1. Introduction
Dental fluorosis—a condition where the appearance of the tooth enamel changes—results from an excessive intake of fluoride during the tooth development period. Fluorosis occurs in many regions of the world [
1,
2,
3], with a global prevalence of over 20 million cases as estimated by [
4]. Although fluoride is known for its benefits in preventing dental caries, its use requires a balance between caries protection and the risk of dental fluorosis. It is evident from the existing literature that excessive fluoride exposure can take place due to the consumption of fluoride-contaminated groundwater [
1]. Occurrences of fluorosis also depend on various factors, such as the dose, the duration of exposure, individual health conditions, and so on. The swallowing of fluoridated toothpastes is also a risk factor for fluorosis in young children under the age of six years [
5]. Many studies have found that the disease is most prevalent between 5 and 8 years of age, with both genders equally affected [
6].
Although mild dental fluorosis does not degrade the health of teeth, the aesthetic appearance of teeth is commonly a major concern in many people. Young people may make negative psychosocial judgements of other young people based on their enamel appearance [
7]. It has been reported that dental fluorosis can diminish their happiness and self-confidence. In addition, several negative attributes—such as being seen as less attractive, less clean, less healthy, less intelligent, less reliable, and less social—are attached to people with severe fluorosis compared to normal people [
8,
9]. Moreover, children with severe fluorosis can also experience significant psychosocial suffering [
10]. Fortunately, treatments for dental fluorosis exist—such as microabrasion in mild cases, or tooth restoration in severe cases (tooth grinding with composite filling, composite veneer, or ceramic veneer)—and can significantly improve patients’ quality of life [
11]. Traditionally, the diagnosis of dental fluorosis relies upon a visual examination of teeth, together with various pathological grading systems for fluorosis. The most commonly used classification system is Dean’s index [
12], developed by H. T. Dean in 1934, which divides the cosmetic deviations of the teeth into six levels, as described in
Table 1. Other alternative indices, such as the Thylstrup-–Fejerskov (TF) index [
13], are also widely used.
In the dental fluorosis screening process, clinical grading of tooth enamel is subject to subjective biases by examiners due to various factors—for example, knowing the vicinity where a subject resides possibly hints at the subject’s fluoridation status. Such a bias can be addressed by using a standardized image-based method, where examiners remotely evaluate clinical photographs without prior knowledge of the subject’s location. However, the examination of clinical photographs is still prone to biases, because individual examiners inherently choose different grading thresholds. As a result, there has been interest in developing an image-based automated system for examining the severity of fluorosis. One of the pioneering works on dental fluorosis image analysis is by Pretty et al. [
15], where the authors utilized image processing techniques to quantify dental fluorosis levels in fluorescence imaging and experimentally showed that the quantity has a good correlation with the TF index. McGrady et al. [
16] also further showed that populations with different levels of fluoride exposure could be discriminated by fluorescence imaging. A dual-camera system that can simultaneously capture both a fluorescence image and a polarized white-light image was used by Liu et al. [
17] as a part of an automatic fluorosis classification system. In their work, both image modalities were used to extract five-dimensional fluorosis feature vectors, and then TF index predictions were obtained by RUSBoost [
18], with a decision tree as a base learner.
The existing literature on automatic fluorosis classification typically relies on fluorescence images acquired from a quantitative light-induced fluorescence (QLF) imaging device, as it can measure the percentage of fluorescence change in demineralized enamel, which becomes lower due to fluorosis. Other approaches based on techniques such as Raman spectroscopy [
19] can also be found in the literature. However, those pieces of specialty equipment come with a disadvantage, due to their non-ubiquity. Alternatively, handheld digital cameras—including smartphone cameras—are more accessible to the public. According to [
20], photographic assessments of dental fluorosis, where the photos were taken using a digital SLR camera, exhibited good agreement with clinical assessments using Dean’s index. As a result, it is intuitively tempting to develop an automated dental fluorosis classification tool to assess the severity of dental fluorosis in photographic images of teeth. Such a device could help reduce examiners’ workload in the screening process, which is normally time-consuming, laborious, and prone to human error.
