
Psychometric Properties of the Greek Version of the Connor–Davidson Resilience Scale (CD-RISC-10) in a Sample of Nurses

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Measures
The Connor–Davidson Resilience Scale (CD-RISC-10)
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Honzik, M.P. Life-span development. Annu. Rev. Psychol. 1984, 35, 309–331. [Google Scholar] [CrossRef] [PubMed]
- Richmond, G.B.; Beardslee, W.R. Research and practical implications for paediatricians. Dev. Behav. Pediatr. 1988, 9, 157–163. [Google Scholar]
- Beardslee, W.R. The role of self-understanding in resilient individuals: The development of a perspective. Am. J. Orthopsychiatry 1989, 59, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Psychosocial Resilience and protective mechanisms. Am. J. Orthopsychiatry 1987, 57, 316–331. [Google Scholar] [CrossRef]
- Caplan, G. Loss, stress, and mental health. Community Ment. Health J. 1990, 26, 27–48. [Google Scholar] [CrossRef]
- Earvolino-Ramirez, M. Resilience: A concept analysis. Nurs. Forum 2007, 42, 73–82. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef]
- Wagnild, G.M. The Resilience Scale User’s Guide for the US English Version of The Resilience Scale and the 14-Item Resilience Scale (RS-14); The Resilience Center: Worden, MT, USA, 2009. [Google Scholar]
- Wagnild, G.M. Resilience and successful ageing: Comparison among low- and high-income older adults. J. Gerontol. Nurs. 2003, 29, 42–49. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Fletcher, D.; Sarkar, M. Psychological resilience. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Luthar, S. Resilience in development: A synthesis of research across five decades. In Developmental Psychopathology: Risk, Disorder, and Adaptation, 2nd ed.; Cicchetti, D., Cohen, D.J., Eds.; John Wiley & Sons Inc.: New York, NY, USA, 2006; pp. 739–795. [Google Scholar]
- Manyena, S.B. The concept of resilience revisited. Disasters 2006, 30, 434–450. [Google Scholar] [CrossRef]
- Streb, M.; Häller, P.; Michael, T. PTSD in paramedics: Resilience and sense of coherence. Behav. Cogn. Psychother. 2014, 42, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and the relation with health: A systematic review. J. Epidemiol. Community Health 2006, 60, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Fransisco, CA, USA, 1987. [Google Scholar]
- Antonovsky, H.; Sagy, S. The development of a sense of coherence and its impact on responses to stress situations. J. Soc. Psychol. 1986, 126, 213–226. [Google Scholar] [PubMed]
- Ungar, M. The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. Am. J. Orthopsychiatry 2011, 81, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Garmezy, N. Stress resistant children: The search for protective factors. In Recent Research in Developmental Psychopathology, Book Suppl Number 4 to J Child Psychol Psych; Pergamon Press: Oxford, UK, 1985. [Google Scholar]
