
Feasibility and Acceptability of a Remote Stepped Care Mental Health Programme for Adolescents during the COVID-19 Pandemic in India
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Quantitative Feasibility Indicators
2.3.2. Qualitative Individual Interviews and Focus Group Discussion
2.3.3. Clinical Outcomes
2.4. Procedures
2.5. Analysis
3. Results
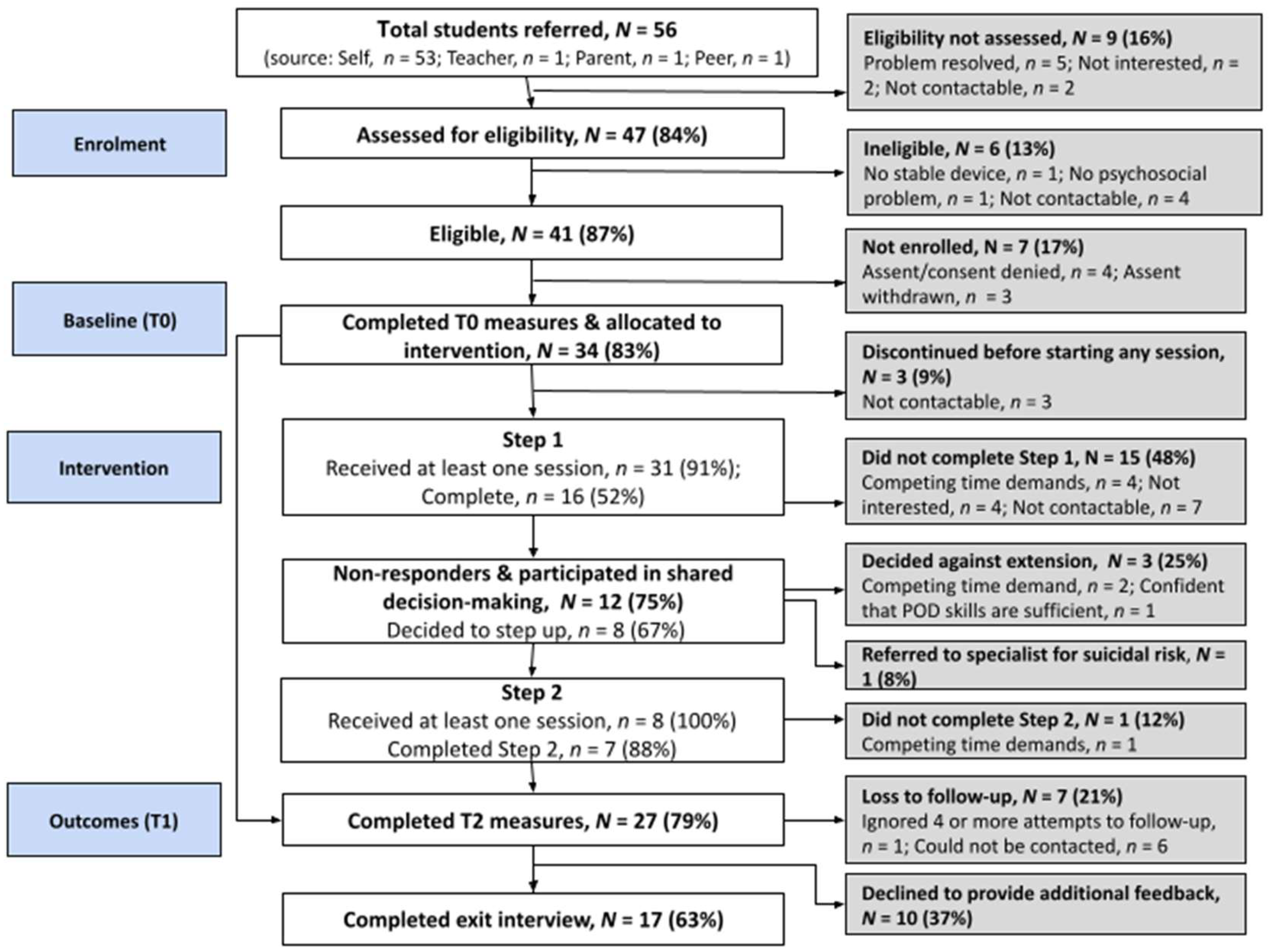
3.1. Feasibility Indicators
3.2. Qualitative Findings
3.2.1. Coherence of the Intervention Steps
“Ma’am, I really liked ‘POD’. Through this, I learned recognising problems, then finding their options and learning to do it.”(Adolescent P9, 15 years, female, dropped out from Step 1)
“I prefer learning problem solving first. To me, being active [the Step 2 behavioural activation module] looked like one option of broad problem-solving framework. So, we should learn problem solving first and then gradually we can learn different options as part of this skill.”(Adolescent P6, 15 years, female, completed both steps)
“Deep breathing and overcoming fear [the Step 2 exposure module] have become my favourite [compared to POD]. Till the fourth or fifth session, [counsellor] sir taught us about POD and these other skills were taken up in the sessions after that. It would have been even better for our progress to learn things like deep breathing and overcoming fear much earlier.”(Adolescent P3, 16 years, male, completed both steps)
3.2.2. Usefulness of Counsellors’ Guidance and Supporting Handouts
“Madam [the counsellor] was very understanding and quickly understood everything I shared with her. She helped me a lot in finding alternative solutions to problems. Initially, I felt very nervous, but madam told us how to proceed and gave us step-by-step directions and tips on finding solutions, which helped me greatly.”(Adolescent P7, 16 years, female, completed Step 1 and opted out of Step 2)
“She [counsellor] neither give me any suggestions, nor did she pressurise me to continue or terminate. She had left it for me to decide, i.e., if I wanted to end, I could end it, and if I wanted to continue, then I could continue also; that was my choice. This was a good thing.”(Adolescent P6, 15 years, female, completed both steps)
“If we sense a student is reluctant to open up or talk about his difficulties, we try to take it slow. We talk about their interest areas, things they like and ask more specific questions to help them express themselves more concretely. We will provide them with step-by-step guidance if they struggle to open up or express their concerns. Usually, by the end of a couple of sessions, they feel more comfortable with the process. By the time they are in Step 2, they are pretty vocal and engaged in the process.”(Counsellor C2, female)
