
Establishing Self-Harm Registers: The Role of Process Mapping to Improve Quality of Surveillance Data Globally
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. SHR Inclusion Criteria
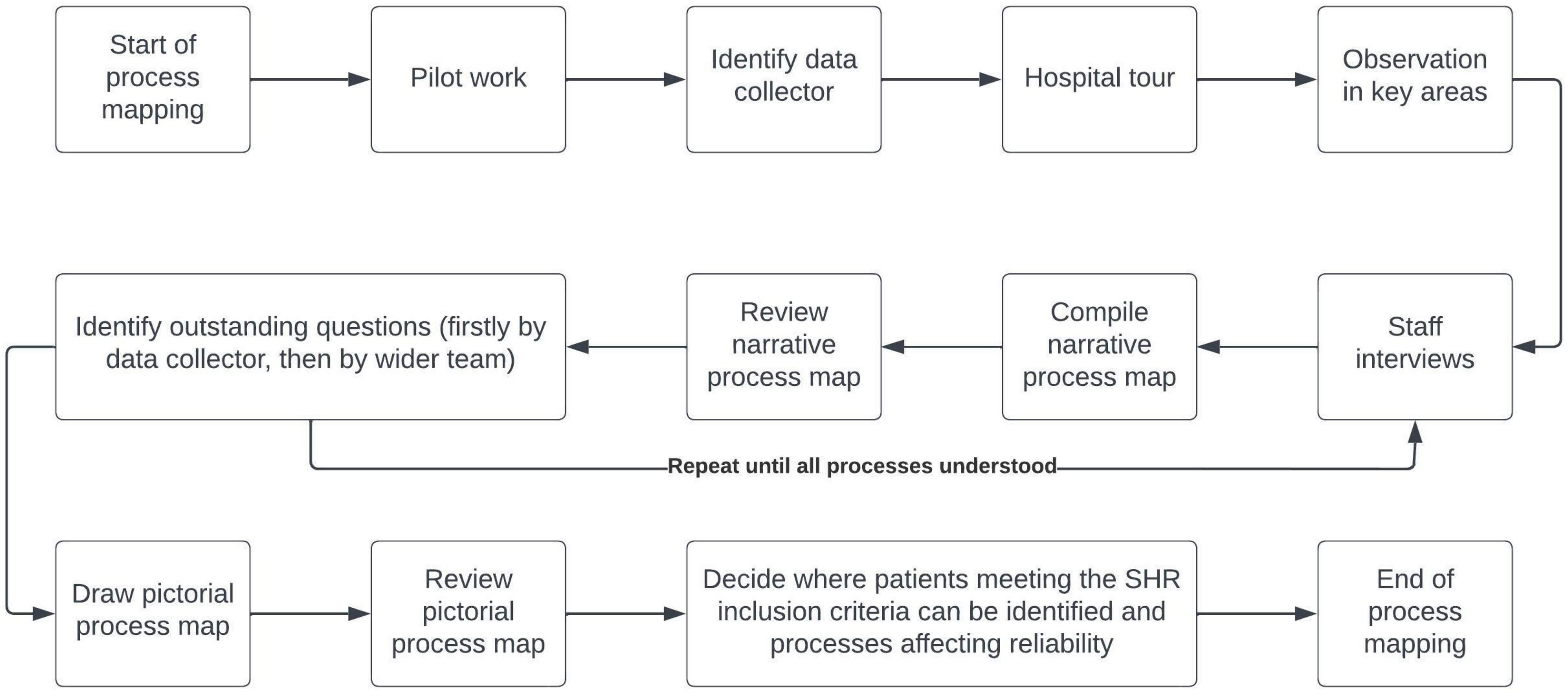
2.3. Approach
2.4. Pilot Work
2.5. Data Collection
2.6. Data Analysis
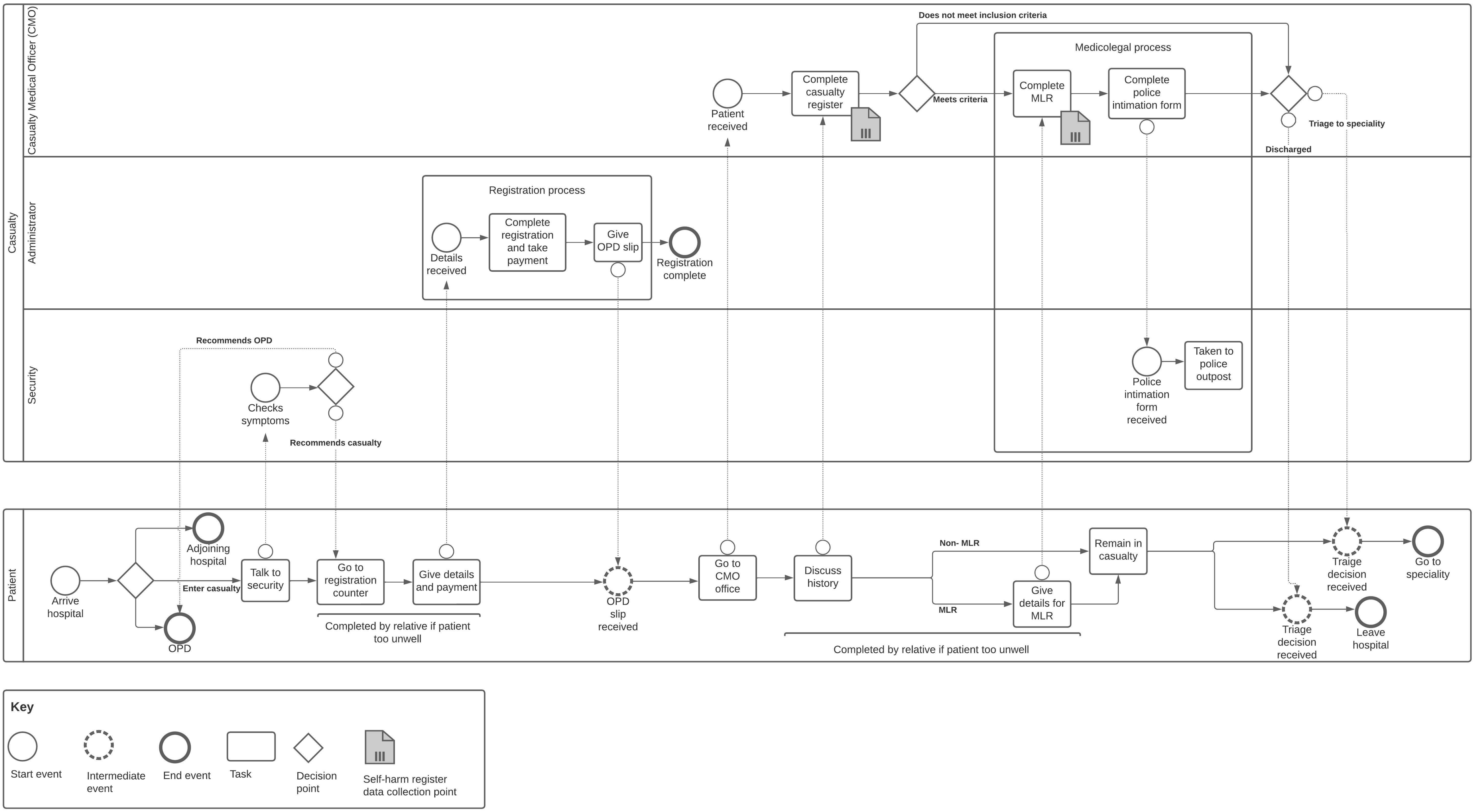
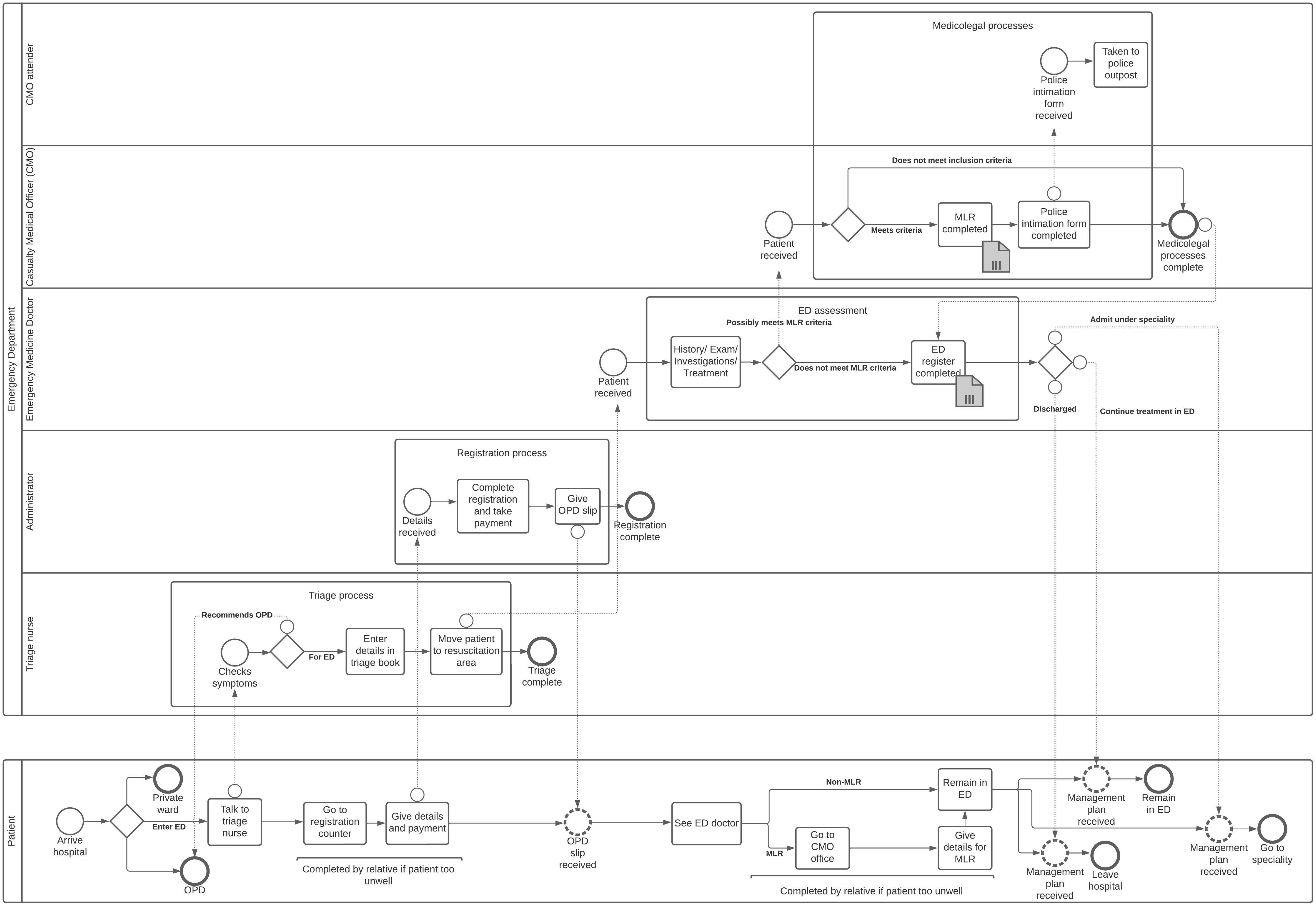
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Preventing Suicide: A Global Imperative; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organisation. Practice Manual for Establishing and Maintaining Surveillance Systems for Suicide Attempts and