
Trend of Correlations between Psychological Symptoms and Socioeconomic Inequalities among Italian Adolescents: Cross-Sectional Study from 2006 to 2018 in Tuscany Region
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Sample
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Adolescent Health. 2023. Available online: https://www.who.int/health-topics/adolescent-health (accessed on 24 February 2023).
- Pajević, I.; Žigić, N.; Bećirović, E.; Pajević, A. Psychological Disorders in Childhood and Adolescent Age—New Classifications. Psychiatr. Danub. 2020, 32 (Suppl. S3), 311–315. [Google Scholar] [PubMed]
- Yu, B.; Wang, E. The Influencing Mechanism of Social and Cultural Adaptation for Chinese Migrant Children: A Longitudinal Intervention Study. Front. Psychol. 2022, 13, 832871. [Google Scholar] [CrossRef] [PubMed]
- Shannon, C.L.; Klausner, J.D. The growing epidemic of sexually transmitted infections in adolescents: A neglected population. Curr. Opin. Pediatr. 2018, 30, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Hayward, R. The invention of the psychosocial: An introduction. Hist. Hum. Sci. 2012, 25, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Peter, C.S.; Ashley, B. Defining and Measuring Social Capital for Young People: A Practical Review of the Literature on Resource-Full Relationships; Report for the Bill & Melinda Gates Foundation; Search Institute: Minneapolis, MN, USA, April 2020; p. 63. Available online: https://www.search-institute.org/wp-content/uploads/2020/05/SOCAP-Lit-Review.pdf (accessed on 11 April 2023).
- Marmot, M. Fair Society, Healthy Lives; The Annual Balzan Lecture; Leo S. Olschki: Florence, Italy, 2013. [Google Scholar]
- Eriksson, M. Social Capital and Health—Implications for Health Promotion. Glob. Health Action 2011, 4, 5611. [Google Scholar] [CrossRef]
- Morgan, A.R.; Rivera, F.; Moreno, C.; Haglund, B.J. Does Social Capital Travel? Influences on the Life Satisfaction of Young People Living in England and Spain. BMC Public Health 2012, 12, 138. [Google Scholar] [CrossRef] [Green Version]
- Stjernqvist, N.W.; Sabinsky, M.; Morgan, A.; Trolle, E.; Thyregod, C.; Maindal, H.T.; Bonde, A.H.; Tetens, I. Building School-Based Social Capital through ‘We Act—Together for Health’—a Quasi-Experimental Study. BMC Public Health 2018, 18, 1141. [Google Scholar] [CrossRef] [Green Version]
- Holstein, B.E.; Currie, C.; Boyce, W.; Damsgaard, M.T.; Gobina, I.; Kökönyei, G.; Hetland, J.; de Looze, M.; Richter, M.; Due, P.; et al. Socio-Economic Inequality in Multiple Health Complaints among Adolescents: International Comparative Study in 37 Countries. Int. J. Public Health 2009, 54, 260–270. [Google Scholar] [CrossRef]
- HBSC Study|Health Behaviour in School-Aged Children Study. Available online: https://hbsc.org/ (accessed on 25 February 2023).
- Lazzeri, G.; Vieno, A.; Charrier, L.; Spinelli, A.; Ciardullo, S.; Pierannunzio, D.; Galeone, D.; Nardone, P. The Methodology of the Italian Health Behaviour in School-Aged Children (HBSC) 2018 Study and Its Development for the next Round. J. Prev. Med. Hyg. 2022, 62, E926. [Google Scholar] [CrossRef]
- Trombetta, C.M.; Manini, I.; Pammolli, A.; Rossi, S.; Pozzi, T.; Montomoli, E.; Lazzeri, G. Medicine Use and Recurrent Complaints among 15-Years-Old Adolescents in Tuscany. Ann. Ist. Super. Sanita 2018, 54, 208–213. [Google Scholar] [CrossRef]
- Gariépy, G.; Elgar, F.J. Trends in Psychological Symptoms among Canadian Adolescents from 2002 to 2014: Gender and Socioeconomic Differences. Can. J. Psychiatry 2016, 61, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C.; The FAS Development Study Group. Psychometric Validation of the Revised Family Affluence Scale: A Latent Variable Approach. Child Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [Green Version]
- Mental Health. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 7 March 2023).