“The most helpful thing in both these booklets was that after reading their story, it seemed that when they [story characters] can [face their fears], why can’t I. The boy in the story feels scared of dogs and no one else feels that way; similarly, I feel scared of certain things, but others don’t. This is something we can learn and correct. Then, I did the right thing after reading the booklet.”(Adolescent P3, 17 years old, male, completed both steps)
“The stories given were very good, as you can understand everything from the story. Then some ready-made solutions have been given, which are also very good. You people [programme developers] can write more stories... like something based on my problem. My main problem is overthinking; you can make a story about it and then you should give me that booklet.”(Adolescent P14, 15 years old, female, completed both steps)
3.2.3. Balancing Structure and Adolescents’ Needs in Shared Decision-Making
“Initially, it was challenging to do the shared decision-making. We struggled with how to say it, frame it in age-appropriate language, explain why [the adolescent] needs to get involved in it, when we should raise this topic, and what the next steps will be. To overcome these challenges, we used to read [the step-by-step manual], and discuss this thing with other counsellors. Then we also did role-play. Our supervisor also helped. It was a bit of a challenge initially, but all this made it easier as we moved ahead.”(Counsellor C5, female)
“Yes, it would have been good if she [counsellor] had explained what will happen next in the counselling journey. For example, had I known the total number of sessions [in Step 2], I would have taken the decision instantly rather than taking too much time to think about it. But I was confused about how long the counselling will go on. Also, she told me the benefits of continuing counselling but not the drawbacks of ending counselling. When you [counsellor] are helping me, explain both benefits and drawbacks so that I can be more confident in making the decision. Ultimately, it will be my decision only, but it will be good if I get more information and help from the counsellor.”(Adolescent P2, 16 years old, female, completed both steps)
3.2.4. Valued Outcomes and Skill Development
“During the sessions, the counsellor made me complete a graph that helped me understand how my problems were going. Then counsellor asked me to work on it. Based on our discussion, I worked on generating and applying alternative solutions, which helped reduce problems.”(Adolescent P4, 18 years old, male, completed Step 1 and opted out of Step 2)