Self-Harm; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- National Institute for Health and Care Excellence. Self-Harm: What Is It? Available online: https://cks.nice.org.uk/topics/self-harm/background-information/definition/ (accessed on 1 November 2022).
- Hawton, K.; Bale, L.; Casey, D.; Shepherd, A.; Simkin, S.; Harriss, L. Monitoring deliberate self-harm presentations to general hospitals. Crisis 2006, 27, 157–163. [Google Scholar] [CrossRef]
- Hawton, K.; Townsend, E.; Deeks, J.; Appleby, L.; Gunnell, D.; Bennewith, O.; Cooper, J. Effects of legislation restricting pack sizes of paracetamol and salicylate on self poisoning in the United Kingdom: Before and after study. BMJ 2001, 322, 1203. [Google Scholar] [CrossRef]
- Pearson, M.; Metcalfe, C.; Jayamanne, S.; Gunnell, D.; Weerasinghe, M.; Pieris, R.; Priyadarshana, C.; Knipe, D.W.; Hawton, K.; Dawson, A.H.; et al. Effectiveness of household lockable pesticide storage to reduce pesticide self-poisoning in rural Asia: A community-based, cluster-randomised controlled trial. Lancet 2017, 390, 1863–1872. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 5 January 2023).
- The World Bank. Total Population—India. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=IN (accessed on 1 November 2022).
