
Does a Kegel Exercise Program Prior to Resistance Training Reduce the Risk of Stress Urinary Incontinence?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
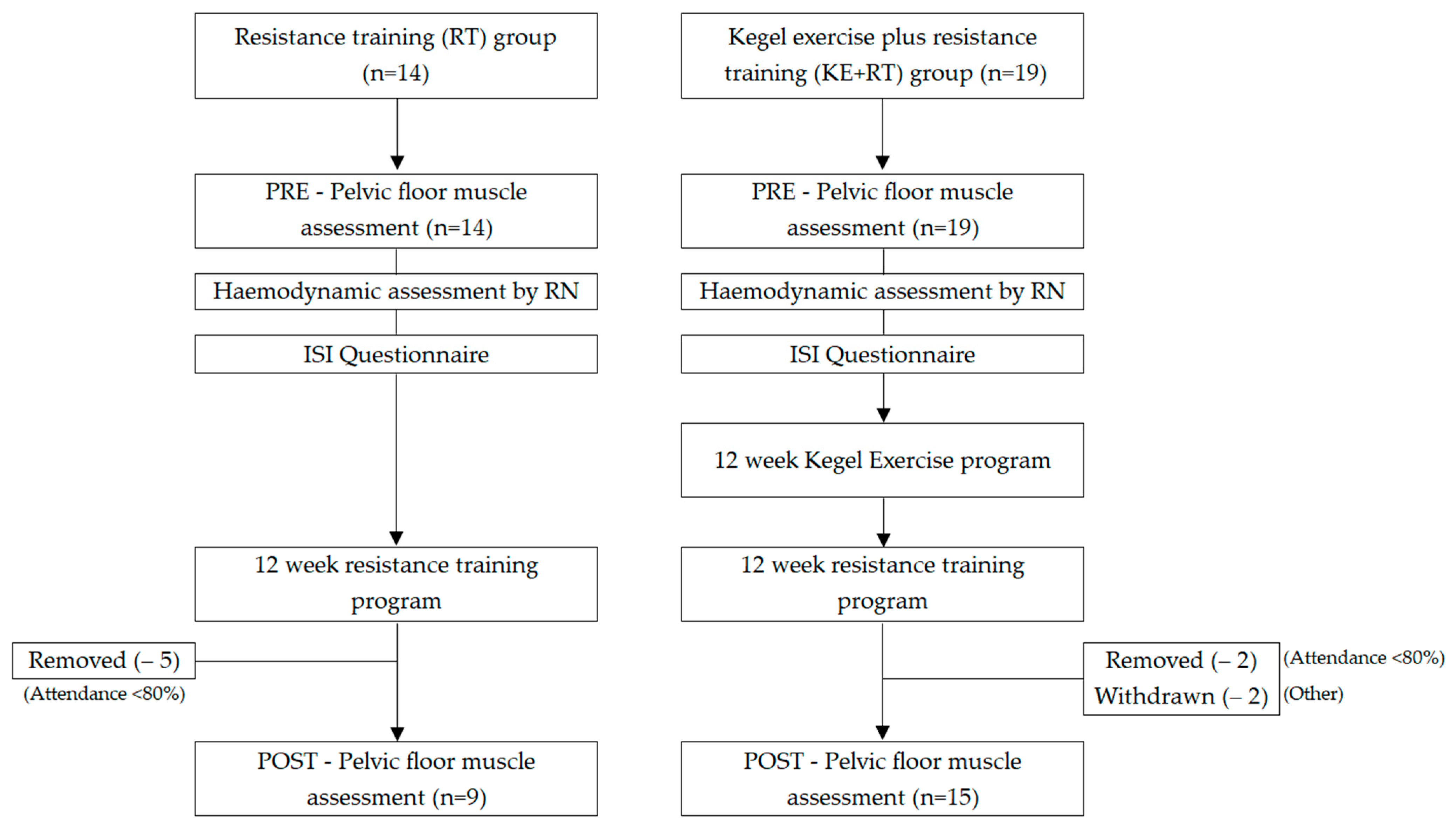
2.1. Study Design
2.2. Study Sample
2.3. Study Interventions
2.4. Study Procedure
2.5. Outcome Measures
2.6. Other Assessment
2.7. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milsom, I.; Gyhagen, M. The prevalence of urinary incontinence. Climacteric 2019, 22, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, B.S.; Lapitan, M.C.M. Prevalence of Urinary Incontinence in Men, Women, and Children—Current Evidence: Findings of the Fourth International Consultation on Incontinence. Urology 2010, 76, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Abufaraj, M.; Xu, T.; Cao, C.; Siyam, A.; Isleem, U.; Massad, A.; Soria, F.; Shariat, S.; Sutcliffe, S.; Yang, L. Prevalence and trends in urinary incontinence among women in the United States, 2005–2018. Am. J. Obstet. Gynecol. 2021, 225, 166.e1–166.e12. [Google Scholar] [CrossRef] [PubMed]
- Rui, Q.Z.; Man, C.X.; Cui, F.; Jia, W.; Xiao, D.B.; Xie, H.J.; Shuang, W.B. Epidemiological survey of adult female stress urinary incontinence. BMC Women’s Health 2021, 21, 172. [Google Scholar]
- Almousa, S.; Van Loon, A.B. The prevalence of urinary incontinence in nulliparous female sportswomen: A systematic review. J. Sports Sci. 2019, 37, 1663–1672. [Google Scholar] [CrossRef]
- Yagmur, Y.; Gul, S. Urinary incontinence in women aged 40 and older: Its prevalence, risk factors, and effect on quality of life. Niger. J. Clin. Pract. 2021, 24, 186–192. [Google Scholar]
- Salvatore, S.; Serati, M.; Laterza, R.; Ucella, S.; Torella, M.; Bolis, P.F. The impact of urinary stress incontinence in young and middle-age women practising recreational sports activity: An epidemiological study. Br. J. Sports Med. 2009, 43, 1115–1119. [Google Scholar] [CrossRef]
- D’Ancona, C.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef]
- Liu, C.-H.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2010, CD002759-CD. [Google Scholar] [CrossRef] [Green Version]
- Leiros-Rodriguez, R.; Soto-Rodriguez, A.; Perez-Ribao, I.; Garcia-Soidan, J.L. Comparisons of the Health Benefits of Strength Training, Aqua-Fitness, and Aerobic Exercise for the Elderly. Rehabil. Res. Pract. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wikander, L.; Cross, D.; Gahreman, D.E. Prevalence of urinary incontinence in women powerlifters: A pilot study. Int. Urogynecol. J. 2019, 30, 2031–2039. [Google Scholar] [CrossRef]
- Magaldi, C.M.; Saraiva, A.; Franciulli, P.M.; Moreno, M.; Miranda, M.L.J.; Maifrino, L.B.M. The Influence of Physical Activity on Functional Performance and Urinary Incontinence in Elderly Women. J. Morphol. Sci. 2018, 35, 1–8. [Google Scholar] [CrossRef]
- Bo, K.; Haakstad, L.; Paulsen, G.; Rustaden, A. Does regular strength training cause urinary incontincence in overweight inactive women? A randomized controlled trial. Int. Urogynecol. J. 2021, 32, 2827–2834. [Google Scholar] [CrossRef]