- Hashmi, R.; Alam, K.; Gow, J. Socioeconomic Inequalities in Mental Health in Australia: Explaining Life Shock Exposure. Health Policy 2020, 124, 97–105. [Google Scholar] [CrossRef]
- World Health Organization. The Economics of the Social Determinants of Health and Health Inequalities: A Resource Book; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Lemma, P.; Borraccino, A.; Berchialla, P.; Dalmasso, P.; Charrier, L.; Vieno, A.; Lazzeri, G.; Cavallo, F. Well-Being in 15-Year-Old Adolescents: A Matter of Relationship with School. J. Public Health 2014, 37, 573–580. [Google Scholar] [CrossRef] [Green Version]
- Voráčová, J.; Sigmund, E.; Sigmundová, D.; Kalman, M. Family Affluence and the Eating Habits of 11- to 15-Year-Old Czech Adolescents: HBSC 2002 and 2014. Int. J. Environ. Res. Public Health 2016, 13, 1034. [Google Scholar] [CrossRef] [Green Version]
- Levin, K.A.; Torsheim, T.; Vollebergh, W.; Richter, M.; Davies, C.A.; Schnohr, C.W.; Due, P.; Currie, C. National Income and Income Inequality, Family Affluence and Life Satisfaction Among 13 Year Old Boys and Girls: A Multilevel Study in 35 Countries. Soc. Indic. Res. 2011, 104, 179–194. [Google Scholar] [CrossRef] [Green Version]
- Hartley, J.E.K.; Levin, K.; Currie, C. A New Version of the HBSC Family Affluence Scale—FAS III: Scottish Qualitative Findings from the International FAS Development Study. Child Indic. Res. 2016, 9, 233–245. [Google Scholar] [CrossRef] [Green Version]
- Szreter, S. Health by Association? Social Capital, Social Theory, and the Political Economy of Public Health. Int. J. Epidemiol. 2004, 33, 650–667. [Google Scholar] [CrossRef]
- De Clercq, B.; Pfoertner, T.-K.; Elgar, F.J.; Hublet, A.; Maes, L. Social Capital and Adolescent Smoking in Schools and Communities: A Cross-Classified Multilevel Analysis. Soc. Sci. Med. 2014, 119, 81–87. [Google Scholar] [CrossRef]
- De Clercq, B.; Abel, T.; Moor, I.; Elgar, F.J.; Lievens, J.; Sioen, I.; Braeckman, L.; Deforche, B. Social Inequality in Adolescents’ Healthy Food Intake: The Interplay between Economic, Social and Cultural Capital. Eur. J. Public Health 2017, 27, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Cosma, A.; Költő, A.; Badura, P.; Winkler, P.; Kalman, M. Time Trends in Adolescent Mental Wellbeing in the Czech Republic between 2002 and 2018: Gender, Age and Socioeconomic Differences. Cent. Eur. J. Public Health 2021, 29, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Bersia, M.; Berchialla, P.; Charrier, L.; Lemma, P.; Borraccino, A.; Nardone, P.; Pierannunzio, D.; Ciardullo, S.; Comoretto, R.I.; Dalmasso, P. Mental Well-Being: 2010–2018 Trends among Italian Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 863. [Google Scholar] [CrossRef] [PubMed]
- Myhr, A.; Anthun, K.S.; Lillefjell, M.; Sund, E.R. Trends in Socioeconomic Inequalities in Norwegian Adolescents’ Mental Health From 2014 to 2018: A Repeated Cross-Sectional Study. Front. Psychol. 2020, 11, 1472. [Google Scholar] [CrossRef] [PubMed]
- Ahlborg, M.; Svedberg, P.; Nyholm, M.; Morgan, A.; Nygren, J.M. Socioeconomic Inequalities in Health among Swedish Adolescents—Adding the Subjective Perspective. BMC Public Health 2017, 17, 838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Droogenbroeck, F.; Spruyt, B.; Keppens, G. Gender Differences in Mental Health Problems among Adolescents and the Role of Social Support: Results from the Belgian Health Interview Surveys 2008 and 2013. BMC Psychiatry 2018, 18, 6. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, D.; Stevens, G.W.J.M.; Duinhof, E.L.; Finkenauer, C. Adolescent Socioeconomic Status and Mental Health Inequalities in the Netherlands, 2001–2017. Int. J. Environ. Res. Public Health 2019, 16, 3605. [Google Scholar] [CrossRef] [Green Version]
