
Effects of a Multicomponent Programme for Improving Physical and Psychological Health in Victims of Intimate Partner Violence: Study Protocol for a Randomised Control Trial
 , ,
, ,  , , , ,
, , , , {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Sample Size
2.3. Randomisation and Blinding
2.4. Participants
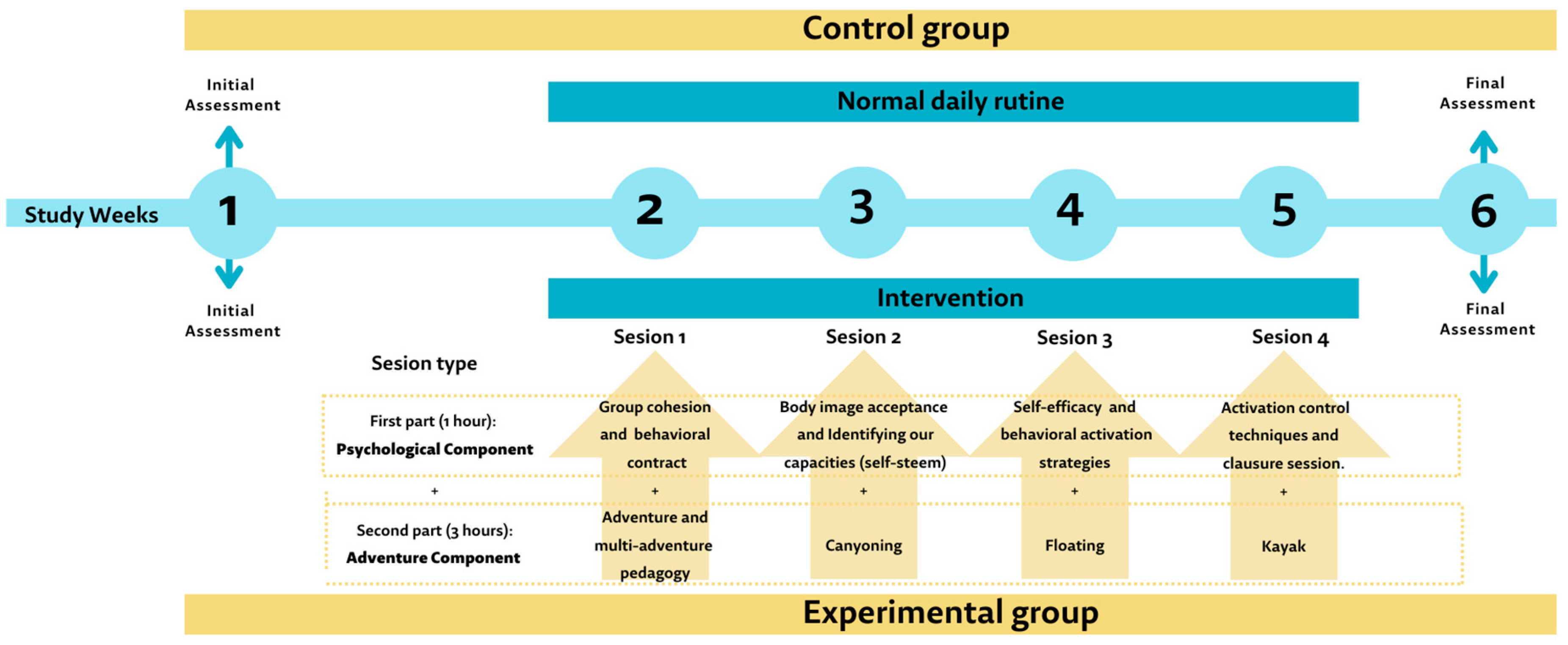
2.5. Intervention
2.6. Measures and Instruments
- -
- Brief socio-demographic data sheet: this will include questions related to age, gender, educational level and socio-economic status, etc., and gender-based violence history (questions to assess lived experiences of gender-based violence).
- -
- Baessler and Schwarzer’s General Self-Efficacy Scale [32]. It aims to assess a stable sense of personal competence to deal effectively with multiple stressful situations. This questionnaire is composed of 10 items with a 4-point Likert-type response.
