
Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study
 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
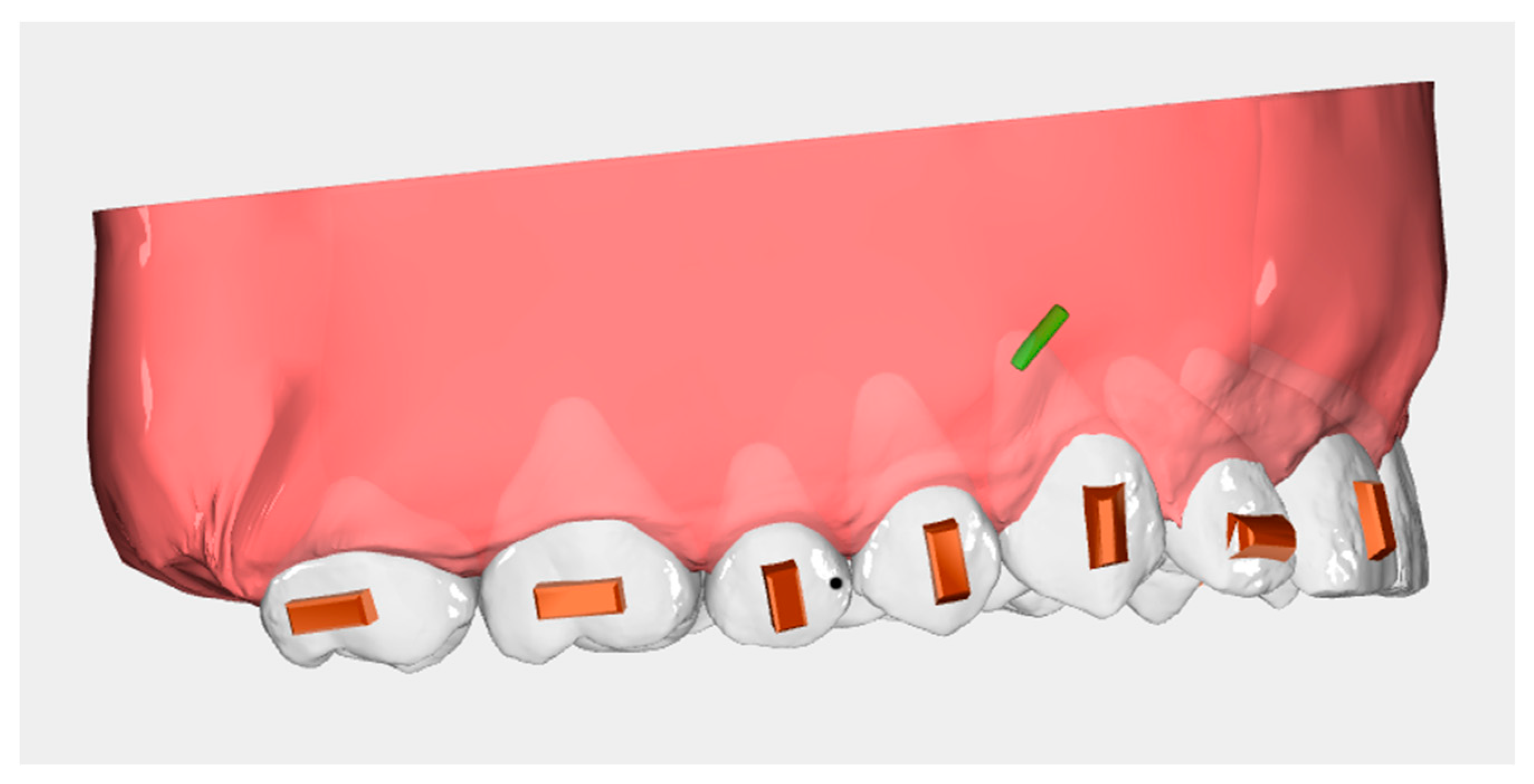
2.2. Treatment Protocol
2.3. Data Collection
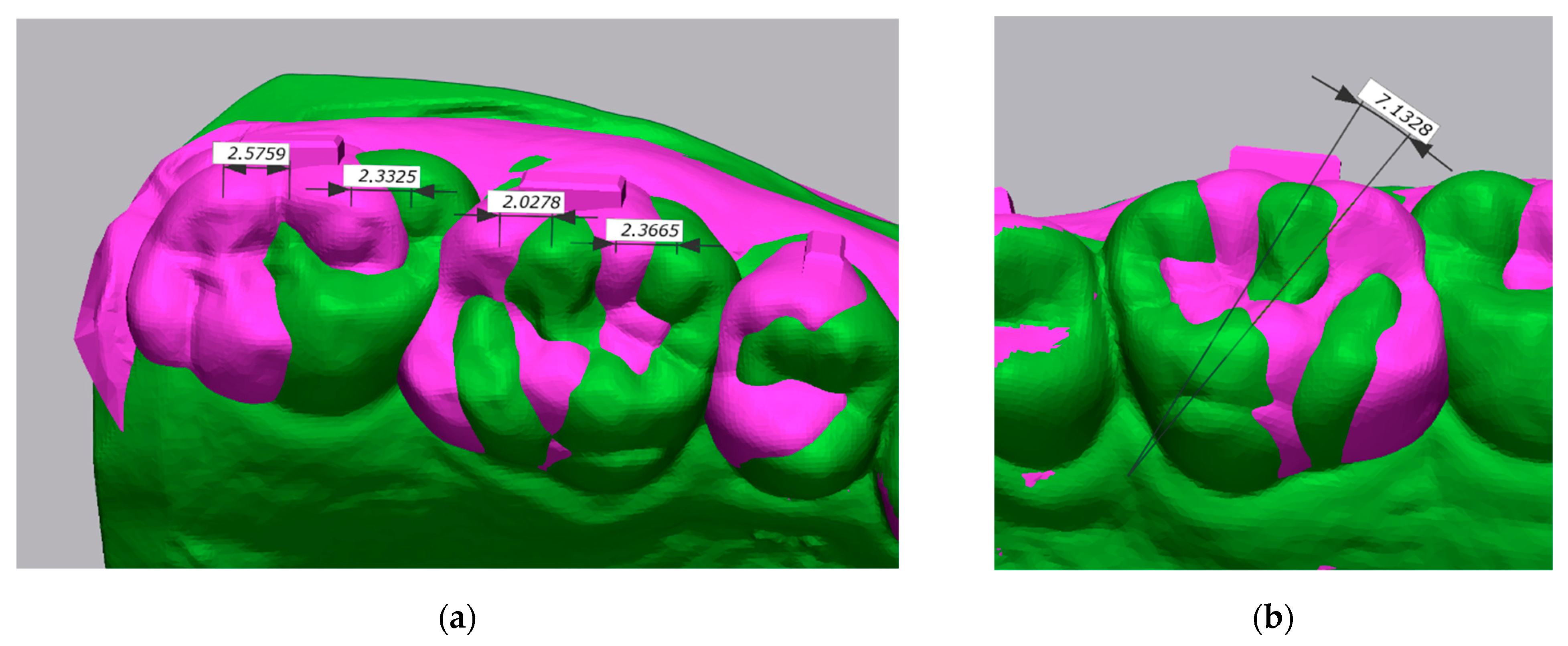
2.4. Superimposition and Measurement Protocol
2.5. Prescription, Achieved Movement, and Accuracy
- Prescription was the amount of distal displacement or derotation measured when comparing pre-treatment (T0) and virtual plan digital models (T1).
- Achieved Movement was the amount of distal displacement or derotation measured when comparing pre-treatment (T0) and post-treatment digital models (T2).