Although photographic image analysis has been introduced to solve some dentistry problems such as dental plaque detection [
20,
21,
22,
23,
24,
25,
26] in the past, a few studies have been conducted on the automatic dental fluorosis classification of photographic images. One example includes the work by Yeesarapat et al. [
14], where the authors proposed an image-based dental fluorosis classification system using multi-prototype fuzzy c-means (FCM) to classify dental fluorosis into four classes adapted from Dean’s index: Normal, Fluorosis Stage 1, Fluorosis Stage 2, and Fluorosis Stage 3. Their Normal, Fluorosis Stage 2, and Fluorosis Stage 3 classes correspond to Normal, Moderate, and Severe in Dean’s index, respectively, while Fluorosis Stage 1 was created to cover three classes: Questionable, Very Mild, and Mild, as summarized in
Table 1. FCM was used to cluster six-dimensional pixel values in the red, green, and blue (RGB) and hue, saturation, and intensity (HIS) color spaces for each of three groups: normal white (either white or yellow), opaque white, and brown pixels. A total of 1600 prototypes were obtained, and the nearest prototype classifier was used to assign each pixel value to one of these three groups. The classification criteria based on the amount of pixel values found in each group were then applied to classify an image of tooth enamel into four dental fluorosis conditions. Their proposed method yielded a correct classification rate of 42.85% for the training set and 53.33% for the blind test set. However, the process required dentists to manually select the tooth regions in the image. Their model selection was also performed manually, and the number of clusters was suboptimal.
Inspired by the work by Yeesarapat et al. [
14], this paper proposes an image-based automatic system for dental fluorosis classification based on image segmentation through multi-prototype unsupervised possibilistic fuzzy clustering (UPFC). Feature vectors composed of pixel values in the RGB and HSI color spaces were clustered into five classes: white, yellow, opaque, brown, and background, where the number of clusters was optimized using the cuckoo Search (CS) algorithm. A set of pixels from seven images were used for training, and the best prototypes were chosen by 10-fold cross-validation. After that, tooth segmentation was implemented based on these clusters through the fuzzy k-nearest neighbor (FKNN) method. The proportions of opaque and brown pixels in the tooth region were used to determine four stages of fluorosis: Normal, Stage 1, Stage 2, and Stage 3, with the same severity levels defined by Yeesarapat et al. [
14]. We evaluated our proposed method on 128 blind test images taken from 128 subjects in both segmentation and classification tasks. In overall, the proposed system provided a correct dental fluorosis classification for 86 out of 128 images, which is 13.33% better than that obtained in the prior work [
14].
Although this image-based fluorosis detection system does not include other tooth deficiency factors—for example, mineralized tissue loss causing cavitation—the dentist can use this system in a pre-screening process to grade the condition before treating the patient. According to the dentist, the treatment rules based on the tooth condition according to the
Table 1 are as follows:
If there are some opaque white areas (Stage 1 fluorosis), the treatment can be whitening or microabrasion.
If there are a lot of opaque white areas and some brown areas (Stage 2 fluorosis), the treatment can be tooth restoration, e.g., tooth grinding with composite filling, composite veneer, or ceramic veneer.
If there are a lot of brown areas (Stage 3 fluorosis), the treatment can be similar to the Stage 2 treatment. However, the ceramic used in the treatment might need to be more opaque to cover all of the underlying color. In addition, a restorative dentistry specialist is needed in this case, rather than a general practice dentist.
However, this system can be used in rural areas where there are not enough dentists. Moreover, the pictures can be taken by non-professional personnel with no mouth retractor or the need for a process to dry the teeth. If any mild/severe cases are detected, those patients can be sent to the dentist to recheck for a definitive diagnosis of their teeth before the treatment.
The rest of this paper is organized as follows:
Section 2 describes the related backgrounds—HSI color space, UPFC, CS, and FKNN. The dataset and the pipeline of our proposed method (i.e., clustering, segmentation, and classification) are described in
Section 3, followed by the experimental results and discussions in
Section 4. Finally, our concluding remarks are provided in
Section 5.
3. Materials and Methods
The proposed automatic system for dental fluorosis classification is based on semantic segmentation of tooth enamel, where each pixel is labeled into five color classes: white, yellow, opaque, brown, and background. The white and light-yellow colors, in general, belong to healthy tooth enamel, while opaque-white and brown colors are considered to be indicators of dental fluorosis in Dean’s index. The background class is assigned to all pixels not in the tooth region. A feature vector was formed by considering a pixel value in both the RGB and HSI color spaces, where the HSI features were computed by (1). The multi-prototype UPFC was used to generate clusters of feature vectors, and the optimal number of clusters was determined by the CS algorithm. One class of colors might consist of multiple clusters. The resulting clusters were used for tooth segmentation to extract a binary mask of the tooth region. Fluorosis severity was graded by evaluating the proportions of opaque and brown pixels in the tooth region. In this paper, four levels of fluorosis are considered, as defined by Yeesarapat et al. [
14] in
Table 1. The ground truth in the experiments was generated by a D.D.S. dentist with more than 10 years of experience.
