
Patterns of Health and Health Service Use in a Prospective Cohort of Aboriginal and Torres Strait Islander Children Aged 5–9 Years Living in Urban, Regional and Remote Areas of South Australia
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
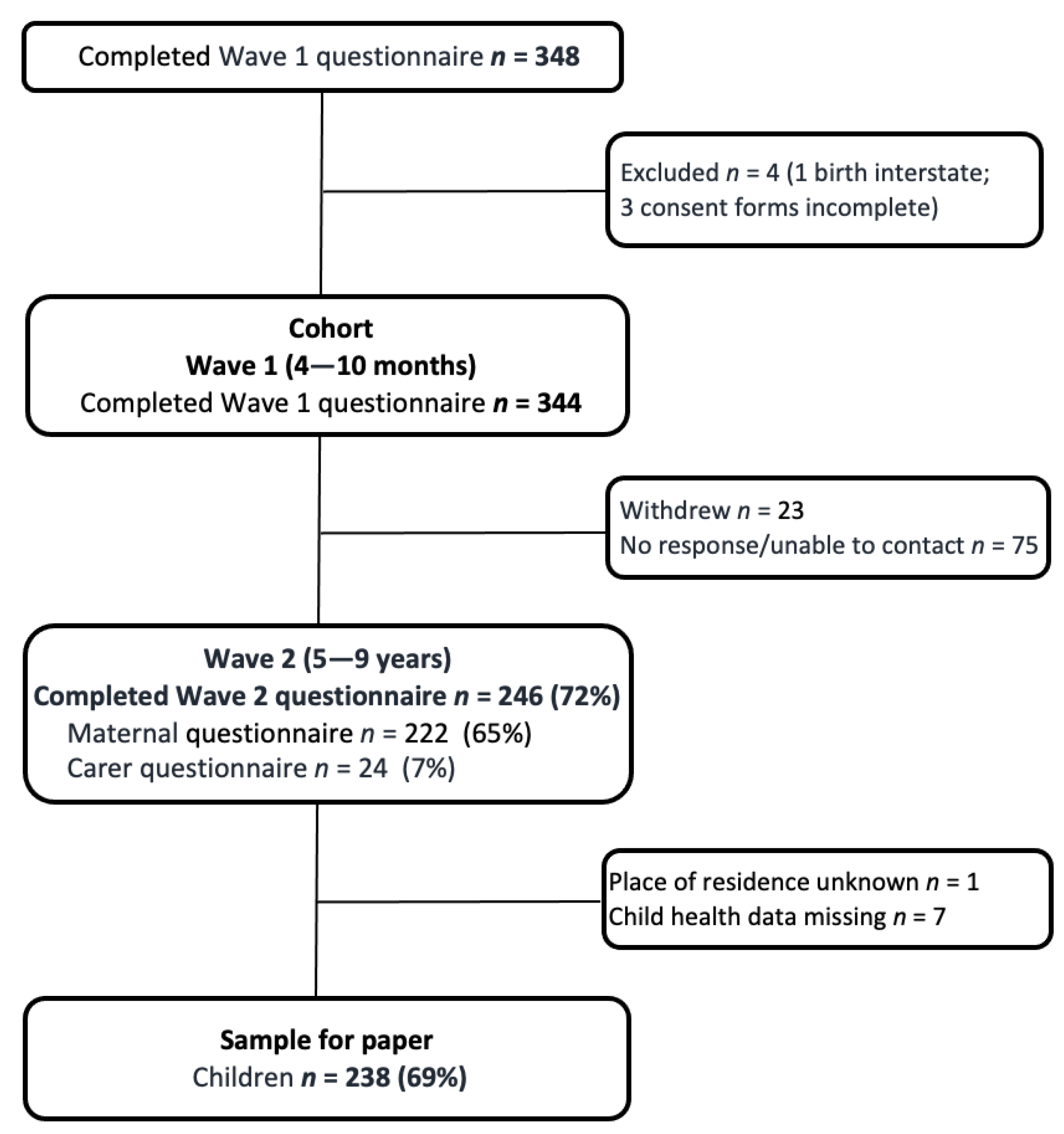
2.1. Participants
2.2. Data Collection
2.3. Analysis
3. Results
3.1. Sample
3.2. Child Health Conditions
3.3. Patterns of Health Service Use
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perkins, R.; Langton, M. (Eds.) First Australians: An Illustrated History; Miegunyah Press: Carlton, VIC, Australia, 2008. [Google Scholar]
- Raphael, B.; Swan, P.; Martinek, N. Intergenerational Aspects of Trauma for Australian Aboriginal People. In International Handbook of Multigenerational Legacies of Trauma the Plenum Series on Stress and Coping; Danieli, Y., Ed.; Springer: Boston, MA, USA, 1998; pp. 327–339. [Google Scholar]
- Zubrick, S.R.; Shepherd, C.C.; Dudgeon, P.; Gee, G.; Paradies, Y.; Scrine, C.; Walker, R. Social Determinants of Social and Emotional Wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice, 2nd ed.; Dudgeon, P., Milroy, H., Walker, R., Eds.; Australian Government, Department of The Prime Minister and Cabinet: Canberra, Australia, 2014; pp. 93–112. [Google Scholar]
- Australian Institute of Health and Welfare. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples 2015; Australian Institute of Health and Welfare: Canberra, Australia, 2015.