- Accuracy, expressed as percentage of achieved vs. planned, was calculated as follows:
2.6. Statistical Analysis
3. Results
3.1. Intraclass Correlation Coefficient
3.2. Prescription vs. Achieved Movement
3.3. Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fujiyama, K.; Honjo, T.; Suzuki, M.; Matsuoka, S.; Deguchi, T. Analysis of Pain Level in Cases Treated with Invisalign Aligner: Comparison with Fixed Edgewise Appliance Therapy. Prog. Orthod. 2014, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- White, D.W.; Julien, K.C.; Jacob, H.; Campbell, P.M.; Buschang, P.H. Discomfort Associated with Invisalign and Traditional Brackets: A Randomized, Prospective Trial. Angle Orthod. 2017, 87, 801–808. [Google Scholar] [CrossRef]
- Rongo, R.; Ametrano, G.; Gloria, A.; Spagnuolo, G.; Galeotti, A.; Paduano, S.; Valletta, R.; D’Antò, V. Effects of Intraoral Aging on Surface Properties of Coated Nickel-Titanium Archwires. Angle Orthod. 2014, 84, 665–672. [Google Scholar] [CrossRef]
- Pango Madariaga, A.C.; Bucci, R.; Rongo, R.; Simeon, V.; D’Antò, V.; Valletta, R. Impact of Fixed Orthodontic Appliance and Clear Aligners on the Periodontal Health: A Prospective Clinical Study. Dent. J. 2020, 8, 4. [Google Scholar] [CrossRef]
- Martina, S.; Rongo, R.; Bucci, R.; Razionale, A.V.; Valletta, R.; D’Antò, V. In Vitro Cytotoxicity of Different Thermoplastic Materials for Clear Aligners. Angle Orthod. 2019, 89, 942–945. [Google Scholar] [CrossRef]
- D’Antò, V.; Bucci, R.; de Simone, V.; Ghislanzoni, L.H.; Michelotti, A.; Rongo, R. Evaluation of Tooth Movement Accuracy with Aligners: A Prospective Study. Materials 2022, 15, 2646. [Google Scholar] [CrossRef]
- D’Antò, V.; Muraglie, S.; Castellano, B.; Candida, E.; Sfondrini, M.F.; Scribante, A.; Grippaudo, C. Influence of Dental Composite Viscosity in Attachment Reproduction: An Experimental in Vitro Study. Materials 2019, 12, 4001. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, M.; Arqub, S.A. Biomechanics of Clear Aligners: Hidden Truths & First Principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Joffe, L. Invisalign: Early Experiences. J. Orthod. 2003, 30, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, W. Force Changes Associated with Different Intrusion Strategies for Deep-Bite Correction by Clear Aligners. Angle Orthod. 2018, 88, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Boyd, R.L. Esthetic Orthodontic Treatment Using the Invisalign Appliance for Moderate to Complex Malocclusions. J. Dent. Educ. 2008, 72, 948–967. [Google Scholar] [CrossRef]
- Womack, W.R. Four-Premolar Extraction Treatment with Invisalign. J. Clin. Orthod. 2006, 40, 493–500. [Google Scholar] [PubMed]
- Staderini, E.; Meuli, S.; Gallenzi, P. Orthodontic Treatment of Class Three Malocclusion Using Clear Aligners: A Case Report. J. Oral Biol. Craniofac. Res. 2019, 9, 360–362. [Google Scholar] [CrossRef]
- D’Antò, V.; Bucci, R.; Franchi, L.; Rongo, R.; Michelotti, A.; Martina, R. Class II Functional Orthopaedic Treatment: A Systematic Review of Systematic Reviews. J. Oral Rehabil. 2015, 42, 624–642. [Google Scholar] [CrossRef]
- Rongo, R.; Bucci, R.; Adaimo, R.; Amato, M.; Martina, S.; Valletta, R.; D’anto, V. Two-Dimensional versus Three-Dimensional Fränkel Manoeuvre: A Reproducibility Study. Eur. J. Orthod. 2020, 42, 157–162. [Google Scholar] [CrossRef]
