
Irish Dancing Injuries and Associated Risk Factors: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
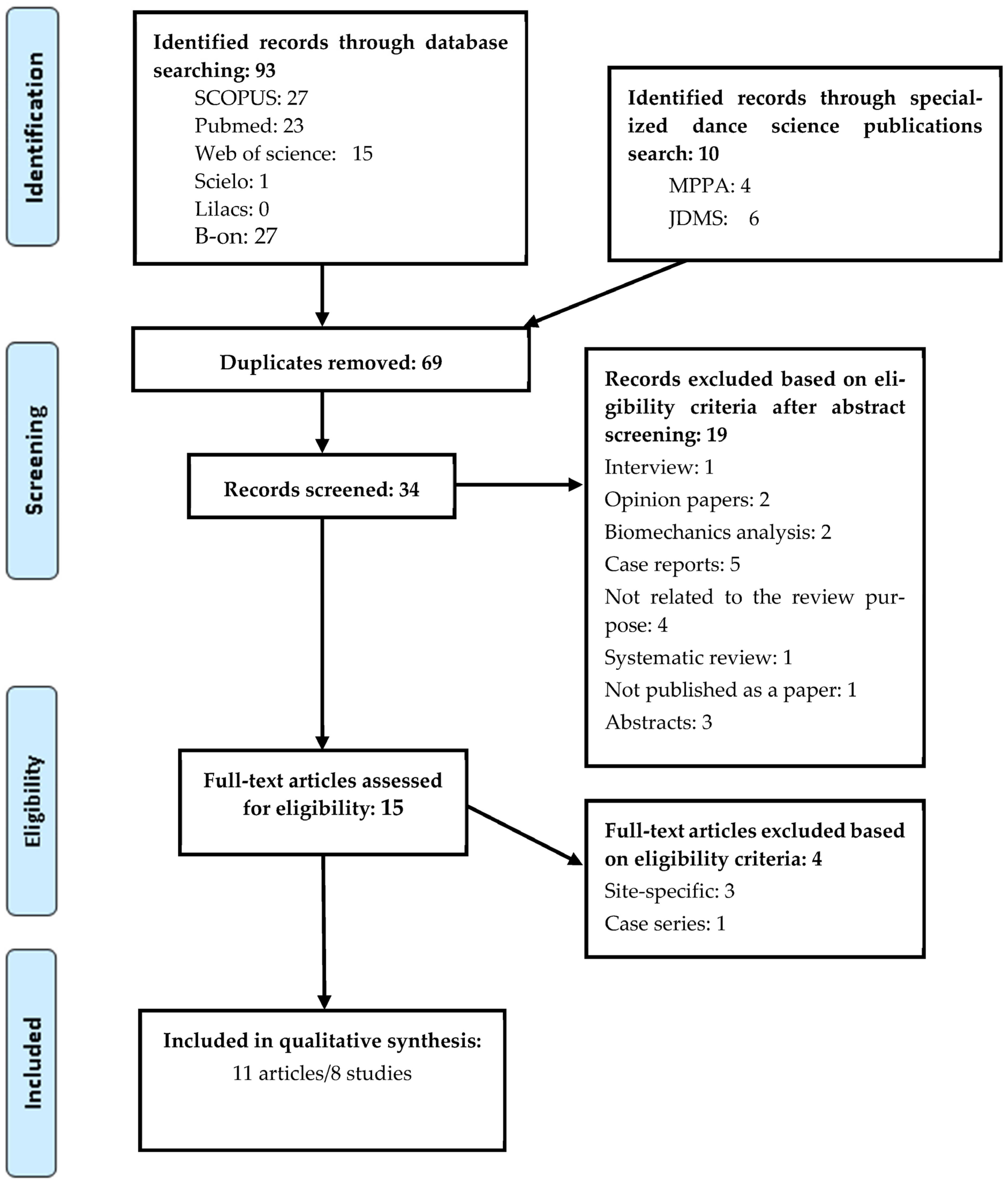
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Study Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Risk of Bias and Level of Evidence
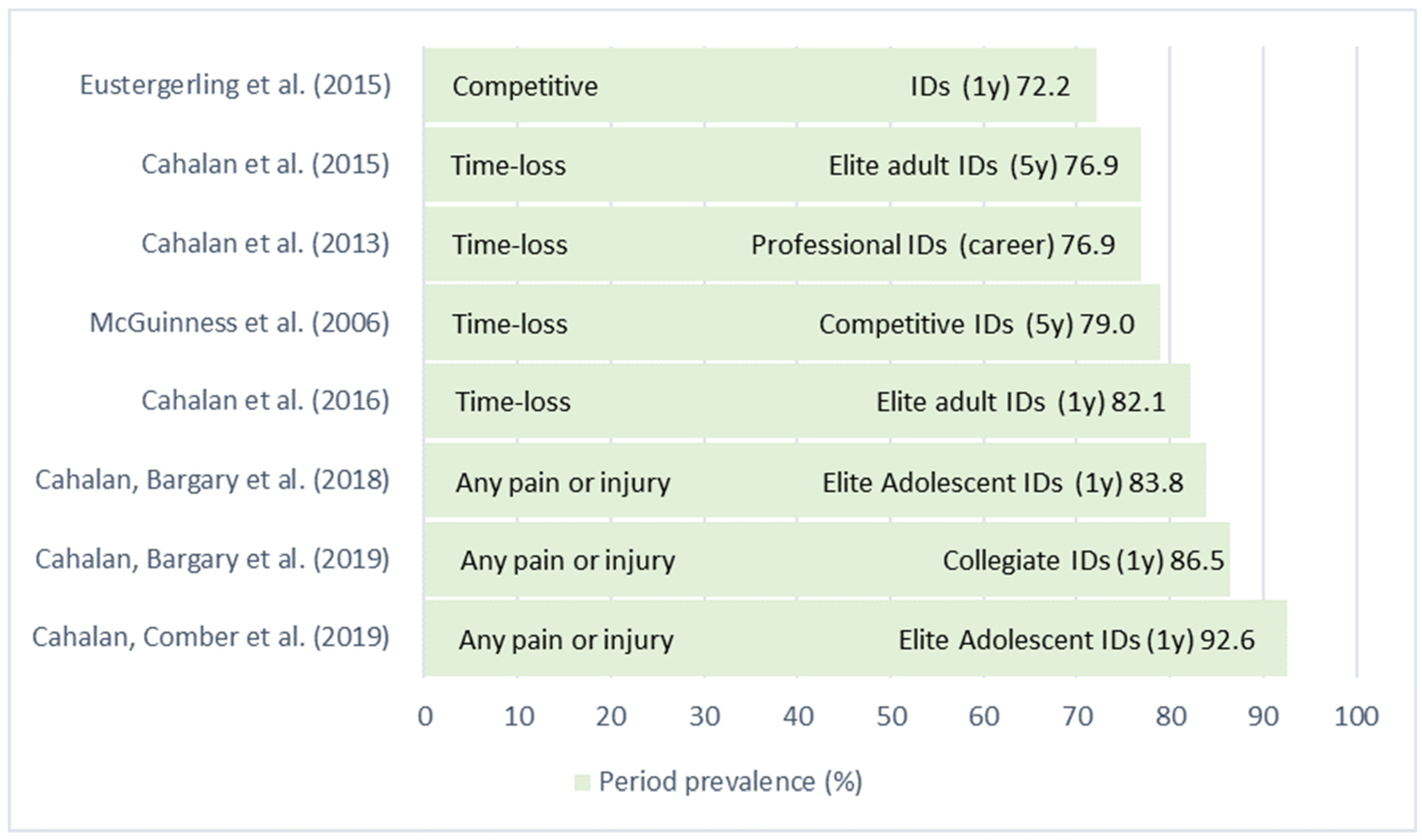
3.3. Injury Estimates
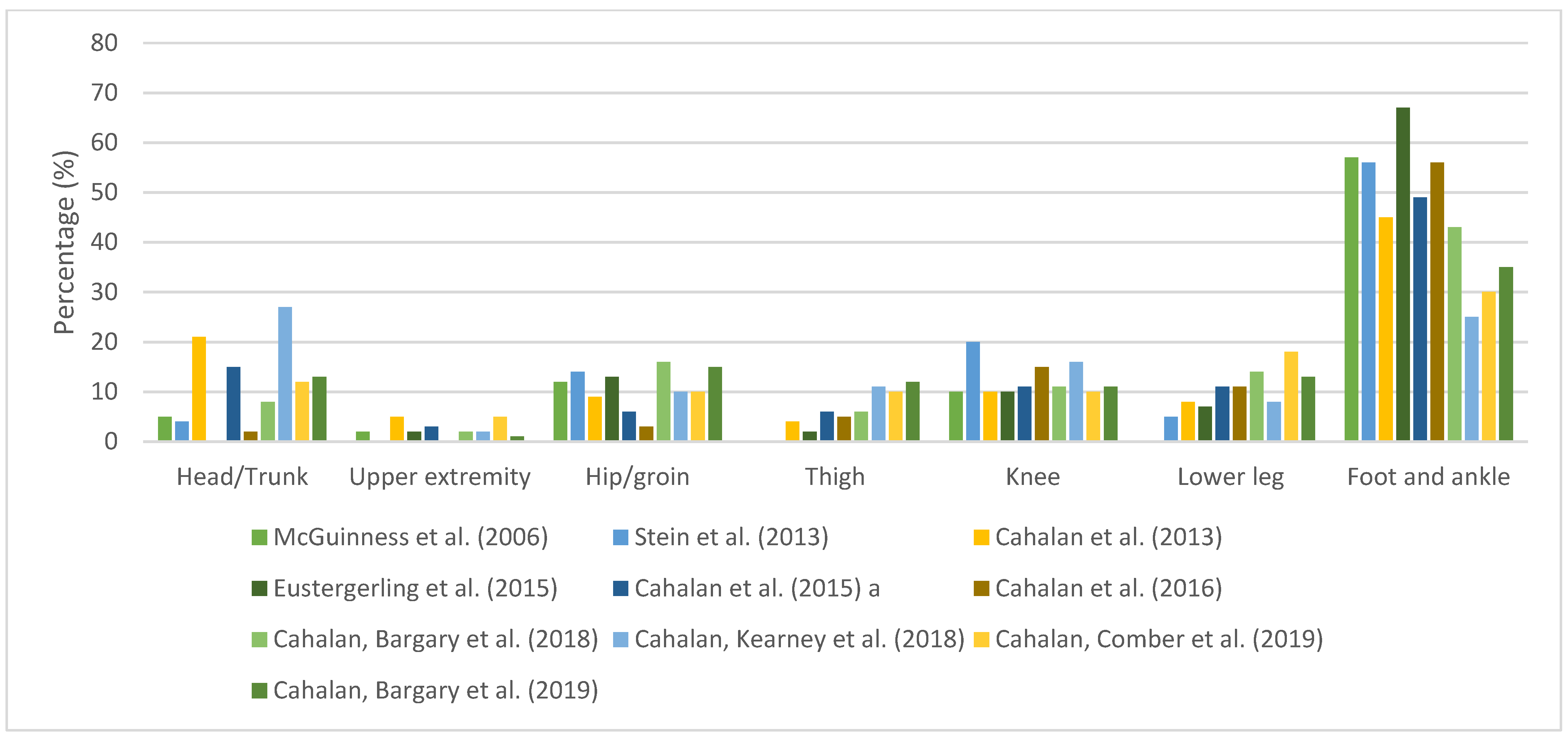
3.4. Anatomical Location
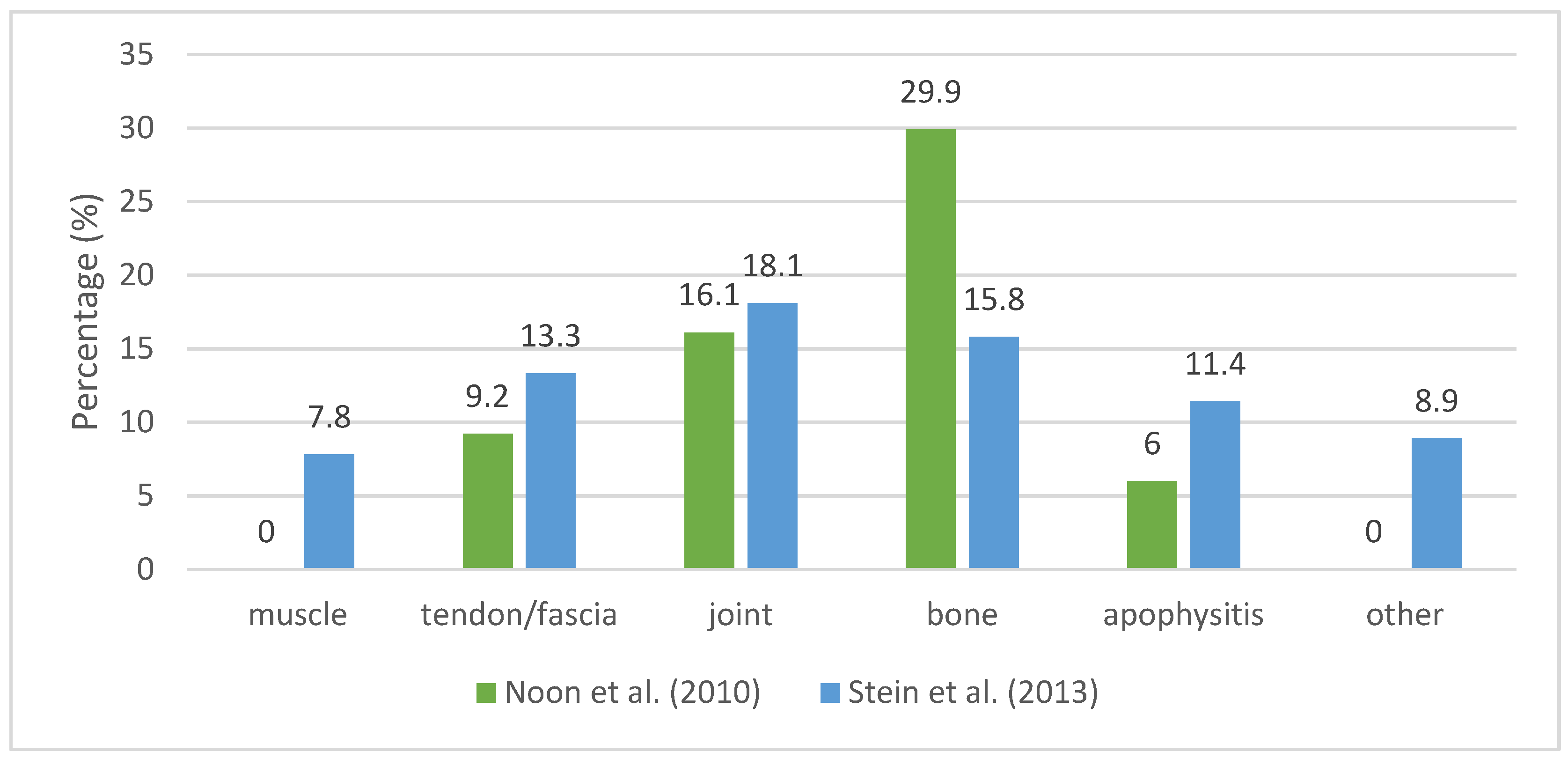
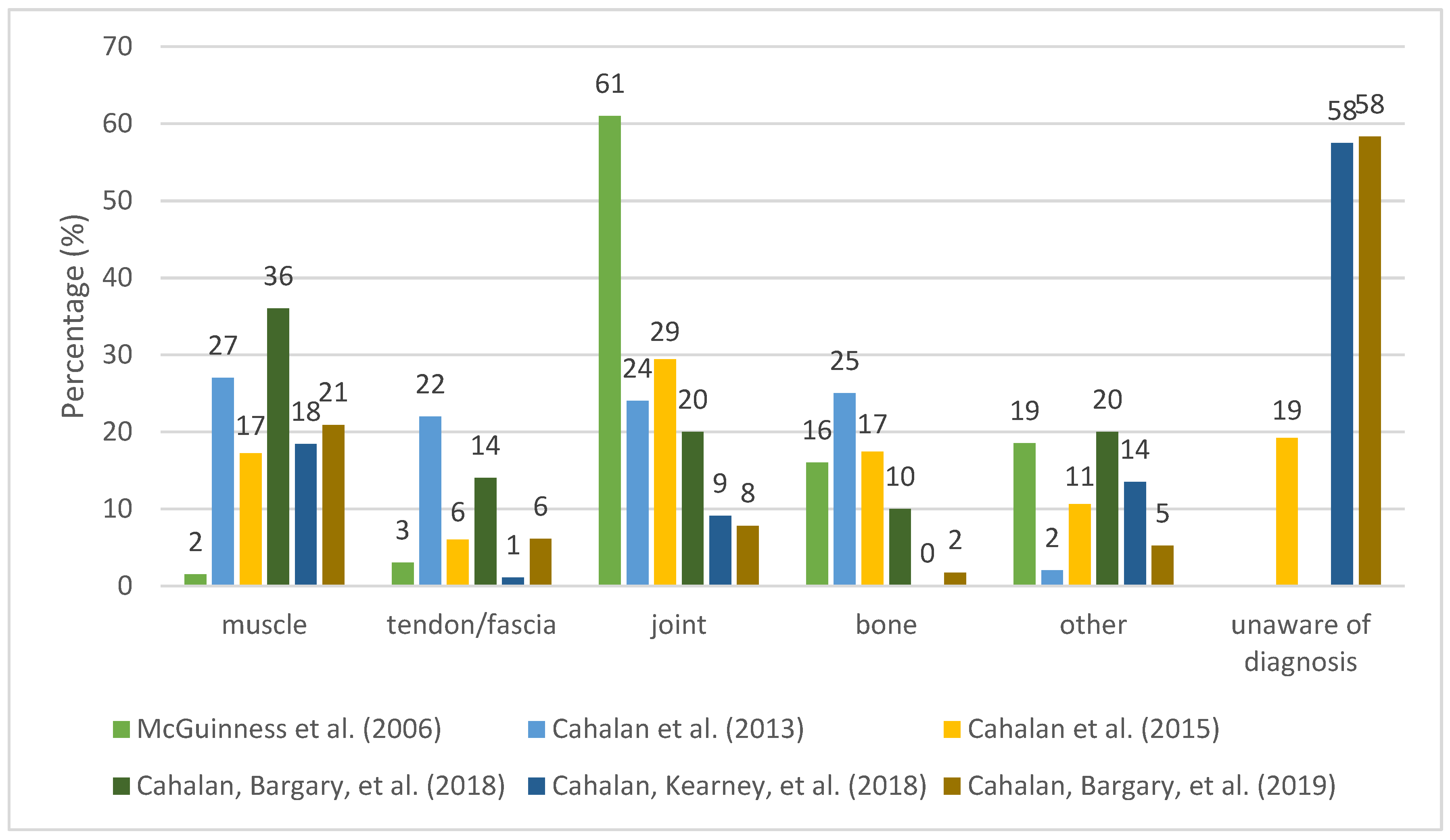
3.5. Type of Injuries
3.6. Nature, Severity and Aetiology of Injuries
3.7. Associated Factors
4. Discussion
4.1. Summary of Evidence
4.1.1. Prevalence/Incidence
4.1.2. Occurrence Pattern of Musculoskeletal Injuries
4.1.3. Associated Factors
- Provide a clear injury definition.
- Measure exposure accurately and with valid and reliable methods.
- Differentiate recurrent from new injuries.
- Describe, when possible, the mechanism of injury in detail, such as the dancer situation (context), behaviour, and biomechanical descriptions.
- Limit the recall period to 6/12 months if using retrospective questionnaires.
- Base the data collected on body area, and symptoms rather than specific diagnosis, if injury data is self-reported.
- Report the type of injury via healthcare professional, with as much detail as possible, combining injury region, type, and diagnosis.
- Complement time-loss and medical attention injury measures with a valid and sensitive self-report instrument.
- Examine risk factors prospectively, with analytical approaches that incorporate repeated measures and using a multivariate statistical approach.