“Earlier I used to procrastinate but now I’m much faster. The counselling helped me learn that we have to plan and take steps to solve problems, troubles won’t go on their own.”(Adolescent P14, 18 years old, male, completed Step 1 and opted out of Step 2)
“I made good improvements in counselling like my problem with overthinking were reduced, my fear subsided, and those negative bad thoughts were also gone down. At times, I still get bad thoughts, but now I can manage them. The most important thing is that I have learned to control, no matter what the situation is... Earlier, if I was afraid to go somewhere, I would not go, but now I try to control, deep breathe, plan to face [my fear] and go wherever I’m needed.”(Adolescent P3, 17 years old, male, completed both steps)
“We talked about [my problem with] trust issues, and came out with a few options, but I did not feel there was any suitable option, given the lockdown constraints. I concluded that leaving it as it is okay, and we do not need anything… Honestly, not much could be done about this but to leave it aside.”(Adolescent P9, 17 years old, female, completed both steps)
3.2.5. Implementation of Remote Delivery Methods
“[Counselling] was very good on the phone because sometimes it happens with me that I cannot tell everything in detail face-to-face, but on the phone, it was easy to tell… If you are face-to-face, then I keep thinking about my and the counsellor’s facial expressions, which makes me feel a little hesitant.”(Adolescent P16, 18 years old, female, completed/responded to Step 1)
“Sometimes our sessions extend beyond an hour, but that is primarily due to network and connectivity issues. With multiple call drops, the counsellor had to wait 10–15 min before we could get into stable connectivity.”(Adolescent P2, 16 years old, female, completed both steps)
“As everything was new [for students] in remote counselling, we had to set the ground rules and agenda, which took longer than we planned… A lot of our time was spent monitoring the progress, especially in the first session; we had to tell students how to do the progress monitoring for each problem. This was very difficult to explain on the phone, the child would be confused and since we could not see them, we just relied on whatever they said…Even other activities in booklets used to take more time, as we were remote, we had to explain to them go on this page, do this here and then go on that page, etc. This used to take half of the session, and then we will reach the main session agenda and to complete them well, it was necessary to spend time there too. So, this is why the session used to go on for longer than what was given in the manual.”(Counsellor C3, Male)