- Wikander, L.; Kirshbaum, M.; Garhreman, D. Urinary Incontinence and Women CrossFit Competitors. Int. J. Women’s Health 2020, 12, 1189–1195. [Google Scholar] [CrossRef]
- Bourcier, A.P. Incontinence During Sports and Fitness Activities. In Pelvic Floor Re-Education Principles and Practice, 2nd ed.; Baessler, K., Burgio, K.L., Norton, P.A., Schüssler, B., Moore, K.H., Stanton, S.L., Eds.; Springer: London, UK, 2008; pp. 267–270. [Google Scholar]
- Hay-Smith, E.J.; Herderschee, R.; Dumoulin, C.; Herbison, G.P. Comparisons of approaches to pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst. Rev. 2011, 12, CD009508. [Google Scholar] [CrossRef]
- Cross, D.; Waheed, N.; Krake, M.; Gahreman, D. Effectiveness of supervised Kegel exercises using bio-feedback versus unsupervised Kegel exercises on stress urinary incontinence: A quasi-experimental study. Int. Urogynecol. J. 2022, 8, 1–8. [Google Scholar] [CrossRef]
- Dumoulin, C.; Cacciari, L.; Hay-Smith, J. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2018, 10, CD005654. [Google Scholar] [CrossRef]
- Bo, K.; Herbert, R. There is not yet strong evidence that exercise regimes other than pelvic floor muscle training can reduce stress urinary incontinence in women: A systematic review. J. Physiother. 2013, 59, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Tosun, O.; Mutlu, E.; Ergenoglu Yeniel, O.; Tosun, G.; Malkoc, M.; Askar, N.; Itil, I.M. Does pelvic floor muscle training abolish symptoms of urinary incontinence? A randomized controlled trial. Clin. Rehabil. 2015, 29, 525–537. [Google Scholar] [CrossRef]
- Kegel, A.H. Progressive resistance exercise in the functional restoration of the perineal muscles. Am. J. Obstet. Gynaecol. 1948, 56, 238–248. [Google Scholar] [CrossRef]
- Newman, D.K.; Wein, A.J. Office-based behavioral therapy for management of incontinence and other pelvic disorders. Urol. Clin. N. Am. 2013, 40, 613–635. [Google Scholar] [CrossRef] [PubMed]
- Pereira, V.; Correia, G.N.; Driusso, P. Individual and group pelvic floor muscle training versus no treatment in female stress urinary incontinence: A randomized controlled pilot study. Eur. J. Obstet. Gynaecol. 2011, 159, 465–471. [Google Scholar] [CrossRef]
- Romero-Franco, N.; Molina-Mula, J.; Bosch-Donate, E.; Casado, A. Therapeutic exercise to improve pelvic floor muscle function in a female sporting population: A systematic review and meta-analysis. Physiotherapy 2021, 113, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Quartly, E.; Hallam, T.; Kilbreath, S.; Refshauge, K. Strength and endurance of the pelvic floor muscles in continent women: An observational study. Physiotherapy 2010, 96, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, N.; Mohseni-Bandpei, M. Application of perineometer in the assessment of pelvic floor muscle strength and endurance: A reliability study. J. Bodyw. Mov. Ther. 2011, 15, 209–214. [Google Scholar] [CrossRef]