- Identify and control potential confounders.
- Investigate what type, duration and intensity of warm-up and cool-down would be most beneficial for Irish dancers.
- Analyse psychosocial variables, such as catastrophizing, mood, self-esteem, and coping skills, when examining risk factors.
- Measure internal and external loads. Utilise non-linear modelling techniques when examining the relationship between training load and injury.
- Address growth-related risk factors and maturational status in young Irish dancers.
- Injury surveillance should be implemented in schools and companies. It would allow an ongoing and systematic collection and analysis of data.
- Injury surveillance should include (not exclusively) sleep quality assessment; general health assessment; a self-report instrument sensitive to overuse injuries; self-report measures of mood, catastrophizing, and coping skills; physical fitness tests of muscular strength, power, balance, flexibility, and endurance.
- Health professionals should be aware of most frequent types of injuries in Irish dancers to better understand and manage the potential risk factors.
- Preventive interventions should focus (although not exclusively) on lower extremities, especially foot and ankle, as they are the most affected body areas.
- Irish dancers should be knowledgeable of psychosocial factors associated with injury.
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Article title: |
| Sample size: |
| Participant details (age/gender/others): |
| Study purpose: |
| Dance experience: |
| Study design: |
| Injury definition: |
| Outcome measures: |
| Inclusion/exclusion criteria: |
| Number of injuries: |
| Injury estimates (incidence, prevalence, time exposure): |
| Nature of injuries (acute traumatic vs chronic overuse): |
| Anatomic injury sites: |
| Types of injuries/symptoms: |
| Injury’s severity: |
| Most common injuries: |
| Associated risk factors: |
| Main limitations & recommendations: |
| Aetiology (mechanism of injury, inciting events): |
| Comments: |
References
- Foley, C. Perceptions of Irish Step Dance: National, Global, and Local. Danc. Res. J. 2001, 33, 34. [Google Scholar] [CrossRef]
- Noon, M.; Hoch, A.Z.A.Z.A.Z.; McNamara, L.; Schimke, J. Injury Patterns in Female Irish Dancers. PM&R 2010, 2, 1030–1034. [Google Scholar] [CrossRef]
- Cahalan, R.; O’Sullivan, P.; Purtill, H.; Bargary, N.; Ni Bhriain, O.; O’Sullivan, K. Inability to perform because of pain/injury in elite adult Irish dance: A prospective investigation of contributing factors. Scand. J. Med. Sci. Sport. 2016, 26, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Cahalan, R.; Kearney, P.; Ni Bhriain, O.; Redding, E.; Quin, E.; McLaughlin, L.C.L.C.L.C.; O’ Sullivan, K. Dance exposure, wellbeing and injury in collegiate Irish and contemporary dancers: A prospective study. Phys. Ther. Sport 2018, 34, 77–83. [Google Scholar] [CrossRef]
- Gans, A. The relationship of heel contact in ascent and descent from jumps to the incidence of shin splints in ballet dancers. Phys. Ther. 1985, 65, 1192–1196. [Google Scholar] [CrossRef] [Green Version]
- Orishimo, K.F.; Kremenic, I.J.; Pappas, E.; Hagins, M.; Liederbach, M. Comparison of landing biomechanics between male and female professional dancers. Am. J. Sport. Med. 2009, 37, 2187–2193. [Google Scholar] [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, P.; O’Sullivan, K. Foot and ankle pain and injuries in elite adult Irish dancers. Med. Probl. Perform. Artist. 2014, 29, 198–206. [Google Scholar] [CrossRef]
- Ward, R.E.; Fong Yan, A.; Orishimo, K.F.; Kremenic, I.J.; Hagins, M.; Liederbach, M.; Hiller, C.E.; Pappas, E. Comparison of lower limb stiffness between male and female dancers and athletes during drop jump landings. Scand. J. Med. Sci. Sport. 2019, 29, 71–81. [Google Scholar] [CrossRef]
- Cahalan, R.; O’Sullivan, K. Musculoskeletal pain and injury in Irish dancing: A systematic review. Physiother. Pract. Res. 2013, 34, 83–92. [Google Scholar] [CrossRef]
- Cahalan, R.; Bargary, N.; O’Sullivan, K. Pain and Injury in Elite Adolescent Irish Dancers: A Cross-Sectional Study. J. Danc. Med. Sci. 2018, 22, 91–99. [Google Scholar] [CrossRef]
- Cahalan, R.; Bargary, N.; O’Sullivan, K. Dance exposure, general health, sleep and injury in elite adolescent Irish dancers: A prospective study. Phys. Ther. Sport 2019, 40, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Cahalan, R.; Comber, L.; Gaire, D.; Quin, E.; Redding, E.; Ni Bhriain, O.; O’Sullivan, K. Biopsychosocial Characteristics of Contemporary and Irish University-Level Student Dancers A Pilot Study. J. Danc. Med. Sci. 2019, 23, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cahalan, R.; Purtill, H.; O’Sullivan, P.; O’Sullivan, K. A cross-sectional study of elite adult Irish dancers: Biopsychosocial traits, pain, and injury. J. Danc. Med. Sci. 2015, 19, 31–43. [Google Scholar] [CrossRef]
- Cahalan, R.; O’Sullivan, K. Injury in Professional Irish Dancers. J. Danc. Med. Sci. 2013, 17, 150–158. [Google Scholar] [CrossRef]
- Eustergerling, M.; Emery, C. Risk Factors for Injuries in Competitive Irish Dancers Enrolled in Dance Schools in Calgary, Canada. Med. Probl. Perform. Artist. 2015, 30, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.J.; Tyson, K.D.; Johnson, V.M.; Popoli, D.M.; D’Hemecourt, P.A.; Micheli, L.J. Injuries in Irish dance. J. Danc. Med. Sci. 2013, 17, 159–164. [Google Scholar] [CrossRef]
- Liederbach, M.; Hagins, M.; Gamboa, J.M.; Welsh, T.M. Assessing and Reporting Dancer Capacities, Risk Factors, and Injuries: Recommendations from the IADMS Standard Measures Consensus Initiative. J. Danc. Med. Sci. 2012, 16, 139–153. [Google Scholar] [CrossRef]
- Van Mechelen, W. Sports injury surveillance systems: “One size fits all?”. Sport. Med. 1997, 24, 164–168. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sport. Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Higgins, J.P.T. Tools for assessing risk of reporting biases in studies and syntheses of studies: A systematic review. BMJ Open 2018, 8, e019703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bradley, J.M.; Baxter, G.D.; McDonough, S.M. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: A comparison study. BMC Res. Notes 2015, 8, 224. [Google Scholar] [CrossRef] [Green Version]
- Moita, J.P.; Nunes, A.; Esteves, J.; Oliveira, R.; Xarez, L. The relationship between muscular strength and dance injuries: A systematic review. Med. Probl. Perform. Artist. 2017, 32, 40–50. [Google Scholar] [CrossRef]
- Howick, J.; Phillips, B.; Ball, C.; Sackett, D.; Badenoch, D.; Straus, S.; Haynes, B.; Dawes, M. Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 15 April 2020).