- Rutter, M. Resilience in the face of adversity: Protective factors and resistance to psychiatric disorders. Br. J. Psych. 1985, 147, 598–611. [Google Scholar] [CrossRef]
- Seligman, M.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef]
- Waysman, M.; Schwarzwald, J.; Solomon, Z. Hardiness: An examination of its relationship with positive and negative long-term changes following trauma. J. Trauma. Stress 2001, 14, 531–554. [Google Scholar] [CrossRef]
- Abiola, T.; Udofia, O. Psychometric assessment of the Wagnild and Young’s resilience scale in Kano, Nigeria. BMC Res. Notes 2011, 4, 509. [Google Scholar] [CrossRef]
- Damásio, B.F.; Borsa, J.C.; Da Silva, J.P. 14-item resilience scale (RS-14): Psychometric properties of the Brazilian version. J. Nurs. Meas. 2011, 19, 131–145. [Google Scholar] [CrossRef]
- Baldwin, D.R.; Jackson, D.; Okoh, I.; Cannon, R.L. Resiliency and optimism: An African American senior citizen’s perspective. J. Black Psychol. 2011, 37, 24–41. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Tugade, M.M.; Waugh, C.E.; Larkin, G.R. What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on 11 September 2001. J. Pers. Soc. Psychol. 2003, 84, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Scali, J.; Gandubert, C.; Ritchie, K.; Soulier, M.; Ancelin, M.L.; Chaudieu, I. Measuring resilience in adult women using the 10-items Connor-Davidson Resilience Scale (CD-RISC): Role of trauma exposure and anxiety disorders. PLoS ONE 2012, 7, e39879.15. [Google Scholar] [CrossRef]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J. Pers. Soc. Psychol. 2004, 86, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [PubMed]
- McCann, C.M.; Beddoe, E.; McCormick, K.; Huggard, P.; Kedge, S.; Adamson, C.; Huggard, J. Resilience in the health professions: A review of recent literature. Int. J. Well-Being 2013, 3, 60–81. [Google Scholar] [CrossRef]
- Ahern, N.R.; Kiehl, E.M.; Sole, M.L.; Byers, J. A review of instruments measuring resilience. Issues Compr. Pediatr. Nurs. 2006, 29, 103–125. [Google Scholar] [CrossRef]
- Losoi, H.; Turunen, S.; Waljas, M.; Helminen, M.; Ohman, J.; Julkunen, J.; Rosti-Otajarvi, E. Psychometric properties of the Finish version of the resilience scale and its short version. Psychol. Community Health 2013, 2, 1–10. [Google Scholar] [CrossRef]
- Wagnild, G.M. The Resilience Scale: User’s Guide for the US English Version of the Resilience Scale and the 14-Item Resilience Scale Ver. 3.33; Resilience Center: Rochester, MN, USA, 2016. [Google Scholar]
- Ntountoulaki, E.; Paika, V.; Kotsis, K.; Papaioannou, D.; Andreoulakis, E.; Fountoulakis, K.N.; Carvalho, A.F.; Hyphantis, T. The Greek version of the resilience scale (RS-14): Psychometric properties in three samples and associations with mental illness, suicidality, and quality of life. J. Psychol. Clin. Psychiatry 2017, 7, 00450. [Google Scholar] [CrossRef]