- Högberg, B.; Strandh, M.; Hagquist, C. Gender and Secular Trends in Adolescent Mental Health over 24 Years—The Role of School-Related Stress. Soc. Sci. Med. 2020, 250, 112890. [Google Scholar] [CrossRef]
- Högberg, B.; Lindgren, J.; Johansson, K.; Strandh, M.; Petersen, S. Consequences of School Grading Systems on Adolescent Health: Evidence from a Swedish School Reform. J. Educ. Policy 2021, 36, 84–106. [Google Scholar] [CrossRef]
- Wiklund, M.; Malmgren-Olsson, E.-B.; Öhman, A.; Bergström, E.; Fjellman-Wiklund, A. Subjective Health Complaints in Older Adolescents Are Related to Perceived Stress, Anxiety and Gender—A Cross-Sectional School Study in Northern Sweden. BMC Public Health 2012, 12, 993. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Cox, R.; Evans, R.E.; Hallingberg, B.; Hawkins, J.; Littlecott, H.J.; Long, S.J.; Murphy, S. School, Peer and Family Relationships and Adolescent Substance Use, Subjective Wellbeing and Mental Health Symptoms in Wales: A Cross Sectional Study. Child Indic. Res. 2018, 11, 1951–1965. [Google Scholar] [CrossRef] [Green Version]
- Zozaya, N.; Vallejo, L. The Effect of the Economic Crisis on Adolescents’ Perceived Health and Risk Behaviors: A Multilevel Analysis. Int. J. Environ. Res. Public Health 2020, 17, 643. [Google Scholar] [CrossRef] [Green Version]
- Elgar, F.J.; Craig, W.; Trites, S.J. Family Dinners, Communication, and Mental Health in Canadian Adolescents. J. Adolesc. Health 2013, 52, 433–438. [Google Scholar] [CrossRef]
- Matos, M.G.; Dadds, M.R.; Barrett, P.M. Family-Related School Issues and the Mental Health of Adolescents: Post Hoc Analyses of the Portuguese National Health Behaviour in School-Aged Children Survey Data 1. J. Fam. Stud. 2006, 12, 261–275. [Google Scholar] [CrossRef]
- Puntscher, S.; Hauser, C.; Walde, J.; Tappeiner, G. The Impact of Social Capital on Subjective Well-Being: A Regional Perspective. J. Happiness Stud. 2015, 16, 1231–1246. [Google Scholar] [CrossRef]
- Addae, E.A. The Mediating Role of Social Capital in the Relationship between Socioeconomic Status and Adolescent Wellbeing: Evidence from Ghana. BMC Public Health 2020, 20, 20. [Google Scholar] [CrossRef]
- Marbell-Pierre, K.N.; Grolnick, W.S.; Stewart, A.L.; Raftery-Helmer, J.N. Parental Autonomy Support in Two Cultures: The Moderating Effects of Adolescents’ Self-Construals. Child Dev. 2019, 90, 825–845. [Google Scholar] [CrossRef]
- Di Domenico, S.I.; Fournier, M.A. Socioeconomic Status, Income Inequality, and Health Complaints: A Basic Psychological Needs Perspective. Soc. Indic. Res. 2014, 119, 1679–1697. [Google Scholar] [CrossRef]
- Buijs, T.; Maes, L.; Salonna, F.; Van Damme, J.; Hublet, A.; Kebza, V.; Costongs, C.; Currie, C.; De Clercq, B. The Role of Community Social Capital in the Relationship between Socioeconomic Status and Adolescent Life Satisfaction: Mediating or Moderating? Evidence from Czech Data. Int. J. Equity Health 2016, 15, 203. [Google Scholar] [CrossRef] [Green Version]
- Ge, T. Effect of Socioeconomic Status on Children’s Psychological Well-Being in China: The Mediating Role of Family Social Capital. J. Health Psychol. 2020, 25, 1118–1127. [Google Scholar] [CrossRef]
- Moore, G.F.; Littlecott, H.J.; Evans, R.; Murphy, S.; Hewitt, G.; Fletcher, A. School Composition, School Culture and Socioeconomic Inequalities in Young People’s Health: Multi-Level Analysis of the Health Behaviour in School-Aged Children (HBSC) Survey in Wales. Br. Educ. Res. J. 2017, 43, 310–329. [Google Scholar] [CrossRef] [Green Version]
- United Nations. COVID-19 and the Need for Action on Mental Health. 2020, p. 17. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health.pdf (accessed on 11 April 2023).