- Brandão, M.; Pinho, H.S.; Urias, D. Clinical and Quantitative Assessment of Headgear Compliance: A Pilot Study. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Hilgers, J.J. The Pendulum Appliance for Class II Non-Compliance Therapy. J. Clin. Orthod. 1992, 26, 706–714. [Google Scholar]
- Carano, A.; Testa, M. The Distal Jet for Upper Molar Distalization. J. Clin. Orthod. 1996, 30, 374–380. [Google Scholar]
- Jambi, S.; Thiruvenkatachari, B.; O’Brien, K.D.; Walsh, T. Orthodontic Treatment for Distalising Upper First Molars in Children and Adolescents. Cochrane Database Syst. Rev. 2013, 2013, CD008375. [Google Scholar] [CrossRef] [PubMed]
- Batista, K.B.; Thiruvenkatachari, B.; Harrison, J.E.; O’Brien, K.D. Orthodontic Treatment for Prominent Upper Front Teeth (Class II Malocclusion) in Children and Adolescents. Cochrane Database Syst. Rev. 2018, 3, CD003452. [Google Scholar] [CrossRef]
- Rongo, R.; Dianišková, S.; Spiezia, A.; Bucci, R.; Michelotti, A.; D’Antò, V. Class II Malocclusion in Adult Patients: What Are the Effects of the Intermaxillary Elastics with Clear Aligners? A Retrospective Single Center One-Group Longitudinal Study. J. Clin. Med. 2022, 11, 7333. [Google Scholar] [CrossRef] [PubMed]
- Dianiskova, S.; Rongo, R.; Buono, R.; Franchi, L.; Michelotti, A.; D’Antò, V. Treatment of Mild Class II Malocclusion in Growing Patients with Clear Aligners versus Fixed Multibracket Therapy: A Retrospective Study. Orthod. Craniofac. Res. 2022, 25, 96–102. [Google Scholar] [CrossRef]
- Gomez, J.P.; Peña, F.M.; Martínez, V.; Giraldo, D.C.; Cardona, C.I. Initial Force Systems during Bodily Tooth Movement with Plastic Aligners and Composite Attachments: A Three-Dimensional Finite Element Analysis. Angle Orthod. 2015, 85, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Nucera, R.; Dolci, C.; Bellocchio, A.M.; Costa, S.; Barbera, S.; Rustico, L.; Farronato, M.; Militi, A.; Portelli, M. Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review. Materials 2022, 15, 533. [Google Scholar] [CrossRef] [PubMed]
- Taffarel, I.A.; Gasparello, G.G.; Mota-Júnior, S.L.; Pithon, M.M.; Taffarel, I.P.; Meira, T.M.; Tanaka, O.M. Distalization of maxillary molars with Invisalign aligners in nonextraction patients with Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e176–e182. [Google Scholar]
- Yassir, Y.A.; Nabbat, S.A.; McIntyre, G.T.; Bearn, D.R. Clinical Effectiveness of Clear Aligner Treatment Compared to Fixed Appliance Treatment: An Overview of Systematic Reviews. Clin. Oral Investig. 2022, 26, 2353–2370. [Google Scholar] [CrossRef]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary Molar Distalization with Aligners in Adult Patients: A Multicenter Retrospective Study. Prog. Orthod. 2016, 17, 1–9. [Google Scholar] [CrossRef]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment Outcome and Efficacy of an Aligner Technique - Regarding Incisor Torque, Premolar Derotation and Molar Distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef]
- Saif, B.S.; Pan, F.; Mou, Q.; Han, M.; Bu, W.; Zhao, J.; Guan, L.; Wang, F.; Zou, R.; Zhou, H.; et al. Efficiency Evaluation of Maxillary Molar Distalization Using Invisalign Based on Palatal Rugae Registration. Am. J. Orthod. Dentofacial. Orthop. 2022, 161, e372–e379. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Kusnoto, B.; Agran, B.; Viana, G. Influence of Attachments and Interproximal Reduction on the Accuracy of Canine Rotation with Invisalign. Angle Orthod. 2008, 78, 682–687. [Google Scholar] [CrossRef]