- Kenny, S.J.; Whittaker, J.L.; Emery, C.A. Risk factors for musculoskeletal injury in preprofessional dancers: A systematic review. Br. J. Sport. Med. 2016, 50, 997–1003. [Google Scholar] [CrossRef]
- Biernacki, J.; Stracciolini, A.; Fraser, J.; Micheli, L.; Sugimoto, D. Risk Factors for Lower-Extremity Injuries in Female Ballet Dancers. Clin. J. Sport Med. 2018, 31, e64–e79. [Google Scholar] [CrossRef]
- Beasley, M.A.; Stracciolini, A.; Tyson, K.D.; Stein, C.J. Knee injury patterns in young Irish dancers. Med. Probl. Perform. Artist. 2014, 29, 70–73. [Google Scholar] [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, K. Biopsychosocial Factors Associated with Foot and Ankle Pain and Injury in Irish Dance: A Prospective Study. Med. Probl. Perform. Artist. 2017, 32, 111–117. [Google Scholar] [CrossRef]
- Walls, R.J.J.; Brennan, S.A.A.; Hodnett, P.; O’Byrne, J.M.M.; Eustace, S.J.J.; Stephens, M.M.M.; O’Byrne, J.M.; Eustace, S.J.J.; Stephens, M.M.M. Overuse ankle injuries in professional Irish dancers. Foot Ankle Surg. 2010, 16, 45–49. [Google Scholar] [CrossRef]
- McGuinness, D.; Doody, C. The injuries of competitive irish dancers. J. Danc. Med. Sci. 2006, 10, 35–39. [Google Scholar] [CrossRef]
- Kenny, S.J.; Palacios-Derflingher, L.; Whittaker, J.L.; Emery, C.A. The influence of injury definition on injury burden in preprofessional ballet and contemporary dancers. J. Orthop. Sport. Phys. Ther. 2018, 48, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.L.; Cassidy, J.D.; Côté, P.; Boyle, E.; Ramel, E.; Ammendolia, C.; Hartvigsen, J.; Schwartz, I. Musculoskeletal injury in professional dancers: Prevalence and associated factors: An international cross-sectional study. Clin. J. Sport Med. 2017, 27, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Mayers, L.; Judelson, D.; Bronner, S. The prevalence of injury among tap dancers. J. Danc. Med. Sci. 2003, 7, 121–125. [Google Scholar] [CrossRef]
- Shippen, J.M.; May, B. Calculation of muscle loading and joint contact forces during the rock step in Irish dance. J. Danc. Med. Sci. Off. Publ. Int. Assoc. Danc. Med. Sci. 2010, 14, 11–18. [Google Scholar] [CrossRef]
- Radcliffe, C.R.; Coltman, C.E.; Spratford, W.A. The effect of fatigue on peak Achilles tendon force in Irish dancing-specific landing tasks. Sport. Biomech. 2021, 27, 1–14. [Google Scholar] [CrossRef]
- Christensen, S.K.; Johnson, A.W.; Van Wagoner, N.; Corey, T.E.; Mcclung, M.S.; Hunter, I. Characteristics of Eight Irish Dance Landings Considerations for Training and Overuse Injury Prevention. J. Danc. Med. Sci. 2021, 25, 30–37. [Google Scholar] [CrossRef]
- Junge, A.; Dvorak, J. Influence of definition and data collection on the incidence of injuries in football. Am. J. Sport. Med. 2000, 28, 40–46. [Google Scholar] [CrossRef]
- Bronner, S.; Ojofeitimi, S.; Mayers, L. Comprehensive Surveillance of Dance Injuries A Proposal for Uniform Reporting Guidelines for Professional Companies. J. Danc. Med. Sci. 2006, 10, 69–80. [Google Scholar] [CrossRef]
- Clarsen, B.; Bahr, R. Matching the choice of injury/illness definition to study setting, purpose and design: One size does not fit all! Br. J. Sport. Med. 2014, 48, 510–512. [Google Scholar] [CrossRef] [Green Version]
- Mainwaring, L.; Krasnow, D.; Kerr, G. And The Dance Goes On: Psychological Impact of Injury. J. Danc. Med. Sci. 2001, 5, 105–115. [Google Scholar] [CrossRef]
- Higginbotham, O.; Cahalan, R. The Collegiate Irish Dancer’s Experience of Injury: A Qualitative Study. Med. Probl. Perform. Artist. 2020, 35, 1–9. [Google Scholar] [CrossRef]
- Gamboa, J.M.; Robert, L.A.; Fergus, A. Injury patterns in elite preprofessional ballet dancers and the utility of screening programs to identify risk characteristics. J. Orthop. Sport. Phys. Ther. 2008, 38, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Luke, A.C.; Kinney, S.A.; D’Hemecourt, P.A.; Baum, J.; Owen, M.; Micheli, L.J. Determinants of injuries in young dancers. Med. Probl. Perform. Artist. 2002, 17, 105–112. [Google Scholar] [CrossRef]
- Allen, N.; Ribbans, W.; Nevill, A.; Wyon, M. Musculoskeletal Injuries in Dance: A Systematic Review. Int. J. Phys. Med. Rehabil. 2014, 3, 1000252. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.J.; Gerrie, B.J.; Varner, K.E.; McCulloch, P.C.; Lintner, D.M.; Harris, J.D. Incidence and Prevalence of Musculoskeletal Injury in Ballet A Systematic Review. Orthop. J. Sport. Med. 2015, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vassallo, A.J.; Trevor, B.L.; Mota, L.; Pappas, E.; Hiller, C.E. Injury rates and characteristics in recreational, elite student and professional dancers: A systematic review. J. Sport. Sci. 2019, 37, 1113–1122. [Google Scholar] [CrossRef]
- Caine, D.; Bergeron, G.; Goodwin, B.J.; Thomas, J.; Caine, C.G.; Steinfeld, S.; Dyck, K.; André, S. A Survey of Injuries Affecting Pre-Professional Ballet Dancers. J. Danc. Med. Sci. 2016, 20, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Allen, N.; Nevill, A.; Brooks, J.; Koutedakis, Y.; Wyon, M. Ballet injuries: Injury incidence and severity over 1 year. J. Orthop. Sport. Phys. Ther. 2012, 42, 781–790. [Google Scholar] [CrossRef]
- Wild, C.Y.; Grealish, A.; Hopper, D. Lower limb and trunk biomechanics after fatigue in competitive female Irish dancers. J. Athl. Train. 2017, 52, 643–648. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, A.M.; Oliveira, R.; Vaz, J.R.; Cortes, N. Professional Dancers Distinct Biomechanical Pattern during Multidirectional Landings. Med. Sci. Sport. Exerc. 2019, 51, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, A.M.; Oliveira, R.; Vaz, J.R.; Cortes, N. Oxford foot model kinematics in landings: A comparison between professional dancers and non-dancers. J. Sci. Med. Sport 2020, 23, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Self, B.P.; Paine, D. Ankle biomechanics during four landing techniques. Med. Sci. Sport. Exerc. 2001, 33, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, J.T.; Padua, D.A. Sagittal-plane trunk position, landing forces, and quadriceps electromyographic activity. J. Athl. Train. 2009, 44, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devita, P.; Skelly, W. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med. Sci. Sport. Exerc. 1992, 24, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Saunier, J.; Chapurlat, R. Stress fracture in athletes. Jt. Bone Spine 2018, 85, 307–310. [Google Scholar] [CrossRef]