“[Counselling] was good on the phone, as my problem is almost resolved. However, it would have been much better if she [counsellor] was offline. This entire year, whether it was counselling or the school classes, it was online, and we do not feel so comfortable with it. Talking face-to-face would have been much better than online. The counsellor will also find it much easier to work out solutions for our problems. Even from our body language, she can observe the smallest of things, which would help her understand us much better. [Even on the phone] she did understand everything, but it would have been better if it was offline.”(Adolescent P7, 16 years old, Female, completed/responded to Step 1)
“We got one advantage [due to COVID restrictions] that 2–3 children out of every five children who came to us were either feeling bored at home or were in a situation where they could not talk to others and express themselves. So, when they came to us, we spent time building trust and genuinely showed concern for them during our session; they liked it a lot. They got engaged, thinking this was a platform where they could talk and express their viewpoints. They intrinsically felt motivated about the sessions and then we didn’t have to put in too much effort… Once the rapport is well-established, they easily open up and start talking about their problems.”(Counsellor C3, male)
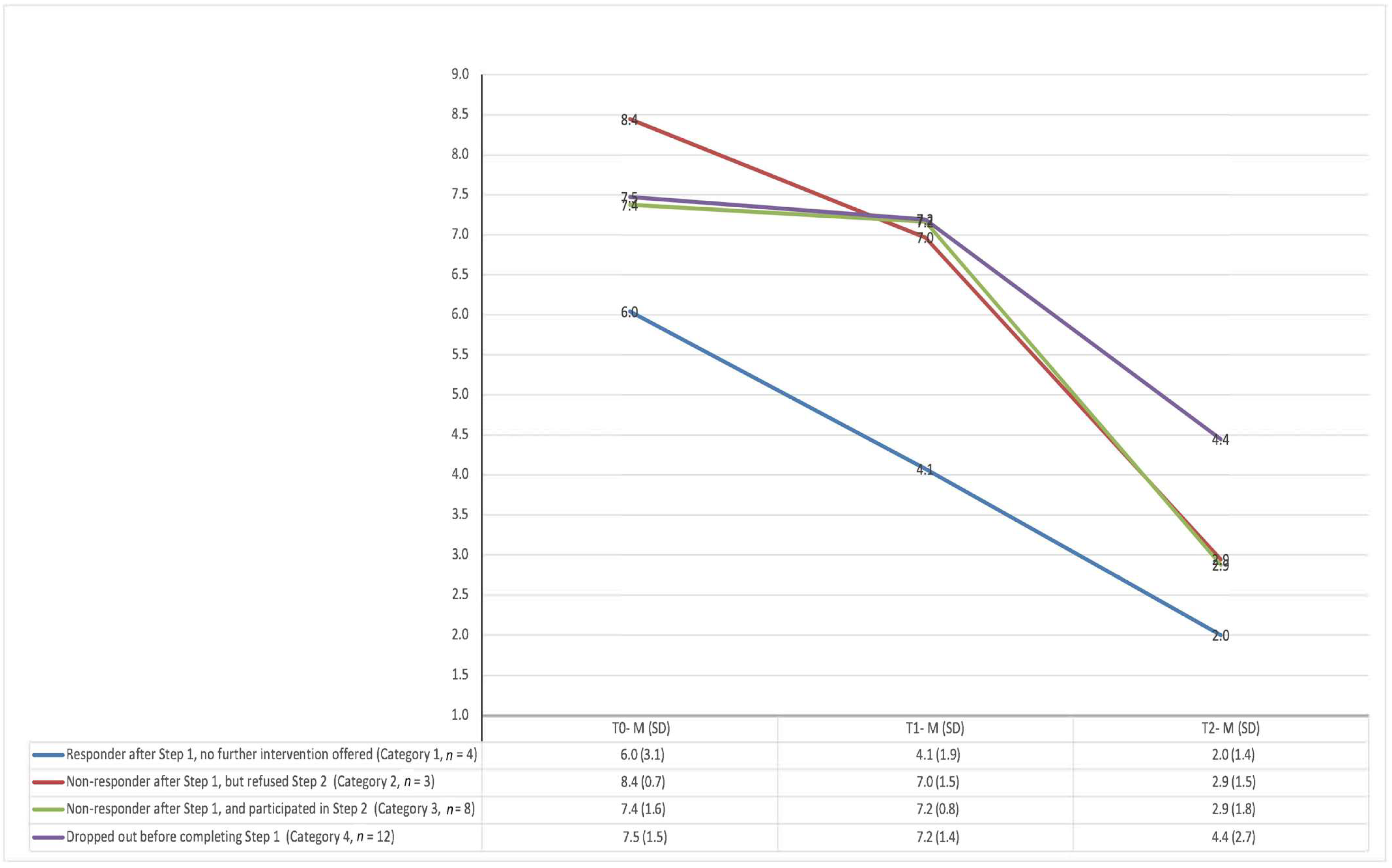
3.3. Indicative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
| S.no | Item | Description | Performance Band |
|---|---|---|---|
| 1. | Remote Delivery Ground Rules |
| 1 2 3 4 NA |
| 2. | Agenda setting |
| 1 2 3 4 NA |
| 3. | Assessing Progress: Assessing progress from first session in terms of achievement of counselling goals and assessment of any risk and suitable management of the same | ||
| a. | Progress monitoring |
| 1 2 3 4 NA |
| b. | Monitoring risk for harm (applicable if needed as per the safety protocol) |
| 1 2 3 4 NA |
| 4. | Use of appropriate intervention: choosing and implementing the module/techniques most suitable to student’s Stage | ||
| a. | Selecting appropriate intervention HINT: to be rated for selection of steps within particular intervention such as problem solving, behavioral activation and choice of one of three elements (BA/Exposure/Communication) in Modular Behavioral Intervention (MBI) |
| 1 2 3 4 NA |
| b. | Rationale for intervention HINT: to be rated for educating about the counselling programme and steps within a particular intervention such as problem solving, behavioral activation and choice of one of three element in Modular Behavioral Intervention (MBI) |