3.1. Multi-Prototype Generation
Given a set of pixel values from the training images, the multi-prototype UPFC was used to generate clusters of RGB and HSI feature vectors. The overall training process was as presented in Algorithm 3, where the CS algorithm was used to determine the optimal number of clusters (
). The training process started by randomly initializing a set of
N nests,
, where
is the
i-th nest. Each nest
contains a randomly chosen integer
representing the number of clusters between
and
. The fitness value of a nest
, denoted as
, was defined by the squared error
where
is the expected clustering accuracy and
is the predicted clustering accuracy for choosing the cluster size
in the UPFC. Note that each cluster was assigned one label (out of five color labels) according to a majority vote, and the cluster accuracy
could be computed by comparing the trained clusters with the pixels in the validation set. The experiment described in
Section 4.1 used 10-fold cross validation—one fold for training and the remaining folds for validation. Therefore, for
N nests, we had a set of fitness values,
. Among all nests, one nest
was randomly selected to obtain cuckoos with Lévy flights, as well as their fitness
.
A fraction
of the worst nests were discovered and abandoned according to a binary random vector whose element was
, where
for
Here, rand is a random number in the range [0, 1], and
is known as the probability of discovery. A nest was rebuilt when
; otherwise, it was kept for the next generation. This process was repeated until the minimum fitness of the best nest was less than a specified threshold value
or the number of iterations exceeded
. Finally, the optimal clusters or multiple prototypes were obtained.
| Algorithm 3. UPFC via cuckoo search algorithm. |
- 1:
Initialize N host nests, - 2:
Randomly choose the number of clusters for each nest as shown in (13) - 3:
Get the best nest and its fitness for the current best nest - 4:
while () or () do - 5:
Get cuckoos by Lévy flights using (7) to (10) - 6:
Calculate the fitness using (14) by performing UPFC on each nest. Keep the centroids - 7:
A fraction of the worst nests are abandoned, and new ones are built - 8:
Calculate the fitness using (14) by performing UPFC on each nest. Keep the centroids - 9:
if then - 10:
Replace with and keep as the new best nest - 11:
end if - 12:
end while - 13:
return the centroid of each prototype
|
3.2. Dental Fluorosis Classification
The multiple prototypes obtained as described in
Section 3.1 were used for tooth segmentation to separate teeth from gums. The severity of fluorosis was later classified based on the proportions of opaque and brown pixels in the tooth region.
To perform tooth segmentation, the pixel values of a given image were first computed against all prototypes and then assigned to one of five classes (white, yellow, opaque, brown, and background) using FKNN with
K = 1 according to (11). Since the tooth region was composed of white, yellow, opaque, and brown pixels, a binary mask of the tooth region could be created. Morphological operators, including opening and dilation, were further used to remove undesired artifacts and enhance the tooth areas. After that, in the resulting binary image, if there were pixels in the tooth area that were misclassified as the background, these pixels would be reclassified again using FKNN with
K = 5. The segmented binary mask (tooth pixel vs. background) was evaluated for its accuracy as described in
Section 4.2.
An extracted tooth region could be used to determine the severity of fluorosis based on the classes of pixel values that fell under the region. Among the four classes, white and yellow pixels are natural colors of normal teeth, so they were considered together as the class of white–yellow pixels. On the other hand, opaque and brown pixels were apparent indicators to quantify fluorosis. As a result, further image segmentation was performed only in the tooth region by considering three classes of pixels: white–yellow, opaque, and brown.
Since fluorosis could be graded by the numbers of opaque and brown pixels appearing in the tooth region, and there might still exist a few tiny areas of opaque or brown pixels after the previous image processing steps, we further processed those tiny objects by removing them if their areas were less than 0.55% of the tooth region for the opaque areas, or less than 0.05% of the tooth region for the brown areas. The resulting tooth segmentation was also evaluated as described in
Section 4.2 for pixel accuracy in predicting white–yellow, opaque, and brown pixels.