- Galan-Lopez, L.; Barcia-Gonzalez, J.; Plasencia, E. A Systematic Review of the Accuracy and Efficiency of Dental Movements with Invisalign®. Korean J. Orthod. 2019, 49, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Forces and Moments Generated by Removable Thermoplastic Aligners: Incisor Torque, Premolar Derotation, and Molar Distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 728–736. [Google Scholar] [CrossRef]
- Kwon, J.S.; Lee, Y.K.; Lim, B.S.; Lim, Y.K. Force Delivery Properties of Thermoplastic Orthodontic Materials. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 228–234. [Google Scholar] [CrossRef]
- Bucci, R.; Rongo, R.; Levatè, C.; Michelotti, A.; Barone, S.; Razionale, A.V.; D’Antò, V. Thickness of Orthodontic Clear Aligners after Thermoforming and after 10 Days of Intraoral Exposure: A Prospective Clinical Study. Prog. Orthod. 2019, 20, 36. [Google Scholar] [CrossRef]
- Tamburrino, F.; D’Antò, V.; Bucci, R.; Alessandri-Bonetti, G.; Barone, S.; Razionale, A.V. Mechanical Properties of Thermoplastic Polymers for Aligner Manufacturing: In Vitro Study. Dent. J. 2020, 8, 47. [Google Scholar] [CrossRef]
- Rongo, R.; Alstergren, P.; Ammendola, L.; Bucci, R.; Alessio, M.; D’Anto, V.; Michelotti, A. Temporomandibular Joint Damage in Juvenile Idiopathic Arthritis: Diagnostic Validity of Diagnostic Criteria for Temporomandibular Disorders. J. Oral Rehabil. 2019, 46, 450–459. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Three-Dimensional Assessment of Morphological Changes Following Nasoalveolar Molding Therapy in Cleft Lip and Palate Patients: A Case Report. Dent. J. 2019, 7, 27. [Google Scholar] [CrossRef]
- Staderini, E.; de Luca, M.; Candida, E.; Rizzo, M.I.; Zadeh, O.R.; Bucci, D.; Zama, M.; Lajolo, C.; Cordaro, M.; Gallenzi, P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina 2019, 55, 576. [Google Scholar] [CrossRef]
- Tyrovola, J.B.; Spyropoulos, M.N. Effects of Drugs and Systemic Factors on Orthodontic Treatment. Quintessence Int. 2001, 32, 365–371. [Google Scholar]
- Ayidaga, C.; Kamiloglu, B. Effects of Variable Composite Attachment Shapes in Controlling Upper Molar Distalization with Aligners: A Nonlinear Finite Element Study. J. Healthc. Eng. 2021, 2021, 7483. [Google Scholar] [CrossRef]
- Grünheid, T.; Loh, C.; Larson, B.E. How Accurate Is Invisalign in Nonextraction Cases? Are Predicted Tooth Positions Achieved? Angle Orthod. 2017, 87, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of Clear Aligners in Controlling Orthodontic Tooth Movement: A Systematic Review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef]
- Adel, S.M.; Vaid, N.R.; El-Harouni, N.; Kassem, H.; Zaher, A.R. Digital Model Superimpositions: Are Different Software Algorithms Equally Accurate in Quantifying Linear Tooth Movements? BMC Oral Health 2022, 22, 103. [Google Scholar] [CrossRef] [PubMed]
- Stucki, S.; Gkantidis, N. Assessment of Techniques Used for Superimposition of Maxillary and Mandibular 3D Surface Models to Evaluate Tooth Movement: A Systematic Review. Eur. J. Orthod. 2020, 42, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Chen, S.; Zhang, X.Y.; Jiang, R.P.; Liu, Y.; Shi, F.H.; Xu, T.M. Stable Region for Maxillary Dental Cast Superimposition in Adults, Studied with the Aid of Stable Miniscrews. Orthod. Craniofac. Res. 2011, 14, 70–79. [Google Scholar] [CrossRef]
