


Implementation of a Community-Based Mind–Body (Tae-Bo) Physical Activity Programme on Health-Related Physical Fitness in Rural Black Overweight and Obese Women with Manifest Risk Factors for Multimorbidity

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
3. Results
3.1. Adherence, Compliance, and Adverse Events
3.2. Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de-Graft Aikins, A.; Unwin, N.; Agyemang, C.; Allotey, P.; Campbell, C.; Arhinful, D. Tackling Africa’s chronic disease burden: From the local to the global. Glob. Health 2010, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayosi, B.M.; Flisher, A.J.; Lalloo, U.G.; Sitas, F.; Tollman, S.M.; Bradshaw, D. The burden of non-communicable diseases in South Africa. Lancet 2009, 374, 934–947. [Google Scholar] [CrossRef] [PubMed]
- Peer, N. The converging burdens of infectious and non-communicable diseases in rural-to-urban migrant Sub-Saharan African populations: A focus on HIV/AIDS, tuberculosis and cardio-metabolic diseases. Trop. Dis. Travel Med. Vaccines 2015, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Global Status Report on Noncommunicable Diseases. 2014. Available online: http://www.who.int/nmh/publications/ncd-status-report2014/en/ (accessed on 13 November 2019).
- Pearson, T.A.; Brown, W.V.; Donato, K.; Franklin, F.A., Jr.; Luepker, R.B.; McBride, P.E.; Mullis, R.M.; Scott, L.W.; Shannon, B.M.; Shekelle, R. Lipids. Workshop IV. AHA Prevention Conference III. Behaviour changes and compliance: Keys to improving cardiovascular health. Circulation 1993, 88, 1397–1401. [Google Scholar] [CrossRef] [Green Version]
- Heine, M.; Lupton-Smith, A.; Pakosh, M.; Grace, S.L.; Derman, W.; Hanekom, S.D. Exercise-based rehabilitation for major non-communicable diseases in low-resource settings: A scoping review. BMJ Glob. Health 2019, 74, e001833. [Google Scholar] [CrossRef]