- Scabini, E.; Iafrate, R. Psicologia dei Legami Familiari, Nuova Editione; Itinerari; Il Mulino: Bologna, Italy, 2019. [Google Scholar]


{kind=link}
| 2006, n (%) | 2010, n (%) | 2014, n (%) | 2018, n (%) | ||
|---|---|---|---|---|---|
| Girls | |||||
| Family affluence scale | Low | 305 (16.9) | 128 (8.1) | 230 (17.5) | 231 (14.6) |
| Medium | 1092 (60.5) | 869 (54.7) | 785 (59.7) | 989 (62.5) | |
| High | 408 (22.6) | 592 (37.3) | 300 (22.8) | 362 (22.9) | |
| Boys | |||||
| Family affluence scale | Low | 239 (13.6) | 134 (7.9) | 206 (17.2) | 243 (15.2) |
| Medium | 1024 (58.2) | 853 (50.1) | 716 (59.9) | 944 (58.9) | |
| High | 496 (28.2) | 715 (42.0) | 274 (22.9) | 415 (25.9) |
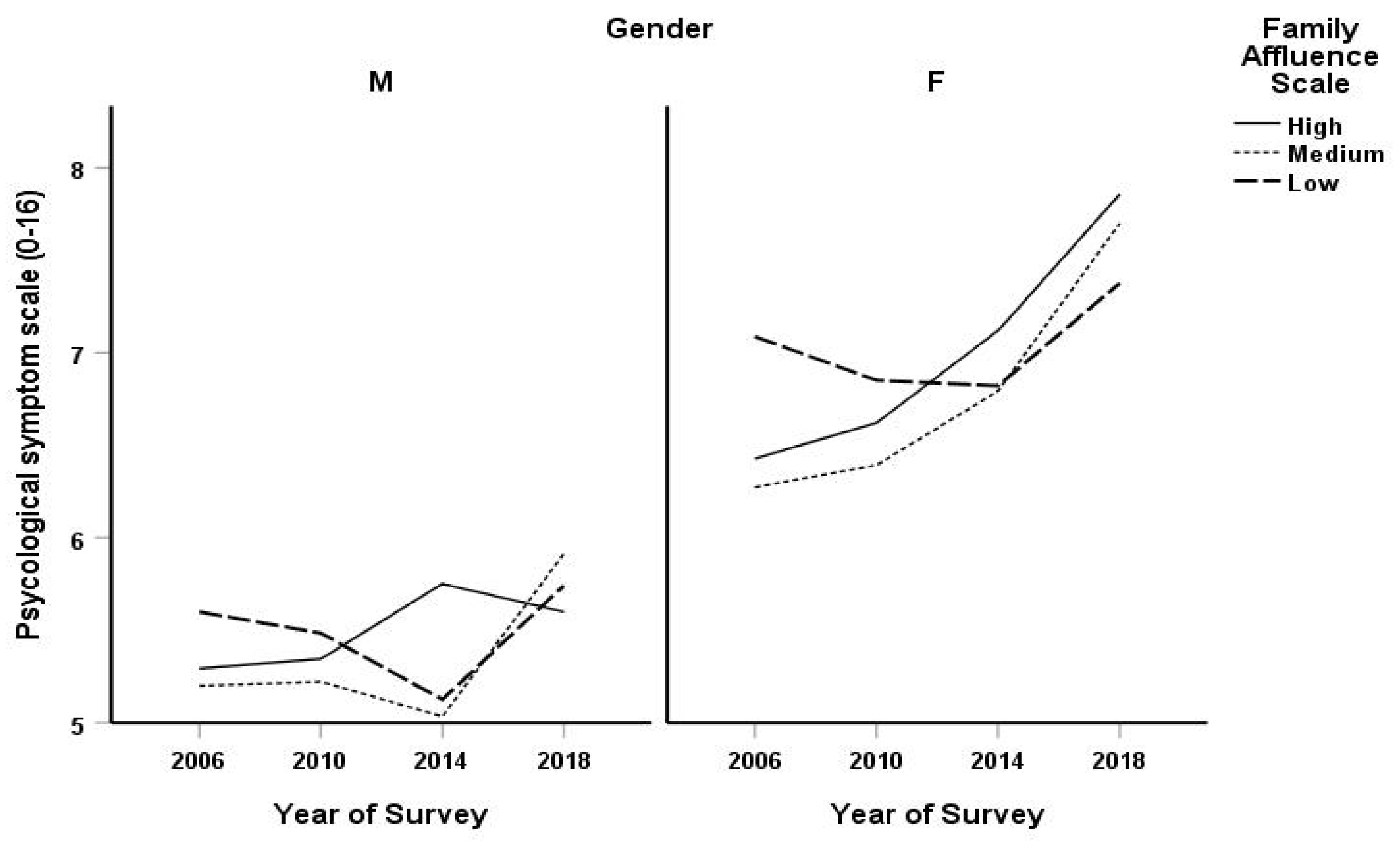
| Family Affluence Scale | 2006 Predicted Score (95% CI) | 2010 Predicted Score (95% CI) | 2014 Predicted Score (95% CI) | 2018 Predicted Score (95% CI) | Difference 2018–2006 | |
|---|---|---|---|---|---|---|
| Girls | ||||||
| Low | 7.09 (7.00, 7.17) | 6.85 (6.73, 6.97) | 6.82 (6.73, 6.91) | 7.37 (7.29, 7.47) | 0.29 (0.17, 0.41) | |
| Medium | 6.27 (6.23, 6.31) | 6.39 (6.35, 6.44) | 6.79 (6.75, 6.84) | 7.70 (7.66, 7.74) | 1.43 (1.37, 1.48) | |
| High | 6.43 (6.37, 6.49) | 6.62 (6.57, 6.67) | 7.12 (7.05, 7.19) | 7.86 (7.79, 7.92) | 1.43 (1.34, 1.52) | |
| Boys | ||||||
| Low | 5.60 (5.51, 5.69) | 5.49 (5.38, 5.59) | 5.13 (5.03, 5.22) | 5.74 (5.65, 5.84) | 0.14 (0.01, 0.27) | |
| Medium | 5.20 (5.16, 5.24) | 5.22 (5.18, 5.27) | 5.03 (4.99, 5.08) | 5.91 (5.87, 5.96) | 0.71 (0.65, 0.77) | |
| High | 5.29 (5.24, 5.35) | 5.35 (5.30, 5.39) | 5.75 (5.68, 5.83) | 5.60 (5.53, 5.67) | 0.31 (0.22, 0.39) |
| Regression Coefficient | 95% CI | p-Value | ||
|---|---|---|---|---|
| Gender | ||||
| Girl | Reference | |||
| Boy | −1.40 | −2.07, −0.73 | <0.001 | |
| Family affluence scale | ||||
| Low | Reference | |||
| Medium | −0.67 | −1.18, −0.17 | 0.009 | |