- Maree, A.; Kerr, B.; Weir, T.; Freer, E. Clinical Expression of Programmed Rotation and Uprighting of Bilateral Winged Maxillary Central Incisors with the Invisalign Appliance: A Retrospective Study. Am. J. Orthod. Dentofacial. Orthop. 2022, 161, 74–83. [Google Scholar] [CrossRef]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign Improved? A Prospective Follow-up Study on the Efficacy of Tooth Movement with Invisalign. Am. J. Orthod. Dentofacial. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of Molar Teeth Distalization with Clear Aligners on Occlusal Vertical Dimension: A Retrospective Study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef]
- Garino, F.; Castroflorio, T.; Daher, S.; Ravera, S.; Rossini, G.; Cugliari, G.; Deregibus, A. Effectiveness of Composite Attachments in Controlling Upper-Molar Movement with Aligners. J. Clin. Orthod. 2016, 50, 341–347. [Google Scholar]
- Rossini, G.; Schiaffino, M.; Parrini, S.; Sedran, A.; Deregibus, A.; Castroflorio, T. Upper Second Molar Distalization with Clear Aligners: A Finite Element Study. Appl. Sci. 2020, 10, 7739. [Google Scholar] [CrossRef]
- Liu, D.; Melsen, B. Reappraisal of Class II Molar Relationships Diagnosed from the Lingual Side. Clin. Orthod. Res. 2001, 4, 97–104. [Google Scholar] [CrossRef]
- Lione, R.; Paoloni, V.; de Razza, F.C.; Pavoni, C.; Cozza, P. The Efficacy and Predictability of Maxillary First Molar Derotation with Invisalign: A Prospective Clinical Study in Growing Subjects. Appl. Sci. 2022, 12, 2670. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Prescription | Achieved Movement | |AM-P| | P v AM | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cusp | n | Mean | SD | CI 95% LL | CI 95% UL | Mean | SD | CI 95% LL | CI 95% UL | Mean ± SD | p Value | |
| M1 Distalization (mm) | MB | 26 | 1.82 | 0.90 | 1.45 | 2.18 | 1.30 | 0.88 | 0.95 | 1.66 | 0.51 ± 0.56 | <0.001 |
| DB | 27 | 1.97 | 0.92 | 1.60 | 2.33 | 1.42 | 0.94 | 1.04 | 1.79 | 0.53 ± 0.60 | <0.001 * | |
| M2 Distalization (mm) | MB | 20 | 2.25 | 1.01 | 1.77 | 2.72 | 1.76 | 1.14 | 1.22 | 2.29 | 0.49 ± 0.64 | 0.0028 |
| DB | 22 | 2.13 | 1.10 | 1.64 | 2.62 | 1.54 | 1.13 | 1.03 | 2.04 | 0.60 ± 0.65 | <0.001 | |
| M1 Derotation (°) | 29 | 11.77 | 5.97 | 9.50 | 14.04 | 8.09 | 4.80 | 6.26 | 9.91 | 3.68 ± 4.67 | <0.001 | |
| M2 Derotation (°) | 26 | 11.28 | 7.03 | 8.44 | 14.12 | 6.40 | 4.14 | 4.73 | 8.07 | 4.89 ± 4.92 | <0.001 * | |
| M1 Accuracy (%) | M2 Accuracy (%) | M1 v M2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | CI 95% LL | CI 95% UL | Mean | SD | CI 95% LL | CI 95% UL | p Value | |
| Distalization/MB | 67.96 | 30.56 | 55.62 | 80.30 | 79.89 | 35.25 | 63.39 | 96.38 | >0.05 |
| Distalization/DB | 70.67 | 29.34 | 59.06 | 82.27 | 70.47 | 37.20 | 53.98 | 86.96 | >0.05 |
| Derotation (°) | 77.54 | 41.21 | 61.87 | 93.22 | 62.66 | 33.57 | 49.10 | 76.22 | >0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Antò, V.; Valletta, R.; Ferretti, R.; Bucci, R.; Kirlis, R.; Rongo, R. Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study. Int. J. Environ. Res. Public Health 2023, 20, 2941. https://doi.org/10.3390/ijerph20042941
D’Antò V, Valletta R, Ferretti R, Bucci R, Kirlis R, Rongo R. Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study. International Journal of Environmental Research and Public Health. 2023; 20(4):2941. https://doi.org/10.3390/ijerph20042941
Chicago/Turabian StyleD’Antò, Vincenzo, Rosa Valletta, Roberto Ferretti, Rosaria Bucci, Robertas Kirlis, and Roberto Rongo. 2023. "Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study" International Journal of Environmental Research and Public Health 20, no. 4: 2941. https://doi.org/10.3390/ijerph20042941