
Challenges in the Management of Sarcopenia in the Primary Care Setting: A Scoping Review

Abstract
:1. Introduction
2. Material and Methods
- How is sarcopenia managed in a primary care setting?
- What are the challenges in the screening of sarcopenia in a primary care setting?
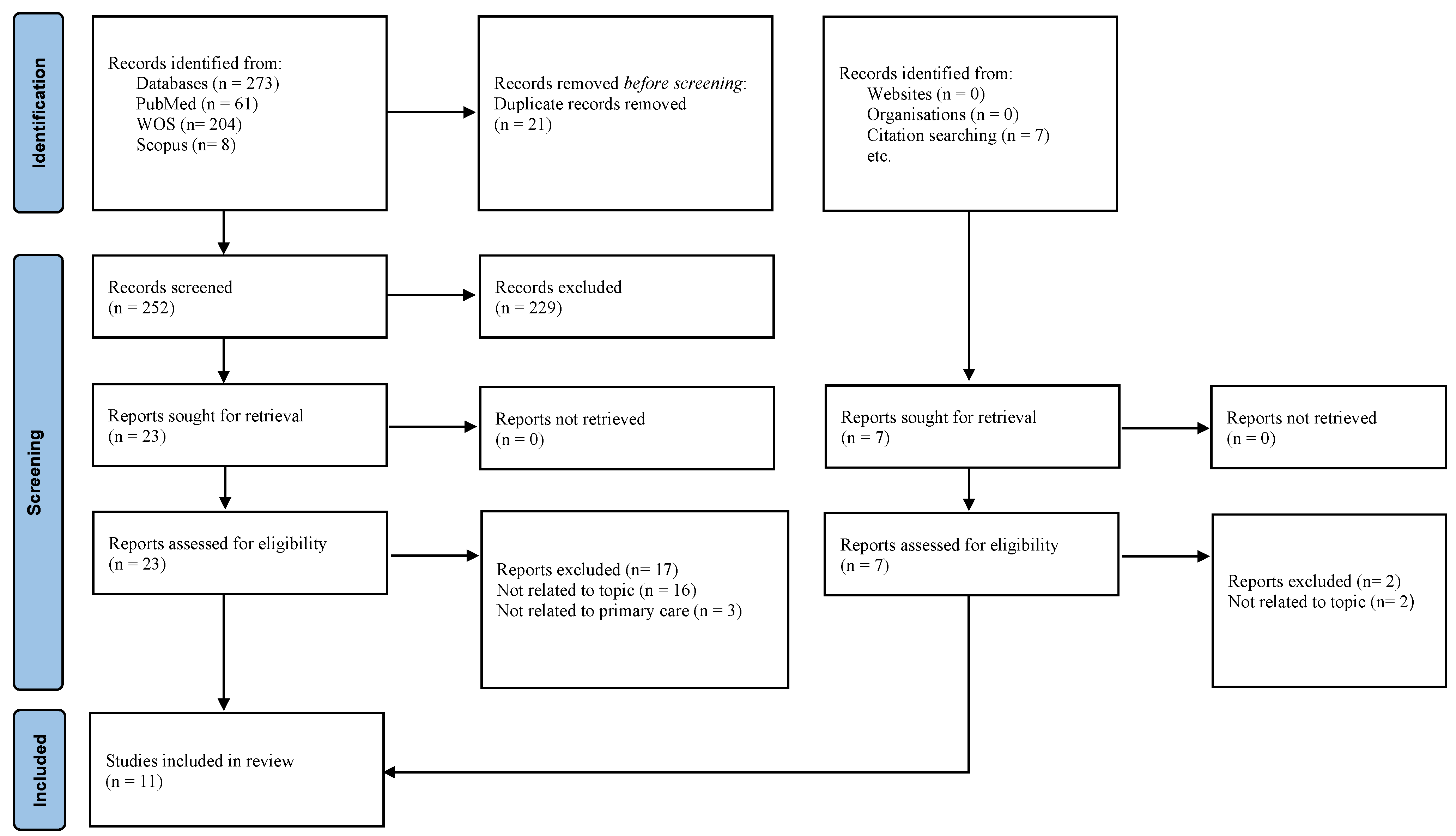
Search Strategy
3. Results
3.1. Challenges in the Screening of Sarcopenia
3.2. Challenges in the Diagnosis of Sarcopenia
4. Discussion
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Ageing and Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 28 December 2022).