| High | −0.47 | −1.05, 0.12 | 0.12 | |
| Year of survey | ||||
| 2006 | Reference | |||
| 2010 | 0.91 | −0.72, 0.91 | 0.83 | |
| 2014 | −0.18 | −0.86, 0.50 | 0.60 | |
| 2018 | 0.34 | −0.34, 1.03 | 0.32 | |
| Age (in years) | 0.39 | 0.35, 0.43 | <0.001 | |
| Gender/Family affluence scale | ||||
| Boy/Medium | 0.31 | −0.45, 1.06 | 0.42 | |
| Boy/High | 0.17 | −0.68, 1.02 | 0.69 | |
| Gender/Year | ||||
| Boy/2010 | 0.14 | −1.02, 1.31 | 0.81 | |
| Boy/2014 | −0.26 | −1.26, 0.74 | 0.62 | |
| Boy/2018 | −0.27 | −1.26, 0.72 | 0.59 | |
| Family affluence scale/Year | ||||
| Medium/2010 | 0.15 | −0.74, 1.03 | 0.75 | |
| High/2010 | 0.13 | −0.83, 1.08 | 0.79 | |
| Medium/2014 | 0.67 | −0.10, 1.44 | 0.09 | |
| High/2014 | 0.70 | −0.20, 1.60 | 0.13 | |
| Medium/2018 | 0.98 | 0.22, 1.74 | 0.01 | |
| High/2018 | 0.90 | 0.01, 1.78 | 0.05 | |
| Gender/Family affluence scale/Year | ||||
| Boy/Medium/2010 | −0.23 | −1.50, 1.04 | 0.73 | |
| Boy/High/2010 | −0.17 | −1.52, 1.17 | 0.80 | |
| Boy/Medium/2014 | −0.46 | −1.58, 0.67 | 0.43 | |
| Boy/High/2014 | 0.16 | −1.14, 1.46 | 0.81 | |
| Boy/Medium/2018 | 0.56 | −1.56, 0.65 | 0.42 | |
| Boy/High/2018 | −0.75 | −2.00, 0.50 | 0.24 |
| Family Affluence Scale | 2006 Predicted Score (95% CI) | 2010 Predicted Score (95% CI) | 2014 Predicted Score (95% CI) | 2018 Predicted Score (95% CI) | Difference 2018–2006 | |
|---|---|---|---|---|---|---|
| GIRLS | ||||||
| Depressed | Low | 0.66 (0.65, 0.66) | 0.64 (0.63, 0.65) | 0.61 (0.60, 0.62) | 0.58 (0.57, 0.59) | −0.08 (−0.09, −0.06) |
| Medium | 0.60 (0.59, 0.60) | 0.59 (0.58, 0.59) | 0.61 (0.61, 0.62) | 0.62 (0.62, 0.63) | 0.03 (0.02, 0.03) | |
| High | 0.61 (0.60, 0.61) | 0.57 (0.56, 0.57) | 0.58 (0.57, 0.59) | 0.61 (0.60, 0.62) | 0.00 (−0.01, 0.01) | |
| GIRLS | ||||||
| Irritable | Low | 0.60 (0.59, 0.61) | 0.52 (0.51, 0.54) | 0.53 (0.52, 0.54) | 0.59 (0.58, 0.60) | −0.01 (−0.02, 0.01) |