- Juma, P.A.; Mohamed, S.F.; Matanje Mwagomba, B.L.; Ndinda, C.; Mapa-Tassou, C.; Oluwasanu, M.; Oladepo, O.; Abiona, O.; Nkhata, M.J.; Wisdom, J.P.; et al. Non-communicable disease prevention policy process in five African countries. BMC Public. Health 2018, 18 (Suppl. S1), 961. [Google Scholar]
- Pojednic, R.; D’Arpino, E.; Halliday, I.; Bantham, A. The benefits of physical activity for people with obesity, independent of weight loss: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 4981. [Google Scholar] [CrossRef]
- Miller, W.C.; Koceja, D.M.; Hamilton, E.J. A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Puhan, M.A.; Gimeno-Santos, E.; Cates, C.J.; Troosters, T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2016, 12, CD005305. [Google Scholar] [CrossRef]
- Goon, D.T.; Toriola, A.L.; Shaw, B.S. Screening for body-weight disorders in Nigerian children using contrasting definitions. Obes. Rev. 2010, 11, 508–515. [Google Scholar] [CrossRef]
- Shaw, B.S.; Shaw, I. Resistance training as a countermeasure for key non-communicable diseases in low-resource settings: A review. Asian J. Sports Med. 2021, 12, e106588. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Rehabilitation. A Call for Action. WHO. 2030. Available online: https://www.who.int/initiatives/rehabilitation-2030 (accessed on 6 February 2019).
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Buys, N.; Jayasinghe, R. Effects of community-based meditative Tai Chi programme on improving quality of life, physical and mental health in chronic heart-failure participants. Aging Ment. Health 2014, 18, 289–295. [Google Scholar] [CrossRef]
- Lazăr, A.G.; Leuciuc, F.V. Study concerning the physical fitness of Romanian students and its effects on their health-related quality of life. Sustainability 2021, 13, 6821. [Google Scholar] [CrossRef]