| 1 2 3 4 NA |
| c. | Implementation of interventionHINT: to be rated for implementing steps within a particular intervention such as problem solving, behavioral activation and choice of one of three element in Modular Behavior Intervention (MBI) |
| 1 2 3 4 NA |
| d. | Reviewing InterventionHINT: to be rated for discussing the intervention done within the session and what were the results of implementing the intervention technique in one of three elements in Modular Behavioral Intervention (MBI)(Applicable for MBI sessions) |
| 1 2 3 4 NA |
| 5. | Sharing Material and Home practice: Giving booklet/resource material with explanation and completion of written work and/or implementation of tasks given in real life) | ||
| a. | Sharing Material |
| 1 2 3 4 NA |
| b. | Rationale for home practice HINT: Covers rationale of reading and writing exercises in booklets and/or implementation of tasks given in booklets |
| 1 2 3 4 NA |
| c. | Reviewing home practice (Session 2 onwards)HINT: Covers review of reading and writing exercises in booklets and/or implementation of tasks given in booklets |
| 1 2 3 4 NA |
| d. | Choosing & planning suitable home practiceHINT: Covers planning of reading and writing exercises in booklets and/or implementation of tasks given in booklets |
| 1 2 3 4 NA |
| 6. | Fostering Therapeutic Relationship | ||
| a. | Engagement |
| 1 2 3 4 NA |
| b. | Confidentiality |
| 1 2 3 4 NA |
| 7. | Shared Decision Making | ||
| a. | Collaboration |
| 1 2 3 4 NA |
| b. | Listing Options |
| 1 2 3 4 NA |
| c. | Exploring Student Understanding of Decision |
| 1 2 3 4 NA |
| d. | Respecting Student Decision |
| 1 2 3 4 NA |
| 8. | Summaries and Feedback |
| 1 2 3 4 NA |
| 9. | Effective use of Time |
| 1 2 3 4 NA |
References
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How Mental Health Care Should Change as a Consequence of the COVID-19 Pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of Mental Health Problems during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Oxfam India. Status Report: Government and Private Schools during COVID-19. 2020. Available online: https://www.oxfamindia.org/sites/default/files/2020-09/Status%20report%20Government%20and%20private%20schools%20during%20COVID%20-%2019.pdf (accessed on 31 October 2022).
- United Nations Children’s Fund; United Nations Educational, Scientific and Cultural Organization; The World Bank. What Have We Learnt: Overview of Findings from a Survey of Ministries of Education on National Responses to COVID-19. 2020. Available online: https://data.unicef.org/resources/national-education-responses-to-covid19/ (accessed on 31 October 2022).