- McPhee, J.S.; Cameron, J.; Maden-Wilkinson, T.; Piasecki, M.; Yap, M.H.; Jones, D.A.; Degens, H. The Contributions of Fiber Atrophy, Fiber Loss, in Situ Specific Force, and Voluntary Activation to Weakness in Sarcopenia. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1287–1294. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Diagnosis and Mechanisms Sarcopenia: Origins and Clinical Relevance. J. Nutr. 1997, 127 (Suppl. S5), 990S–991S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Pang, B.W.J.; Wee, S.L.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Ng, D.H.M.; Tan, Q.L.L.; Chen, K.K.; Jagadish, M.U.; Ng, T.P. Prevalence and Associated Factors of Sarcopenia in Singaporean Adults—The Yishun Study. J. Am. Med. Dir. Assoc. 2021, 22, 885.e1–885.e10. [Google Scholar] [CrossRef]
- Pipek, L.Z.; Baptista, C.G.; Nascimento RF, V.; Taba, J.V.; Suzuki, M.O.; do Nascimento, F.S.; Martines, D.R.; Nii, F.; Iuamoto, L.R.; Carneiro-D’Albuquerque, L.A.; et al. The impact of properly diagnosed sarcopenia on postoperative outcomes after gastrointestinal surgery: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0237740. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2021, 13, 86–99. [Google Scholar] [CrossRef]
- Ranee, R.; Shahar, S.; You, Y.X.; Singh DK, A.; Sakian NI, M. Prevalence and Risk Factors of Sarcopenia among Community Dwelling Older Adults in Klang Valley. Malays. J. Med. Health Sci. 2022, 18, 177–186. [Google Scholar]
- Sazlina, S.-G.; Lee, P.Y.; Chan, Y.M.; AHamid, M.S.; Tan, N.C. The prevalence and factors associated with sarcopenia among community living elderly with type 2 diabetes mellitus in primary care clinics in Malaysia. PLoS ONE 2020, 15, e0233299. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Reginster, J. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [Green Version]
- WHO. Primary Care Key Facts 1–6. 2021. Available online: https://www.who.int/teams/integrated-health-services/clinical-services-and-systems/primarycare#:~:text=Primary%20care%20is%20a%20model,have%20equal%20access%20to%20services (accessed on 17 January 2023).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Social Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Joanne Briggs Institute. Methodology for JBI Scoping Reviews; Joanne Briggs Institute: Adelaide, Australia, 2015; pp. 1–24. [Google Scholar]
- Hong, Q.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT): User Guide; McGill: Montréal, QC, Canada, 2018; pp. 1–11. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Lino, V.T.S.; Rodrigues, N.C.P.; O’Dwyer, G.; Andrade, M.K.D.N.; Mattos, I.E.; Portela, M.C. Handgrip strength and factors associated in poor elderly assisted at a primary care unit in Rio de Janeiro, Brazil. PLoS ONE 2016, 11, e0166373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merchant, R.A.; Hui, R.J.Y.; Kwek, S.C.; Sundram, M.; Tay, A.; Jayasundram, J.; Chen, M.Z.; Ng, S.E.; Tan, L.F.; Morley, J.E. Rapid Geriatric Assessment Using Mobile App in Primary Care: Prevalence of Geriatric Syndromes and Review of Its Feasibility. Front. Med. 2020, 7, 261. [Google Scholar] [CrossRef]
- Lera, L.; Albala, C.; Leyton, B.; Márquez, C.; Angel, B.; Saguez, R.; Sánchez, H. Reference values of hand-grip dynamometry and the relationship between low strength and mortality in older Chileans. Clin. Interv. Aging 2018, 13, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lera, L.; Angel, B.; Márquez, C.; Saguez, R.; Albala, C. Software for the diagnosis of sarcopenia in community-dwelling older adults: Design and validation study. JMIR Med. Inform. 2020, 8, e13657. [Google Scholar] [CrossRef] [PubMed]
- Offord, N.J.; Clegg, A.; Turner, G.; Dodds, R.M.; Sayer, A.A.; Witham, M.D. Current practice in the diagnosis and management of sarcopenia and frailty—Results from a UK-wide survey. J. Frailty Sarcopenia Falls 2019, 4, 71–77. [Google Scholar] [CrossRef]