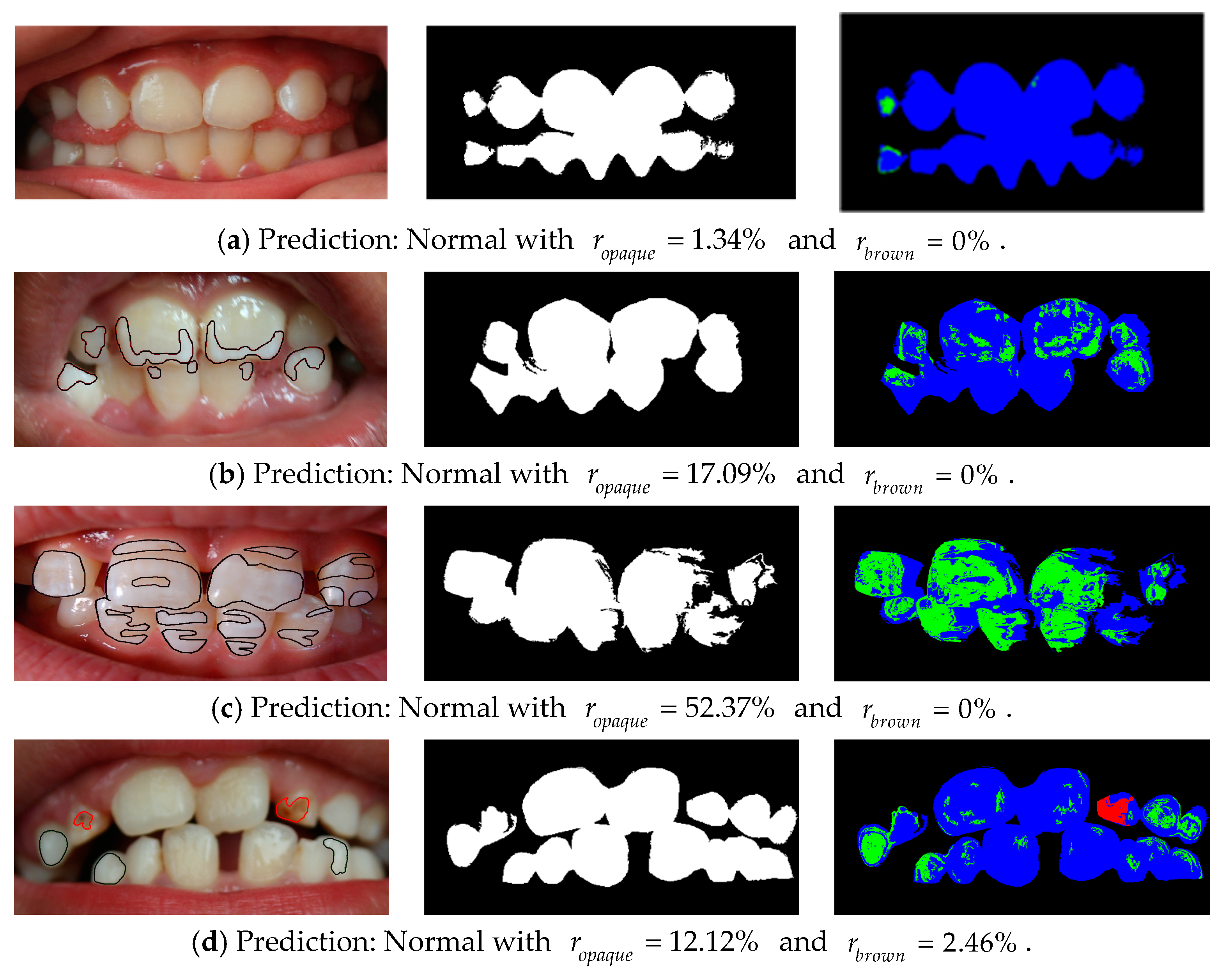
Upon completion of the image segmentation task, the numbers of white–yellow, opaque, and brown pixels in the tooth region could be determined. As a result, we designed a fluorosis classification rule (Algorithm 4) based on these quantities, where
and
are the percentages of opaque and brown pixels in the tooth area, respectively. The idea behind this rule closely followed the enamel description in
Table 1, i.e., the size of opaque and brown areas increased as fluorosis became more severe. Furthermore, Stage 2 and Stage 3 fluorosis not only involved brown pixels alone, but were also associated with a reasonably large area of opaque pixels. The choices of parameters used in this rule are discussed in
Section 3.3. Its experimental results are shown in
Section 4.3. Although this rule was motivated by Yeesarapat et al. [
14], there was one key aspect of difference, as discussed in
Section 4.4.