- Abbott, A.; Bird, M.L.; Wild, E.; Brown, S.M.; Stewart, G.; Mulcahey, M.K. Part I: Epidemiology and risk factors for stress fractures in female athletes. Physician Sportsmed. 2020, 48, 17–24. [Google Scholar] [CrossRef]
- Goulart, M.; O’Malley, M.J.; Hodgkins, C.W.; Charlton, T.P. Foot and Ankle Fractures in Dancers. Clin. Sport. Med. 2008, 27, 295–304. [Google Scholar] [CrossRef]
- Trégouët, P.; Merland, F. The Effects of Different Shoes on Plantar Forces in Irish Dance. J. Danc. Med. Sci. 2013, 17, 41–46. [Google Scholar] [CrossRef]
- Ahonen, J. Biomechanics of the Foot in Dance A Literature Review. J. Danc. Med. Sci. 2008, 12, 99–108. [Google Scholar] [CrossRef]
- Cimelli, S.N.; Curran, S.A. Influence of turnout on foot posture and its relationship to overuse musculoskeletal injury in professional contemporary dancers: A preliminary investigation. J. Am. Podiatr. Med. Assoc. 2012, 102, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Gabbett, T.J. The training-injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sport. Med. 2016, 50, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyon, M. Preparing to perform: Periodization and dance. J. Danc. Med. Sci. 2010, 14, 67–72. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Finch, C.; Bennell, K.L.; Wajswelner, H. How valid is a self reported 12 month sports injury history? Br. J. Sport. Med. 2003, 37, 545–547. [Google Scholar] [CrossRef]
- Caine, D.; Goodwin, B.J.; Caine, C.G.; Bergeron, G. Epidemiological Review of Injury in Pre-Professional Ballet Dancers. J. Danc. Med. Sci. 2015, 19, 140–149. [Google Scholar] [CrossRef]
- Russell, J.A. Preventing dance injuries: Current perspectives. Open Access J. Sport. Med. 2013, 4, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Sobrino, F.J.; de la Cuadra, C.; Guillen, P. Overuse Injuries in Professional Ballet: Injury-Based Differences Among Ballet Disciplines. Orthop. J. Sport. Med. 2015, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Grove, J.R.; Main, L.C.; Sharp, L. Stressors, recovery processes, and manifestations of training distress in dance. J. Danc. Med. Sci. 2013, 17, 70–78. [Google Scholar] [CrossRef] [Green Version]
- McEwen, K.; Young, K. Ballet and pain: Reflections on a risk-dance culture. Qual. Res. Sport. Exerc. Health 2011, 3, 152–173. [Google Scholar] [CrossRef]
- Lampe, J.; Borgetto, B.; Groneberg, D.A.; Wanke, E.M. Prevalence, localization, perception and management of pain in dance: An overview. Scand. J. Pain 2018, 18, 567–574. [Google Scholar] [CrossRef]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sport. Med. 2005, 39, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Bolling, C.; Van Mechelen, W.; Pasman, H.R.; Verhagen, E. Context Matters: Revisiting the First Step of the ‘Sequence of Prevention’ of Sports Injuries. Sport. Med. 2018, 48, 2233–2240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krosshaug, T.; Andersen, T.E.; Olsen, O.E.O.; Myklebust, G.; Bahr, R. Research approaches to describe the mechanisms of injuries in sport: Limitations and possibilities. Br. J. Sport. Med. 2005, 39, 330–339. [Google Scholar] [CrossRef]
- Bowling, A. Injuries to Dancers: Prevalence, Treatment and Perceptions of Causes. BMJ 1989, 298, 731–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, T.R.; Ambegaonkar, J.P.; Redding, E.; Wyon, M. Fit to dance survey: A comparison with dancesport injuries. Med. Probl. Perform. Artist. 2014, 29, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Bolling, C.; Mellette, J.; Pasman, H.R.; Van Mechelen, W.; Verhagen, E. From the safety net to the injury prevention web: Applying systems thinking to unravel injury prevention challenges and opportunities in Cirque du Soleil. BMJ Open Sport Exerc. Med. 2019, 5, e000492. [Google Scholar] [CrossRef] [Green Version]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring athlete training loads: Consensus statement. Int. J. Sport. Physiol. Perform. 2017, 12, 161–170. [Google Scholar] [CrossRef]
- Halson, S.L. Monitoring Training Load to Understand Fatigue in Athletes. Sport. Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [Green Version]
- West, S.W.; Clubb, J.; Torres-Ronda, L.; Howells, D.; Leng, E.; Vescovi, J.D.; Carmody, S.; Posthumus, M.; Dalen-Lorentsen, T.; Windt, J. More than a Metric: How Training Load is Used in Elite Sport for Athlete Management. Int. J. Sport. Med. 2020, 42, 300–306. [Google Scholar] [CrossRef]
- Ekegren, C.L.; Quested, R.; Brodrick, A. Injuries in pre-professional ballet dancers: Incidence, characteristics and consequences. J. Sci. Med. Sport 2014, 17, 271–275. [Google Scholar] [CrossRef]
- Eckard, T.G.; Padua, D.A.; Hearn, D.W.; Pexa, B.S.; Frank, B.S. The Relationship between Training Load and Injury in Athletes: A Systematic Review; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; Volume 48, ISBN 0123456789. [Google Scholar]
- Gabbett, T.J. Debunking the myths about training load, injury and performance: Empirical evidence, hot topics and recommendations for practitioners. Br. J. Sport. Med. 2020, 54, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition—Narrative review and new concept. Br. J. Sport. Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowerman, E.; Whatman, C.; Harris, N.; Bradshaw, E.; Karin, J. Are maturation, growth and lower extremity alignment associated with overuse injury in elite adolescent ballet dancers? Phys. Ther. Sport 2014, 15, 234–241. [Google Scholar] [CrossRef]
- Johnson, D.M.; Williams, S.; Bradley, B.; Sayer, S.; Murray Fisher, J.; Cumming, S. Growing pains: Maturity associated variation in injury risk in academy football. Eur. J. Sport Sci. 2020, 20, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Wik, E.H.; Martínez-Silván, D.; Farooq, A.; Cardinale, M.; Johnson, A.; Bahr, R. Skeletal maturation and growth rates are related to bone and growth plate injuries in adolescent athletics. Scand. J. Med. Sci. Sport. 2020, 30, 894–903. [Google Scholar] [CrossRef]