- Hurtes, K.P.; Allen, L.R. Measuring resiliency in youth: The resiliency attitudes and skills profile. Therap. Recreat. J. 2001, 35, 333–347. [Google Scholar]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M. A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? Int. J. Methods Psychiatr. Res. 2003, 12, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Oladipo, S.E.; Idemudia, E.S. Reliability and validity of Wagnild and Young’s resilience scale in a sample of Nigerian youth. J. Psychol. 2015, 6, 57–65. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Mealer, M.; Schmiege, S.; Meek, P. The Connor-Davidson Resilience Scale in critical care nurses: A psychometric analysis. J. Nurs. Meas. 2016, 24, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Cavadino, A.; Mackay, L.; Ward, K.; King, A.; Smith, M. Physical activity and personal factors associated with nurse resilience in intensive care units. J. Clin. Nurs. 2020, 29, 3246–3262. [Google Scholar] [CrossRef]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensive Crit. Care Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef]
- Cai, W.; Lianb, B.; Songa, X.; Houa, T.; Denga, G.; Lib, H. A cross-sectional study on mental health among health care workers during the outbreak of Corona Virus Disease 2019. Asian J. Psychiatry 2020, 51, 102–111. [Google Scholar] [CrossRef]
- Arrogante, O. Mediator effect of resilience between burnout and health in nursing staff. Enferm. Clin. 2014, 24, 283–289. [Google Scholar] [CrossRef]
- Mealer, M.; Jones, J.; Newman, J.; McFann, K.K.; Rothbaum, B.; Moss, M. The presence of resilience is associated with healthier psychological profile in intensive care unit (ICU) nurses: Results of a national survey. Int. J. Nurs. Stud. 2012, 49, 292–299. [Google Scholar] [CrossRef]
- Fuchs, A.; Abegglen, S.; Berger-Estilita, J.; Greif, R.; Eigenmann, H. Distress and resilience of healthcare professionals during the COVID-19 pandemic (DARVID): Study protocol for a mixed-methods research project. BMJ Open 2020, 10, e039832. [Google Scholar] [CrossRef]
- Wu, L.; Tan, Y.; Liu, Y. Factor structure and psychometric evaluation of the Connor-Davidson resilience scale in a new employee population of China. BMC Psychiatry 2017, 17, 49. [Google Scholar] [CrossRef]
- Yu, X.; Zhang, J. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Soc. Behav. Pers. 2007, 35, 19–30. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Tu, Z.; He, J.; Wang, Z.; Song, M.; Tian, J.; Wang, C.; Ba, J.; Shen, X. Psychometric properties of the 10-item Connor-Davidson Resilience Scale in Chinese military personnel. Front. Psychol. 2023, 14, 1163382. [Google Scholar] [CrossRef] [PubMed]
- Goins, R.T.; Gregg, J.J.; Fiske, A. Psychometric properties of the Connor-Davidson Resilience Scale with older American Indians: The native elder care study. Res. Aging 2013, 35, 123–143. [Google Scholar] [CrossRef] [PubMed]
- Coates, E.E.; Phares, V.; Dedrick, R.F. Psychometric properties of the Connor-Davidson Resilience Scale 10 among low-income, African American men. Psychol. Assess 2013, 25, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Dong, D.; He, J.; Zhong, X.; Yao, S. Psychometric properties of the 10-item Connor–Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J. Affect. Disord. 2020, 261, 211–220. [Google Scholar] [CrossRef]