| Algorithm 4. Fluorosis classification rule. |
- 1:
Given and - 2:
function FluorosisClassifier(, ) - 3:
if then return Normal - 4:
else if and then return Normal - 5:
else if and then return Stage 1 - 6:
else if then return Stage 2 - 7:
else return Stage 3 - 8:
end if - 9:
end function
|
3.3. Dataset and Parameter Settings
To evaluate the performance of the proposed fluorosis classification algorithm as well as its tooth segmentation steps, we used the dataset of Yeesarapat et al. [
14], which was collected by the Intercountry Centre for Oral Health (ICOH), Ministry of Public Health, from children in the rural areas of Chiang Mai province, Thailand. The images were taken with a RICOH Caplio RX camera without any advance preparation. In the study of Yeesarapat et al., experiments were conducted with a total of 22 images, where 7 images and 15 images were assigned for the training and test sets, respectively. In this paper, we used the same 7-image training set for training the UPFC. Furthermore, an additional 113 images were added to the original 15 test set images, resulting in a blind test set of 128 images. Each collected image was taken from each child. Although the number of teeth in each image was different, according to the dentist, this does not affect the performance of the fluorosis stage detection. This is because the detection rule is set based on the treatment condition (mentioned in the Introduction section), where the ratio of the opaque or brown area to the whole teeth area is considered. In addition, this system can be used as a pre-screening system before the patient is sent to see the dentist.
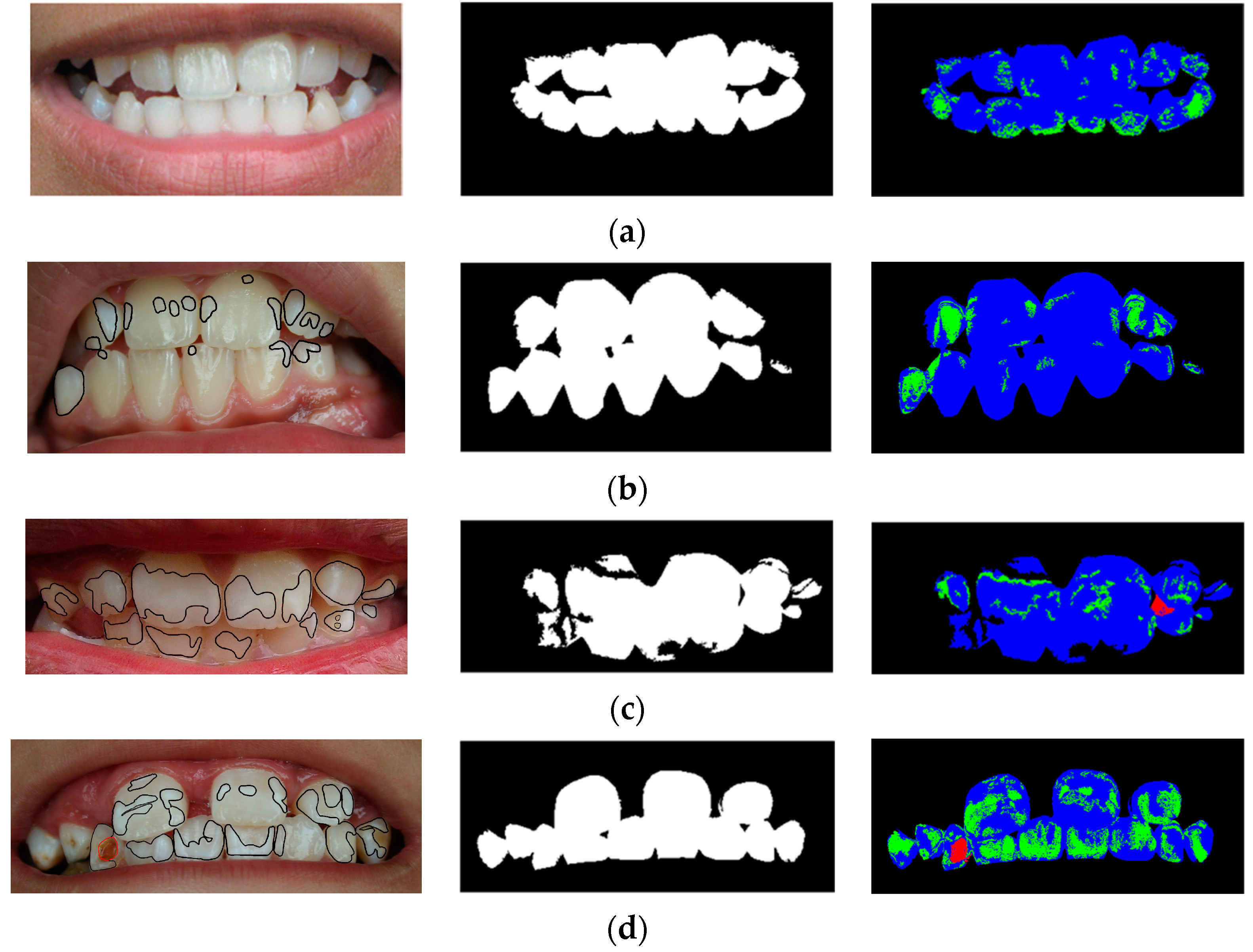
All images were cropped to the mouth region, to clearly show the teeth of each subject, where the final image sizes spanned from 815 × 517 to 1784 × 825 pixels. In addition, these collected images had varied resolutions to show that the proposed system is size- and resolution-invariant. One expert—a dentist with more than 10 years of experience—was asked to grade the severity of fluorosis in all of the images: Normal (no fluorosis), Stage 1 (questionable/mild), Stage 2 (moderate), and Stage 3 (severe). The same expert also provided five classes of pixel-level labels: white, yellow, opaque, brown, and background, where the background encompasses lips, tongues, and gums. The white class also includes reflected light spots in the images.
The parameter settings for the UPFC and cuckoo search in the experiment are shown in
Table 2. However, for the fluorosis classifier, the parameters were manually set as follows:
,
. The choice of these parameters was based on practical observations. If there was a very small number of opaque pixels (
), or a slightly larger number of opaque pixels (
) together with a very small number of brown pixels (
), the image would be graded as Normal. As the number of opaque pixels became higher, fluorosis became more severe, as seen by the values
. A large number of opaque pixels (
) but a small number of brown pixels (