- Cheng, K.Y.K.; Chow, S.K.H.; Hung, V.W.Y.; Wong, C.H.W.; Wong, R.M.Y.; Tsang, C.S.L.; Kwok, T.; Cheung, W.H. Diagnosis of sarcopenia by evaluating skeletal muscle mass by adjusted bioimpedance analysis validated with dual-energy X-ray absorptiometry. J. Cachexia Sarcopenia Muscle 2021, 12, 2163–2173. [Google Scholar] [CrossRef]
- Piotrowicz, K.; Głuszewska, A.; Czesak, J.; Fedyk-Łukasik, M.; Klimek, E.; Sánchez-Rodríguez, D.; Skalska, A.; Gryglewska, B.; Grodzicki, T.; Gąsowski, J. SARC-F as a case-finding tool for sarcopenia according to the EWGSOP2. National validation and comparison with other diagnostic standards. Aging Clin. Exp. Res. 2021, 33, 1821–1829. [Google Scholar] [CrossRef]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J.; Wang, Y.; Li, Y.; Han, Z.; Zhang, D.; et al. SARC-F for sarcopenia screening in community-dwelling older adults Are 3 items enough? Medicine 2018, 97, e11726. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Q.; Li, Y.; Xia, X.; Deng, C.; Wu, X.; Hou, L.; Yue, J.; Dong, B. Associations of geriatric nutrition risk index and other nutritional risk-related indexes with sarcopenia presence and their value in sarcopenia diagnosis. BMC Geriatr. 2022, 22, 327. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Park, S. Gender-Specific Risk Factors and Prevalence for Sarcopenia among Community-Dwelling Young-Old Adults. Int. J. Environ. Res. Public Health 2022, 19, 7232. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.F.; do Livramento Fortes Figueiredo, M.; Darder, J.J.T.; Dos Santos, A.M.R.; Tyrrell, M.A.R. Sarcopenia screening in elderly in primary health care: Nurse knowledge and practices. Rev. Bras. Enferm. 2020, 73 (Suppl. S3), e20200421. [Google Scholar] [CrossRef]
- Dedeyne, L.; Reijnierse, E.M.; Pacifico, J.; Kay, J.E.; Maggs, P.; Verschueren, S.; Tournoy, J.; Gielen, E.; Lim, W.K.; Maier, A.B. SARC-F Is Inaccurate to Identify Geriatric Rehabilitation Inpatients at Risk for Sarcopenia: RESORT. Gerontology 2021, 68, 252–260. [Google Scholar] [CrossRef]
- Tanaka, T.; Takahashi, K.; Akishita, M.; Tsuji, T.; Iijima, K. “Yubi-wakka” (finger-ring) test: A practical self-screening method for sarcopenia, and a predictor of disability and mortality among Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2018, 18, 224–232. [Google Scholar] [CrossRef]
- Ishii, S.; Tanaka, T.; Shibasaki, K.; Ouchi, Y.; Kikutani, T.; Higashiguchi, T.; Obuchi, S.P.; Ishikawa-Takata, K.; Hirano, H.; Kawai, H.; et al. Development of a simple screening test for sarcopenia in older adults. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 93–101. [Google Scholar] [CrossRef]
- Witham, M.D.; Heslop, P.; Dodds, R.M.; Clegg, A.P.; Hope, S.V.; Mcdonald, C.; Smithard, D.; Storey, B.; Tan, A.L.; Thornhill, A.; et al. Developing a UK sarcopenia registry: Recruitment and baseline characteristics of the SarcNet pilot. Age Ageing 2021, 50, 1762–1769. [Google Scholar] [CrossRef]


{kind=link}
| Population | Concept | Context |
|---|---|---|
| (i) Elderly population (ii) Male and female gender | Any challenges in the management of sarcopenia from a primary care perspective from 2012 through 2022. | (i) Research articles are limited to studies written in English language; (ii) Original research articles; (iii) Full text of original articles. |
| Is the Sampling Strategy Relevant to Address the Research Question? | Is the Sample Representative of the Target Population | Are the Measurements Appropriate? | Is the Risk of Nonresponse Bias Low? | Is the Statistical Analysis Appropriate to Answer the Research Question? | ||
|---|---|---|---|---|---|---|
| (Lino et al., 2016) [18] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Merchant et al., 2020) [19] | Quantitative descriptive | Yes | Yes | Yes | Cannot tell | Yes |
| (Lera et al., 2018) [20] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Lera et al., 2020) [21] | Quantitative descriptive | Yes | Yes | Yes | Cannot tell | Yes |