- Rezaeipandari, H.; Mohammadpoorasl, A.; Morowatisharifabad, M.A.; Shaghaghi, A. Psychometric properties of the Persian version of abridged Connor-Davidson Resilience Scale 10 (CD-RISC-10) among older adults. BMC Psychiatry 2022, 22, 493. [Google Scholar] [CrossRef]
- Neyer, M.A.; Henry, R.S.; Carrier, M.; Kwakkenbos, L.; Wojeck, R.K.; Gietzen, A.; Gottesman, K.; Guillot, G.; Lawrie-Jones, A.; Mayes, M.D.; et al. Validity, reliability, and differential item functioning of English and French versions of the 10-Item Connor-Davidson Resilience Scale in systemic sclerosis: A scleroderma patient-centered intervention network cohort study. Arthritis Care Res. 2023. [Google Scholar] [CrossRef]
- Aloba, O.; Olabisi, O.; Aloba, T. The 10-Item Connor-Davidson Resilience Scale: Factorial structure, reliability, validity, and correlates among student nurses in southwestern Nigeria. J. Am. Psychiatr. Nurses Assoc. 2016, 22, 43–51. [Google Scholar] [CrossRef]
- Notario-Pacheco, B.; Solera-Martínez, M.; Serrano-Parra, M.D.; Bartolomé-Gutiérrez, R.; García-Campayo, J.; Martínez-Vizcaíno, V. Reliability and validity of the Spanish version of the 10-item Connor-Davidson Resilience Scale (10-item CD-RISC) in young adults. Health Qual. Life Outcomes 2011, 9, 63. [Google Scholar] [CrossRef]
- Tsigkaropoulou, E.; Douzenis, A.; Tsitas, N.; Ferentinos, P.; Liappas, I.; Michopoulos, I. Greek version of the Connor-Davidson Resilience Scale: Psychometric properties in a sample of 546 Subjects. In Vivo 2018, 32, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Duan, X.; Jiang, J.; Zeng, L.; Zhang, P.; Zhao, S. Experience in the development of nurses’ personal resilience: A meta-synthesis. Nurs. Open. 2023, 10, 2780–2792. [Google Scholar] [CrossRef] [PubMed]
- Sierra-García, E.; Sosa-Palanca, E.M.; Saus-Ortega, C.; Ruiz-Hontangas, A.; Juárez-Vela, R.; Gea-Caballero, V. Modulating elements of nurse resilience in population care during the COVID-19 Pandemic. Int. J. Env. Res. Public Health 2022, 19, 4452. [Google Scholar] [CrossRef]
- Dahl, K.; Nortvedt, L.; Schrøder, J.; Bjørnnes, A.K. Internationally educated nurses and resilience: A systematic literature review. Int. Nurs. Rev. 2022, 69, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Kaitelidou, D. Relationship between social support and resilience among nurses: A systematic review. Int. J. Caring Sci. 2022, 15, 1675–1681. [Google Scholar]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2020, 25, 3186–3191. [Google Scholar] [CrossRef]
- Baumgartner, H.; Homburg, C. Applications of structural equation modeling in marketing and consumer research: A review. Int. J. Res. Mark. 1996, 13, 139–161. [Google Scholar] [CrossRef]