- Mathunjwa, M.L.; Semple, S.J.; du Preez, C. A 10-week aerobic exercise program reduces cardiometabolic disease risk in overweight/obese female African university students. Ethn. Dis. 2013, 23, 143–148. [Google Scholar] [PubMed]
- Milenković Dand Veselinović, N. Effect of experimental Tae Bo training model for coordination development of young women. Sport. Sci. 2010, 3, 57–60. [Google Scholar]
- American College of Sports Medicine (ACSM) and Centres for Disease Control and Prevention (CDC). Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Christ, T. Experimental control and threats to internal validity of concurrent and nonconcurrent multiple baseline designs. Psychol. Sch. 2007, 44, 451–459. [Google Scholar] [CrossRef]
- Lavie, C.J.; Arena, R.; Swift, D.L.; Johannsen, N.M.; Sui, X.; Lee, D.C.; Earnest, C.P.; Church, T.S.; O’Keefe, J.H.; Milani, R.V.; et al. Exercise and the cardiovascular system: Clinical science and cardiovascular outcomes. Circ. Res. 2015, 117, 207–219. [Google Scholar] [CrossRef]
- Schweda, S.; Müller, G.; Munz, B.; Sudeck, G.; Martus, P.; Dierkes, K.; Krauss, I. Implementation and evaluation of an individualized physical exercise promotion program in people with manifested risk factors for multimorbidity (MultiPill-Exercise): A study protocol for a pragmatic randomized controlled trial. BMC Public Health 2022, 22, 1174. [Google Scholar] [CrossRef]
- Shaw, I.; Shaw, B.S.; Brown, G.A. Concurrent training and pulmonary function in smokers. Int. J. Sports Med. 2011, 32, 776–780. [Google Scholar] [CrossRef]
- Shandu, N.M.; Mathunjwa, M.L.; Shaw, B.S.; Shaw, I. Effects of high-intensity interval training and continuous aerobic training on health-fitness, health related quality of life, and psychological measures in college-aged smokers. Int. J. Environ. Res. Public Health 2022, 20, 653. [Google Scholar] [CrossRef] [PubMed]
- Norton, K.; Olds, T. Anthropometrica: A Textbook of Body Measurement for Sports and Health Courses; Southwood Press: Marrickville, NSW, Australia, 1996. [Google Scholar]