- Williamson, A.; Gibberd, A.; Hanly, M.J.; Banks, E.; Eades, S.; Clapham, K.; Falster, K. Social and emotional developmental vulnerability at age five in Aboriginal and non-Aboriginal children in New South Wales: A population data linkage study. Int. J. Equity Health 2019, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Chando, S.; Craig, J.C.; Burgess, L.; Sherriff, S.; Purcell, A.; Gunasekera, H.; Banks, S.; Smith, N.; Banks, E.; Woolfenden, S. Developmental risk among Aboriginal children living in urban areas in Australia: The Study of Environment on Aboriginal Resilience and Child Health (SEARCH). BMC Pediatr. 2020, 20, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, J.L.; Comino, E.; Knight, J.; Webster, V. Developmental progress in urban Aboriginal infants: A cohort study. J. Paediatr. Child. Health 2012, 48, 114–121. [Google Scholar] [CrossRef]
- Askew, D.A.; Schluter, P.J.; Spurling, G.K.; Bond, C.J.; Brown, A.D. Urban Aboriginal and Torres Strait Islander children’s exposure to stressful events: A cross-sectional study. Med. J. Aust. 2013, 199, 42–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, C.; Craig, J.C.; Clapham, K.; Williams, S.; Williamson, A. Stressful life events and resilience among caregivers of Aboriginal children in urban New South Wales: Cross-sectional findings from the Study of Environment on Aboriginal Resilience and Child Health (SEARCH). BMJ Open 2018, 8, e021687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weetra, D.; Glover, K.; Buckskin, M.; Kit, J.A.; Leane, C.; Mitchell, A.; Stuart-Butler, D.; Turner, M.; Yelland, J.; Gartland, D.; et al. Stressful events, social health issues and psychological distress in Aboriginal women having a baby in South Australia: Implications for antenatal care. BMC Pregnancy Childbirth 2016, 16, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priest, N.; Thompson, L.; Mackean, T.; Baker, A.; Waters, E. ‘Yarning up with Koori kids’—Hearing the voices of Australian urban Indigenous children about their health and well-being. Ethn. Health 2017, 22, 631–647. [Google Scholar] [CrossRef]
- Gee, G.; Dudgeon, P.; Schultz, C.; Hart, A.; Kelly, K. Aboriginal and Torres Strait Islander Social and Emotional Wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice, 2nd ed.; Dudgeon, P., Milroy, H., Walker, R., Eds.; Australian Government Department of the Prime Minister and Cabinet: Canberra, Australia, 2014; pp. 55–68. [Google Scholar]
- Shepherd, C.C.J.; Li, J.; Cooper, M.N.; Hopkins, K.D.; Farrant, B.M. The impact of racial discrimination on the health of Australian Indigenous children aged 5–10 years: Analysis of national longitudinal data. Int. J. Equity Health 2017, 16, 116. [Google Scholar] [CrossRef] [Green Version]
- Anderst, A.; Hunter, K.; Andersen, M.; Walker, N.; Coombes, J.; Raman, S.; Moore, M.; Ryan, L.; Jersky, M.; Mackenzie, A.; et al. Screening and social prescribing in healthcare and social services to address housing issues among children and families: A systematic review. BMJ Open. 2022, 12, e054338. [Google Scholar] [CrossRef]
- Chamberlain, C.; Gray, P.; Bennet, D.; Elliott, A.; Jackomos, M.; Krakouer, J.; Marriott, R.; O’Dea, B.; Andrews, J.; Andrews, S.; et al. Supporting Aboriginal and Torres Strait Islander Families to Stay Together from the Start (SAFeST Start): Urgent call to action to address crisis in infant removals. Aust. J. Soc. Issues 2022, 57, 252–273. [Google Scholar] [CrossRef]
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Daelmans, B.; Darmstadt, G.L.; Lombardi, J.; Black, M.M.; Britto, P.R.; Lye, S.; Dua, T.; Bhutta, Z.A.; Richter, L.M. Early childhood development: The foundation of sustainable development. Lancet 2017, 389, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, P.S.; Kennedy, E.C.; Patton, G.C.; Power, R.; Roseby, R.D.; Sawyer, S.M.; Brown, A.D. The quality of health research for young Indigenous Australians: Systematic review. Med. J. Aust. 2013, 199, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Comino, E.; Craig, P.; Harris, E.; McDermott, D.; Harris, M.; Henry, R.; Pulver, L.J.; Kemp, L.; Knight, J. The Gudaga Study: Establishing an Aboriginal birth cohort in an urban community. Aust. N. Z. J. Public. Health 2010, 34 (Suppl. S1), S9–S17. [Google Scholar] [CrossRef] [PubMed]
- Grace, R.; Elcombe, E.; Knight, J.; McMahon, C.; McDonald, J.; Comino, E. Early childhood development over time for a cohort of Australian Aboriginal children living in an urban environment. Aust. J. Educ. Dev. Psychol. 2017, 15, 35–52. [Google Scholar]
- The SEARCH Investigators. The Study of Environment on Aboriginal Resilience and Child Health (SEARCH): Study protocol. BMC Public. Health 2010, 10, 287. [Google Scholar]