- -
- Rosenberg Self-Esteem Scale [33]. The scale assesses feelings of self-respect and self-acceptance. The scale includes ten items, half of which are stated positively and half negatively. The items are answered on a 4-point Likert scale (1 = strongly agree, 2 = agree, 3 = disagree, 4 = strongly disagree), and the total score ranges from 10 to 40. Participants will complete the Spanish version adapted by Morejón, et al. [34] (α= 0.72 to 0.88).
- -
- Body Shape Questionnaire (BSQ) [35]. This questionnaire assesses the presence of concern and dissatisfaction with body image. It measures dissatisfaction with one’s own body, fear of gaining weight, low self-concept about physical appearance, and desire to lose weight. It consists of 34 items including 4 subscales (body dissatisfaction, fear of gaining weight, low esteem related to appearance, and desire to lose weight) which are measured on a 6-point scale, ranging from “never” to “always”. The total score ranges from 34 to 204, with higher scores showing greater body dissatisfaction. The Spanish validation of Raich, et al. [36], will be completed by participants (α = 0.95 to 0.97) [36].
- -
- Beck Depression Inventory, Second Edition (BDI-II) [37]. This is a questionnaire that assesses the presence and severity of depression in adolescents and adults. This consists of 21 items from different areas such as sadness, loss of pleasure, suicidal ideation, etc. Scores range from 0 to 63, including different cut-off points to classify patients according to the following subgroups: normal to minimal depression (0 to 13), mild depression (20 to 28), moderate depression (20 to 28), and severe depression (scores above 29) (α = 0.83) [38].
- -
- Perceived Stress Test (PSS) [39]. The PSS assesses the perception of control over environmental demands. It is a self-report instrument consisting of 14 items with a five-point scale response format (0 = never, 1 = hardly ever, 2 = occasionally, 3 = often, 4 = very often). A higher total score obtained is an indication of a higher level of perceived stress (α = 0.82 to 0.81) [40].
- -
- EQ-5D-5L. The EQ-5D-5L [41] is a questionnaire that aims to assess health-related quality of life (HRQoL). It is composed of 5 dimensions (mobility, self-care, usual activities, pain or discomfort, and anxiety or depression), with five possible response levels. Health states can be described by a 5-digit number, where the first number is the response to the first question, the second number is the response to the second question, and the third number is the response to the third question. is the answer to the first question, the second number is the answer to the second question, and so on. Given Since the EQ-5D is a preference-based questionnaire, these health states can be converted into a utility index by applying the appropriate formula. This instrument also includes a Visual Analogue Scale (VAS) with a range from 0 (worst imaginable health state) to 100 (best imaginable health state). (best imaginable health state).
- -
- Physiological measures will include glucocorticoids, cortisol, and dehydroepiandrosterone (DHEA) analysis through saliva samples. The participants will provide a minimum of 0.5 mL of saliva in a plastic tube recipient Salitubes SLV-4157 (DRG Instruments GmbH, Marburg, Germany) specifically to be used with DRG Salivary Cortisol/DHEA ELISA Kits (DRG Instruments GmbH, Marburg, Germany) twice a day (between 8 and 9 AM for DHEA and cortisol, and between 8 and 9 PM for evening cortisol). All samples will be triplicated to ensure process reliability. Participants will be instructed to collect samples in their homes. Saliva samples will be frozen in women’s freezers and will be brought to the Department of Anatomy of the University of Extremadura medicine Faculty in a mobile freezer, where they were being kept frozen at 21 °C previously to be analysed following the protocol indicated in the kits.
2.7. Cost-Effectiveness Analysis
2.8. Statistical Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nations, U. Transformar Nuestro Mundo: La Agenda 2030 para el Desarrollo Sostenible. Available online: https://sdgs.un.org/es/2030agenda (accessed on 20 November 2022).
- WHO. Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017.
- González, A.Á.M.; González, C.J.L.; Hernández, C.F. Revalorización del producto turístico a través del turismo de salud. In Turismo pos-COVID-19: Reflexiones, Retos y Oportunidades; Cátedra de Turismo Caja Canarias-Ashotel de la Universidad de La Laguna: Santa Cruz, Spain, 2020; pp. 545–557. [Google Scholar]
- Voigt, C.; Pforr, C. Wellness Tourism: A Destination Perspective; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Dirección General de Turismo. Extremadura Activa, Deporte y Actividades en la Naturaleza. 2020. Available online: https://issuu.com/extremadura_tur/docs/extremadura_activa (accessed on 22 November 2022).
