
Socioeconomic, Behavioural, and Social Health Correlates of Optimism and Pessimism in Older Men and Women: A Cross-Sectional Study
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Optimism and Pessimism
2.3. Independent Variables
2.3.1. Participant Characteristics
2.3.2. Health-Related Behaviours
2.3.3. Socioeconomic Factors
2.3.4. Social Health
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Baseline Participant Characteristics
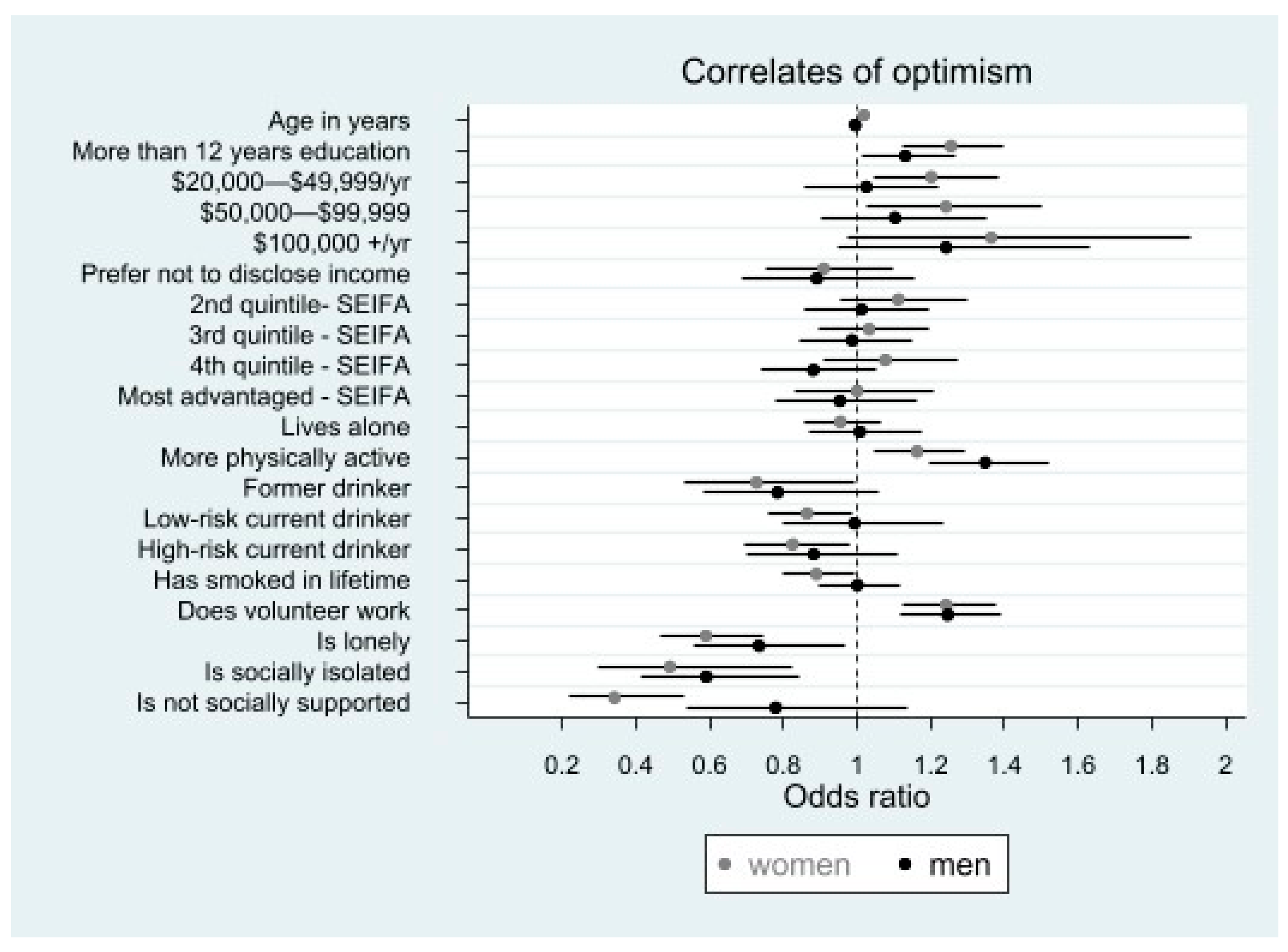
3.2. Correlates of Optimism
3.2.1. Factors Associated with Higher Optimism
3.2.2. Factors Associated with Lower Optimism
3.2.3. Gender Differences for Correlates of Optimism