- Van Der Sluis, A.; Elferink-Gemser, M.T.; Coelho-E-Silva, M.J.; Nijboer, J.A.; Brink, M.S.; Visscher, C. Sport injuries aligned to Peak Height Velocity in talented pubertal soccer players. Int. J. Sport. Med. 2014, 35, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.S.; Lehr, M.E.; Livingston, A.; McCurdy, M.; Ware, J.K. Intrinsic modifiable risk factors in ballet dancers: Applying evidence based practice principles to enhance clinical applications. Phys. Ther. Sport 2019, 38, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.J.; Palacios-Derflingher, L.; Shi, Q.; Whittaker, J.L.; Emery, C.A. Association between Previous Injury and Risk Factors for Future Injury in Preprofessional Ballet and Contemporary Dancers. Clin. J. Sport Med. 2017, 29, 209–217. [Google Scholar] [CrossRef]
- Verhagen, E.; Van Dyk, N.; Clark, N.; Shrier, I. Do not throw the baby out with the bathwater; Screening can identify meaningful risk factors for sports injuries. Br. J. Sport. Med. 2018, 52, 1223–1224. [Google Scholar] [CrossRef]
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A Dynamic Model of Etiology in Sport Injury: The Recursive Nature of Risk and Causation. Clin. J. Sport Med. 2007, 17, 215–219. [Google Scholar] [CrossRef]
- Adam, M.U.; Brassington, G.S.; Steiner, H.; Matheson, G.O. Psychological Factors Associated with Performance-Limiting Injuries in Professional Ballet Dancers. J. Danc. Med. Sci. 2004, 8, 43–46. [Google Scholar] [CrossRef]
- Gao, B.; Dwivedi, S.; Milewski, M.D.; Cruz, A.I. Lack of Sleep and Sports Injuries in Adolescents: A Systematic Review and Meta-analysis. J. Pediatr. Orthop. 2019, 39, e324–e333. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.M. Sleep and Athletic Performance. Curr. Sport. Med. Rep. 2017, 16, 413–418. [Google Scholar] [CrossRef] [PubMed]
- von Rosen, P.; Frohm, A.; Kottorp, A.; Fridén, C.; Heijne, A. Multiple factors explain injury risk in adolescent elite athletes: Applying a biopsychosocial perspective. Scand. J. Med. Sci. Sport. 2017, 27, 2059–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.; Blom, V. Development and validation of two measures of contingent self-esteem. Individ. Differ. Res. 2007, 5, 300–328. [Google Scholar]
- Elison, J.; Partridge, J. a Relationships between shame-coping, fear of failure, and perfectionism in college athletes. J. Sport Behav. 2012, 35, 19–39. [Google Scholar]
- Hamilton, L.H.; Solomon, R.; Solomon, J. A Proposal for Standardized Psychological Screening of Dancers. J. Danc. Med. Sci. 2006, 10, 40–45. [Google Scholar] [CrossRef]
- Truong, L.K.; Bekker, S.; Whittaker, J.L. Removing the training wheels: Embracing the social, contextual and psychological in sports medicine. Br. J. Sport. Med. 2020, 55, 466–467. [Google Scholar] [CrossRef]
- Mainwaring, L.M.; Finney, C. Psychological Risk Factors and Outcomes of Dance Injury A Systematic Review. J. Danc. Med. Sci. 2017, 21, 87–96. [Google Scholar] [CrossRef]
- Truong, L.K.; Mosewich, A.D.; Holt, C.J.; Le, C.Y.; Miciak, M.; Whittaker, J.L. Psychological, social and contextual factors across recovery stages following a sport-related knee injury: A scoping review. Br. J. Sport. Med. 2020, 54, 1149–1156. [Google Scholar] [CrossRef] [Green Version]
- Wiese-Bjornstal, D.M. Psychology and socioculture affect injury risk, response, and recovery in high-intensity athletes: A consensus statement. Scand. J. Med. Sci. Sport. 2010, 20, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J. Types of Research Questions: Descriptive, Predictive, or Causal. J. Orthop. Sport. Phys. Ther. 2020, 50, 468–469. [Google Scholar] [CrossRef] [PubMed]
- Meuli, L.; Dick, F. Understanding Confounding in Observational Studies. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 737. [Google Scholar] [CrossRef] [Green Version]
- Bahr, R.; Holme, I. Risk factors for sports injuries—A methodological approach. Br. J. Sport. Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, R.O.; Simonsen, N.S.; Casals, M.; Stamatakis, E.; Mansournia, M.A. Methods matter and the ‘too much, too soon’ theory (part 2): What is the goal of your sports injury research? Are you describing, predicting or drawing a causal inference? Br. J. Sport. Med. 2020, 52, 1307–1309. [Google Scholar] [CrossRef]
- Dekkers, O.M.; Vandenbroucke, J.P.; Cevallos, M.; Renehan, A.G.; Altman, D.G.; Egger, M. COSMOS-E: Guidance on conducting systematic reviews and meta-analyses of observational studies of etiology. PLoS Med. 2019, 16, e1002742. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design (Data Source) | Sample Size (n=) | Age (Means ± SD (Range) Years | Sex (F/M) | Level | Dance Experience (Means ± SD Years) |
|---|---|---|---|---|---|---|
| McGuinness et al. (2006) [32] | Cross-sectional retrospective (questionnaire 5 y) | 159 | 18 ± 3 (15–27) | 142/17 | Competitors | 11 ± 4 (1–20) |
| Noon et al. (2010) [2] | Cross-sectional retrospective (chart review 7 y) | 69 | 13.1 (8–23) | 69/0 | 3 (compete in small, local competitions), 4 (as well as regional competitions) and 5 (qualify for international competitions) | Not reported |
| Stein et al. (2013) [16] | Cross-sectional retrospective (medical records 11 y) + Cross-sectional retrospective (questionnaire) | 255 | 13.7 ± 5 (4–47), 95% < 19 | 247/8 | Not reported | Not reported |
| Cahalan et al. (2013) [14] | Cross-sectional (retrospective online questionnaire—entire career) | 178 | >18.72% (25–34) | 111/67 | Professional | 13.2 ± 3.4 |
| Eustergerling et al. (2015) [15] | Cross-sectional retrospective questionnaire (1 y) | 36 | 16 (12–46) | 35/1 | 22 elite/14 non-elite | Not reported |
| Cahalan et al. (2015) [13] Cahalan et al. (2016) [3] | Cross-sectional retrospective (questionnaire 5 y + physical screening) | 104 (questionnaire) 84 (physical screening) | Median (IQR) prof. 23 (21; 27.5), stud. 20 (19.2), comp. 20 (18.5; 20) | % prof. 50/50 stud. 85.7/14.3 comp. 80/20 | Elite: 36 (34.6%) professionals, 28 (26.9%) students, 40 (38.5%) competitive | Prof. 17.5 ± 5.6 stud. 13.8 ± 5.3 comp. 13.0 ± 3.8 |
| Prospective cohort (1 y) (online questionnaire every month) | 84 | Median (IQR) 20 (19–23.5) | 66/18 | Elite: 15 professionals, 31 students, 38 competitive | 14 (approx.) | |