- World Health Organisation. Suicide in the World: Global Health Estimates; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Global SDG Indicator Platform. 3.4.2 Number of Deaths Attributed to Suicide. Available online: https://sdg.tracking-progress.org/indicator/3-4-1-number-of-deaths-attributed-to-suicide/ (accessed on 5 January 2023).
- Hawton, K.; Zahl, D.; Weatherall, R. Suicide following deliberate self-harm: Long-term follow-up of patients who presented to a general hospital. Br. J. Psychiatry 2003, 182, 537–542. [Google Scholar] [CrossRef]
- Geulayov, G.; Casey, D.; Bale, L.; Brand, F.; Clements, C.; Farooq, B.; Kapur, N.; Ness, J.; Waters, K.; Tsiachristas, A.; et al. Suicide following presentation to hospital for non-fatal self-harm in the Multicentre Study of Self-harm: A long-term follow-up study. Lancet Psychiatry 2019, 6, 1021–1030. [Google Scholar] [CrossRef]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: Systematic review and meta-analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef]
- Knipe, D.; Metcalfe, C.; Hawton, K.; Pearson, M.; Dawson, A.; Jayamanne, S.; Konradsen, F.; Eddleston, M.; Gunnell, D. Risk of suicide and repeat self-harm after hospital attendance for non-fatal self-harm in Sri Lanka: A cohort study. Lancet Psychiatry 2019, 6, 659–666. [Google Scholar] [CrossRef]
- Tsiachristas, A.; McDaid, D.; Casey, D.; Brand, F.; Leal, J.; Park, A.L.; Geulayov, G.; Hawton, K. General hospital costs in England of medical and psychiatric care for patients who self-harm: A retrospective analysis. Lancet Psychiatry 2017, 4, 759–767. [Google Scholar] [CrossRef]
- McDaid, D.; Tsiachristas, A.; Hawton, K. Understanding the true economic impact of self-harming behaviour—Authors’ reply. Lancet Psychiatry 2017, 4, 901. [Google Scholar] [CrossRef]
- Kinchin, I.; Doran, C.M.; Hall, W.D.; Meurk, C. Understanding the true economic impact of self-harming behaviour. Lancet Psychiatry 2017, 4, 900–901. [Google Scholar] [CrossRef] [Green Version]
- Witt, K.; Robinson, J. Sentinel surveillance for self-harm. Crisis 2019, 40, 1–6. [Google Scholar] [CrossRef]
- Rybarczyk, M.M.; Ludmer, N.; Broccoli, M.C.; Kivlehan, S.M.; Niescierenko, M.; Bisanzo, M.; Checkett, K.A.; Rouhani, S.A.; Tenner, A.G.; Geduld, H.; et al. Emergency Medicine Training Programs in Low- and Middle-Income Countries: A Systematic Review. Ann. Glob. Health 2020, 86, 60. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Abujaber, S.; Makar, M.; Stoll, S.; Kayden, S.R.; Wallis, L.A.; Reynolds, T.A.; Acute Care Development Consortium. Emergency care in 59 low- and middle-income countries: A systematic review. Bull. World Health Organ. 2015, 93, 577G–586G. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Witt, K.; Lamblin, M.; Spittal, M.J.; Carter, G.; Verspoor, K.; Page, A.; Rajaram, G.; Rozova, V.; Hill, N.T.M.; et al. Development of a Self-Harm Monitoring System for Victoria. Int. J. Environ. Res. Public Health 2020, 17, 9385. [Google Scholar] [CrossRef]
- Kuramoto-Crawford, S.J.; Spies, E.L.; Davies-Cole, J. Detecting Suicide-Related Emergency Department Visits Among Adults Using the District of Columbia Syndromic Surveillance System. Public Health Rep. 2017, 132, 88S–94S. [Google Scholar] [CrossRef]
- Hansen, K.; Boyle, A.; Holroyd, B.; Phillips, G.; Benger, J.; Chartier, L.B.; Lecky, F.; Vaillancourt, S.; Cameron, P.; Waligora, G.; et al. Updated framework on quality and safety in emergency medicine. Emerg. Med. J. 2020, 37, 437–442. [Google Scholar] [CrossRef]
- Clements, C.; Turnbull, P.; Hawton, K.; Geulayov, G.; Waters, K.; Ness, J.; Townsend, E.; Khundakar, K.; Kapur, N. Rates of self-harm presenting to general hospitals: A comparison of data from the Multicentre Study of Self-Harm in England and Hospital Episode Statistics. BMJ Open 2016, 6, e009749. [Google Scholar] [CrossRef]