- Williamson, A.; Skinner, A.; Falster, K.; Clapham, K.; Eades, S.J.; Banks, E. Mental health-related emergency department presentations and hospital admissions in a cohort of urban Aboriginal children and adolescents in New South Wales, Australia: Findings from SEARCH. BMJ Open 2018, 8, e023544. [Google Scholar] [CrossRef] [Green Version]
- Harding, G.; Hu, N.; Larter, N.; Montgomery, A.; Stephensen, J.; Callaghan, L.; Zwi, K.; Lingam, R.; Woolfenden, S. Health status and health service use of urban Aboriginal children attending an Aboriginal community child health service in Sydney. J. Paediatr. Child. Health 2021, 57, 1072–1077. [Google Scholar] [CrossRef]
- D’Aprano, A.; Brookes, I.; Browne, L.; Bartlett, C. Uptake of the culturally appropriate ASQ-TRAK developmental screening tool in the Australian Aboriginal and Torres Strait Islander context. Child. Care Health Dev. 2022, 49, 54–61. [Google Scholar] [CrossRef]
- Glover, K.; Morey, K.; Rumbold, A.; Middleton, P.; Brown, S.J. Transformation Protocol: Aboriginal and Torres Strait Islander Maternal and Child Health Continuity of Care Systems in South Australia; South Australian Health and Medical Research Institute: Adelaide, Australia, 2022. [Google Scholar]
- Young, C.; Gunasekera, H.; Kong, K.; Purcell, A.; Muthayya, S.; Vincent, F.; Wright, D.; Gordon, R.; Bell, J.; Gillor, G.; et al. A case study of enhanced clinical care enabled by Aboriginal health research: The Hearing, EAr health and Language Services (HEALS) project. Aust. N. Z. J. Public. Health 2016, 40, 523–528. [Google Scholar] [CrossRef]
- Buckskin, M.; Ah Kit, J.; Glover, K.; Mitchell, A.; Miller, R.; Weetra, D.; Wiebe, J.; Yelland, J.S.; Newbury, J.; Robinson, J.; et al. Aboriginal Families Study: A population-based study keeping community and policy goals in mind right from the start. Int. J. Equity Health 2013, 12, 41. [Google Scholar] [CrossRef] [Green Version]
- Weetra, D.; Glover, K.; Miller, R.; Wilson, R.; Leane, C.; Stuart-Butler, D.; Mitchell, A.; Gartland, D.; Brown, S. Community engagement in the Aboriginal Families Study: Strategies to promote participation. Women Birth 2019, 32, 72–79. [Google Scholar] [CrossRef]
- StataCorp. Stata 16 Base Reference Manual; Stata Press: College Station, TX, USA, 2019. [Google Scholar]
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure; Australian Bureau of Statistics: Canberra, Australia, 2016.
- Brown, S.J.; Weetra, D.; Glover, K.; Buckskin, M.; Ah Kit, J.; Leane, C.; Mitchell, A.; Stuart-Butler, D.; Turner, M.; Gartland, D.; et al. Improving Aboriginal women’s experiences of antenatal care: Findings from the Aboriginal families study in South Australia. Birth 2015, 42, 27–37. [Google Scholar] [CrossRef]
- Dobbins, T.A.; Sullivan, E.A.; Roberts, C.L.; Simpson, J.M. Australian national birthweight percentiles by sex and gestational age, 1998–2007. Med. J. Aust. 2012, 197, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Kong, K.; Coates, H.L. Natural history, definitions, risk factors and burden of otitis media. Med. J. Aust. 2009, 191, S39–S43. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Ear and Hearing Health of Aboriginal and Torres Strait Islander People 2021; Australian Institute of Health and Welfare: Canberra, Australia, 2022.
- Burns, J.; Thomson, N. Review of ear health and hearing among Indigenous Australians. Aust. Indig. Health Bull. 2013, 13, 1–22. [Google Scholar]
- Jervis-Bardy, J.; Sanchez, L.; Carney, A.S. Otitis media in Indigenous Australian children: Review of epidemiology and risk factors. J. Laryngol. Otol. 2014, 128 (Suppl. S1), S16–S27. [Google Scholar] [CrossRef] [PubMed]
- Zubrick, S.; Silburn, S.R.; Lawrence, D.; Mitrou, F.G.; Dalby, R.B.; Blair, E.; Griffin, J.; Milroy, H.; De Maio, J.A.; Cox, A.; et al. The Western Australian Aboriginal Child Health Survey: The Social and Emotional Wellbeing of Aboriginal Children and Young People; Curtin University of Technology and Telethon Institute for Child Health Research: Perth, Australia, 2005. [Google Scholar]
- Australian Institute of Health and Welfare. Queensland’s Deadly Ears Program: Indigenous Children Receiving Services for Ear Disease and Hearing Loss 2007–2019; Australian Institute of Health and Welfare: Canberra, Australia, 2021.
- Senate Community Affairs References Committee. Prevalence of Different Types of Speech, Language and Communication Disorders and Speech Pathology Services in Australia; Australian Institute of Health and Welfare: Canberra, Australia, 2014.
- Closing the Gap Clearinghouse (AIHW & AIFS). Ear Disease in Aboriginal and Torres Strait Islander Children. Resource Sheet No. 35. Produced by the Closing the Gap Clearinghouse; Australian Institute of Health and Welfare & Melbourne: Australian Institute of Family Studies: Canberra, Australia, 2014.
