
Can an Aerobic Exercise Programme Improve the Response of the Growth Hormone in Fibromyalgia Patients? A Randomised Controlled Trial

 and
and
Abstract
:1. Introduction
2. Materials and Methods
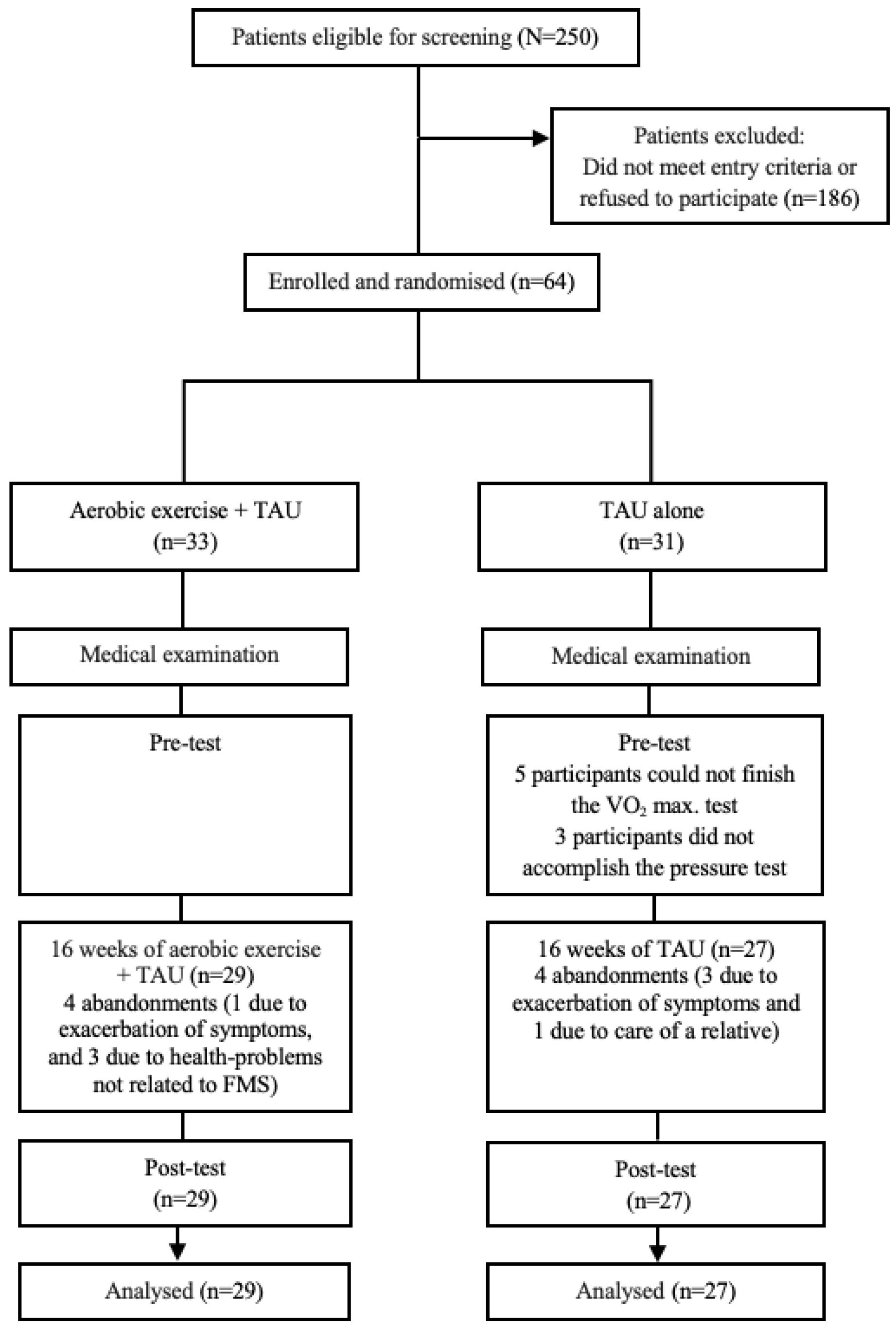
2.1. Participants
2.2. Interventions
2.3. Measurements
2.3.1. Main Outcome
2.3.2. Secondary Outcomes
2.4. Statistical Analyses
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bertolucci, P.H.F.; Oliveira, F.F. Cognitive Impairment in Fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 344. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef]
- Wolfe, F.; Brähler, E.; Hinz, A.; Häuser, W. Fibromyalgia prevalence, somatic symptom reporting, and the dimensionality of polysymptomatic distress: Results from a survey of the general population. Arthritis Care Res. 2013, 65, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.-A.; Perrot, S.; Häuser, W. Comorbid fibromyalgia: A qualitative review of prevalence and importance. Eur. J. Pain 2018, 22, 1565–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glombiewski, J.A.; Sawyer, A.T.; Gutermann, J.; Koenig, K.; Rief, W.; Hofmann, S.G. Psychological treatments for fibrom-yalgia: A meta-analysis. Pain 2010, 151, 280–295. [Google Scholar] [CrossRef]
- Montoya, M.G.; Martin, Á.P.; Salio, A.M.; Fuentes, J.V.; Alberch, E.A.; de la Cámara, A.G. Documento de Consenso interdisciplinar para el tratamiento de la fibromialgia. Actas Esp. Psiquiatr. 2010, 38, 108–120. [Google Scholar]
- Aaron, L.A.; Buchwald, D. A review of the evidence for overlap among unexplained clinical conditions. Ann. Intern. Med. 2001, 134, 868–981. [Google Scholar] [CrossRef]
- Lowe, J.C. Thyroid status of 38 fibromyalgia patients: Implications for the etiology of fibromyalgia. Clin. Bull. Myofascial Ther. 1997, 2, 36–41. [Google Scholar] [CrossRef]
- Van Houdenhove, B.; Egle, U.T. Fibromyalgia: A stress disorder? Piecing the biopsychosocial puzzle together. Psychother. Psychosom. 2004, 73, 267–275. [Google Scholar] [CrossRef]