| Medium | 0.53 (0.52, 0.53) | 0.52 (0.51, 0.53) | 0.55 (0.54, 0.56) | 0.64 (0.63, 0.64) | 0.11 (0.10, 0.12) | |
| High | 0.54 (0.53, 0.55) | 0.56 (0.56, 0.57) | 0.56 (0.55, 0.57) | 0.65 (0.64, 0.66) | 0.11 (0.10, 0.12) | |
| GIRLS | ||||||
| Nervous | Low | 0.64 (0.63, 0.65) | 0.59 (0.58, 0.61) | 0.61 (0.60, 0.62) | 0.65 (0.64, 0.66) | 0.02 (0.00, 0.03) |
| Medium | 0.61 (0.61, 0.62) | 0.59 (0.58, 0.59) | 0.62 (0.62, 0.63) | 0.68 (0.67, 0.68) | 0.06 (0.06, 0.07) | |
| High | 0.58 (0.57, 0.59) | 0.63 (0.63, 0.64) | 0.62 (0.62, 0.63) | 0.69 (0.68, 0.69) | 0.10 (0.09, 0.11) | |
| GIRLS | ||||||
| Sleep difficulties | Low | 0.29 (0.29, 0.29) | 0.31 (0.31, 0.31) | 0.31 (0.31, 0.31) | 0.42 (0.42, 0.42) | 0.13 (0.13, 0.13) |
| Medium | 0.23 (0.23, 0.23) | 0.28 (0.28, 0.28) | 0.29 (0.29, 0.29) | 0.40 (0.40, 0.40) | 0.17 (0.17, 0.17) | |
| High | 0.25 (0.25, 0.25) | 0.31 (0.31, 0.31) | 0.37 (0.37, 0.37) | 0.40 (0.40, 0.40) | 0.15 (0.15, 0.15) | |
| BOYS | ||||||
| Depressed | Low | 0.46 (0.45, 0.47) | 0.48 (0.47, 0.49) | 0.41 (0.40, 0.42) | 0.44 (0.43, 0.45) | −0.02 (−0.03, −0.01) |
| Medium | 0.41 (0.40, 0.41) | 0.43 (0.42, 0.43) | 0.41 (0.40, 0.41) | 0.46 (0.45, 0.46) | 0.05 (0.05, 0.06) | |
| High | 0.43 (0.42, 0.44) | 0.42 (0.42, 0.43) | 0.46 (0.45, 0.47) | 0.39 (0.38, 0.40) | −0.04 (−0.05, −0.03) | |
| BOYS | ||||||
| Irritable | Low | 0.43 (0.42, 0.44) | 0.39 (0.37, 0.40) | 0.43 (0.42, 0.44) | 0.43 (0.42, 0.45) | 0.01 (−0.01, 0.02) |
| Medium | 0.46 (0.46, 0.47) | 0.43 (0.43, 0.44) | 0.41 (0.40, 0.41) | 0.49 (0.49, 0.50) | 0.03 (0.02, 0.04) | |
| High | 0.44 (0.43, 0.45) | 0.45 (0.44, 0.46) | 0.46 (0.45, 0.47) | 0.49 (0.48, 0.50) | 0.05 (0.04, 0.06) | |
| BOYS | ||||||
| Nervous | Low | 0.54 (0.53, 0.55) | 0.54 (0.53, 0.56) | 0.44 (0.43, 0.45) | 0.52 (0.51, 0.53) | 0.01 (−0.03, −0.00) |
| Medium | 0.50 (0.50, 0.51) | 0.50 (0.50, 0.51) | 0.46 (0.45, 0.46) | 0.56 (0.56, 0.57) | 0.06 (0.05, 0.07) | |