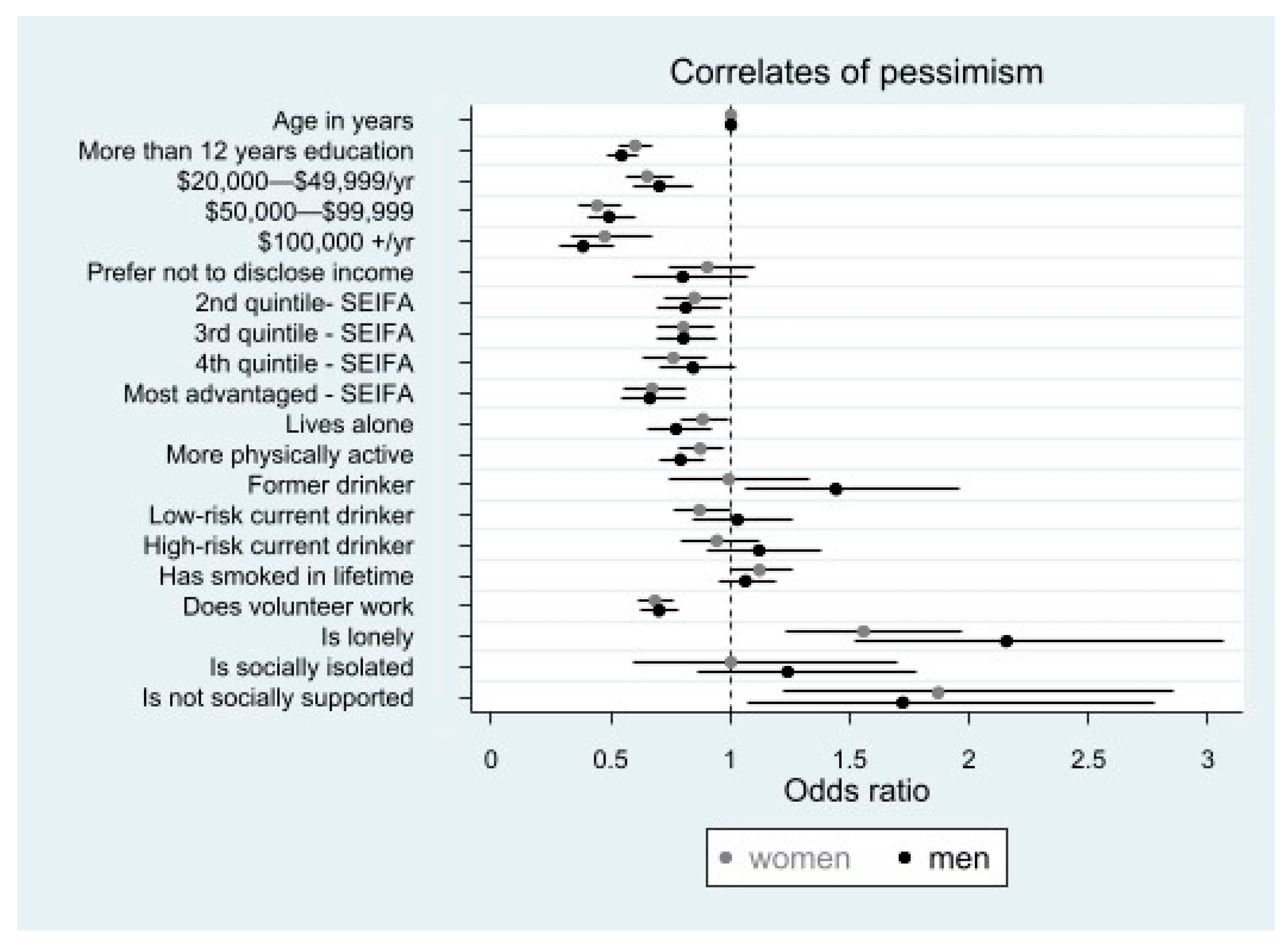
3.3. Correlates of Pessimism
3.3.1. Factors Associated with Higher Pessimism
3.3.2. Factors Associated with Lower Pessimism
3.3.3. Gender Differences for Correlates of Pessimism
4. Discussion
4.1. Socioeconomic Correlates
4.2. Behavioural Correlates
4.3. Social Health Correlates
4.4. Gender Differences
4.5. Implications
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations [UN]. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430). 2019. In Department of Economics and Social Affairs. United Nations, Population Division (Ed.). Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 21 October 2022).