- Borghouts, J.; Eikey, E.; Mark, G.; Leon, C.D.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.; Sorkin, D.H. Barriers to and Facilitators of User Engagement With Digital Mental Health Interventions: Systematic Review. J. Med. Internet Res. 2021, 23, e24387. [Google Scholar] [CrossRef] [PubMed]
- James, K. Remote Mental Health Interventions for Young People: A Rapid Review of the Evidence. Youth Access. 2022. Available online: https://childhub.org/sites/default/files/library/attachments/remote-mental-health-interventions-for-young-people-rapid-review.pdf (accessed on 31 October 2022).
- Mondal, I.; Anand, N.; Sharma, M.K.; Kohli, T.; Thakur, P.C.; Kande, J.S.; Venkateshan, S.; Sj, A. Telephonic Psychotherapy in India: A Reminder of Challenges in Times of COVID-19. Asian J. Psychiatry 2020, 53, 102432. [Google Scholar] [CrossRef] [PubMed]
- Gonsalves, P.; Sharma, R.; Jambhale, A.; Chodankar, B.; Verma, M.; Hodgson, E.S.; Weiss, H.A.; Laurent, B.; Cavanagh, K.; Fairburn, C.; et al. Pilot randomised controlled trial of a remotely delivered online intervention for adolescent mental health problems in India: Lessons learned about low acceptability and feasibility during the COVID-19 pandemic. BJPsych Open 2022, 9, e7. [Google Scholar] [CrossRef]
- Chew, A.M.K.; Ong, R.; Lei, H.-H.; Rajendram, M.; Grisan, K.V.; Verma, S.K.; Fung, D.S.S.; Leong, J.J.; Gunasekeran, D.V. Digital Health Solutions for Mental Health Disorders During COVID-19. Front. Psychiatry 2020, 11, 582007. [Google Scholar] [CrossRef]
- Aboujaoude, E.; Gega, L.; Parish, M.B.; Hilty, D.M. Editorial: Digital Interventions in Mental Health: Current Status and Future Directions. Front. Psychiatry 2020, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Sagar, R.; Singh, S. National Tele-Mental Health Program in India: A Step towards Mental Health Care for All? Indian J. Psychiatry 2022, 64, 117–119. [Google Scholar] [CrossRef]
- Koly, K.N.; Saba, J.; Muzaffar, R.; Modasser, R.B.; M, T.H.; Colon-Cabrera, D.; Warren, N. Exploring the Potential of Delivering Mental Health Care Services Using Digital Technologies in Bangladesh: A Qualitative Analysis. Internet Interv. 2022, 29, 100544. [Google Scholar] [CrossRef]
- Michelson, D.; Malik, K.; Krishna, M.; Sharma, R.; Mathur, S.; Bhat, B.; Parikh, R.; Roy, K.; Joshi, A.; Sahu, R.; et al. Development of a Transdiagnostic, Low-Intensity, Psychological Intervention for Common Adolescent Mental Health Problems in Indian Secondary Schools. Behav. Res. Ther. 2020, 130, 103439. [Google Scholar] [CrossRef]
- Chorpita, B.F.; Daleiden, E.L.; Malik, K.; Gellatly, R.; Boustani, M.M.; Michelson, D.; Knudsen, K.; Mathur, S.; Patel, V.H. Design Process and Protocol Description for a Multi-Problem Mental Health Intervention within a Stepped Care Approach for Adolescents in India. Behav. Res. Ther. 2020, 133, 103698. [Google Scholar] [CrossRef]
- Roy, K.; Shinde, S.; Sarkar, B.K.; Malik, K.; Parikh, R.; Patel, V. India’s response to adolescent mental health: A policy review and stakeholder analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Michelson, D.; Malik, K.; Parikh, R.; Weiss, H.A.; Doyle, A.M.; Bhat, B.; Sahu, R.; Chilhate, B.; Mathur, S.; Krishna, M.; et al. Effectiveness of a Brief Lay Counsellor-Delivered, Problem-Solving Intervention for Adolescent Mental Health Problems in Urban, Low-Income Schools in India: A Randomised Controlled Trial. Lancet Child Adolesc. Health 2020, 4, 571–582. [Google Scholar] [CrossRef]