- Salmon, M.; Skelton, F.; Thurber, K.A.; Kneebone, L.B.; Gosling, J.; Lovett, R.; Walter, M. Intergenerational and early life influences on the well-being of Australian Aboriginal and Torres Strait Islander children: Overview and selected findings from Footprints in Time, the Longitudinal Study of Indigenous Children. J. Dev. Orig. Health Dis. 2019, 10, 17–23. [Google Scholar] [CrossRef]


{kind=link}
| Urban | Regional | Remote | Total | |
|---|---|---|---|---|
| n 1 (%) | n (%) | n (%) | n (%) | |
| Family members involved in parenting study child | ||||
| Mother | 103 (98.1) | 83 (100) | 46 (97.9) | 232 (98.7) |
| Father | 66 (62.9) | 50 (60.2) | 29 (61.7) | 145 (61.7) |
| Aunts/uncles | 68 (64.8) | 34 (41) | 27 (57.4) | 129 (54.9) |
| Grandparents | 43 (41.0) | 29 (34.9) | 20 (42.6) | 92 (39.1) |
| Older siblings | 37 (35.2) | 22 (26.5) | 18 (38.3) | 77 (32.8) |
| Mother’s partner | 32 (30.5) | 27 (32.5) | 16 (34) | 75 (31.9) |
| Study child lives with | ||||
| Mother | 98 (92.5) | 73 (85.9) | 43 (91.5) | 214 (89.9) |
| Father (not living with mother) | 1 (0.9) | 3 (3.5) | 0 (0) | 4 (1.7) |
| Other primary caregiver | 7 (6.6) | 9 (10.6) | 4 (8.5) | 20 (8.4) |
| Study child age at wave 2 follow-up | ||||
| 5–6 years | 62 (58.5) | 52 (61.2) | 19 (40.4) | 133 (55.9) |
| 7–9 years | 44 (41.5) | 33 (38.8) | 28 (59.6) | 105 (44.1) |
| Indigenous status of parents | ||||
| Mother Aboriginal and/or Torres Strait Islander | 96 (90.6) | 72 (84.7) | 44 (93.6) | 212 (89.1) |
| Father Aboriginal and/or Torres Strait Islander | 77 (72.6) | 62 (74.7) | 42 (89.4) | 181 (76.7) |
| Study child spends time with biological father | ||||
| Daily | 52 (49.1) | 48 (60.8) | 27 (60.0) | 127 (55.2) |
| Weekly | 5 (4.7) | 3 (3.8) | 0 (0) | 8 (3.5) |
| Monthly | 13 (12.3) | 2 (2.5) | 3 (6.7) | 18 (7.8) |
| Yearly | 9 (8.5) | 4 (5.1) | 7 (15.6) | 20 (8.7) |
| Not at all | 27 (25.5) | 22 (27.8) | 8 (17.8) | 57 (24.8) |
| Number of adults in household | ||||
| One adult | 36 (34.6) | 32 (38.1) | 10 (21.7) | 78 (33.3) |
| Two adults | 53 (51) | 41 (48.8) | 21 (45.7) | 115 (49.1) |
| Three or more adults | 15 (14.4) | 11 (13.1) | 15 (32.6) | 41 (17.5) |
| Siblings living in household | ||||
| None | 6 (5.7) | 10 (11.8) | 1 (2.1) | 17 (7.1) |
| One or two | 50 (47.2) | 28 (32.9) | 15 (31.9) | 93 (39.1) |
| Three or four | 37 (34.9) | 41 (48.2) | 22 (46.8) | 100 (42) |
| Five or more | 13 (12.3) | 6 (7.1) | 9 (19.1) | 28 (11.8) |
| Other children in household | ||||
| None | 85 (80.2) | 66 (77.6) | 37 (78.7) | 188 (79) |
| One or two | 14 (13.2) | 14 (16.5) | 7 (14.9) | 35 (14.7) |
| Three or more | 7 (6.6) | 5 (5.9) | 3 (6.4) | 15 (6.3) |
| Housing tenure 2 | ||||
| Public housing | 40 (40.8) | 34 (47.2) | 31 (72.1) | 105 (49.3) |
| Private rental | 35 (35.7) | 25 (34.7) | 7 (16.3) | 67 (31.5) |
| Own house/mortgage | 20 (20.4) | 12 (16.7) | 4 (9.3) | 36 (16.9) |
| Refuge | 3 (3.1) | 1 (1.4) | 1 (2.3) | 5 (2.3) |
| Housing stability (past 5 years) 2 | ||||
| Lived in same house | 21 (21.6) | 13 (18.3) | 14 (32.6) | 48 (22.7) |
| Moved once or twice | 39 (40.2) | 38 (53.5) | 20 (46.5) | 97 (46) |
| Moved three or more times | 37 (38.1) | 20 (28.2) | 9 (20.9) | 66 (31.3) |
| Stressful events and social health issues (past 12 months) 2 | ||||
| None | 13 (13.3) | 7 (9.6) | 5 (11.6) | 25 (11.7) |
| One or two | 25 (25.5) | 24 (32.9) | 16 (37.2) | 65 (30.4) |
| Three or more | 60 (61.2) | 42 (57.5) | 22 (51.2) | 124 (57.9) |
| Financial stress (past 12 months) 2 | ||||