- Montero-Marin, J.; Andrés-Rodríguez, L.; Tops, M.; Luciano, J.V.; Navarro-Gil, M.; Feliu-Soler, A.; López-Del-Hoyo, Y.; Garcia-Campayo, J. Effects of attachment-based compassion therapy (ABCT) on brain-derived neurotrophic factor and low-grade inflammation among fibromyalgia patients: A randomized controlled trial. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.D.; Deodhar, P.; Lorentzen, A.; Bennett, R.M.; Deodhar, A.A. Growth Hormone Perturbations in Fibromyalgia: A Review. Semin. Arthritis Rheum. 2007, 36, 357–379. [Google Scholar] [CrossRef] [PubMed]
- Díaz Robredo, L.A.; Robles Sanchez, J.I. Estabilidad emocional y cortisol como factores diferenciadores de la fibromialgia. Sanid. Mil. 2011, 67, 11–17. [Google Scholar] [CrossRef]
- Crofford, L.J.; Pillemer, S.R.; Kalogeras, K.T.; Cash, J.M.; Michelson, D.; Kling, M.A.; Sternberg, E.M.; Gold, P.W.; Chrousos, G.P.; Wilder, R.L. Hypothalamic-pituitary-adrenal axis perturbations in patients with fibrom-yalgia. Arthritis Rheum. 1994, 37, 1583–1592. [Google Scholar] [CrossRef] [PubMed]
- Griep, E.N.; Boersma, J.W.; De Kloet, E.R. Altered reactivity of the hypothalamic-pituitary-adrenal axis in the primary fibromyalgia syndrome. J. Rheumatol. 1993, 20, 469–474. [Google Scholar] [PubMed]
- McCain, G.A.; Tilbe, K.S. Diurnal hormone variation in fibromyalgia syndrome: A comparison with rheumatoid arthritis. J. Rheumatol. 1989, 19, 154–157. [Google Scholar]
- Bazzichi, L.; Rossi, A.; Giuliano, T.; De Feo, F.; Giacomelli, C.; Consensi, A.; Ciapparelli, A.; Consoli, G.; Dell’Osso, L.; Bombardieri, S. Association between thyroid autoimmunity and fibromyalgic disease severity. Clin. Rheumatol. 2007, 26, 2115–2120. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, F.; Karaca, Z.; Unluhizarci, K.Ü.; Kelestimur, F. The hypothalamopituitary-adrenal axis in chronic fatigue syndrome and fibromyalgia syndrome. Stress 2007, 10, 13–25. [Google Scholar]
- Bennett, R.; Smythe, H.; Wolfe, F. Recognizing fibromyalgia. Patient Care 1992, 26, 211–228. [Google Scholar]
- Denko, C.W.; Malemud, C.J. Role of the Growth Hormone/Insulin-like Growth Factor-1 Paracrine Axis in Rheumatic Diseases. Semin. Arthritis Rheum. 2005, 35, 24–34. [Google Scholar] [CrossRef]
- Povedano, J.; Salaberri, J.; Corteguera, M.; García, A. Fibrositis como forma de presentación de un mieloma no secretor. Rev. Clin. Esp. 1989, 185, 107–108. [Google Scholar]
