; Frempong, A.H.; Jahn, H.J. Challenges for health promotion among the unemployed: JOBS Program Germany as an example. Public Health Forum. 2023, 31, 175–180. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollederer, A.; Jahn, H.J. Results from a Nationwide Evaluation Study of Labor Market-Integrative Health Promotion for the Unemployed: Impact of the JOBS Program Germany. Int. J. Environ. Res. Public Health 2023, 20, 6835. https://doi.org/10.3390/ijerph20196835
Hollederer A, Jahn HJ. Results from a Nationwide Evaluation Study of Labor Market-Integrative Health Promotion for the Unemployed: Impact of the JOBS Program Germany. International Journal of Environmental Research and Public Health. 2023; 20(19):6835. https://doi.org/10.3390/ijerph20196835
Chicago/Turabian StyleHollederer, Alfons, and Heiko J. Jahn. 2023. "Results from a Nationwide Evaluation Study of Labor Market-Integrative Health Promotion for the Unemployed: Impact of the JOBS Program Germany" International Journal of Environmental Research and Public Health 20, no. 19: 6835. https://doi.org/10.3390/ijerph20196835