| Could not pay bills on time | 55 (56.1) | 35 (48.6) | 14 (32.6) | 104 (48.8) |
| Went without meals | 13 (13.3) | 12 (16.9) | 6 (14.3) | 31 (14.7) |
| Unable to heat/cool home | 12 (12.2) | 11 (15.5) | 6 (14) | 29 (13.7) |
| Pawned/sold something | 24 (24.5) | 11 (15.5) | 5 (11.6) | 40 (18.9) |
| Assistance from welfare organisation | 21 (21.4) | 14 (19.7) | 3 (7) | 38 (17.9) |
| Mothers’ age at wave 2 follow-up 2 | ||||
| 20–24 years | 5 (4.7) | 6 (7.1) | 1 (2.1) | 12 (5) |
| 25–29 years | 43 (40.6) | 23 (27.1) | 10 (21.3) | 76 (31.9) |
| 30–34 years | 30 (28.3) | 23 (27.1) | 19 (40.4) | 72 (30.3) |
| ≥35 years | 28 (26.4) | 33 (38.8) | 17 (36.2) | 78 (32.8) |
| Mothers’ highest level education 2 | ||||
| University Degree | 11 (11.5) | 4 (5.6) | 0 (0) | 15 (7.1) |
| Diploma/Certificate | 28 (29.2) | 15 (20.8) | 13 (31) | 56 (26.7) |
| Completed Year 12 | 14 (14.6) | 14 (19.4) | 4 (9.5) | 32 (15.2) |
| Year 10 or less | 43 (44.8) | 39 (54.2) | 25 (59.5) | 107 (51) |
| Mothers’ participation in paid employment 2 | ||||
| Working full time | 16 (16.3) | 10 (13.7) | 7 (16.3) | 33 (15.4) |
| Working part time | 21 (21.4) | 12 (16.4) | 12 (27.9) | 45 (21.1) |
| Not working in paid employment | 60 (61.2) | 51 (69.9) | 24 (55.8) | 135 (63.4) |
| Study child at birth | ||||
| Infant birthweight | ||||
| ≥2500 g | 88 (85.4) | 68 (87.2) | 42 (93.3) | 198 (87.6) |
| <2500 g | 15 (14.6) | 10 (12.8) | 3 (6.7) | 28 (12.4) |
| Infant gestation | ||||
| ≥37 weeks (not preterm) | 85 (86.7) | 68 (85) | 40 (87) | 193 (86.2) |
| <37 weeks (preterm) | 13 (13.3) | 12 (15) | 6 (13) | 31 (13.8) |
| Infant birthweight for gestational age | ||||
| ≥10th percentile | 77 (83.7) | 60 (81.1) | 34 (79.1) | 171 (81.8) |
| <10th percentile | 15 (16.3) | 14 (18.9) | 9 (20.9) | 38 (18.2) |
| Total | 106 (100) | 85 (100) | 47 (100) | 238 (100) |
| Cohort (n = 238) | Urban (n = 106) | Regional (n = 85) | Remote (n = 47) | ||||
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | OR [95%CI] | n (%) | OR [95%CI] | n (%) | OR [95%CI] | |
| Physical Health | |||||||
| Respiratory condition 1 | 59 (25.0) | 29 (27.4) | 1.0 [ref] | 20 (23.8) | 0.8 [0.4–1.6] | 10 (21.7) | 0.7 [0.3–1.7] |
| Allergy/eczema | 52 (22.1) | 19 (17.9) | 1.0 [ref] | 18 (21.7) | 1.3 [0.6–2.6] | 15 (32.6) | 2.2 [1.0–4.9] |
| Skin infection | 28 (11.9) | 12 (11.3) | 1.0 [ref] | 5 (6.0) | 0.5 [0.2–1.5] | 11 (23.9) | 2.5 [1.0–6.1] |
| Injury/burn/scald | 23 (9.8) | 8 (7.5) | 1.0 [ref] | 10 (12.0) | 1.7 [0.6–4.5] | 5 (10.9) | 1.5 [0.5–4.8] |
| Ears health condition 2 | 64 (27.1) | 34 (32.1) | 1.0 [ref] | 14 (16.7) | 0.4 [0.2–0.9] | 16 (34.8) | 1.1 [0.5–2.3] |
| Hearing problem | 24 (10.2) | 9 (8.5) | 1.0 [ref] | 7 (8.3) | 1.0 [0.3–2.8] | 8 (17.4) | 2.3 [0.8–6.3] |
| Eye/vision issue | 31 (13.2) | 17 (16.0) | 1.0 [ref] | 12 (14.5) | 0.9 [0.4–2.0] | 2 (4.3) | 0.2 [0.1–1.1] |
| Weight issue (underweight/overweight) | 16 (6.8) | 7 (6.6) | 1.0 [ref] | 5 (6.0) | 0.9 [0.3–3.0] | 4 (8.7) | 1.3 [0.4–4.8] |
| Any physical health issue | 147 (62.3) | 67 (63.2) | 1.0 [ref] | 49 (58.3) | 0.8 [0.5–1.5] | 31 (67.4) | 1.2 [0.6–2.5] |
| Mental Health | |||||||
| Emotional/behavioural issue 3 | 21 (9.0) | 12 (11.3) | 1.0 [ref] | 6 (7.4) | 0.6 [0.2–1.7] | 3 (6.4) | 0.5 [0.1–2.0] |
| Anxiety/worries | 46 (19.6) | 25 (23.6) | 1.0 [ref] | 15 (18.1) | 0.7 [0.3–1.5] | 6 (13.0) | 0.5 [0.2–1.3] |
| Sleep issue | 32 (13.6) | 15 (14.2) | 1.0 [ref] | 11 (13.3) | 0.9 [0.4–2.1] | 6 (13.0) | 0.9 [0.3–2.5] |