- Demitrack, M.A. Evidence for and pathophysilogic implications of hypothalamic-pituitary-adrenal axis dysregulation in fi-bromyalgia and chronic fatigue syndrome. Ann. N. Y. Acad. Sci. 1998, 840, 684–697. [Google Scholar] [CrossRef] [Green Version]
- Tavares, M.R.; Frazao, R.; Donato, J. Understanding the role of growth hormone in situations of metabolic stress. J. Endocrinol. 2023, 256, e220159. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Clark, S.C.; Walczyk, J. A Randomized, Double-Blind, Placebo-controlled Study of Growth Hormone in the Treatment of Fibromyalgia. Am. J. Med. 1998, 104, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Cuatrecasas, G.; Alegre, C.; Fernandezsola, J.; Gonzalez, M.J.; Garciafructuoso, F.J.; Pocadias, V.; Nadal, A.; Cuatrecasas, G.; Navarro, F.J.; Mera, A.C.; et al. Growth hormone treatment for sustained pain reduction and improvement in quality of life in severe fibromyalgia. Pain 2012, 153, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.; Basuodan, R.M.; Alwhaibi, R.; Ebrahim, E.E.; Verma, A.; Sd, S.; Mohamed, S.H.P.; Aldhafian, O.R.; Nwihadh, N.A.; Saleh, A.K. Clinical and endocrinological responses to different exercise training methods in chronic low back pain: A randomized controlled trial. Endocr. Metab. Immune Disord.-Drug Targets 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Mannerkorpi, K.; Nordeman, L.; Cider, A.A.S.; Jonsson, G. Does moderate-to-high intensity Nordic walking improve functional capacity and pain in fibromyalgia? A prospective randomized controlled trial. Thromb. Haemost. 2010, 12, R189. [Google Scholar] [CrossRef] [Green Version]
- Harriss, D.J.; Atkinson, G. Update—Ethical Standards in Sport and Exercise Science Research. Int. J. Sports Med. 2011, 32, 819–821. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 6th ed.; Lip-pincott Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Yusta, A.; Laguna, P.; Ballina, J. Criterios diagnósticos y exploración. Fibromialgia. Reunión de expertos. Cátedra Extraordinaria del Dolor “Fundación Grünenthal”. Salamanca, España. Available online: http://www.catedradeldolor.com/PDFs/Docencia_Expertos/2001%20Fibromialgias.pdf (accessed on 21 January 2023).