- Sakr, M.; Wardrope, J. Casualty, accident and emergency, or emergency medicine, the evolution. Emerg. Med. J. 2000, 17, 314. [Google Scholar] [CrossRef]
- Rajendra, R.; Krishna, M.; Majgi, S.; Heggere, N.; Robinson, C.; Poole, R. A feasibility study to establish a Deliberate Self-harm Register in a state hospital in southern India. Br. J. Med. Pract. 2015, 8, a807. [Google Scholar]
- Daruwalla, N.; Belur, J.; Kumar, M.; Tiwari, V.; Sarabahi, S.; Tilley, N.; Osrin, D. A qualitative study of the background and in-hospital medicolegal response to female burn injuries in India. BMC Womens Health 2014, 14, 142. [Google Scholar] [CrossRef]
- Peck, M.D. Epidemiology of burns throughout the World. Part II: Intentional burns in adults. Burns 2012, 38, 630–637. [Google Scholar] [CrossRef]
- Antonacci, G.; Reed, J.E.; Lennox, L.; Barlow, J. The use of process mapping in healthcare quality improvement projects. Health Serv. Manag. Res. 2018, 31, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Antonacci, G.; Lennox, L.; Barlow, J.; Evans, L.; Reed, J. Process Mapping in Healthcare: A Systematic Review. BMC Health Serv. Res. 2020, 21, 342. [Google Scholar] [CrossRef]
- NHS Institute of Innovation and Improvement. Process Mapping, Analysis and Redesign; NHS Institute of Innovation and Improvement: London, UK, 2005.
- NHS England and NHS Improvement. Online Library of Quality, Service Improvement and Redesign Tools: Conventional Process Mapping; NHS Institute of Innovation and Improvement: London, UK.
- Graham, B. The Roots of the Business Process Mapping; BPTrends: Newton, MA, USA, 2008. [Google Scholar]
- Gilbreth, F.; Gilbreth, L.M. Process Charts. In Proceedings of the Annual Meeting of The American Society of Mechanical Engineers, New York, NY, USA, 5–9 December 1921. [Google Scholar]
- de Savigny, D.; Cobos Muñoz, D. Understanding CRVS Systems: The Importance of Process Mapping. CRVS Best-Practice and Advocacy; Bloomberg Philanthropies, Data for Health Initiative, Civil Registration and Vital Statistics Improvement, The University of Melbourne: Melbourne, Australia, 2018. [Google Scholar]
- Trebble, T.M.; Hansi, N.; Hydes, T.; Smith, M.A.; Baker, M. Process mapping the patient journey: An introduction. BMJ 2010, 341, c4078. [Google Scholar] [CrossRef]
- Jester, B.; Schwerzmann, J.; Mustaquim, D.; Aden, T.; Brammer, L.; Humes, R.; Shult, P.; Shahangian, S.; Gubareva, L.; Xu, X.; et al. Mapping of the US Domestic Influenza Virologic Surveillance Landscape. Emerg. Infect. Dis. 2018, 24, 1300–1306. [Google Scholar] [CrossRef]
- Bhartia, S.; Wahi, P.; Goyal, R. Reducing delay in laboratory reports for outpatients from 16% to <3% at a non-profit hospital in New Delhi, India. BMJ Open Qual. 2019, 8, e000547. [Google Scholar] [CrossRef]
- Durski, K.N.; Naidoo, D.; Singaravelu, S.; Shah, A.A.; Djingarey, M.H.; Formenty, P.; Ihekweazu, C.; Banjura, J.; Kebela, B.; Yinka-Ogunleye, A.; et al. Systems thinking for health emergencies: Use of process mapping during outbreak response. BMJ Glob. Health 2020, 5, e003901. [Google Scholar] [CrossRef]
- Frew, G.H.; Abraham, I.; Lancaster, D.; Drake, P.J.H.; Cassell, J.A. Evaluating the patient experience of an emergency burns assessment service in a UK burn unit using a service user evaluation questionnaire and process mapping. Burns 2020, 46, 1066–1072. [Google Scholar] [CrossRef]
- LaMonica, H.M.; Davenport, T.A.; Ottavio, A.; Rowe, S.C.; Cross, S.P.; Iorfino, F.; Jackson, T.A.; Easton, M.A.; Melsness, J.; Hickie, I.B. Optimising the integration of technology-enabled solutions to enhance primary mental health care: A service mapping study. BMC Health Serv. Res. 2021, 21, 68. [Google Scholar] [CrossRef]
- Holleran, L.; Baker, S.; Cheng, C.; Wilson, J.; Mickelson, R.; Kazana, I.; Messinger-Rapport, B.; Shahin, J.; Cully, J.; Naik, A.D.; et al. Using Multisite Process Mapping to Aid Care Improvement: An Examination of Inpatient Suicide-Screening Procedures. J. Healthc. Qual. Off. Publ. Natl. Assoc. Healthc. Qual. 2019, 41, 110–117. [Google Scholar] [CrossRef]