| Any mental health issue | 65 (27.3) | 34 (32.1) | 1.0 [ref] | 20 (23.5) | 0.7 [0.3–1.2] | 11 (23.4) | 0.6 [0.3–1.4] |
| Development | |||||||
| Autism/attention problem 3 | 23 (9.8) | 8 (7.5) | 1.0 [ref] | 12 (14.8) | 2.1 [0.8–5.5] | 3 (6.4) | 0.8 [0.2–3.3] |
| Developmental issue 3 | 15 (6.4) | 8 (7.5) | 1.0 [ref] | 4 (4.9) | 0.6 [0.2–2.2] | 3 (6.4) | 0.8 [0.2–3.3] |
| Speech or language problem 3 | 39 (16.7) | 17 (16.0) | 1.0 [ref] | 15 (18.5) | 1.2 [0.6–2.6] | 7 (14.9) | 0.9 [0.4–2.4] |
| Learning difficulty 3 | 27 (11.5) | 14 (13.2) | 1.0 [ref] | 10 (12.3) | 0.9 [0.4–2.2] | 3 (6.4) | 0.4 [0.1–1.6] |
| Disability 3 | 9 (3.8) | 2 (1.9) | 1.0 [ref] | 4 (4.9) | 2.7 [0.5–15.1] | 3 (6.4) | 3.5 [0.6–22.0] |
| Any developmental issue | 58 (24.8) | 26 (24.5) | 1.0 [ref] | 24 (29.6) | 1.3 [0.7–2.5] | 8 (17.0) | 0.6 [0.3–1.5] |
| Preterm (<37 Weeks Gestation) n = 31/224 | Low Birthweight (<2500 g) n = 28/226 | Small for Gestational Age (<10th percentile) 4 n = 39/209 | ||||
|---|---|---|---|---|---|---|
| n (%) | OR [95%CI] | n (%) | OR [95%CI] | n (%) | OR [95%CI] | |
| Physical Health | ||||||
| Respiratory condition 1 | 7 (22.6) | 0.9 [0.4–2.2] | 7 (25.0) | 1.0 [0.4–2.6] | 4 (10.8) | 0.3 [0.1–1.0] |
| Allergy/eczema | 3 (10.0) | 0.4 [0.1–1.2] | 1 (3.6) | 0.1 [0.0–0.8] | 3 (8.1) | 0.3 [0.1–0.9] |
| Skin infection | 1 (3.3) | 0.2 [0.0–1.6] | 1 (3.6) | 0.2 [0.0–1.8] | 2 (5.4) | 0.3 [0.1–1.4] |
| Injury/burn/scald | 3 (10.0) | 1.0 [0.3–3.6] | 1 (3.6) | 0.3 [0.0–2.5] | 2 (5.4) | 0.5 [0.1–2.2] |
| Ear health condition 2 | 12 (38.7) | 1.9 [0.9–4.3] | 9 (32.1) | 1.4 [0.6–3.3] | 6 (16.2) | 0.5 [0.2–1.4] |
| Hearing problem | 4 (12.9) | 1.5 [0.5–4.8] | 3 (10.7) | 1.1 [0.3–4.1] | 3 (8.1) | 0.8 [0.2–3.1] |
| Eye/vision issue | 6 (20.0) | 1.7 [0.6–4.5] | 6 (21.4) | 1.9 [0.7–5.0] | 6 (16.2) | 1.2 [0.5–3.3] |
| Weight issue (underweight/overweight) | 4 (13.3) | 2.8 [0.8–9.5] | 6 (21.4) | 5.0 [1.7–15.2] | 4 (10.8) | 2.4 [0.7–8.6] |
| Any physical health issue | 17 (54.8) | 0.7 [0.3–1.5] | 16 (57.1) | 0.8 [0.4–1.8] | 18 (48.6) | 0.5 [0.2–1.1] |
| Mental Health | ||||||
| Emotional/behavioural difficulty 3 | 3 (9.7) | 1.1 [0.3–3.9] | 2 (7.1) | 0.7 [0.2–3.2] | 5 (13.2) | 1.5 [0.5–4.5] |
| Anxiety/worries | 9 (30.0) | 1.8 [0.8–4.4] | 8 (28.6) | 1.7 [0.7–4.0] | 6 (16.2) | 0.7 [0.3–1.8] |
| Sleep issue | 6 (20.0) | 1.7 [0.6–4.7] | 5 (17.9) | 1.4 [0.5–4.0] | 4 (10.8) | 0.8 [0.3–2.5] |
| Any mental health issue | 12 (38.7) | 1.9 [0.8–4.1] | 12 (42.9) | 2.1 [0.9–4.7] | 10 (26.3) | 0.9 [0.4–2.1] |
| Development | ||||||
| Autism/attention problem 3 | 6 (19.4) | 2.6 [0.9–7.3] | 4 (14.3) | 1.6 [0.5–5.3] | 5 (13.2) | 1.7 [0.6–4.9] |
| Developmental issue 3 | 4 (12.9) | 2.7 [0.8–9.1] | 3 (10.7) | 1.8 [0.5–6.9] | 3 (7.9) | 1.5 [0.4–5.9] |
| Speech or language problem 3 | 6 (19.4) | 1.3 [0.5–3.4] | 7 (25.0) | 2.0 [0.8–5.1] | 10 (26.3) | 2.4 [1.0–5.5] |
| Learning difficulty 3 | 4 (12.9) | 1.1 [0.4–3.5] | 4 (14.3) | 1.2 [0.4–3.9] | 6 (15.8) | 1.6 [0.6–4.2] |
| Disability 3 | 2 (6.5) | 1.8 [0.4–9.1] | 2 (7.1) | 2.1 [0.4–10.5] | 2 (5.3) | 1.5 [0.3–7.7] |
| Any developmental issue | 8 (25.8) | 1.1 [0.4–2.5] | 9 (32.1) | 1.6 [0.7–3.7] | 13 (34.2) | 1.8 [0.9–3.9] |
| a. Health service utilisation in the past 12 months by study children living in urban, regional and remote areas of South Australia (n = 238) | |||||||
|---|---|---|---|---|---|---|---|
| Cohort | Urban | Regional | Remote | ||||
| n (%) | n (%) | OR [95%CI] | n (%) | OR [95%CI] | n (%) | OR [95%CI] | |
| Primary Health Care | |||||||