- Fourie, M.; Gildenhuys, G.M.; Shaw, I.; Shaw, B.S.; Toriola, A.L.; Goon, D.T. Effects of a mat pilates program on flexibility in elderly women. Med. Sport. 2013, 66, 545–553. [Google Scholar]
- Mookerjee, S.; McMahon, M.J. Electromyographic analysis of muscle activation during sit-and-reach flexibility tests. J. Strength. Cond. Res. 2014, 28, 3496–3501. [Google Scholar] [CrossRef] [PubMed]
- Zumana, N.; Olivier, B.; Godlwana, L.; Martin, C. Intra-rater and inter-rater reliability of six musculoskeletal preparticipatory screening tests. S. Afr. J. Physiother. 2019, 75, 469. [Google Scholar] [CrossRef] [PubMed]
- Patrizio, E.; Calvani, R.; Marzetti, E.; Cesari, M. Physical functional assessment in older adults. J. Frailty Aging 2021, 10, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Morales, O.; Peña-Ibagon, J.C.; Palacios-López, A.; Prieto-Benavides, D.H.; Vivas, A.; Correa-Bautista, J.E.; Lobelo, F.; Alonso-Martínez, A.; Izquierdo, M. Normative reference values for handgrip strength in Colombian schoolchildren: The FUPRECOL Study. J. Strength. Cond. Res. 2017, 31, 217–226. [Google Scholar] [CrossRef]
- Blomqvist, S.; Olsson, J.; Wallin, L.; Wester, A.; Rehn, B. Adolescents with intellectual disability have reduced postural balance and muscle performance in trunk and lower limbs compared to peers without intellectual disability. Res. Dev. Disabil. 2013, 34, 198–206. [Google Scholar] [CrossRef]
- Tancredi, G.; Quattrucci, S.; Scalercio, F.; De Castro, G.; Zicari, A.M.; Bonci, E.; Cingolani, S.; Indinnimeo, L.; Midulla, F. 3-min step test and treadmill exercise for evaluating exercise-induced asthma. Eur. Res. J. 2004, 23, 569–574. [Google Scholar] [CrossRef]