- Zhao, P.; Xie, J. Aging: A Global Challenge. In Population Aging and Age-Friendly Transport in China; Springer Nature: Singapore, 2023; pp. 25–41. [Google Scholar]
- World Health Organization. Decade of Healthy Ageing. 2020. Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 21 October 2022).
- Kim, E.S.; Tkatch, R.; Martin, D.; MacLeod, S.; Sandy, L.; Yeh, C. Resilient aging: Psychological well-being and social well-being as targets for the promotion of healthy aging. Gerontol. Geriatr. Med. 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Chen, Y.; Long, K.; Kim, E.S.; Trudel-Fitzgerald, C.; Kubzansky, L.D. Positive Epidemiology? Epidemiology 2020, 31, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Health, Stress, and Coping; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- James, P.; Kim, E.S.; Kubzansky, L.D.; Zevon, E.S.; Trudel-Fitzgerald, C.; Grodstein, F. Optimism and healthy aging in women. Am. J. Prev. Med. 2019, 56, 116–124. [Google Scholar] [CrossRef]
- Scheier, M.F.; Carver, C.S. Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychol. 1985, 4, 219–247. [Google Scholar] [CrossRef] [PubMed]
- Gawronski, A.B.K.; Kim, S.E.; Langa, M.K.; Kubzansky, L.D. Dispositional optimism and incidence of cognitive impairment in older adults. Psychosom. Med. 2016, 78, 819–828. [Google Scholar] [CrossRef]
- Tindle, H.A.; Chang, Y.F.; Kuller, L.H.; Manson, J.E.; Robinson, J.G.; Rosal, M.C.; Siegle, G.J.; Matthews, K.A. Optimism, cynical hostility, and incident coronary heart disease and mortality in the Women’s Health Initiative. Circulation 2009, 120, 656–662. [Google Scholar] [CrossRef]
- Ruisoto, P.; Contador, I.; Fernández-Calvo, B.; Palenzuela, D.; Ramos, F. Exploring the association between optimism and quality of life among informal caregivers of persons with dementia. Int. Psychogeriatr. 2019, 31, 309–315. [Google Scholar] [CrossRef]
- Sherman, A.M.; Cotter, K.A. Well-being among older adults with OA: Direct and mediated patterns of control beliefs, optimism and pessimism. Aging Ment. Health 2013, 17, 595–608. [Google Scholar] [CrossRef]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Pers. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Crowson, A.D.; Colligan, R.C.; Matteson, E.L.; Davis, J.M.; Crowson, C.S. Explanatory style in patients with rheumatoid arthritis: An unrecognized predictor of mortality. J. Rheumatol. 2017, 44, 170–173. [Google Scholar] [CrossRef] [Green Version]
- Whitfield, J.B.; Zhu, G.; Landers, J.G.; Martine, N.G. Pessimism is associated with greater all-cause and cardiovascular mortality, but optimism is not protective. Sci. Rep. 2020, 10, 12609. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Schwartz, J.; Peters, J.L.; Baccarelli, A.A.; Hoxha, M.; Dioni, L.; Spiro, A.; Sparrow, D.; Vokonas, P.; Kubzansky, L.D. Pessimistic orientation in relation to telomere length in older men: The VA normative aging study. Psychoneuroendocrinology 2014, 42, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Malouff, J.M.; Schutte, N.S. Can psychological interventions increase optimism? A meta-analysis. J. Posit. Psychol. 2016, 12, 594–604. [Google Scholar] [CrossRef]
- Chopik, W.J.; Oh, J.; Kim, E.S.; Schwaba, T.; Krӓmer, M.D.; Richter, D.; Smith, J. Changes in optimism and pessimism in response to life events: Evidence from three large panel studies*. J. Res. Pers. 2020, 88, 103985. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Koenig, H.H. Does the beginning and the end of income poverty affect psychosocial factors among middle-aged and older adults? Findings based on nationally representative longitudinal data. Aging Ment. Health 2020, 25, 906–912. [Google Scholar] [CrossRef]
- Robb, K.; Simon, A.; Wardle, J. Socioeconomic disparities in optimism and pessimism. Int. J. Behav. Med. 2009, 16, 331–338. [Google Scholar] [CrossRef]