- Brown, T. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Hu, L.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Yusoff, M.S.B.; Arifin, W.N.; Hadie, S.N.H. ABC of Questionnaire Development and Validation for Survey Research. Educ. Med. J. 2021, 13, 97–108. [Google Scholar] [CrossRef]
- Putnick, D.L.; Bornstein, M.H. Measurement invariance conventions and reporting: The state of the art and future directions for psychological research. Dev. Rev. 2016, 41, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Manomenidis, G.; Panagopoulou, E.; Montgomery, A. Resilience in nursing: The role of internal and external factors. J. Nurs. Manag. 2019, 27, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, L.A. Work engagement, moral distress, education level, and critical reflective practice in intensive care nurses. Nurs. Forum 2011, 46, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Xianyu, Y.; Lambert, V.A. Investigation of the relationships among workplace stressors, ways of coping, and the mental health of Chinese head nurses. Nurs. Health Sci. 2006, 8, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Afshari, D.; Nourollahi-darabad, M.; Chinisaz, N. Demographic predictors of resilience among nurses during the COVID-19 pandemic. Work 2021, 68, 297–303. [Google Scholar] [CrossRef]
- Lin, J.; Ren, Y.H.; Gan, H.J.; Chen, Y.; Huang, Y.F.; You, X.M. Factors associated with resilience among non-local medical workers sent to Wuhan, China during the COVID-19 outbreak. BMC Psychiatry 2020, 20, 417–423. [Google Scholar] [CrossRef]
- Hellenic Statistical Authority. Population-Housing Census. 2021. Available online: https://www.statistics.gr/en/2021-census-pop-hous (accessed on 10 July 2023).
- Zurlo, M.C.; Vallone, F.; Smith, A.P. Work-family conflict and psychophysical health conditions of nurses: Gender differences and moderating variables. Jpn. J. Nurs. Sci. 2020, 7, e12324. [Google Scholar] [CrossRef]
- Förster, C.; Duchek, S.; Geithner, S.; Krägler, M. Developing an integrated framework of healthcare leaders’ resilience. Rev. Manag. Sci. 2023, 17, 1765–1788. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender (n = 583) | ||
| Males | 282 | 48.4 |
| Females | 301 | 51.6 |
| Age (n = 577) | 45.8 a | 6.4 b |
| Living arrangement (n = 583) | ||
| Alone | 78 | 13.4 |
| With family/partner/spouse | 506 | 86.6 |
| Children (n = 565) | ||
| No | 141 | 25.0 |
| Yes | 424 | 75.0 |
| Job Position (n = 584) | ||
| Internal departments | 447 | 76.5 |
| ICU | 137 | 22.5 |
| MSc/PhD (n = 584) | ||
| No | 277 | 47.5 |
| Yes | 307 | 52.5 |
| Clinical experience (n = 577) | 14.1 a | 9.8 b |
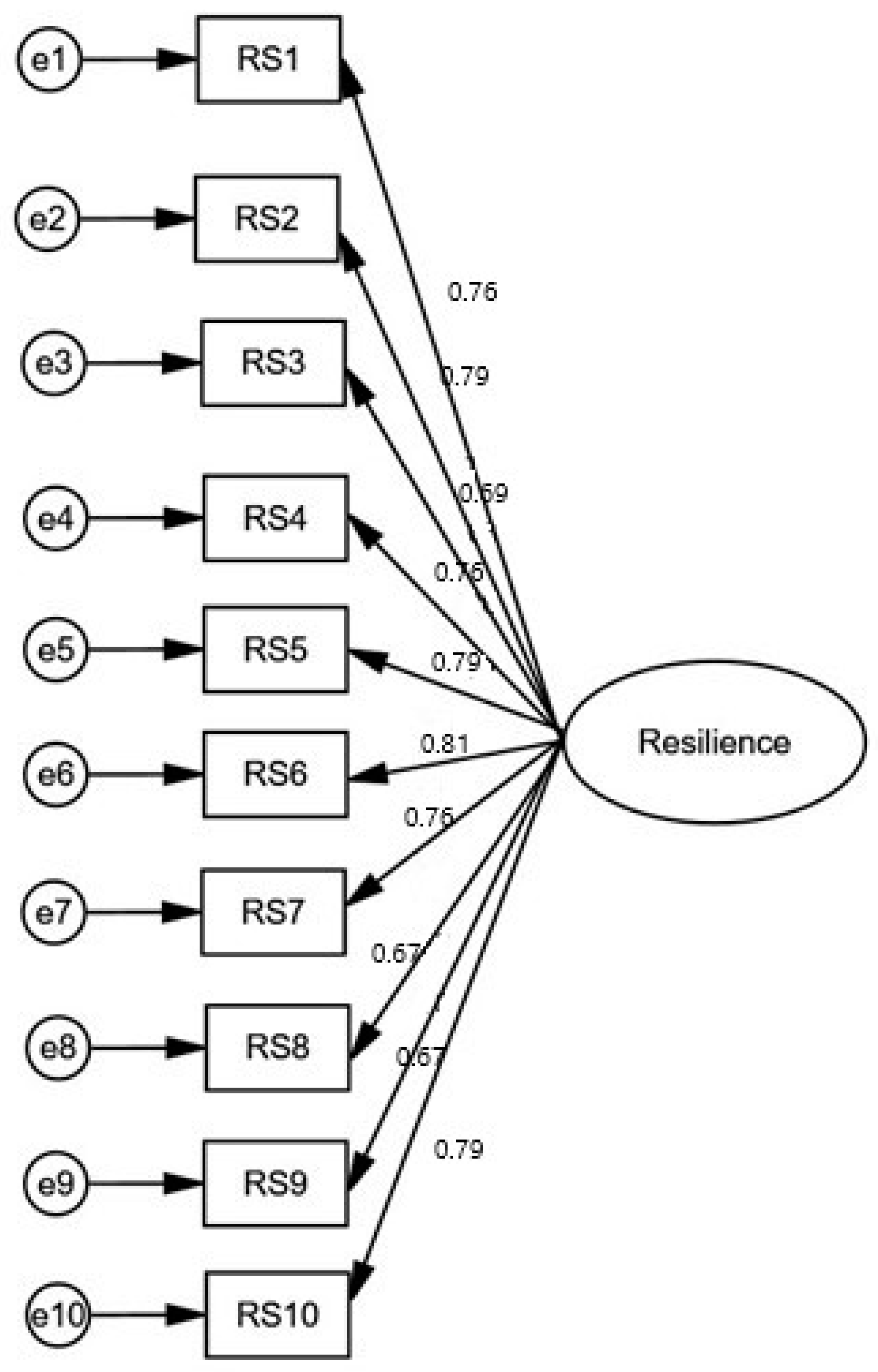
| CD-RISC-10 Items | Mean | Standard Deviation | Median | Skewness | Kurtosis | Factor Weights | Cronbach’s Alpha When a Single Item Was Deleted | Corrected Item–Total Correlation Coefficient |
|---|---|---|---|---|---|---|---|---|
| Adapt to change | 2.57 | 0.98 | 3 | −0.33 | −0.40 | 0.76 | 0.915 | 0.728 |
| Deal with whatever comes my way | 2.29 | 1.00 | 2 | −0.14 | −0.70 | 0.79 | 0.914 | 0.755 |