- O’Brien, K.K.; Davis, A.M.; Chan Carusone, S.; Avery, L.; Tang, A.; Solomon, P.; Aubry, R.; Zobeiry, M.; Ilic, I.; Pandovski, Z.; et al. Examining the impact of a community-based exercise intervention on cardiorespiratory fitness, cardiovascular health, strength, flexibility and physical activity among adults living with HIV: A three-phased intervention study. PLoS ONE 2021, 16, e0257639. [Google Scholar] [CrossRef]
- Uritani, D.; Matsumoto, D.; Asano, Y.; Yoshizaki, K.; Nishida, Y.; Shima, M. Effects of regular exercise and nutritional guidance on body composition, blood pressure, muscle strength and health-related quality of life in community-dwelling Japanese women. Obes. Res. Clin. Pr. 2013, 7, e155–e163. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 9 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 January 2022).
- Flegal, K.M. Waist circumference of healthy men and women in the United States. Int. J. Obes. 2007, 31, 1134–1139. [Google Scholar]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A consensus statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Teixeira do Amaral, V.; Fernandes, B.; Ngomane, A.Y.; Marçal, I.R.; Zanini, G.S.; Ciolac, E.G. Short-term community-based exercise programs in low-income older women: Does exercise intensity and modality matters? Exp. Geronto. 2021, 156, 111591. [Google Scholar] [CrossRef]
- Myers, J. Exercise and Cardiovascular Health. Circulation 2003, 107, e2–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtani. B.A.; Sparto, P.J.; Whitney, S.L.; Greenspan, S.L.; Perera, S.; VanSwearingen, J.; Brach, J.S. Effect of community-based group exercise interventions on standing balance and strength in independent living older adults. J. Geriatr. Phys. Ther. 2019, 42, E7–E15. [Google Scholar]
- Schell, J.; Leelarthaepin, B. Physical Fitness Assessment in Exercise and Sports Science, 2nd ed.; Leelar Biomedisience Services: Matraville, NSW, Australia, 1994. [Google Scholar]