- Romero-Culleres, G.; Pena-Pitarch, E.; Jane-Feixas, C.; Vilaseca-Grane, A.; Montesinos, J.; Arnau, A. Reliability and diagnostic accuracy of a new vaginal dynamometer to measure pelvic floor muscle strength. Female Pelvic Med. Reconstr. Surg. 2020, 26, 514–519. [Google Scholar] [CrossRef]
- Pereira, V.S.; Santos, J.Y.C.E.; Correia, G.N.; Driusso, P. Translation and validation into Portuguese of a questionnaire to evaluate the severity of urinary incontinence. Rev. Bras. Ginecol. Obs. 2011, 33, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Virtuoso, J.F.; Menezes, E.C.; Mazo, G.Z. Effect of Weight Training with Pelvic Floor Muscle Training in Elderly Women with Urinary Incontinence. Res. Q. Exerc. Sport 2019, 90, 141–150. [Google Scholar] [CrossRef]
- Kucukkaya, B.; Kahyaoglu, S. Effectiveness of pelvic floor muscle and abdominal training in women with stress urinary incontinence. J. Psychol. Health Med. 2020, 26, 779–786. [Google Scholar] [CrossRef]
- Dos Santos, K.M.; DaRoza, T.; Mochizuki, L.; Arbieto, E.R.; DaLuz, S.C. Assessment of abdominal and pelvic floor muscle function among continent and incontinent athletes. Int. Urogynecol. J. 2019, 30, 693–699. [Google Scholar] [CrossRef]
- Marques, A.; Stothers, L.; Macnab, A. The status of pelvic floor muscle training for women. Can. Urol. Assoc. J. 2010, 4, 419–424. [Google Scholar] [CrossRef]
- Pires, T.F.; Pires, P.M.; Moreira, M.H.; Gabriel, R.; Viana, S.A.; Viana, R.A. Assessment of pelvic floor muscles in sportswomen: Quality of life and related factors. Phys. Ther. Sport 2020, 43, 151–156. [Google Scholar] [CrossRef]
- Ree, M.L.; Nygaard, I.; Bo, K. Muscular fatigue in the pelvic floor muscles after strenuous physical activity. Acta Obstet. Et Gynaecol. Scand. 2007, 86, 870–876. [Google Scholar]
- Opara, J.A.; Socha, T.; Poswiata, A. Pelvic floor muscle exercise as the best stress urinary incontinence prevention method in women practising competitive sport. Physiotherapy 2013, 21, 57–63. [Google Scholar] [CrossRef]
- Dumoulin, C.; Glazener, C.; Jenkinson, D. Determining the optimal pelvic floor muscle training regimen for women with stress urinary incontinence. Neurourol. Urodyn. 2011, 30, 746–753. [Google Scholar] [CrossRef]
- Grewar, H.; McLean, L. The integrated continence system: A manual therapy approach to the treatment of stress urinary incontinence. Man. Ther. 2008, 13, 375–386. [Google Scholar] [CrossRef]
- Madill, S.; McLean, L. Relationship between abdominal and pelvic floor muscle activation and intravaginal pressure during pelvic floor muscle contractions in healthy continent women. J. Neurol. Urodyn. 2006, 25, 722–730. [Google Scholar] [CrossRef]
- Madill, S.J.; McLean, L. Quantification of abdominal and pelvic floor muscle synergies in response to voluntary pelvic floor muscle contractions. J. Electromyogr. Kinesiol. 2008, 18, 955–964. [Google Scholar] [CrossRef]