| General practitioner | 189 (80.8) | 87 (82.1) | 1.0 [ref] | 63 (75.9) | 0.7 [0.3–1.4] | 39 (86.7) | 1.4 [0.5–3.8] |
| Child health nurse | 100 (42.4) | 37 (34.9) | 1.0 [ref] | 27 (32.5) | 0.9 [0.5–1.7] | 36 (76.6) | 6.1 [2.8–13.4] |
| Aboriginal health worker | 111 (47.2) | 34 (32.4) | 1.0 [ref] | 38 (45.8) | 1.8 [1.0–3.2] | 39 (83.0) | 10.2 [4.3–24.1] |
| Specialist Medical Practitioner | |||||||
| Paediatrician | 74 (31.2) | 32 (30.2) | 1.0 [ref] | 23 (27.4) | 0.9 [0.5–1.6] | 19 (40.4) | 1.6 [0.8–3.2] |
| Ear nose and throat specialist | 30 (12.7) | 13 (12.3) | 1.0 [ref] | 7 (8.3) | 0.7 [0.2–1.7] | 10 (21.3) | 1.9 [0.8–4.8] |
| Allied Health Practitioner | |||||||
| Audiologist | 83 (35.0) | 34 (32.1) | 1.0 [ref] | 25 (29.8) | 0.9 [0.5–1.7] | 24 (51.1) | 2.2 [1.1–4.5] |
| Speech pathologist | 64 (27.0) | 23 (21.7) | 1.0 [ref] | 28 (33.3) | 1.8 [0.9–3.4] | 13 (27.7) | 1.4 [0.6–3.0] |
| Optometrist | 73 (30.8) | 31 (29.2) | 1.0 [ref] | 30 (35.7) | 1.3 [0.7–2.5] | 12 (25.5) | 0.8 [0.4–1.8] |
| Physiotherapist | 29 (12.2) | 12 (11.3) | 1.0 [ref] | 9 (10.7) | 0.9 [0.4–2.3] | 8 (17.0) | 1.6 [0.6–4.2] |
| Psychologist/counsellor | 37 (15.6) | 18 (17.0) | 1.0 [ref] | 10 (11.9) | 0.7 [0.3–1.5] | 9 (19.1) | 1.2 [0.5–2.8] |
| Hospital Care | |||||||
| Child attended emergency department | 49 (20.8) | 17 (16.0) | 1.0 [ref] | 19 (22.9) | 1.6 [0.7–3.2] | 13 (27.7) | 2.0 [0.9–4.6] |
| Child admitted hospital | 27 (11.5) | 10 (9.5) | 1.0 [ref] | 10 (11.9) | 1.3 [0.5–3.2] | 7 (15.2) | 1.7 [0.6–4.8] |
| Child attended hospital outpatients | 37 (15.8) | 17 (16.3) | 1.0 [ref] | 13 (15.5) | 0.9 [0.4–2.1] | 7 (15.2) | 0.9 [0.4–2.4] |
| b. Health service utilisation by Aboriginal children born preterm, low birthweight and/or small for gestational age) (n = 238) | |||||||
| Preterm (<37 Weeks Gestation) n = 31/224 | Low Birthweight (<2500 g) n = 28/226 | Small for Gestational Age (<10th percentile) 1 n = 39/209 | |||||
| n (%) | OR [95%CI] | n (%) | OR [95%CI] | n (%) | OR [95%CI] | ||
| Primary Health Care | |||||||
| General practitioner | 24 (77.4) | 0.8 [0.3–2.0] | 21 (75.0) | 0.7 [0.3–1.7] | 23 (62.2) | 0.3 [0.1–0.6] | |
| Child health nurse | 14 (45.2) | 1.2 [0.5–2.5] | 12 (42.9) | 1.1 [0.5–2.4] | 12 (31.6) | 0.6 [0.3–1.4] | |
| Aboriginal health worker | 19 (61.3) | 1.9 [0.9–4.1] | 11 (39.3) | 0.7 [0.3–1.5] | 13 (34.2) | 0.5 [0.2–1.0] | |
| Specialist Medical Practitioner | |||||||
| Paediatrician | 12 (38.7) | 1.5 [0.7–3.2] | 13 (46.4) | 2.1 [0.9–4.6] | 14 (36.8) | 1.4 [0.7–3.0] | |
| Ear nose and throat specialist | 9 (29.0) | 4.2 [1.7–10.6] | 7 (25.0) | 3.1 [1.2–8.3] | 6 (15.8) | 2.1 [0.7–5.8] | |
| Allied Health Practitioner | |||||||
| Audiologist | 12 (38.7) | 1.2 [0.6–2.6] | 10 (35.7) | 1.1 [0.5–2.5] | 12 (31.6) | 0.9 [0.4–1.9] | |
| Speech pathologist | 11 (35.5) | 1.7 [0.7–3.7] | 8 (28.6) | 1.1 [0.5–2.8] | 11 (28.9) | 1.2 [0.6–2.7] | |
| Optometrist | 11 (35.5) | 1.2 [0.5–2.7] | 10 (35.7) | 1.4 [0.6–3.1] | 12 (31.6) | 1.0 [0.5–2.2] | |
| Physiotherapist | 5 (16.1) | 1.5 [0.5–4.3] | 6 (21.4) | 2.3 [0.8–6.3] | 7 (18.4) | 2.2 [0.8–5.7] | |
| Psychologist/counsellor | 7 (22.6) | 1.6 [0.6–4.2] | 6 (21.4) | 1.6 [0.6–4.2] | 5 (13.2) | 0.9 [0.3–2.5] | |
| Hospital Care | |||||||
| Child attended emergency department | 5 (16.1) | 0.7 [0.2–1.8] | 3 (10.7) | 0.4 [0.1–1.4] | 3 (7.9) | 0.3 [0.1–0.9] | |
| Child admitted to hospital | 4 (12.9) | 1.2 [0.4–3.7] | 1 (3.6) | 0.3 [0.0–2.0] | 1 (2.6) | 0.2 [0.0–1.3] | |
| Child attended hospital outpatients | 7 (23.3) | 1.8 [0.7–4.5] | 4 (14.8) | 0.9 [0.3–2.7] | 4 (10.8) | 0.6 [0.2–1.8] | |