- Andrews, G.J.; Chen, S.; Myers, S. The ‘taking place’of health and wellbeing: Towards non-representational theory. Soc. Sci. Med. 2014, 108, 210–222. [Google Scholar] [CrossRef]
- Filep, S. Consider prescribing tourism. J. Travel Med. 2014, 21, 150–152. [Google Scholar] [CrossRef]
- Moreno-González, A.-A.; León, C.J.; Fernández-Hernández, C. Health destination image: The influence of public health management and well-being conditions. J. Destin. Mark. Manag. 2020, 16, 100430. [Google Scholar] [CrossRef]
- Medina-Muñoz, D.R.; Medina-Muñoz, R.D. The attractiveness of wellness destinations: An Importance—Performance—Satisfaction approach. Int. J. Tour. Res. 2014, 16, 521–533. [Google Scholar] [CrossRef]
- United Nations. Declaration on the Elimination of Violence Against Women; UN: New York, NY, USA, 1993.
- National Center for Injury Prevention and Control. Costs of Intimate Partner Violence Against Women in the United States; Centre for Disease Control and Prevention: Atlanta, Georgia, 2003.
- WHO. Preventing Intimate Partner and Sexual Violence Against Women: Taking Action and Generating Evidence; World Health Organization: Geneva, Switzerland, 2010.
- García-Moreno, C.; Pallitto, C.; Devries, K.; Stöckl, H.; Watts, C.; Abrahams, N. Global and Regional Estimates of Violence Against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-Partner Sexual Violence; World Health Organization: Geneva, Switzerland, 2013.
- Karakurt, G.; Koç, E.; Katta, P.; Jones, N.; Bolen, S.D. Treatments for female victims of intimate partner violence: Systematic review and meta-analysis. Front. Psychol. 2022, 13, 793021. [Google Scholar] [CrossRef]
- Cirici Amell, R.; Soler, A.R.; Cobo, J.; Soldevilla Alberti, J.M. Psychological consequences and daily life adjustment for victims of intimate partner violence. Int. J. Psychiatry Med. 2022, 58, 00912174211050504. [Google Scholar] [CrossRef] [PubMed]
- Weaver, T.L.; Griffin, M.G.; Mitchell, E.R. Symptoms of posttraumatic stress, depression, and body image distress in female victims of physical and sexual assault: Exploring integrated responses. Health Care Women Int. 2014, 35, 458–475. [Google Scholar] [CrossRef] [PubMed]
- Weaver, T.L.; Resnick, H.S.; Kokoska, M.S.; Etzel, J.C. Appearance-related residual injury, posttraumatic stress, and body image: Associations within a sample of female victims of intimate partner violence. J. Trauma. Stress 2007, 20, 999–1008. [Google Scholar] [CrossRef]
- Rioli, G.; Sgarbi, C.; Moretti, V.; Sinisi, A.; De Fazio, G.L.; Giambalvo, N.; Ferrari, S.; Galeazzi, G.M. An update on intimate partner violence and mental health. Minerva Psichiatr. 2017, 58, 216–233. [Google Scholar] [CrossRef]
- Lagdon, S.; Armour, C.; Stringer, M. Adult experience of mental health outcomes as a result of intimate partner violence victimisation: A systematic review. Eur. J. Psychotraumatol. 2014, 5, 24794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seedat, S.; Stein, M.B.; Kennedy, C.; Hauger, R. Plasma cortisol and neuropeptide Y in female victims of intimate partner violence. Psychoneuroendocrinology 2003, 28, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Inslicht, S.S.; Marmar, C.R.; Neylan, T.C.; Metzler, T.J.; Hart, S.L.; Otte, C.; McCaslin, S.E.; Larkin, G.L.; Hyman, K.B.; Baum, A. Increased cortisol in women with intimate partner violence-related posttraumatic stress disorder. Psychoneuroendocrinology 2006, 31, 825–838. [Google Scholar] [CrossRef] [PubMed]
- Chaudhury, P.; Banerjee, D. “Recovering with nature”: A review of ecotherapy and implications for the COVID-19 pandemic. Front. Public Health 2020, 8, 604440. [Google Scholar] [CrossRef]
- Bowen, D.J.; Neill, J.T. A meta-analysis of adventure therapy outcomes and moderators. Open Psychol. J. 2013, 6, 28–53. [Google Scholar] [CrossRef]
- American Psychological Association, Girls and Women Guidelines Group. APA Guidelines for Psychological Practice with Girls and Women. 2018. Available online: http://www.apa.org/about/policy/psychological-practice-girls-women.pdf (accessed on 20 November 2022).