- Malik, K.; Ibrahim, M.; Mathur, S.; Jose, J.E.; Nair, P.; Sahu, R.; Krishna, M.; Jangra, D.; Mathews, R.; Cuijpers, P.; et al. Development of a Transdiagnostic Stepped Care Programme for Common Adolescent Mental Health Problems in Indian Secondary Schools: Lessons from a Pilot Study Examining Acceptability and Feasibility. Glob. Ment. Health 2022, 9, 521–525. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef] [Green Version]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Healthcare Interventions: An Overview of Reviews and Development of a Theoretical Framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- Parikh, R.; Michelson, D.; Malik, K.; Shinde, S.; Weiss, H.A.; Hoogendoorn, A.; Ruwaard, J.; Krishna, M.; Sharma, R.; Bhat, B.; et al. The Effectiveness of a Low-Intensity Problem-Solving Intervention for Common Adolescent Mental Health Problems in New Delhi, India: Protocol for a School-Based, Individually Randomized Controlled Trial with an Embedded Stepped-Wedge, Cluster Randomized Controlled Recruitment Trial. Trials 2019, 20, 568. [Google Scholar] [CrossRef] [Green Version]
- Mishra, P.; Udas, A.; Pahwa, S.; Sen, S.; Haldar, K. Adapting a Revised Child Anxiety and Depression Scale for Rural India: A Pilot, Amenable to Scale Up. PsyArXiv 2016. [Google Scholar] [CrossRef]
- Ebesutani, C.; Reise, S.P.; Chorpita, B.F.; Ale, C.; Regan, J.; Young, J.; Higa-McMillan, C.; Weisz, J.R. The Revised Child Anxiety and Depression Scale-Short Version: Scale Reduction via Exploratory Bifactor Modeling of the Broad Anxiety Factor. Psychol. Assess. 2012, 24, 833–845. [Google Scholar] [CrossRef] [Green Version]
- Krause, K.R.; Edbrooke-Childs, J.; Singleton, R.; Wolpert, M. Are We Comparing Apples with Oranges? Assessing Improvement Across Symptoms, Functioning, and Goal Progress for Adolescent Anxiety and Depression. Child Psychiatry Hum. Dev. 2022, 53, 737–753. [Google Scholar] [CrossRef]
- Weisz, J.R.; Chorpita, B.F.; Frye, A.; Ng, M.Y.; Lau, N.; Bearman, S.K.; Ugueto, A.M.; Langer, D.A.; Hoagwood, K.E. Research Network on Youth Mental Health Youth Top Problems: Using Idiographic, Consumer-Guided Assessment to Identify Treatment Needs and to Track Change during Psychotherapy. J. Consult. Clin. Psychol. 2011, 79, 369–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, R.; Hoogendoorn, A.; Michelson, D.; Ruwaard, J.; Sharma, R.; Bhat, B.; Malik, K.; Sahu, R.; Cuijpers, P.; Patel, V. Increasing Demand for School Counselling through a Lay Counsellor-Delivered Classroom Sensitisation Intervention: A Stepped-Wedge Cluster Randomised Controlled Trial in New Delhi, India. BMJ Glob. Health 2021, 6, e003902. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Extended Version of the Strengths and Difficulties Questionnaire as a Guide to Child Psychiatric Caseness and Consequent Burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef]
- Makoul, G.; Clayman, M.L. An Integrative Model of Shared Decision Making in Medical Encounters. Patient Educ. Couns. 2006, 60, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the Framework Method for the Analysis of Qualitative Data in Multi-Disciplinary Health Research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Pretorius, C.; Chambers, D.; Coyle, D. Young People’s Online Help-Seeking and Mental Health Difficulties: Systematic Narrative Review. J. Med. Internet Res. 2019, 21, e13873. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, G.M.; Donovan, C.L.; March, S.; Forbes, Y. Logging into Therapy: Adolescent Perceptions of Online Therapies for Mental Health Problems. Internet Interv. 2019, 15, 93–99. [Google Scholar] [CrossRef]