- Pavey, T.G.; Burton, N.W.; Brown, W.J. Prospective relationships between physical activity and optimism in young and mid-aged women. J. Phys. Act. Health 2015, 12, 915–923. [Google Scholar] [CrossRef]
- Steptoe, A.; Wright, C.; Kunz-Ebrecht, S.R.; Iliffe, S. Dispositional optimism and health behaviour in community dwelling older people: Associations with healthy ageing. Br. J. Health Psychol. 2006, 11, 71–84. [Google Scholar] [CrossRef]
- Mellor, D.; Hayashi, Y.; Firth, L.; Stokes, M.; Chambers, S.; Cummins, R. Volunteering and well-being: Do self-esteem, optimism, and perceived control mediate the relationship? J. Soc. Serv. Res. 2008, 34, 61–70. [Google Scholar] [CrossRef]
- Serlachius, A.; Pulkki-Råback, L.; Elovainio, M.; Hintsanen, M.; Mikkilä, V.; Laitinen, T.T.; Rosenström, T.; Josefsson, K.; Juonala, M.; Lehtimäki, T. Is dispositional optimism or dispositional pessimism predictive of ideal cardiovascular health? The Young Finns Study. Psychol. Health 2015, 30, 1221–1239. [Google Scholar] [CrossRef]
- Chopik, W.J.; Kim, E.S.; Smith, J. Changes in optimism are associated with changes in health over time among older adults. Soc. Psychol. Personal. Sci. 2015, 6, 814–822. [Google Scholar] [CrossRef]
- Koga, H.K.; Trudel-Fitzgerald, C.; Lee, L.O.; James, P.; Kroenke, C.; Garcia, L.; Shadyab, A.H.; Salmoirago-Blotcher, E.; Manson, J.E.; Grodstein, F.; et al. Optimism, lifestyle, and longevity in a racially diverse cohort of women. J. Am. Geriatr. Soc. 2022, 70, 2793–2804. [Google Scholar] [CrossRef] [PubMed]
- ASPREE Investigator Group. Study design of ASPirin in Reducing Events in the Elderly (ASPREE): A randomized, controlled trial. Contemp. Clin. Trials 2013, 36, 555–564. [Google Scholar] [CrossRef] [PubMed]
- McNeil, J.J.; Woods, R.L.; Ward, S.; Britt, C.J.; Lockery, J.E.; Beilin, L.J.; Owen, A.J. Cohort Profile: The ASPREE Longitudinal Study of Older Persons (ALSOP). Int. J. Epidemiol. 2019, 48, 1048–1049h. [Google Scholar] [CrossRef]
- McNeil, J.J.; Nelson, M.R.; Woods, R.L.; Lockery, J.E.; Wolfe, R.; Reid, C.M.; Kirpach, B.; Shah, R.C.; Ives, D.G.; Storey, E.; et al. Effect of aspirin on all-cause mortality in the healthy elderly. N. Engl. J. Med. 2018, 379, 1519–1528. [Google Scholar] [CrossRef]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E.; et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- McNeil, J.J.; Woods, R.L.; Nelson, M.R.; Reid, C.M.; Kirpach, B.; Wolfe, R.; Storey, E.; Shah, R.C.; Lockery, J.E.; Tonkin, A.M.; et al. Effect of aspirin on disability-free survival in the healthy elderly. N. Engl. J. Med. 2018, 379, 1499–1508. [Google Scholar] [CrossRef]
- Kim, E.S.; Hagan, K.A.; Grodstein, F.; DeMeo, D.L.; De Vivo, I.; Kubzansky, L.D. Optimism and cause-specific mortality: A prospective cohort study. Am. J. Epidemiol. 2017, 185, 21–29. [Google Scholar] [CrossRef]
- Scheier, M.F.; Swanson, J.D.; Barlow, M.A.; Greenhouse, J.B.; Wrosch, C.; Tindle, H.A. Optimism versus pessimism as predictors of physical health: A comprehensive reanalysis of dispositional optimism research. Am. Psychol. 2020, 76, 529–548. [Google Scholar] [CrossRef]
- Hingle, M.D.; Wertheim, B.C.; Tindle, H.A.; Tinker, L.; Seguin, R.A.; Rosal, M.C.; Thomson, C.A. Optimism and diet quality in the Women’s Health Initiative. J. Acad. Nutr. Diet. 2014, 114, 1036–1045. [Google Scholar] [CrossRef] [Green Version]
- Trudel-Fitzgerald, C.; James, P.; Kim, E.S.; Zevon, E.S.; Grodstein, F.; Kubzansky, L.D. Prospective associations of happiness and optimism with lifestyle over up to two decades. Prev. Med. 2019, 126, 105754. [Google Scholar] [CrossRef]
- National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking Alcohol. 2020. Available online: https://www.nhmrc.gov.au/health-advice/alcohol (accessed on 21 October 2022).