- Lohman, T.; Roche, A.; Martello, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1988. [Google Scholar]
- Rivera, J.; González, T. The Fibromyalgia Impact Questionnaire: A validated Spanish version to assess the health status in women with fibromyalgia. Ann. Rheum. Dis. 2004, 22, 554–560. [Google Scholar]
- Rabin, R.; Oemar, M.; Oppe, M. EQ-5D-3L User Guide: Basic Information on How to Use the EQ-5D-3L Instrument. In EQ-5D-3L User Guide: Basic Information on How to Use the EQ-5D-3L Instrument (The EuroQol Group); EuroQol Group: Rotterdam, The Netherlands, 2011; pp. 1–23. [Google Scholar]
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Riedel, W.; Schlapp, U.; Leck, S.; Netter, P.; Neeck, G. Blunted ACTH and cortisol responses to systemic injection of corticotropin-releasing hormone (CRH) in fibromyalgia: Role of somatostatin and CRH-binding protein. Ann. N. Y. Acad. Sci 2002, 966:, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Gürsel, Y.; Ergin, S.; Ulus, Y.; Erdoğan, M.F.; Yalçın, P.; Evcik, D. Hormonal Responses to Exercise Stress Test in Patients with Fibromyalgia Syndrome. Clin. Rheumatol. 2001, 20, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Paiva, E.S.; Deodhar, A.; Jones, K.D.; Bennett, R. Impaired growth hormone secretion in fibromyalgia patients: Evidence for augmented hypothalamic somatostatin tone. Arthritis Rheum. 2002, 46, 1344–1350. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B.; Rivest, S. Effect of a chronic stress on CRF neuronal activity and expression of its type 1 receptor in the rat brain. Am. J. Physiol. Integr. Comp. Physiol. 1998, 275, R1438–R1449. [Google Scholar] [CrossRef] [PubMed]
- Kanaley, J.A.; Weltman, J.Y.; Veldhuis, J.D.; Rogol, A.; Hartman, M.L.; Weltman, A. Human growth hormone response to repeated bouts of aerobic exercise. J. Appl. Physiol. 1997, 83, 1756–1761. [Google Scholar] [CrossRef]
- Pritzlaff, C.J.; Wideman, L.; Weltman, J.Y.; Abbott, R.D.; Gutgesell, M.E.; Hartman, M.L.; Veldhuis, J.D.; Weltman, A. Impact of acute exercise intensity on pulsatile growth hormone release in men. J. Appl. Physiol. 1999, 87, 498–504. [Google Scholar] [CrossRef]
- Manetta, J.; Brun, J.F.; Maimoun, L.; Callis, A.; Prefaut, C.; Mercier, J. Effect of training on the GH/IGF-I axis during exercise in middle-aged men: Relationship to glucose homeostasis. Am. J. Physiol. Metab. 2002, 283, E929–E936. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, J.W.; Holden, N.; Hills, R.K.; Wheatley, K.; Clayton, R.N.; Bates, A.S.; Sheppard, M.C.; Stewart, P.M. Association between premature mortality and hypopituitarism: West Midlands Prospective Hypopituitary Study Group. Lancet 2001, 357, 425–431. [Google Scholar] [CrossRef]
- Miller, K.K.; Biller, B.M.K.; Lipman, J.G.; Bradwin, G.; Rifai, N.; Klibanski, A. Truncal Adiposity, Relative Growth Hormone Deficiency, and Cardiovascular Risk. J. Clin. Endocrinol. Metab. 2005, 90, 768–774. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.J.; Barber, K.A.; Overend, T.J.; Peloso, P.M.J.; Schachter, C.L. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst. Rev. 2007, 4, CD003786. [Google Scholar] [CrossRef]
- Jones, K.D.; Adams, D.; Winters-Stone, K.; Burckhardt, C.S. A comprehensive review of 46 exercise treatment studies in fibromyalgia (1988–2005). Health Qual. Life Outcomes 2006, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Energy, Nutrition and Human Performance, 5th ed.; Lip-pincott Williams & Wilkins: Baltimore, MD, USA, 2001. [Google Scholar]


{kind=link}
| Exercise (n = 29) | TAU (n = 27) | p | |
|---|---|---|---|
| Sociodemographic and Medication | |||