- Ward, J.; Bailey, D. A participatory action research methodology in the management of self-harm in prison. J. Ment. Health 2013, 22, 306–316. [Google Scholar] [CrossRef]
- Cobos Muñoz, D.; de Savigny, D.; Sorchik, R.; Bo, K.S.; Hart, J.; Kwa, V.; Ngomituje, X.; Richards, N.; Lopez, A.D. Better data for better outcomes: The importance of process mapping and management in CRVS systems. BMC Med. 2020, 18, 67. [Google Scholar] [CrossRef] [PubMed]
- National Statistics Office Government of India. Health in India, National Sample Survey 75th Round; National Statistics Office Government of India: New Delhi, India, 2020.
- Lucidchart. Diagram Your People, Processes, and Systems. Available online: www.lucidchart.com/pages/product (accessed on 1 November 2022).
- Object Management Group. Business Process Model And Notation. Available online: https://www.omg.org/spec/BPMN (accessed on 1 November 2022).
- Meera, T. Medicolegal cases: What every doctor should know. J. Med. Soc. 2016, 30, 133–134. [Google Scholar] [CrossRef]
- Vadlamani, L.N.; Gowda, M. Practical implications of Mental Healthcare Act 2017: Suicide and suicide attempt. Indian J. Psychiatry 2019, 61, S750–S755. [Google Scholar] [CrossRef]
- Nowacki, A.K.; Landes, M.; Azazh, A.; Ritchie, L.M.P. A review of published literature on emergency medicine training programs in low- and middle-income countries. Int. J. Emerg. Med. 2013, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Mowafi, H.; Ngaruiya, C.; Reilly, G.; Kobusingye, O.; Kapil, V.; Rubiano, A.M.; Ong, M.; Puyana, J.C.; Rahman, A.K.M.F.; Jooma, R.; et al. Emergency care surveillance and emergency care registries in low-income and middle-income countries: Conceptual challenges and future directions for research. BMJ Glob. Health 2019, 4, e001442. [Google Scholar] [CrossRef]
- Bertolote, J.M.; Fleischmann, A.; De Leo, D.; Phillips, M.R.; Botega, N.J.; Vijayakumar, L.; De Silva, D.; Schlebusch, L.; Nguyen, V.T.; Sisask, M.; et al. Repetition of suicide attempts: Data from emergency care settings in five culturally different low- and middle-income countries participating in the WHO SUPRE-MISS study. Crisis J. Crisis Interv. Suicide Prev. 2010, 31, 194–201. [Google Scholar] [CrossRef]
- Vats, D.R.K. Public Notice—Amendment to Minimum Requirements for Annual MBBS Admissions 50/100/150/200/250 Regulations, 1999 to Include Department of Emergency Medicine; National Medical Commission: New Delhi, India, 2020. [Google Scholar]
- Hawton, K.; Simkin, S.; Deeks, J. Co-proxamol and suicide: A study of national mortality statistics and local non-fatal self poisonings. BMJ 2003, 326, 1006. [Google Scholar] [CrossRef]
- Lee, P.; Chin, K.; Liew, D.; Stub, D.; Brennan, A.L.; Lefkovits, J.; Zomer, E. Economic evaluation of clinical quality registries: A systematic review. BMJ Open 2019, 9, e030984. [Google Scholar] [CrossRef]
- The Australian Commission on Safety and Quality in Health Care. Economic Evaluation of Clinical Quality Registries: Final Report; The Australian Commission on Safety and Quality in Health Care: Canberra, Australia, 2016. [Google Scholar]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How We Design Feasibility Studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| SASHI Self-Harm Register Inclusion Criteria |
|---|
| Poisoning (medication and non-medication) |
| Burn injury |
| Hanging |
| Drowning |
| Fall from height |
| Fall in front of train |
| Self-laceration |
| Firearm injury |
| Unspecified self-harm |
| Topic | Specific Details Addressed in Tours and Interviews |
|---|---|
| Overview | Type of hospital, funding, size and specialities. |
| Other types of healthcare provision available locally. | |