- Australian Bureau of Statistics (ABS) (2016) Census of Population and Housing: Socio-economic Indexes for Areas (SEIFA). Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/2033.0.55.001 (accessed on 21 October 2022).
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Arbel, R.; Segel-Karpas, D.; Chopik, W. Optimism, pessimism, and health biomarkers in older couples. Br. J. Health Psychol. 2020, 25, 1055–1073. [Google Scholar] [CrossRef]
- Hinz, A.; Sander, C.; Glaesmer, H.; Brähler, E.; Zenger, M.; Hilbert, A.; Kocalevent, R.D. Optimism and pessimism in the general population: Psychometric properties of the Life Orientation Test (LOT-R). Int. J. Clin. Health Psychol. 2017, 17, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Marbaniang, S.P.; Srivastava, S.; Kumar, P.; Chauhan, S.; Simon, D.J. Gender differential in low psychological health and low subjective well-being among older adults in India: With special focus on childless older adults. PLoS ONE 2021, 16, e0247943. [Google Scholar] [CrossRef] [PubMed]
- Curvers, N.; Pavlova, M.; Hajema, K.; Groot, W.; Angeli, F. Social participation among older adults (55+): Results of a survey in the region of South Limburg in the Netherlands. Health Soc. Care Community 2018, 26, E85–E93. [Google Scholar] [CrossRef]
- Hsu, H.C.; Liang, J.; Luh, D.L.; Chen, C.F.; Wang, Y.W. Social determinants and disparities in active aging among older Taiwanese. Int. J. Environ. Res. Public Health 2019, 16, 3005. [Google Scholar] [CrossRef]
- University of the Third Age, Victoria (U3A). Available online: https://u3avictoria.org.au (accessed on 15 January 2022).
- Loveridge, R.; Sallu, S.M.; Pesha, I.J.; RMarshall, A. Measuring human wellbeing: A protocol for selecting local indicators. Environ. Sci. Policy 2020, 114, 461–469. [Google Scholar] [CrossRef]
- Segerstrom, S.C. Optimism and resources: Effects on each other and on health over 10 years. J. Res. Pers. 2007, 41, 772–786. [Google Scholar] [CrossRef] [Green Version]
- Alghadir, A.H.; Gabr, S.A. Hormonal Function Responses to Moderate Aerobic Exercise in Older Adults with Depression. Clin. Interv. Aging 2020, 15, 1271–1283. [Google Scholar] [CrossRef] [PubMed]
- Melancon, M.O.; Lorrain, D.; Dionne, I.J. Exercise and sleep in aging: Emphasis on serotonin. Pathol. Biol. 2014, 62, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M.J. Why people smoke. BMJ 2004, 328, 277–279. [Google Scholar] [CrossRef]
- Boehm, J.K.; Chen, Y.; Koga, H.; Mathur, M.B.; Vie, L.L.; Kubzansky, L.D. Is optimism associated with healthier cardiovascular-related behavior? Meta-analyses of 3 health behaviors. Circ. Res. 2018, 122, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Rotondo, A.; Lensi, E.; Vista, O.D.; Arpone, F.; Reda, M.A. Optimism and its impact on mental and physical well-being. Clin. Pract. Epidemiol. Ment. Health 2010, 6, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Flanders, W.D.; Lin, L.; Pirkle, J.L.; Caudill, S.P. Assessing the direction of causality in cross-sectional studies. Am. J. Epidemiol. 1992, 135, 926–935. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Hu, J.; Phyo, A.Z.Z.; Barker, F. Does social isolation, social support or loneliness influence health or well-being after a cardiovascular disease event? A narrative thematic systematic review. Health Soc. Care Community 2022, 30, e16–e38. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; The National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Hu, J.; Fitzgerald, S.M.; Owen, A.J.; Ryan, J.; Joyce, J.; Chowdhury, E.; Reid, C.M.; Britt, C.; Woods, R.L.; McNeil, J.J.; et al. Social isolation, social support, loneliness and cardiovascular disease risk factors: A cross-sectional study among older adults. Int. J. Geriatr. Psychiatry 2021, 36, 1795–1809. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Ryan, J.; Tran, T.; Owen, A.; Power, J.M.; Berk, M.; Stocks, N.; Gonzalez-Chica, D.; Lowthian, J.A.; Fisher, J.; et al. Social isolation, social support and loneliness as independent concepts, and their relationship with health-related quality of life among older women. Aging Ment. Health 2022, 26, 1335–1344. [Google Scholar] [CrossRef]
- Phyo, A.Z.Z.; Gonzalez-Chica, D.A.; Stocks, N.P.; Woods, R.L.; Fisher, J.; Tran, T.; Owen, A.J.; Ward, S.A.; Britt, C.J.; Ryan, J.; et al. Impact of economic factors, social health and stressful life events on physical health-related quality of life trajectories in older Australians. Qual. Life Res. 2022, 31, 1321–1333. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Ronzi, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Freak-Poli, R.; Ryan, J.; Neumann, J.T.; Tonkin, A.; Reid, C.M.; Woods, R.L.; Nelson, M.; Stocks, N.; Berk, M.; McNeil, J.J.; et al. Social isolation, social support and loneliness as predictors of cardiovascular disease incidence and mortality. BMC Geriatr. 2021, 21, 711. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Hu, J.; Phyo, A.Z.Z.; Barker, S.F. Are social isolation, lack of social support or loneliness risk factors for cardiovascular disease in Australia and New Zealand? A systematic review and meta-analysis. Health Promot. J. Aust. 2022, 33, 278–315. [Google Scholar] [CrossRef] [PubMed]
- Freak-Poli, R.; Wagemaker, N.; Wang, R.; Lysen, T.S.; Ikram, M.A.; Vernooij, M.W.; Dintica, C.S.; Vernooij-Dassen, M.; Melis, R.J.; Laukka, E.J.; et al. Loneliness, Not Social Support, Is Associated with Cognitive Decline and Dementia Across Two Longitudinal Population-Based Cohorts. J. Alzheimer’s Dis. 2022, 85, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Joyce, J.; Ryan, J.; Owen, A.; Hu, J.; McHugh Power, J.; Shah, R.; Woods, R. Social isolation, social support, and loneliness and their relationship with cognitive health and dementia. Int. J. Geriatr. Psychiatry 2021, 37. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.C.; Yeung, D.; Kwok, S.Y. Development and evaluation of the positive psychology intervention for older adults. J. Posit. Psychol. 2014, 9, 187–197. [Google Scholar] [CrossRef]
- Report of the Annual Social Prescribing Network Conference; Wellcome Trust, & College of Medicine, University of Westminster: London, UK, 2016.
- Drinkwater, C.; Wildman, J.; Moffatt, S. Social prescribing. BMJ 2019, 364, l1285. [Google Scholar] [CrossRef]
- Htun, H.L.; Teschale, A.B.; Cumpston, M.; Demos, L.; Ryan, J.; Owen, A.; Freak-Poli, R. Effectiveness of social prescribing for chronic disease prevention in adults: A systematic review and meta-analysis of randomized controlled trials. J. Epidemiol. Community Health 2023, in press. [Google Scholar]
- Griffiths, C.; Hina, F.; Jiang, H. Social Prescribing through Primary Care: A Systematic Review of the Evidence. Open J. Prev. Med. 2022, 12, 31–58. [Google Scholar] [CrossRef]
- Pescheny, J.V.; Randhawa, G.; Pappas, Y. The impact of social prescribing services on service users: A systematic review of the evidence. Eur. J. Public Health 2019, 30, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.; Avery, L.; Scott, J.; Ashley, K.; Jordan, C.; Errington, L.; Flynn, D. Effectiveness and active ingredients of social prescribing interventions targeting mental health: A systematic review. BMJ Open 2022, 12, e060214. [Google Scholar] [CrossRef] [PubMed]