| (Offord et al., 2019) [22] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Cheng et al., 2021 [23] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Piotrowicz et al., 2021) [24] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Yang et al., 2018) [25] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Xiang et al., 2022) [26] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| (Hwang and Park 2022) [27] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| Author | Types of Study | 1.1 | 1.2 | 1.3 | 1.4 | 1.5 |
| Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated by data? | Is there coherence between qualitative data sources, collection, analysis, and interpretation? | ||
| (Silva et al., 2020) [28] | Qualitative | Yes | Yes | Yes | Yes | Yes |
| Author | Article Type | Sample Size | Challenges in the Management of Sarcopenia in Primary Care Setting |
|---|---|---|---|
| (Lino et al., 2016) [18] | Cross sectional | 180 | Hand grip strength assessment is a feasible and cheaper option in primary care that offers solutions to the usual high cost involved in identifying the risk of sarcopenia. |
| (Merchant et al., 2020) [19] | Cross sectional | 2589 | Primary care physicians face the problem of a shortage of time, multidisciplinary resources, or skills to perform geriatric assessment, and the RGA app is a quick and feasible tool that offers a solution to the problem. |
| (Lera et al., 2018) [20] | Cohort | 5250 | A dynamometer could be used as a low-cost and feasible tool to identify the elderly at risk for sarcopenia in primary health care and overcome the issue of the expensive and inaccessible method of dual-energy X-ray absorptiometry. |
| (Silva et al., 2020) [28] | Qualitative | 24 | Nurses in primary care lack knowledge on sarcopenia. |
| (Lera et al., 2020) [21] | Cohort | 430 | (HTSMayor) software serves as an alternative for the expensive and inaccessible DXA in primary care. |
| (Offord et al., 2019) [22] | Cross sectional | 61 | Identification of sarcopenia among UK healthcare professionals is low, and there is a lack of diagnosis based on the standard guideline. |
| (Cheng et al., 2021) [23] | Cross sectional | 1587 | BIA can be used in a community setting but may overestimate skeletal muscle mass. Prevalence (40.8%) based on predicted ASM from BIA compared to (39.4%) on DXA-measured ASM. |
| (Piotrowicz et al., 2021) [24] | Cross sectional | 73 | SARC-F has a limitation in the case finding of sarcopenia due to its low sensitivity (35%). A high specificity (85.7%) of SARC-F could be used to rule out sarcopenia. |
| (Yang et al., 2018) [25] | Cross sectional | 384 | The 3-item SARC-F may not be suitable for sarcopenia screening at the community level compared to the standard SARC-F with sensitivity and specificity values of 29.5% and 98.1%. |
| (Xiang et al., 2022) [26] | Cohort | 3829 | Diagnostic tools such as DXA or BIA may be unavailable in the primary care setting due to the cost involved. |
| (Hwang and Park 2022) [27] | Cross sectional | 1293 | Risk factors for sarcopenia are rarely identified by primary care health professionals. Lack of knowledge about sarcopenia increases the tendency to miss the diagnosis of sarcopenia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandayah, T.; Safian, N.; Azhar Shah, S.; Abdul Manaf, M.R. Challenges in the Management of Sarcopenia in the Primary Care Setting: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 5179. https://doi.org/10.3390/ijerph20065179
Kandayah T, Safian N, Azhar Shah S, Abdul Manaf MR. Challenges in the Management of Sarcopenia in the Primary Care Setting: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(6):5179. https://doi.org/10.3390/ijerph20065179
Chicago/Turabian StyleKandayah, Thinakaran, Nazarudin Safian, Shamsul Azhar Shah, and Mohd Rizal Abdul Manaf. 2023. "Challenges in the Management of Sarcopenia in the Primary Care Setting: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 6: 5179. https://doi.org/10.3390/ijerph20065179