- Melzer, I.; Oddsson, L.I. Altered characteristics of balance control in obese older adults. Obesity Res. Clin. Prac. 2016, 10, 151–158. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.P.; Kraemer, W.J.; Snih, S.A.; Peterson, M.D. Handgrip strength and health in aging adults. Sports Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; Buchanan, T.A.; Spicer, D.; Tripathy, D.; et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: A randomized controlled trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar]
- Strasser, B.; Burtscher, M. Survival of the fittest: VO2max, a key predictor of longevity? Front. Biosci. 2018, 23, 1505–1516. [Google Scholar] [CrossRef]
- Morrow, J.R.; Jackson, A.; Disch, J.; Mood, D. Measurement and Evolution in Human Performance, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Lawrence, K.E.; Shaw, I.; Shaw, B.S. Hemodynamic changes in normotensive overweight and obese individuals following home-based calisthenics training. Afr. J. Phys. Health Educ. Recreat. Danc. 2014, 20 (Suppl. S2), 82–90. [Google Scholar]
- Paterson, M.; Green, M.; Maunder, E.M. Running before we walk: How can we maximise the benefits from community service dietitians in KwaZulu-Natal, South Africa? Health Policy 2007, 82, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Irandoust, K.; Morteza, T. The effect of aquatic exercises on inflammatory markers of cardiovascular disease in obese women. Int. Arch. Health Sci. 2018, 5, 145–149. [Google Scholar] [CrossRef]
- Jafari, M.; Bizheh, N.; Atri, A.E.; Aralloo, S.F. Acute and chronic effects of physical activity on emerging risk factors of heart attack in overweight men. Int. J. Sport. Stud. Hlth. 2019, 2, e94437. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 65) | Treatment Group (n = 60) | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (n = 60) | Post-Control (n = 60) | Baseline (n = 60) | Mid-Programme (n = 60) | Post-Programme (n = 60) | Δ% Baseline to Mid | Δ% Baseline to Post | Effect Size | |
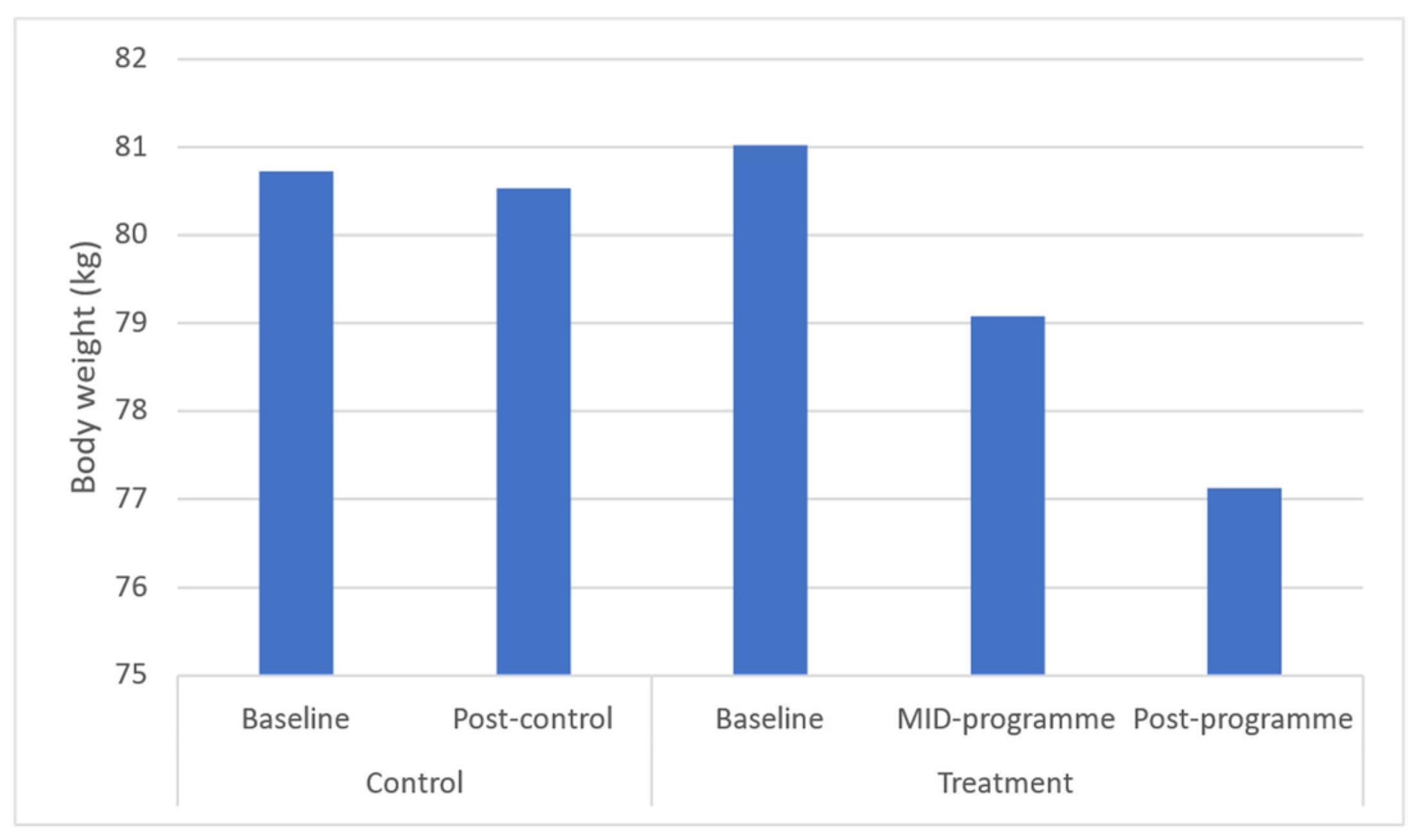