- Sáez, G.; López-Nuñez, C.; Carlos-Vivas, J.; Barrios-Fernández, S.; Rojo-Ramos, J.; Adsuar, J.C.; Collado-Mateo, D. A multicomponent program to improve self-concept and self-esteem among intimate partner violence victims: A study protocol for a randomized controlled pilot trial. Int. J. Env. Res. Public Health 2021, 18, 4930. [Google Scholar] [CrossRef]
- Reizvikh, D.D. How Women from Domestic Violence Situations Experience Informal Nature Therapy as Part of Their Trauma Healing Journey. Master’s Thesis, University of Lethbridge, Lethbridge, AB, Canada, 2012. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 2010, 1, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, J.; Kruse, M.; Gudex, C.; Helweg-Larsen, K.; Brønnum-Hansen, H. Physical violence and health-related quality of life: Danish cross-sectional analyses. Health Qual. Life Outcomes 2012, 10, 113. [Google Scholar] [CrossRef]
- Coretti, S.; Ruggeri, M.; McNamee, P. The minimum clinically important difference for EQ-5D index: A critical review. Expert Rev. Pharmacoecon. Outcomes Res. 2014, 14, 221–233. [Google Scholar] [CrossRef]
- Rosner, B. Fundamentals of Biostatistics; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0) [Computer software]. 2013. Available online: http://www.randomizer.org/ (accessed on 22 June 2013).
- Baessler, J.; Schwarzer, R. Evaluación de la autoeficacia: Adaptación española de la escala de Autoeficacia General. Ansiedad Estrés 1996, 2, 1–8. [Google Scholar]
- Rosenberg, M. Conceiving the Self; Basic Books: New York, NY, USA, 1979. [Google Scholar]
- Morejón, A.J.V.; García-Bóveda, R.J.; Jiménez, R.V.-M. Escala de autoestima de Rosenberg: Fiabilidad y validez en población clínica española. Apunt. Psicol. 2004, 22, 247–255. [Google Scholar]
- Rosen, J.C.; Jones, A.; Ramirez, E.; Waxman, S. Body Shape Questionnaire: Studies of validity and reliability. Int. J. Eat. Disord. 1996, 20, 315–319. [Google Scholar] [CrossRef]
- Raich, R.M.; Mora, M.; Soler, A.; Ávila, C.; Clos, I.; Zapater, L. Adaptación de un instrumento de evaluación de la insatisfacción corporal. Clínica Salud 1996, 7, 51–66. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sanz, J.; Vázquez, C. Fiabilidad, validez y datos normativos del Inventario para la Depresión de Beck. Psicothema 1998, 10, 303–318. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived stress scale. In Measuring Stress: A Guide for Health and Social Scientists; Oxford University Press: Oxford, UK, 1997. [Google Scholar]
- Remor, E. Psychometric properties of a European Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- López Bastida, J.; Oliva, J.; Antoñanzas, F.; García-Altés, A.; Gisbert, R.; Mar, J.; Puig-Junoy, J. Propuesta de guía para la evaluación económica aplicada a las tecnologías sanitarias. Gac. Sanit. 2010, 24, 154–170. [Google Scholar] [CrossRef]
- Sanders, G.D.; Neumann, P.J.; Basu, A.; Brock, D.W.; Feeny, D.; Krahn, M.; Kuntz, K.M.; Meltzer, D.O.; Owens, D.K.; Prosser, L.A. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: Second panel on cost-effectiveness in health and medicine. JAMA 2016, 316, 1093–1103. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Flynn, T.N.; Peters, T.J. Cluster randomized trials: Another problem for cost-effectiveness ratios. Int. J. Technol. Assess. Health Care 2005, 21, 403–409. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon, UK, 2013. [Google Scholar]
- McBride, D.; Korell, G. Terapia en el desierto para mujeres maltratadas. Rev. Can. Cons. 2005, 1, 3–14. [Google Scholar]