| High | 0.49 (0.48, 0.50) | 0.55 (0.54, 0.56) | 0.52 (0.52, 0.53) | 0.56 (0.55, 0.57) | 0.07 (0.06, 0.08) | |
| BOYS | ||||||
| Sleep difficulties | Low | 0.23 (0.23, 0.23) | 0.25 (0.25, 0.25) | 0.24 (0.24, 0.24) | 0.30 (0.30, 0.30) | 0.07 (0.07, 0.07) |
| Medium | 0.20 (0.20, 0.20) | 0.23 (0.23, 0.23) | 0.25 (0.25, 0.25) | 0.32 (0.32, 0.32) | 0.13 (0.13, 0.13) | |
| High | 0.19 (0.19, 0.19) | 0.24 (0.24, 0.24) | 0.32 (0.32, 0.32) | 0.28 (0.28, 0.28) | 0.09 (0.09, 0.09) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipari, D.; Bocci, B.M.; Rivieri, C.; Frongillo, E.; Miserendino, A.; Pammolli, A.; Trombetta, C.M.; Manini, I.; Simi, R.; Lazzeri, G. Trend of Correlations between Psychological Symptoms and Socioeconomic Inequalities among Italian Adolescents: Cross-Sectional Study from 2006 to 2018 in Tuscany Region. Int. J. Environ. Res. Public Health 2023, 20, 6473. https://doi.org/10.3390/ijerph20156473
Lipari D, Bocci BM, Rivieri C, Frongillo E, Miserendino A, Pammolli A, Trombetta CM, Manini I, Simi R, Lazzeri G. Trend of Correlations between Psychological Symptoms and Socioeconomic Inequalities among Italian Adolescents: Cross-Sectional Study from 2006 to 2018 in Tuscany Region. International Journal of Environmental Research and Public Health. 2023; 20(15):6473. https://doi.org/10.3390/ijerph20156473
Chicago/Turabian StyleLipari, Dario, Bianca Maria Bocci, Cesare Rivieri, Elena Frongillo, Antonella Miserendino, Andrea Pammolli, Claudia Maria Trombetta, Ilaria Manini, Rita Simi, and Giacomo Lazzeri. 2023. "Trend of Correlations between Psychological Symptoms and Socioeconomic Inequalities among Italian Adolescents: Cross-Sectional Study from 2006 to 2018 in Tuscany Region" International Journal of Environmental Research and Public Health 20, no. 15: 6473. https://doi.org/10.3390/ijerph20156473