| Urban | Regional | Remote | Total | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Ear health condition (n = 64) | ||||
| General practitioner | 28 (82.4) | 11 (78.6) | 15 (93.8) | 54 (84.4) |
| Child health nurse | 12 (35.3) | 7 (53.8) | 12 (75.0) | 31 (49.2) |
| Aboriginal health worker | 18 (52.9) | 9 (69.2) | 14 (87.5) | 41 (65.1) |
| Paediatrician | 13 (38.2) | 6 (42.9) | 9 (56.3) | 28 (43.8) |
| Ear nose and throat (ENT) specialist | 10 (29.4) | 5 (35.7) | 7 (43.8) | 22 (34.4) |
| Paediatrician and/or ENT specialist | 16 (47.1) | 8 (57.1) | 9 (56.3) | 33 (51.6) |
| Audiologist | 13 (38.2) | 7 (50.0) | 10 (62.5) | 30 (46.9) |
| Speech pathologist | 13 (38.2) | 6 (42.9) | 6 (37.5) | 25 (39.1) |
| Hospital outpatient department | 7 (21.2) | 3 (21.4) | 4 (25.0) | 14 (22.2) |
| Hospital emergency department | 5 (14.7) | 7 (53.8) | 4 (25.0) | 16 (25.4) |
| Mental health issue (n = 65) | ||||
| General practitioner | 29 (85.3) | 15 (75.0) | 10 (90.9) | 54 (83.1) |
| Child health nurse | 11 (32.4) | 6 (30.0) | 8 (72.7) | 25 (38.5) |
| Aboriginal health worker | 13 (39.4) | 11 (55.0) | 9 (81.8) | 33 (51.6) |
| Paediatrician | 14 (41.2) | 11 (55.0) | 6 (54.5) | 31 (47.7) |
| Psychologist/counsellor | 12 (35.3) | 7 (35.0) | 4 (36.4) | 23 (35.4) |
| Hospital outpatient department | 10 (30.3) | 6 (30.0) | 2 (20.0) | 18 (28.6) |
| Hospital emergency department | 5 (14.7) | 4 (20.0) | 4 (36.4) | 13 (20.0) |
| Developmental issue (n = 58) | ||||
| General practitioner | 20 (76.9) | 21 (87.5) | 7 (87.5) | 48 (82.8) |
| Child health nurse | 10 (38.5) | 6 (25.0) | 8 (100.0) | 24 (41.4) |
| Aboriginal health worker | 12 (46.2) | 11 (45.8) | 8 (100.0) | 31 (53.4) |
| Paediatrician | 18 (69.2) | 13 (54.2) | 6 (75.0) | 37 (63.8) |
| Audiologist | 10 (38.5) | 8 (33.3) | 5 (62.5) | 23 (39.7) |
| Speech pathologist | 14 (53.8) | 18 (75.0) | 5 (62.5) | 37 (63.8) |
| Physiotherapist | 8 (30.8) | 4 (16.7) | 3 (37.5) | 15 (25.9) |
| Psychologist/counsellor | 10 (38.5) | 5 (20.8) | 4 (50.0) | 19 (32.8) |
| Hospital outpatient department | 9 (34.6) | 7 (29.2) | 1 (14.3) | 17 (29.8) |
| Hospital emergency department | 3 (11.5) | 7 (29.2) | 2 (25.0) | 12 (20.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gartland, D.; Nikolof, A.; Glover, K.; Leane, C.; Cahir, P.; Hameed, M.; Brown, S.J. Patterns of Health and Health Service Use in a Prospective Cohort of Aboriginal and Torres Strait Islander Children Aged 5–9 Years Living in Urban, Regional and Remote Areas of South Australia. Int. J. Environ. Res. Public Health 2023, 20, 6172. https://doi.org/10.3390/ijerph20126172
Gartland D, Nikolof A, Glover K, Leane C, Cahir P, Hameed M, Brown SJ. Patterns of Health and Health Service Use in a Prospective Cohort of Aboriginal and Torres Strait Islander Children Aged 5–9 Years Living in Urban, Regional and Remote Areas of South Australia. International Journal of Environmental Research and Public Health. 2023; 20(12):6172. https://doi.org/10.3390/ijerph20126172
Chicago/Turabian StyleGartland, Deirdre, Arwen Nikolof, Karen Glover, Cathy Leane, Petrea Cahir, Mohajer Hameed, and Stephanie J. Brown. 2023. "Patterns of Health and Health Service Use in a Prospective Cohort of Aboriginal and Torres Strait Islander Children Aged 5–9 Years Living in Urban, Regional and Remote Areas of South Australia" International Journal of Environmental Research and Public Health 20, no. 12: 6172. https://doi.org/10.3390/ijerph20126172