- Stuart, S.M. Lifting Spirits: Creating Gardens in California Domestic Violence Shelters. In Urban Place: Reconnecting with the Natural World; Barlett, P.F., Ed.; MIT Press: Cambridge, MA, USA, 2005; pp. 61–68. [Google Scholar]
- Wicks, C.; Barton, J.; Orbell, S.; Andrews, L. Psychological benefits of outdoor physical activity in natural versus urban environments: A systematic review and meta-analysis of experimental studies. Appl. Psychol. Health Well Being 2022, 14, 1037–1061. [Google Scholar] [CrossRef]
- Fernandez, M.P.; Ernst, K.C.; Bron, G.M.; Berry, K.; Diuk-Wasser, M.A.; Hayden, M.H. Outdoor Activity Associated with Higher Self-Reported Emotional Well-Being During COVID-19. EcoHealth 2022, 19, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhang, X.; Bi, S.; Cao, Y.; Zhang, G. Psychological benefits of green exercise in wild or urban greenspaces: A meta-analysis of controlled trials. Urban For. Urban Green. 2022, 68, 127458. [Google Scholar] [CrossRef]
- Boyadjiev, N.; Georgieva, K.N.; Hristova, P.A.A. Outdoor Recreation: Physiological Effects and Prevention of Socially Important Diseases. In Outdoor Recreation-Physiological and Psychological Effects on Health; IntechOpen: London, UK, 2020. [Google Scholar]
- Hameed, M.; O’Doherty, L.; Gilchrist, G.; Tirado-Muñoz, J.; Taft, A.; Chondros, P.; Feder, G.; Tan, M.; Hegarty, K. Psychological therapies for women who experience intimate partner violence. Cochrane Database Syst. Rev. 2020, 7, CD013017. [Google Scholar] [PubMed]
- Paphitis, S.A.; Bentley, A.; Asher, L.; Osrin, D.; Oram, S. Improving the mental health of women intimate partner violence survivors: Findings from a realist review of psychosocial interventions. PLoS ONE 2022, 17, e0264845. [Google Scholar] [CrossRef] [PubMed]
- Varning Poulsen, D.; Lygum, V.L.; Djernis, H.G.; Stigsdotter, U.K. Nature is just around us! Development of an educational program for implementation of nature-based activities at a crisis shelter for women and children exposed to domestic violence. J. Soc. Work. Pract. 2021, 35, 159–175. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calle-Guisado, V.; Adsuar, J.C.; Barrios-Fernandez, S.; Mendoza-Muñoz, M.; Muñoz-Bermejo, L.; Domínguez-Muñoz, F.J.; Ortiz-González, L.; Rojo-Ramos, J. Effects of a Multicomponent Programme for Improving Physical and Psychological Health in Victims of Intimate Partner Violence: Study Protocol for a Randomised Control Trial. Int. J. Environ. Res. Public Health 2023, 20, 2815. https://doi.org/10.3390/ijerph20042815
Calle-Guisado V, Adsuar JC, Barrios-Fernandez S, Mendoza-Muñoz M, Muñoz-Bermejo L, Domínguez-Muñoz FJ, Ortiz-González L, Rojo-Ramos J. Effects of a Multicomponent Programme for Improving Physical and Psychological Health in Victims of Intimate Partner Violence: Study Protocol for a Randomised Control Trial. International Journal of Environmental Research and Public Health. 2023; 20(4):2815. https://doi.org/10.3390/ijerph20042815
Chicago/Turabian StyleCalle-Guisado, Violeta, Jose Carmelo Adsuar, Sabina Barrios-Fernandez, María Mendoza-Muñoz, Laura Muñoz-Bermejo, Francisco Javier Domínguez-Muñoz, Luis Ortiz-González, and Jorge Rojo-Ramos. 2023. "Effects of a Multicomponent Programme for Improving Physical and Psychological Health in Victims of Intimate Partner Violence: Study Protocol for a Randomised Control Trial" International Journal of Environmental Research and Public Health 20, no. 4: 2815. https://doi.org/10.3390/ijerph20042815