| Patient arrival | Referral options (e.g., from other hospitals, primary care). |
| Means of arrival (e.g., walk, ambulance), method of ascertaining that means (e.g., national telephone number) and associated costs. | |
| Point of arrival | Departments providing emergency care at the hospital (e.g., casualty, emergency department, outpatient department). |
| Method by which patients are directed to the appropriate department. | |
| Main emergency care area | Consensus on the department responsible for providing immediate emergency care to newly presenting patients (e.g., casualty, emergency department). |
| Triage processes for new patients. | |
| Patient registration and payment procedures. | |
| Inclusion criteria for any routinely collected registers. | |
| Areas of the department where patients may be treated. | |
| Management in the main emergency care area | Clinician responsibilities and training. |
| Whether there are any medicolegal processes. | |
| Medicolegal processes (if applicable) | Clinician responsible for completing medicolegal processes (e.g., casualty medical officer). |
| Patient groups requiring medicolegal processing. | |
| Paperwork completed for each patient (e.g., medicolegal register). | |
| Inclusion criteria for any routinely collected registers, and details entered into these registers. | |
| Clinician discretion for medicolegal processing. | |
| Police involvement in medicolegal processes in hospital. | |
| Length of time records kept. | |
| Payment processes. | |
| Disposition from main emergency care area | Main area or specialities where patients who meet the self-harm register inclusion criteria go (if applicable). |
| Inpatient admission registration and payment. | |
| Alternative means by which patients can access emergency care (e.g., outpatient department, nearby hospitals, private ward) | Method by which patients access these services. |
| Handling of medicolegal processes. | |
| Patient groups (e.g., priority, injury type) that could present to these areas or the main emergency care area. | |
| Methods by which patients can be admitted to these areas directly and bypass normal administrative routes. |
| Number of Patients | |||
|---|---|---|---|
| 2019 | 2020 | 2021 | |
| Government hospital (KR Hospital) | |||
| Outpatients (including casualty and outpatient department) | 476,012 | 297,682 | 329,978 |
| Medicolegal cases | 24,404 | 17,969 | 24,029 |
| Non-profit hospital (JSS Hospital) | |||
| Outpatients (including casualty and outpatient department) | 664,650 | 376,870 | 415,034 |
| Emergency department | 29,330 | 23,204 | 19,153 |
| Outpatient department | 635,320 | 353,666 | 395,881 |
| Medicolegal cases | 3969 | 2917 | 3021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bebbington, E.; Poole, R.; Kumar, S.P.; Krayer, A.; Krishna, M.; Taylor, P.; Hawton, K.; Raman, R.; Kakola, M.; Srinivasarangan, M.; et al. Establishing Self-Harm Registers: The Role of Process Mapping to Improve Quality of Surveillance Data Globally. Int. J. Environ. Res. Public Health 2023, 20, 2647. https://doi.org/10.3390/ijerph20032647
Bebbington E, Poole R, Kumar SP, Krayer A, Krishna M, Taylor P, Hawton K, Raman R, Kakola M, Srinivasarangan M, et al. Establishing Self-Harm Registers: The Role of Process Mapping to Improve Quality of Surveillance Data Globally. International Journal of Environmental Research and Public Health. 2023; 20(3):2647. https://doi.org/10.3390/ijerph20032647
Chicago/Turabian StyleBebbington, Emily, Rob Poole, Sudeep Pradeep Kumar, Anne Krayer, Murali Krishna, Peter Taylor, Keith Hawton, Rajesh Raman, Mohan Kakola, Madhu Srinivasarangan, and et al. 2023. "Establishing Self-Harm Registers: The Role of Process Mapping to Improve Quality of Surveillance Data Globally" International Journal of Environmental Research and Public Health 20, no. 3: 2647. https://doi.org/10.3390/ijerph20032647