| Body weight (kg) | 80.73 ± 16.61 (77.50–87.28) | 80.53 ± 12.43 (76.51–87.29) | 81.02 ± 15.08 (77.93–86.10) | 79.08 ± 15.07 * (75.53–84.62) | 77.13 ± 15.92 * (72.64–81.63) | ↓2.5 | ↓5.9 | 0.3 |
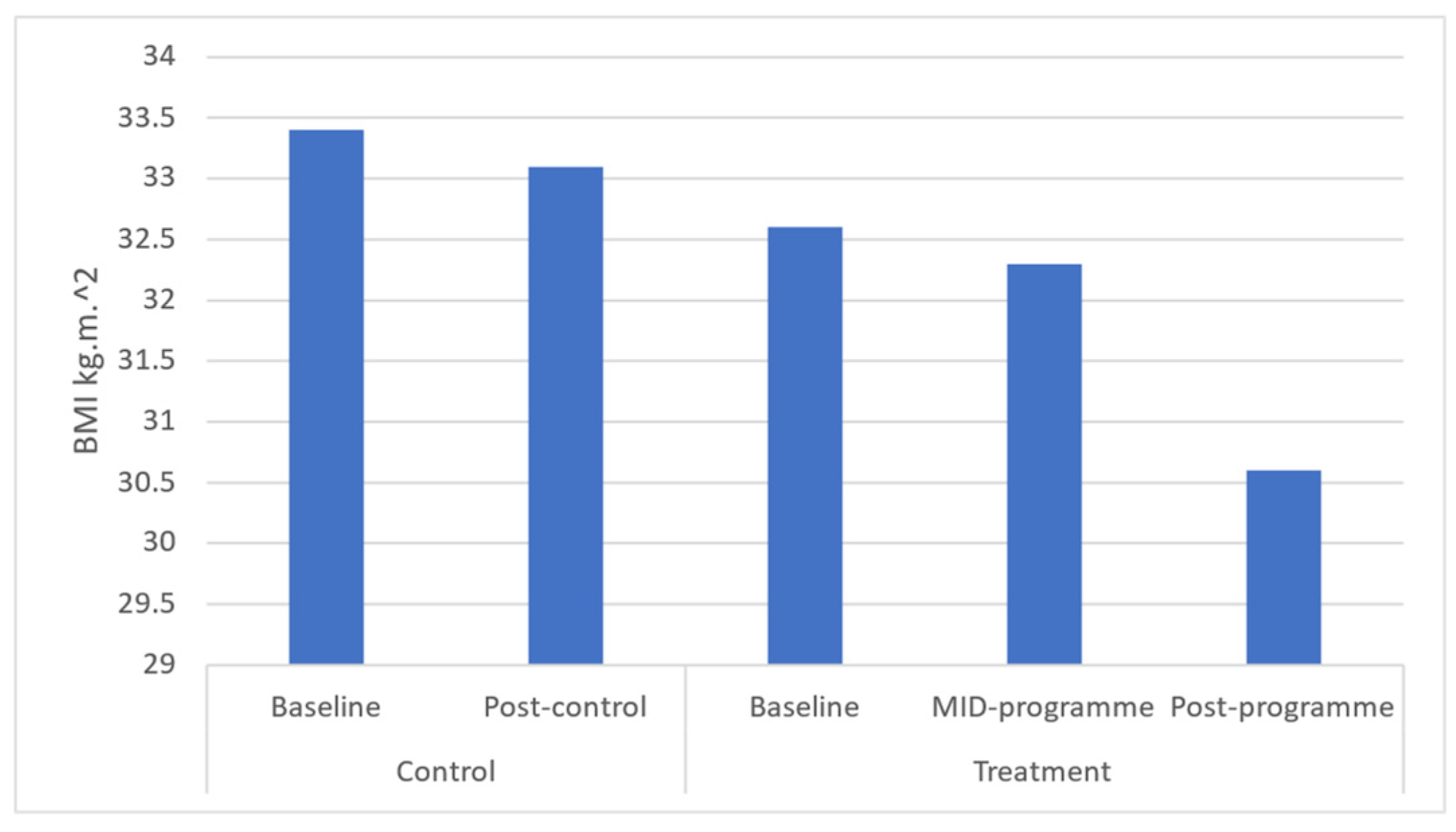
| BMI (kg·m−2) | 33.4 ± 6.02 (30.43–33.71) | 33.1 ± 6.22 (30.54–33.06) | 32.6 ± 5.84 (30.61–33.59) | 32.3 ± 3.14 * (31.49–32.11) | 30.60 ± 5.16 * (28.78–31.42) | ↓0.9 | ↓6.7 | 0.2 |
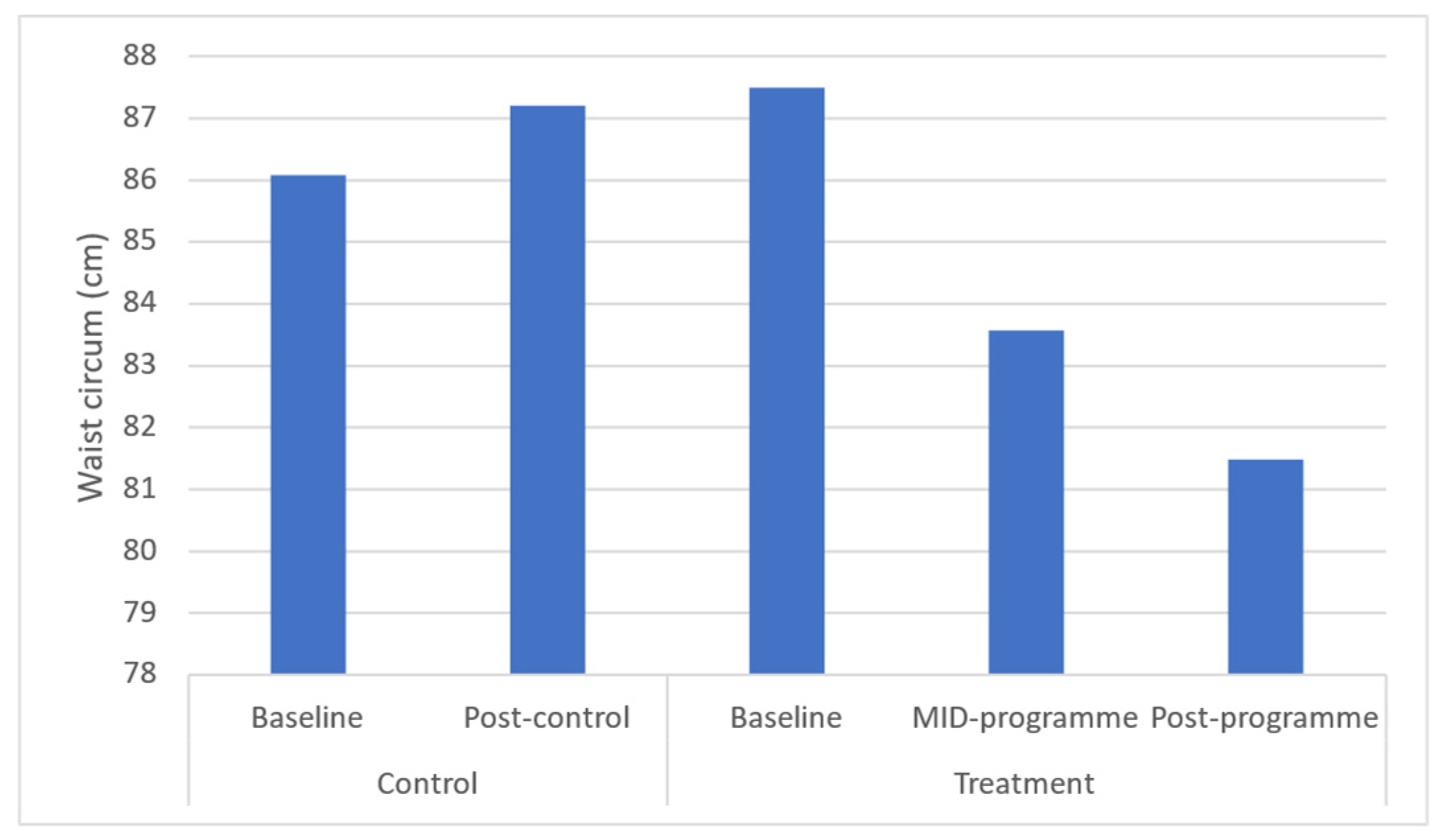
| Waist circum (cm) | 86.08 ± 11.25 (86.01–91.77) | 87.20 ± 10.57 (85.46–91.64) | 87.49 ± 9.65 (85.19–90.60) | 83.57 ± 9.24 * (81.47–86.66) | 81.48 ± 10.71 * (79.52–84.44) | ↓4.5 | ↓6.6 | 0.6 |
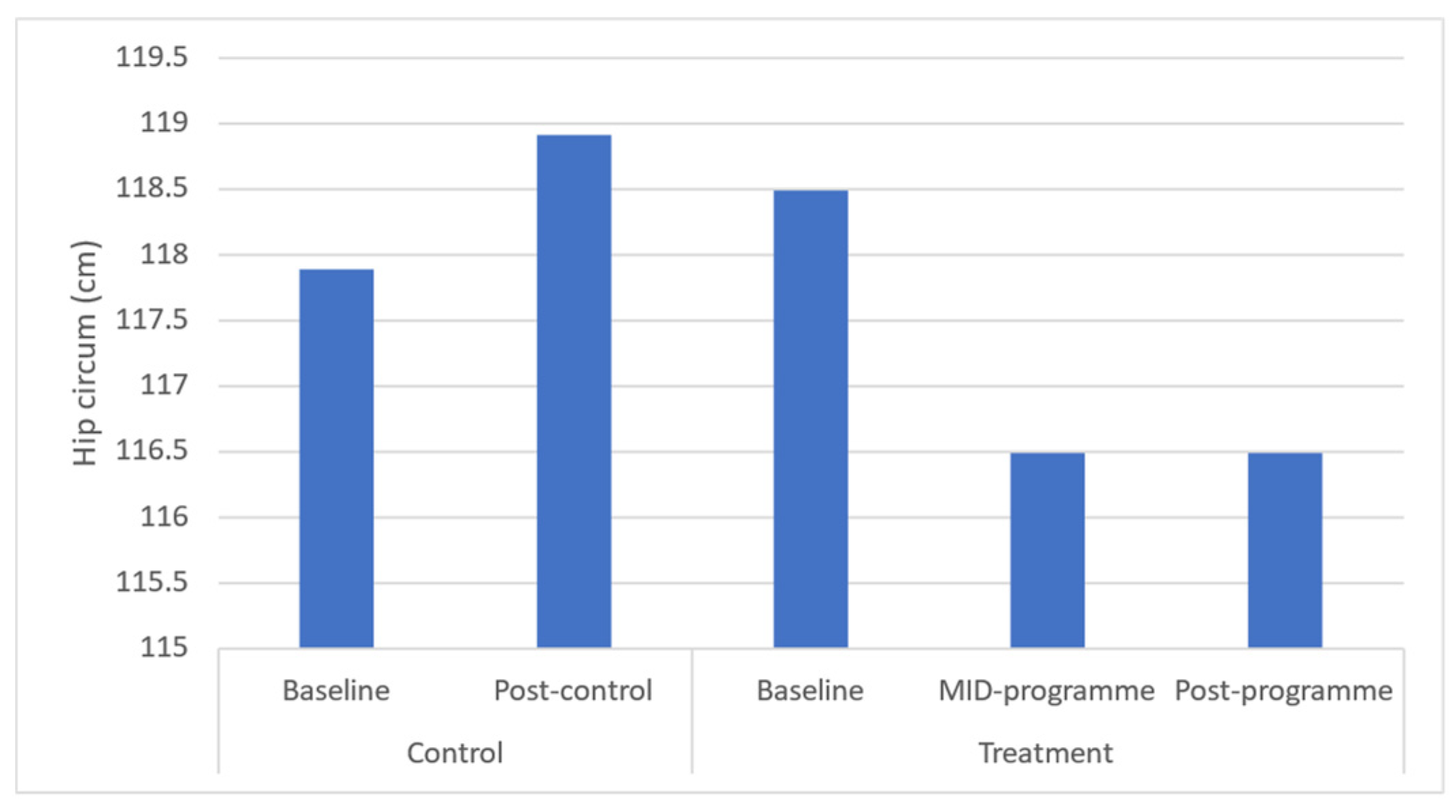
| Hip circum (cm) | 117.89 ± 10.53 (117.25–128.65) | 118.91 ± 8.99 (116.87–127.58) | 118.49 ± 9.65 (115.19–121.60) | 116.49 ± 9.65 (116.19–119.60) | 116.49 ± 10.65 (113.19–119.60) | ↓2.0 | ↓3.5 | 0.4 |
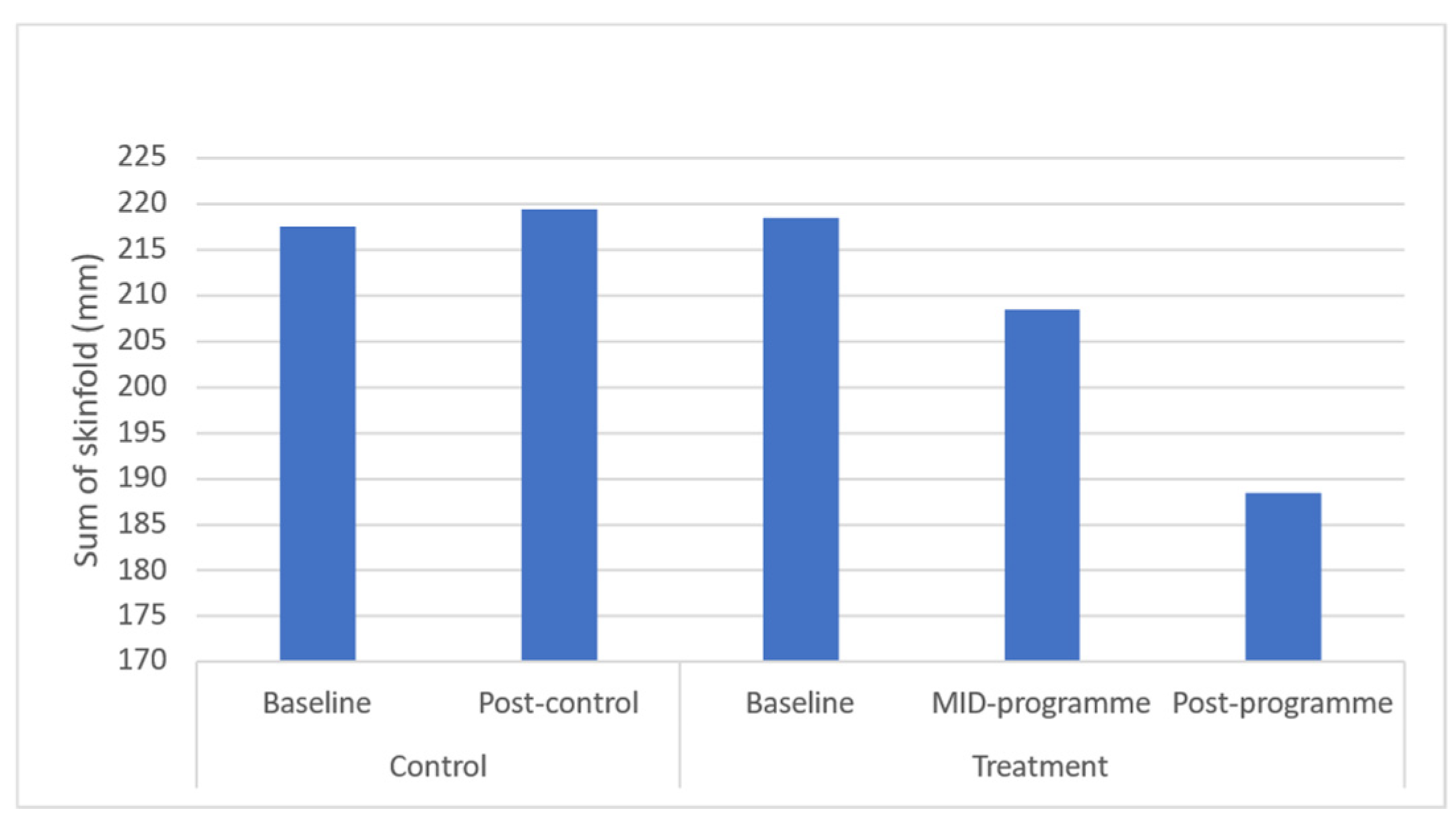
| Sum of skinfolds (mm) | 217.55 ± 28.67 (203.87–226.43) | 219.47 ± 30.05 (202.92–224.11) | 218.49 ± 33.65 (205.19–221.60) | 208.49 ± 34.65 (195.19–211.60) | 188.49 ± 34.65 (175.19–191.60) | ↓5.72 | ↓11.7 | 0.7 |
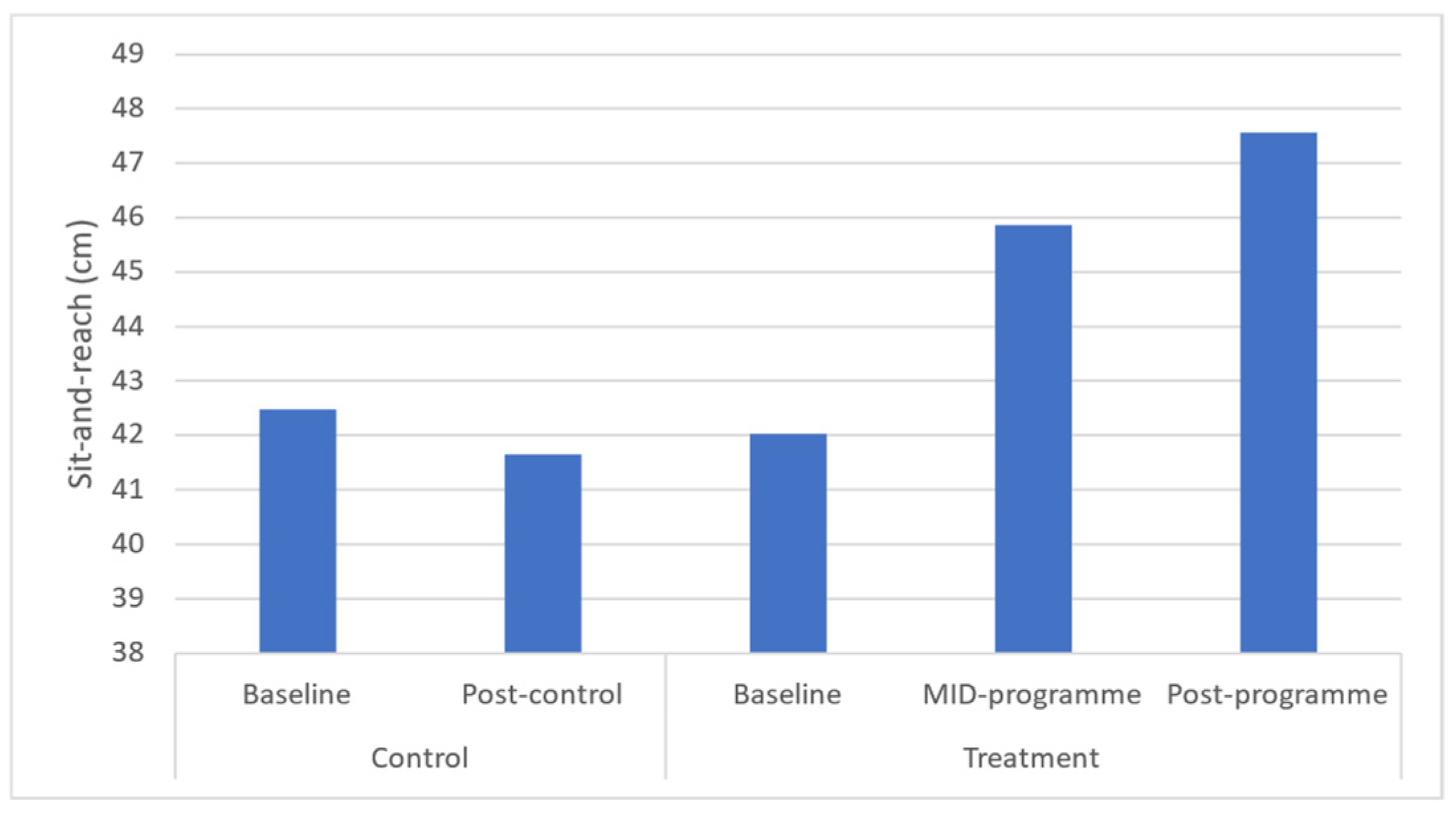
| Sit-and-reach (cm) | 42.48 ± 9.88 (41.43–47.42) | 41.65 ± 10.01 (40.73–46.70) | 42.02 ± 8.08 (39.93–44.10) | 45.87 ± 7.56 * (43.91–47.82) | 47.57 ± 7.5 * (45.63–49.5) | ↑3.85 | ↑5.6 | −0.7 |
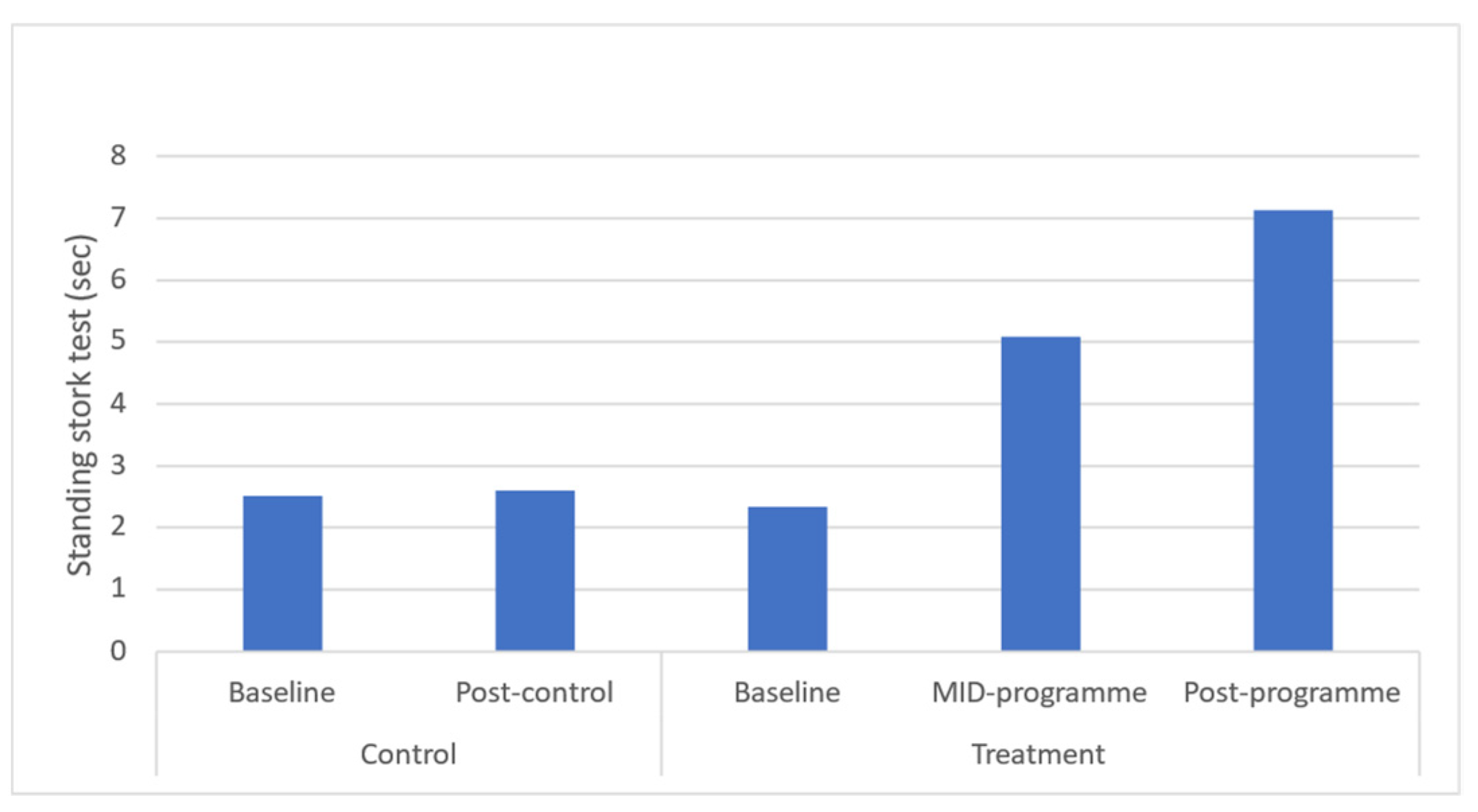
| Standing stork test (s) | 2.51 ±1.64 (1.77–2.43) | 2.60 ±1.43 (1.75–2.68) | 2.34 ±1.58 (1.93–2.76) | 5.08 ±2.07 * (4.53–5.62) | 7.13 ± 1.92 * (6.64–7.63) | ↑2.7 | ↑4.8 | −2.7 |
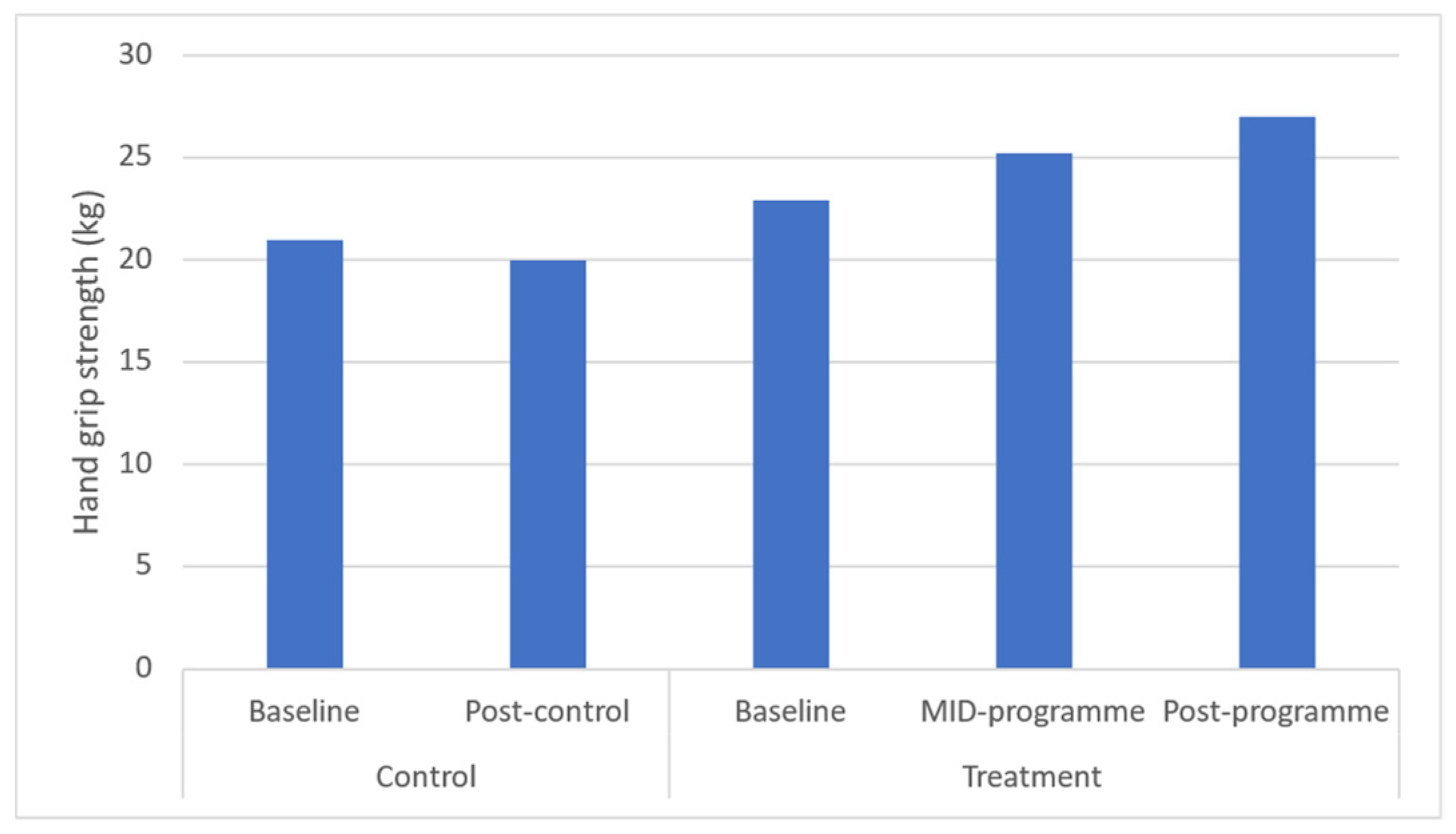
| Hand grip strength (kg) | 20.98 ± 3.87 (22.65–24.54) | 19.98 ± 5.46 (21.41–24.17) | 22.91 ± 4.39 (21.76–24.07) | 25.22 ± 4.55 * (24.03–26.42) | 27.00 ± 3.96 * (25.96–28.04) | ↑2.3 | ↑4.1 | −0.9 |