| Age, years, M (SD) | 46.9 (9.7) | 48.7 (7.8) | 0.465 |
| Age of first illness symptoms, years, M (SD) | 30.1 (12.8) | 32.7 (11.9) | 0.371 |
| Years from first symptoms to diagnosis, M (SD) | 13.3 (12.5) | 11.8 (10.4) | 0.805 |
| Length of illness, years, M (SD) | 16.8 (13) | 15.8 (10.8) | 0.954 |
| Educational level, frequency (%) | 0.950 | ||
| No studies/primary | 14 (48.3) | 13 (48.1) | |
| Secondary studies | 8 (27.6) | 8 (29.6) | |
| University | 7 (24.1) | 6 (22.2) | |
| Work outside home, yes, frequency (%) | 23 (79.3) | 21 (77.8) | 0.890 |
| Pain medication, yes, frequency (%) | 16 (55.2) | 13 (48.1) | 0.599 |
| Antidepressant medication, yes, frequency (%) | 14 (48.3) | 11 (40.7) | 0.571 |
| Anxiolytic medication, yes, frequency (%) | 13 (44.8) | 10 (37.0) | 0.554 |
| Exercise (n = 29) | TAU (n = 27) | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Pre- | Post- | Δ% | Pre- | Post- | Δ% | p | Ƞ2 |
| GH 20’ (ng/mL) | 2.87 (2.88) | 4.74 (6.00) | 65.2 | 3.76 (4.84) | 3.38 (5.21) | −10.1 | 0.048 | 0.07 |
| GH (ng/mL) | 3.65 (3.89) | 3.45 (4.57) | −5.5 | 2.40 (2.72) | 2.60 (4.99) | 8.3 | 0.656 | <0.01 |
| VO2 Max. (ml/kg/min) a | 20.06 (5.58) | 22.02 (5.68) | 9.8 | 19.18 (4.60) | 18.47 (4.17) | −3.7 | 0.006 | 0.15 |
| Pressure (cm3) b | 5.68 (2.58) | 6.53 (2.68) | 15.0 | 5.58 (2.70) | 5.94 (2.17) | 6.5 | 0.296 | 0.02 |
| BMI (kg/m2) | 26.71 (3.90) | 26.64 (4.15) | −0.3 | 27.03 (5.89) | 26.43 (5.66) | −2.2 | 0.091 | 0.05 |
| Σ skinfolds | 156.78 (43.77) | 141.23 (39.39) | −9.9 | 153.41 (51.65) | 149.37 (42.72) | −2.6 | 0.042 | 0.08 |
| FIQ | 66.90 (14.44) | 58.71 (19.08) | −12.4 | 75.81 (14.08) | 68.36 (20.44) | −9.8 | 0.807 | <0.01 |
| EQ-5D | 0.22 (0.29) | 0.40 (0.34) | 81.8 | 0.21 (0.31) | 0.23 (0.31) | 8.7 | 0.019 | 0.10 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. GH 20’ | |||||||
| 2. GH basal | 0.72 *** | ||||||
| 3. VO2 max | 0.33 ** | 0.47 *** | |||||
| 4. Pressure | 0.19 | 0.19 | 0.16 | ||||
| 5. BMI | −0.41 *** | −0.50 *** | −0.50 *** | 0.01 | |||
| 6. Σ skinfolds | −0.45 *** | −0.49 *** | −0.38 ** | 0.15 | 0.83 *** | ||
| 7. FIQ | −0.11 | −0.19 | −0.34 ** | −0.18 | 0.07 | 0.27 * | |
| 8. EQ-5D | 0.15 | 0.23 * | 0.34 ** | 0.27 | −0.14 | −0.30 * | −0.87 *** |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. GH 20’ | |||||||
| 2. GH basal | 0.88 *** | ||||||
| 3. VO2 max | 0.48 ** | 0.38 ** | |||||
| 4. Pressure | 0.17 | 0.20 | 0.22 | ||||
| 5. BMI | −0.52 *** | −0.50 *** | −0.41 ** | −0.12 | |||
| 6. Σ skinfolds | −0.49 *** | −0.47 *** | −0.40 ** | 0.05 | 0.79 *** | ||
| 7. FIQ | −0.20 | −0.15 | −0.40 ** | −0.38 ** | 0.10 | 0.18 | |
| 8. EQ-5D | 0.27 * | 0.22 | 0.43 ** | 0.19 | −0.07 | −0.21 | −0.79 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estrada-Marcén, N.C.; Casterad-Seral, J.; Montero-Marin, J.; Serrano-Ostáriz, E. Can an Aerobic Exercise Programme Improve the Response of the Growth Hormone in Fibromyalgia Patients? A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 2261. https://doi.org/10.3390/ijerph20032261
Estrada-Marcén NC, Casterad-Seral J, Montero-Marin J, Serrano-Ostáriz E. Can an Aerobic Exercise Programme Improve the Response of the Growth Hormone in Fibromyalgia Patients? A Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(3):2261. https://doi.org/10.3390/ijerph20032261
Chicago/Turabian StyleEstrada-Marcén, Nerea C., Jaime Casterad-Seral, Jesus Montero-Marin, and Enrique Serrano-Ostáriz. 2023. "Can an Aerobic Exercise Programme Improve the Response of the Growth Hormone in Fibromyalgia Patients? A Randomised Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 3: 2261. https://doi.org/10.3390/ijerph20032261