| Cahalan, Kearney et al. (2018) [4] Cahalan, Comber et al. (2019) [12] | Prospective (questionnaire every week over 1 year) | 21 ID + 29 CD | 21.5 ± 1.7 | 20/1 | Pre-professional students (full-time students in university) | “Extensive dance experience” |
| Cross-sectional (retrospective questionnaire 1 y + physical screening) | 27 ID | Median (IQR) 21(3) | 24/3 | Pre-professional students (full time students university) | “Extensive dance experience” | |
| Cahalan, Bargary et al. (2019) [11] Cahalan, Bargary et al. (2018) [10] | Prospective (questionnaire every week over 1 year) | 37 | 13–17 | 33/4 | Elite | Competing at open (elite) level for a period of at least 1 year |
| Cross-sectional (retrospective questionnaire 1 y + physical screening) | 37 | 13–17 | 33/4 | Elite | Competing at open (elite) level for a period of at least 1 year |
| Items/ Reference | McGuinness et al. (2006) [32] | Noon et al. (2010) [2] | Stein et al. (2013) [16] | Cahalan et al. (2013) [14] | Eustergerling et al. (2015) [15] | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | Cahalan, Bargary et al. (2018) [10] | Cahalan, Kearney et al. (2018) [4] | Cahalan, Comber et al. (2019) [12] | Cahalan, Bargary et al. (2019) [11] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Reporting | |||||||||||
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2 | 1 | 0 a | 1 | 1 | 0 a | 1 | 1 | 0 a | 1 | 0 a | 1 |
| 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | NA | 0 |
| 6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 7 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| External Validity | |||||||||||
| 11 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Internal Validity (Bias) | |||||||||||
| 16 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 18 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 20 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Internal Validity (Confounding) | |||||||||||
| 21 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 1 |
| 22 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 1 |
| 25 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Score | 10 | 7 | 10 | 10 | 10 | 11 | 11 | 10 | 11 | 8 | 11 |
| Percentage Score (%) | 63 | 44 | 63 | 63 | 63 | 69 | 69 | 63 | 69 | 67 | 69 |
| Level of Evidence | 3c | 3c | 3c | 3c | 3c | 3c | 3b | 3c | 3b | 3c | 3b |
| Authors | McGuinness et al. (2006) [32] | Cahalan et al. (2013) [14] | Eustergerling et al. (2015) [15] | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | Cahalan, Bargary et al. (2018) [10] | Cahalan, Kearney et al. (2018) [4] | Cahalan, Bargary et al. (2019) [11] | |
|---|---|---|---|---|---|---|---|---|---|
| Factors | |||||||||
| Use of split sole sneakers | ↓ | ||||||||
| Cool down | ↓ | = | = | ||||||
| Warm up | ↓ | = | ↑ failure to complete | ||||||
| Cross-training | = | = | = | = | = | ||||
| Dance exposure | = | = | = | ↓ | |||||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, multivariate | Multivariate | Univariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | 3c | 3b | 3b | |
| Authors | McGuinness et al. (2006) [32] | Cahalan et al. (2013) [14] | Eustergerling et al. (2015) [15] | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | |
|---|---|---|---|---|---|---|
| Factors | ||||||
| Elite level | ↑ | |||||
| Years dancing/experience | = | ↑ | = | = | ↑ | |
| Sex | = | ↑ ♀ | ||||
| Age | = | ↑ | ↑ | = | ||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, multivariate | Multivariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | |
| Authors | McGuinness et al. (2006) [32] | Cahalan et al. (2013) [14] | Eustergerling et al. (2015) [15] | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | Cahalan, Bargary et al. (2018) [10] | |
|---|---|---|---|---|---|---|---|
| Factors | |||||||
| Psychological problems/complains | ↑ | ↑ | = | ||||
| Lower mood | ↑ | = | = | ||||
| Higher catastrophizing | ↑ | = | = | ||||
| Higher levels of anger-hostility | = | ↑ | ↑ | ||||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, multivariate | Multivariate | Univariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | 3c | |
| Authors | Cahalan et al. (2013) [14] | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | Cahalan, Bargary et al. (2018) [10] | Cahalan, Kearney et al. (2018) [4] | Cahalan, Bargary et al. (2019) [11] | |
|---|---|---|---|---|---|---|---|
| Factors | |||||||
| Higher number of subjective health complaints | ↑ | ↑ | = | ||||
| A higher level of general everyday pain | ↑ | ||||||
| More body parts affected by pain/injury | ↑ | ↑ | ↑ | ||||
| Always/often dancing in pain | = | ↑ | ↑ | ||||
| Insufficient/poor sleep | ↑ | ↓ better sleep | = | ||||
| General health scores | ↓ | ||||||
| Number of weeks participants reported poor/very poor general health | ↑ | ||||||
| Statistics | Univariate | Univariate, multivariate | Multivariate | Univariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3c | 3b | 3c | 3b | 3b | |
| Authors | Cahalan et al. (2015) [13] | Cahalan et al. (2016) [3] | Cahalan, Bargary et al. (2018) [10] | Cahalan, Bargary et al. (2019) [11] | |
|---|---|---|---|---|---|
| Factors | |||||
| Physical screening tests | = | = | = | ||
| Change in weight or height | = | ||||
| Statistics | Univariate multivariate | Multivariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3b | 3c | 3b | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Póvoa, A.R.; Costa, C.M.; Simões, S.; Azevedo, A.M.; Oliveira, R. Irish Dancing Injuries and Associated Risk Factors: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 6190. https://doi.org/10.3390/ijerph20126190
Póvoa AR, Costa CM, Simões S, Azevedo AM, Oliveira R. Irish Dancing Injuries and Associated Risk Factors: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(12):6190. https://doi.org/10.3390/ijerph20126190
Chicago/Turabian StylePóvoa, Ana Rita, Cláudia Maria Costa, Sérgio Simões, Ana Morais Azevedo, and Raul Oliveira. 2023. "Irish Dancing Injuries and Associated Risk Factors: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 12: 6190. https://doi.org/10.3390/ijerph20126190