- Cousineau, L.S.; Misener, K. Volunteering as meaning-making in the transition to retirement. Can. J. Nonprofit Soc. Econ. Res. 2019, 10, 61–77. [Google Scholar] [CrossRef]
- Rius-Ottenheim, N.; Kromhout, D.; Mast, R.C.; Zitman, F.G.; Geleijnse, J.M.; Giltay, E.J. Dispositional optimism and loneliness in older men. Int. J. Geriatr. Psychiatry 2012, 27, 151–159. [Google Scholar] [CrossRef]
- Vollmann, M.; Antoniw, K.; Hartung, F.M.; Renner, B. Social support as mediator of the stress buffering effect of optimism: The importance of differentiating the recipients’ and providers’ perspective. Eur. J. Pers. 2011, 25, 146. [Google Scholar] [CrossRef]
- Hyde, J.S. Gender similarities and differences. Annu. Rev. Psychol. 2014, 65, 373–398. [Google Scholar] [CrossRef]
- Schmitt, D.P.; Long, A.E.; McPhearson, A.; O’Brien, K.; Remmert, B.; Shah, S.H. Personality and gender differences in global perspective: Gender and Personality. Int. J. Psychol. 2017, 52, 45–56. [Google Scholar] [CrossRef]
- Kim, E.S.; Fong, K.; Lee, L.; Spiro, A.; Schwartz, J.; Whitsel, E.; Horvath, S.; Wang, C.; Hou, L.; Baccarelli, A.A.; et al. Optimism is not associated with two indicators of DNA methylation aging. Aging 2019, 11, 4970–4989. [Google Scholar] [CrossRef]
- Kim, E.S.; Tindle, H.A.; Kubzansky, L.D.; Liu, S.; Duncan, M.S.; Manson, J.E.; Springfield, S.; Salmoirago-Blotcher, E.; Shadyab, A.H.; Liu, B.; et al. The Relation of Optimism to Relative Telomere Length in Older Men and Women. Psychosom. Med. 2020, 82, 165–171. [Google Scholar] [CrossRef]
- Ranzijn, R. Towards a positive psychology of ageing: Potentials and barriers. Aust. Psychol. 2002, 37, 79–85. [Google Scholar] [CrossRef]
- Rojer, A.G.M.; Ramsey, K.A.; Amaral Gomes, E.S.; D’Andrea, L.; Chen, C.; Szoeke, C.; Meskers, C.G.M.; Reijnierse, E.M.; Maier, A.B. Objectively assessed physical activity and sedentary behavior and global cognitive function in older adults: A systematic review. Mech. Ageing Dev. 2021, 198, 111524. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Galindo, D.E.; Arnáiz, E.G.; Vicente, P.F.; Ballesteros-Pomar, M.D. Effects of physical exercise in sarcopenia. A systematic review. Endocrinol. Diabetes. Nutr. (Engl. Ed.) 2021, 68, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.H.S.; Thoresen, C.E. Volunteering is associated with delayed mortality in older people: Analysis of the Longitudinal Study of Aging. J. Health Psychol. 2005, 10, 739–752. [Google Scholar] [CrossRef] [PubMed]
- Anderson, N.D.; Damianakis, T.; Kröger, E.; Wagner, L.M.; Dawson, D.R.; Binns, M.A.; Bernstein, S.; Caspi, E.; Cook, S.L. The benefits associated with volunteering among seniors: A critical review and recommendations for future research. Psychol. Bull. 2014, 140, 1505–1533. [Google Scholar] [CrossRef]
- Griffin, B.; Sherman, K.A.; Jones, M.; Bayl-Smith, P. The clustering of health behaviours in older Australians and its association with physical and psychological status, and sociodemographic indicators. Ann. Behav. Med. 2014, 48, 205–214. [Google Scholar] [CrossRef]
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2011, 61, e12–e21. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ALL: n = 10,146 | Men: n = 4874 | Women: n = 5272 | p a | |
|---|---|---|---|---|
| Optimism subscore (Mean ± SD) | 12.36 ± 2.34 | 12.25 ± 2.33 | 12.46 ± 2.34 | <0.001 |
| Pessimism subscore (Mean ± SD) | 6.58 ± 3.10 | 6.85 ± 3.07 | 6.32 ± 3.10 | <0.001 |
| Unidimensional optimism score (Mean ± SD) | 23.78 ± 4.47 | 23.39 ± 4.40 | 24.13 ± 4.50 | <0.001 |
| Age (Mean ± SD) | 74.9 ± 4.13 | 74.9 ± 4.17 | 74.9 ± 4.10 | 0.65 |