) was classified as Stage 2, while the most severe level was indicated by a large number of brown pixels (
). These parameter settings were based on the treatment condition according to the experienced dentist mentioned in the Introduction section.
The performance [
39,
40] of the system in pixel-wise and fluorosis classifications was evaluated in term of true positive (TP), true negative (TN), false positive (FP), false negative (FN), true positive rate (TPR), true negative rate (TNR), false positive rate (FPR), false negative rate (FNR), positive predictive value (PPV), negative predictive value (NPV), and accuracy (Acc).
5. Conclusions
In this paper, we proposed an automatic system of dental fluorosis classification using six color features from the RGB and HSI color spaces as feature vectors. Unsupervised possibilistic fuzzy clustering (UPFC) was used to cluster these features, since each feature vector had a label in one of five classes—white, yellow, opaque, brown, or background—based on the color of that pixel and whether the pixel was in the tooth area. We applied the cuckoo search algorithm to optimize the numbers of clusters in each class. A set of pixels from seven training images, trained with these algorithms, resulted in a set of optimal prototypes, where tooth segmentation was then performed using the fuzzy k-nearest neighbor (FKNN) algorithm, together with some morphological operations. We classified the stages of fluorosis into Normal, Stage 1, Stage 2, and Stage 3, based on the proportions of opaque and brown pixels in the tooth area. Our experimental results showed that the proposed method was superior to prior works, as it correctly classified four fluorosis classes for 86 out of 128 images in the blind test set. In addition, the average pixel accuracy of the segmented binary tooth masks was 92.24%, and the average pixel accuracy of teeth segmented into white–yellow, opaque, and brown pixels was 79.46%.
In future works, it will be possible to improve the performance of the proposed method by replacing the fluorosis classification rule with a learning algorithm. Increasing the size of the training set—especially with more variations in fluorosis conditions and light conditions—would also be another way to enhance the performance. Moreover, to improve the efficiency of the system, the results need to be confirmed with clinical tests. Otherwise, the fluorosis stage detections from the system might be mistaken for other enamel hypoplasias or pigmentations due to drugs or smoking, etc. In addition, to increase the performance of the application from the point of view of a homogeneous application, we could develop a system that requires a captured image to cover the vestibular surface of at least four upper and lower incisors.
As our proposed model is lightweight, one practical direction would be to deploy our model to mobile devices and evaluate its real-world performance in both clinical and non-clinical settings.



 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}