- Galagali, P.M.; Ghosh, S.; Bhargav, H. The Role of Telemedicine in Child and Adolescent Healthcare in India. Curr. Pediatr. Rep. 2021, 9, 154–161. [Google Scholar] [CrossRef]
- O’Connor, M. School Counselling during COVID-19: An Initial Examination of School Counselling Use during a 5-Week Remote Learning Period. Pastor. Care Educ. 2022, 40, 81–91. [Google Scholar] [CrossRef]
- Madigan, S.; Racine, N.; Cooke, J.E.; Korczak, D.J. COVID-19 and Telemental Health: Benefits, Challenges, and Future Directions. Can. Psychol. 2021, 62, 5–11. [Google Scholar] [CrossRef]
- Witteveen, A.B.; Young, S.; Cuijpers, P.; Ayuso-Mateos, J.L.; Barbui, C.; Bertolini, F.; Cabello, M.; Cadorin, C.; Downes, N.; Franzoi, D.; et al. Remote Mental Health Care Interventions during the COVID-19 Pandemic: An Umbrella Review. Behav. Res. Ther. 2022, 159, 104226. [Google Scholar] [CrossRef]


| Activity/Material | Description |
|---|---|
| Student webinar | Adapted from an existing in-person classroom ‘sensitisation’ session [25]. Attendees were presented with an animated video and a PowerPoint presentation that contained age-appropriate information about common mental health problems and explained the rationale for the available intervention. This was followed by a counsellor-facilitated group discussion about the practicalities of remote delivery and procedures for enrolling in the study. Separate webinars were offered to each class. |
| Teacher webinar | Structured around a similar PowerPoint presentation as the student webinar, followed by a group discussion concerned with how teachers could effectively disseminate information about the study and encourage students to participation in the intervention. |
| Digital flyer | Contained a brief description of the available intervention and how to enrol in the study. This was circulated by teachers to class WhatsApp groups. Students were able to begin the enrolment process either by calling or messaging (WhatsApp) a designated number without incurring any airtime charges. |
| YouTube video | Contained an abbreviated version of the same information that was presented by counsellors during the webinar, in which a member of the study spoke to camera. It was intended for students who could not attend the live webinar due to technical issues or competing activities. Teachers circulated this to class WhatsApp groups along with the flyer. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, K.; Shetty, T.; Mathur, S.; Jose, J.E.; Mathews, R.; Sahay, M.; Chauhan, P.; Nair, P.; Patel, V.; Michelson, D. Feasibility and Acceptability of a Remote Stepped Care Mental Health Programme for Adolescents during the COVID-19 Pandemic in India. Int. J. Environ. Res. Public Health 2023, 20, 1722. https://doi.org/10.3390/ijerph20031722
Malik K, Shetty T, Mathur S, Jose JE, Mathews R, Sahay M, Chauhan P, Nair P, Patel V, Michelson D. Feasibility and Acceptability of a Remote Stepped Care Mental Health Programme for Adolescents during the COVID-19 Pandemic in India. International Journal of Environmental Research and Public Health. 2023; 20(3):1722. https://doi.org/10.3390/ijerph20031722
Chicago/Turabian StyleMalik, Kanika, Tejaswi Shetty, Sonal Mathur, James E. Jose, Rhea Mathews, Manogya Sahay, Preeti Chauhan, Pooja Nair, Vikram Patel, and Daniel Michelson. 2023. "Feasibility and Acceptability of a Remote Stepped Care Mental Health Programme for Adolescents during the COVID-19 Pandemic in India" International Journal of Environmental Research and Public Health 20, no. 3: 1722. https://doi.org/10.3390/ijerph20031722