| Age group (years) n (%) | ||||
| 70–74 | 6260 (61.7) | 3034 (62.2) | 3226 (61.2) | 0.43 |
| 75–84 | 3590 (35.4) | 1694 (34.8) | 1896 (36.0) | |
| 85+ | 296 (2.92) | 146 (3.0) | 150 (2.8) | |
| Education level n (%) | ||||
| ≤12 years | 5768 (56.9) | 2618 (53.7) | 3150 (59.7) | <0.001 |
| >12 years | 4378 (43.2) | 2256 (46.3) | 2122 (40.3) | |
| Marital status n (%) | ||||
| Not married | 3633 (35.8) | 1078 (22.1) | 2555 (48.5) | <0.001 |
| Married | 6513 (64.2) | 3796 (77.9) | 2717 (51.5) | |
| Living situation n (%) | ||||
| Lives with others | 7218 (71.1) | 4080 (83.7) | 3138 (59.5) | <0.001 |
| Lives alone | 2928 (28.9) | 794 (16.3) | 2134 (40.5) | |
| SEIFA 1 n (%) | ||||
| Least advantaged | 2119 (20.9) | 1009 (20.7) | 1110 (21.1) | 0.48 |
| 2nd quintile | 2057 (20.3) | 994 (20.4) | 1063 (20.2) | |
| 3rd quintile | 2938 (29.0) | 1381 (28.3) | 1557 (29.5) | |
| 4th quintile | 1719 (16.9) | 855 (17.5) | 864 (16.4) | |
| Most advantaged | 1313 (12.9) | 635 (13.0) | 678 (12.9) | |
| Annual gross household income (AUD) n (%) | ||||
| <AUD 20,000 | 1465 (14.4) | 558 (11.4) | 907 (17.2) | <0.001 |
| AUD 20,000–49,999 | 5326 (52.5) | 2543 (52.2) | 2783 (52.8) | |
| AUD 50,000–99,999 | 1895 (18.7) | 1130 (23.2) | 765 (14.5) | |
| AUD 100,000+ | 468 (4.6) | 315 (6.5) | 153 (2.9) | |
| Prefer not to answer | 992 (9.8) | 328 (6.7) | 664 (12.6) | |
| Physical activity n (%) | ||||
| Less physically active 2 | 3386 (33.4) | 1280 (26.3) | 2106 (39.9) | <0.001 |
| More physically active 3 | 6760 (66.6) | 3594 (73.7) | 3166 (60.1) | |
| Smoking status n (%) | ||||
| Never | 5589 (55.1) | 2105 (43.2) | 3484 (66.1) | <0.001 |
| Current/former | 4557 (44.9) | 2769 (56.8) | 1788 (33.9) | |
| Alcohol intake n (%) | ||||
| Never drank alcohol | 1455 (14.3) | 398 (8.2) | 1057 (20.0) | <0.001 |
| Former drinker | 461 (4.5) | 254 (5.2) | 207 (3.9) | |
| Current—low risk 4 | 5571 (54.9) | 2495 (51.2) | 3076 (58.3) | |
| Current—high risk 5 | 2659 (26.2) | 1727 (35.4) | 932 (17.7) | |
| Volunteer work n (%) | ||||
| No | 5770 (56.9) | 2892 (59.3) | 2878 (54.6) | <0.001 |
| Yes | 4376 (43.1) | 1982 (40.7) | 2394 (45.4) | |
| Loneliness n (%) | ||||
| Not lonely | 9670 (95.3) | 4670 (95.8) | 5000 (94.8) | 0.02 |
| Lonely | 476 (4.7) | 204 (4.2) | 272 (5.2) | |
| Social isolation n (%) | ||||
| Not socially isolated | 9949 (98.1) | 4746 (97.4) | 5203 (98.7) | <0.001 |
| Socially isolated | 197 (1.9) | 128 (2.6) | 69 (1.4) | |
| Social support n (%) | ||||
| Socially supported | 9950 (98.1) | 4764 (97.7) | 5186 (98.4) | 0.02 |
| Low social support | 196 (1.9) | 110 (2.3) | 86 (1.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Craig, H.; Gasevic, D.; Ryan, J.; Owen, A.; McNeil, J.; Woods, R.; Britt, C.; Ward, S.; Freak-Poli, R. Socioeconomic, Behavioural, and Social Health Correlates of Optimism and Pessimism in Older Men and Women: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 3259. https://doi.org/10.3390/ijerph20043259
Craig H, Gasevic D, Ryan J, Owen A, McNeil J, Woods R, Britt C, Ward S, Freak-Poli R. Socioeconomic, Behavioural, and Social Health Correlates of Optimism and Pessimism in Older Men and Women: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3259. https://doi.org/10.3390/ijerph20043259
Chicago/Turabian StyleCraig, Heather, Danijela Gasevic, Joanne Ryan, Alice Owen, John McNeil, Robyn Woods, Carlene Britt, Stephanie Ward, and Rosanne Freak-Poli. 2023. "Socioeconomic, Behavioural, and Social Health Correlates of Optimism and Pessimism in Older Men and Women: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 4: 3259. https://doi.org/10.3390/ijerph20043259