| See humorous side of things | 1.79 | 1.24 | 2 | 0.03 | −1.00 | 0.66 | 0.922 | 0.636 |
| Stress makes me stronger | 1.99 | 1.19 | 2 | −0.15 | −0.89 | 0.76 | 0.915 | 0.734 |
| Bounce back after illness or injury | 2.25 | 1.15 | 2 | −0.21 | −0.82 | 0.79 | 0.913 | 0.759 |
| Believe I can achieve goals despite obstacles | 2.44 | 0.97 | 2 | −0.17 | −0.35 | 0.81 | 0.913 | 0.776 |
| Under pressure, I stay focused | 2.33 | 0.92 | 2 | −0.09 | −0.19 | 0.76 | 0.916 | 0.721 |
| Not easily discouraged by failure | 2.06 | 0.99 | 2 | 0.06 | −0.35 | 0.67 | 0.920 | 0.637 |
| Think of myself as a strong person when facing challenges | 2.68 | 0.88 | 3 | −0.44 | 0.07 | 0.67 | 0.920 | 0.637 |
| Able to handle unpleasant feelings | 2.24 | 0.97 | 2 | −0.04 | −0.61 | 0.79 | 0.913 | 0.758 |
| Characteristics | Mean CD-RISC-10 Score | Standard Deviation | p-Value |
|---|---|---|---|
| Gender (n = 583) | 0.11 a | ||
| Males | 22.1 | 7.9 | |
| Females | 23.2 | 8.1 | |
| Age (n = 577) | 0.03 b | 0.50 b | |
| Living arrangement (n = 583) | 0.44 a | ||
| Alone | 24.0 | 8.1 | |
| With family/partner/spouse | 23.0 | 7.8 | |
| Children (n = 565) | <0.001 a | ||
| No | 20.6 | 7.4 | |
| Yes | 23.6 | 8.0 | |
| Job position (n = 584) | 0.46 | ||
| Internal departments | 22.5 | 7.9 | |
| ICU | 23.1 | 8.2 | |
| PhD/MSc (n = 584) | 0.02 a | ||
| No | 22.2 | 8.2 | |
| Yes | 23.8 | 7.5 | |
| Clinical experience (n = 577) | 0.03 c | 0.50 c |
| Independent Variables | Adjusted Coefficient Beta | 95% CI for Beta | p-Value |
|---|---|---|---|
| Females vs. males | 1.02 | −0.27 to 2.31 | 0.121 |
| Age | −0.37 | −1.55 to 0.80 | 0.533 |
| Living alone vs. living with others | 1.23 | −0.15 to 1.89 | 0.102 |
| Children | 4.06 | 2.46 to 5.67 | <0.001 |
| ICU vs. internal departments | 0.86 | 0.65 to 2.37 | 0.263 |
| PhD/MSc | 2.75 | 1.44 to 4.05 | <0.001 |
| Clinical experience | 0.04 | −0.07 to 0.15 | 0.446 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galanis, P.; Psomiadi, M.E.; Karagkounis, C.; Liamopoulou, P.; Manomenidis, G.; Panayiotou, G.; Bellali, T. Psychometric Properties of the Greek Version of the Connor–Davidson Resilience Scale (CD-RISC-10) in a Sample of Nurses. Int. J. Environ. Res. Public Health 2023, 20, 6752. https://doi.org/10.3390/ijerph20186752
Galanis P, Psomiadi ME, Karagkounis C, Liamopoulou P, Manomenidis G, Panayiotou G, Bellali T. Psychometric Properties of the Greek Version of the Connor–Davidson Resilience Scale (CD-RISC-10) in a Sample of Nurses. International Journal of Environmental Research and Public Health. 2023; 20(18):6752. https://doi.org/10.3390/ijerph20186752
Chicago/Turabian StyleGalanis, Petros, Maria Elissavet Psomiadi, Chrysovalantis Karagkounis, Polyxeni Liamopoulou, Georgios Manomenidis, Georgios Panayiotou, and Thalia Bellali. 2023. "Psychometric Properties of the Greek Version of the Connor–Davidson Resilience Scale (CD-RISC-10) in a Sample of Nurses" International Journal of Environmental Research and Public Health 20, no. 18: 6752. https://doi.org/10.3390/ijerph20186752