| Sit ups (reps in 1 min) | 18.14 ± 8.66 (14.02–18.43) | 17.75 ± 7.31 (14.33–18.28) | 16.32 ± 6.32 (14.68–17.95) | 22.12 ± 6.13 * (20.53–23.7) | 26.83 ± 6.13 * (25.48–28.19) | ↑5.8 | ↑10.5 | −1.8 |
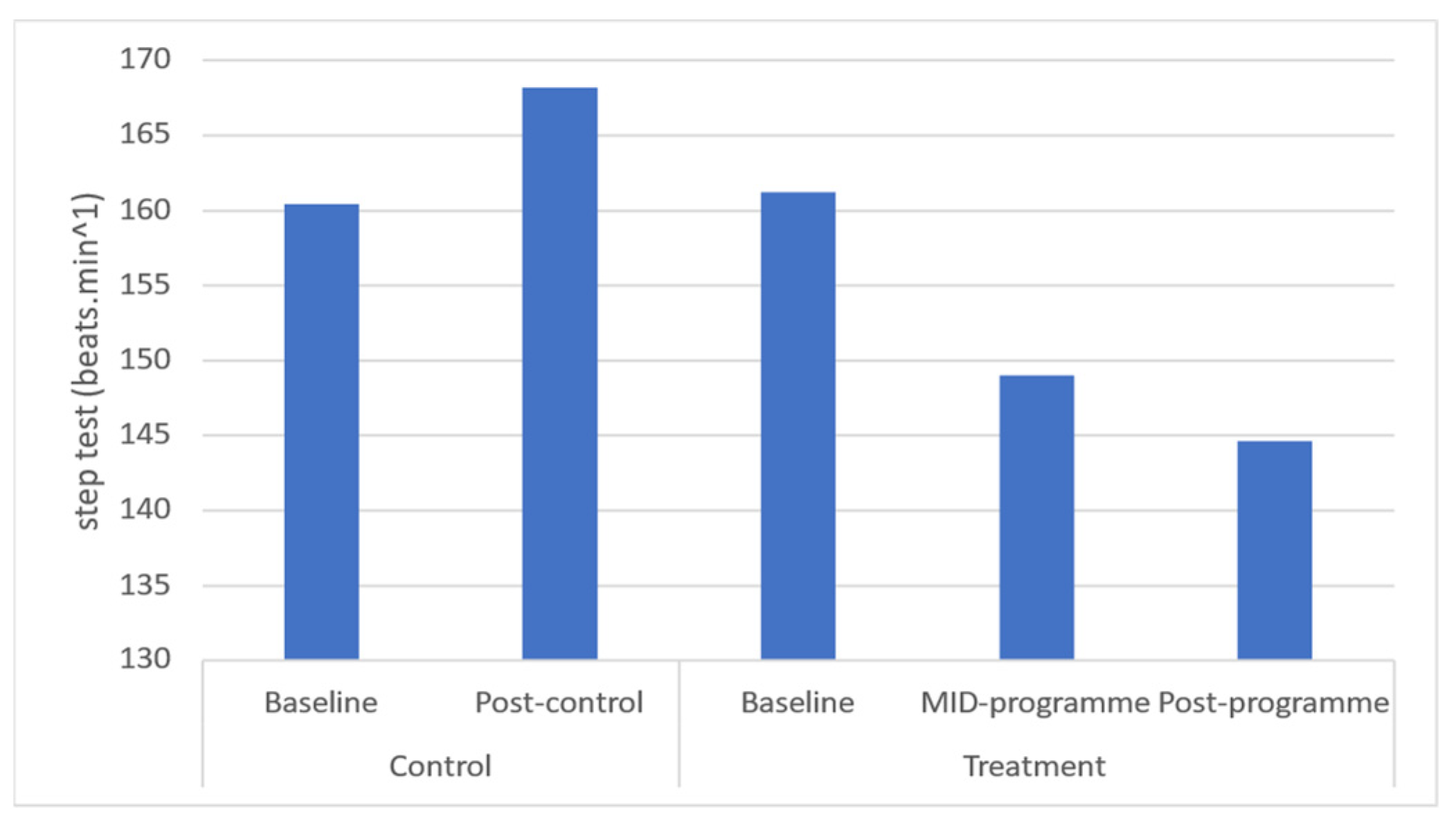
| Step test (beats.min−1) | 160.4 ± 27.12 (152.5–164.4) | 168.2 ± 31.03 (151.7–176.1) | 161.20 ± 20.81 (155.8–166.6) | 149.00 ±19.92 * (143.8–154.2) | 144.60 ±16.92 * (140.1–149.0) | ↓12.2 | ↓16.6 | 0.9 |
| Week | Training Intensity in Rating of Perceived Exertion (RPE) |
|---|---|
| 1 | 11.26 ± 1.28 |
| 2 | 12.46 ± 1.32 |
| 3 | 12.07 ± 1.33 |
| 4 | 12.44 ± 1.22 |
| 5 | 13.49 ± 0.99 |
| 6 | 13.81 ± 0.98 |
| 7 | 13.95 ± 1.47 |
| 8 | 14.75 ± 1.42 |
| 9 | 14.86 ± 1.41 |
| 10 | 15.35 ± 1.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathunjwa, M.; Shaw, I.; Moran, J.; Sandercock, G.R.; Brown, G.A.; Shaw, B.S. Implementation of a Community-Based Mind–Body (Tae-Bo) Physical Activity Programme on Health-Related Physical Fitness in Rural Black Overweight and Obese Women with Manifest Risk Factors for Multimorbidity. Int. J. Environ. Res. Public Health 2023, 20, 6463. https://doi.org/10.3390/ijerph20156463
Mathunjwa M, Shaw I, Moran J, Sandercock GR, Brown GA, Shaw BS. Implementation of a Community-Based Mind–Body (Tae-Bo) Physical Activity Programme on Health-Related Physical Fitness in Rural Black Overweight and Obese Women with Manifest Risk Factors for Multimorbidity. International Journal of Environmental Research and Public Health. 2023; 20(15):6463. https://doi.org/10.3390/ijerph20156463
Chicago/Turabian StyleMathunjwa, Musa, Ina Shaw, Jason Moran, Gavin R. Sandercock, Gregory A. Brown, and Brandon S. Shaw. 2023. "Implementation of a Community-Based Mind–Body (Tae-Bo) Physical Activity Programme on Health-Related Physical Fitness in Rural Black Overweight and Obese Women with Manifest Risk Factors for Multimorbidity" International Journal of Environmental Research and Public Health 20, no. 15: 6463. https://doi.org/10.3390/ijerph20156463