- Ferla, L.; Paiva, L.; Darki, C.; Vieira, A. Comparison of the functionality of pelvic floor muscles in women who practice the Pilates method and sedentary women: A pilot study. Int. Urogynaecological J. 2016, 27, 123–128. [Google Scholar] [CrossRef]
- Bo, K.; Nygaard, I. Is physical activity good or bad for the female pelvic floor? A narrative review. Sports Med. 2020, 50, 471–484. [Google Scholar] [CrossRef] [Green Version]
- Sheng, Y.; Carpenter, J.S.; Ashton-Miller, J.A.; Miller, J. Mechanisms of pelvic floor muscle training for managing urinary incontinence in women: A scoping review. BMC Women’s Health 2022, 22, 1–161. [Google Scholar] [CrossRef] [PubMed]
- Wikander, L.; Kirshbaum, M.N.; Waheed, N.; Gahreman, D.E. Urinary Incontinence in Competitive Women Powerlifters: A Cross-Sectional Survey. Sports Med. Open 2021, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Braekken, I.H.; Majida, M.; Engh, M.E.; Bo, K. Are Pelvic Floor Muscle Thickness and Size of Levator Hiatus Associated With Pelvic Floor Muscle Strength, Endurance and Vaginal Resting Pressure in Women With Pelvic Organ Prolapse Stages I-III? A Cross Sectional 3D Ultrasound Study. Neurourol. Urodyn. 2014, 33, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, I.; Shaw, J.; Egger, M. Exploring the association between lifetime physical activity and pelvic floor disorders: Study and design challenges. Contemp. Clin. Trials 2012, 33, 819–827. [Google Scholar] [CrossRef]


{kind=link}
| Warm Up Reps | Sets | Deadlift (kg) | Squat (kg) | Rest Time (mins) | ||
|---|---|---|---|---|---|---|
| Lead up weeks | training specific to individual’s capabilities | |||||
| Week 4 | Session 1 | 10, 10 | 3 × 10 | 40 | 27.5 | 8 |
| Session 2 | 25 | 22.5 | 8 | |||
| Week 5 | Session 1 | 10, 10 | 3 × 10 | 45 | 20 | 8 |
| Session 2 | 27.5 | 27.5 | 8 | |||
| Week 6 | Session 1 | 8, 5, 5 | 3 × 8 | 50 | 22.5 | 8 |
| Session 2 | 30 | 35 | 8 | |||
| Week 7 | Session 1 | 8, 5, 5 | 3 × 8 | 55 | 22.5 | 8 |
| Session 2 | 32.5 | 40 | 8 | |||
| Week 8 | Session 1 | 6, 5, 3 | 3 × 6 | 60 | 25 | 8 |
| Session 2 | 35 | 42.5 | 8 | |||
| Week 9 | Session 1 | 6, 5, 3 | 3 × 6 | 65 | 25 | 8 |
| Session 2 | 35 | 45 | 8 | |||
| Week 10 | Session 1 | 5, 3, 2 | 3 × 5 | 70 | 27.5 | 10 |
| Session 2 | 37.5 | 47.5 | 10 | |||
| Week 11 | Session 1 | 5, 3, 2 | 3 × 5 | 75 | 27.5 | 10 |
| Session 2 | 37.5 | 50 | 10 | |||
| Week 12 | Session 1 | 5, 3, 1, 1 | 2 × 2 | 85 | 27.5 | 12 |
| Session 2 | 37.5 | 60 | 12 | |||
| Resistance Training (RT) Group (n = 9) | Kegel Exercise + Resistance Training (KE + RT) Group (n = 15) | |||||
|---|---|---|---|---|---|---|
| Pre | Post | ES | Pre | Post | ES | |
| ISI Total score | 2.89 ± 0.93 | 1.44 ± 0.73 | 1.73 * | 4.53 ± 3.31 | 1.60 ± 1.50 | 1.14 * |
| - Frequency | 2.33 ± 0.71 | 1.44 ± 0.73 | 1.24 * | 2.60 ± 0.91 | 1.33 ± 0.91 | 1.34 * |
| - Severity | 1.33 ± 0.50 | 1.00 ± 0.00 | 0.94 * | 1.67 ± 0.72 | 1.00 ± 0.53 | 1.11 * |
| PF at rest (cm H2O) | 31.17 ± 13.76 | 31.11 ± 10.24 | 0.005 | 32.71 ± 13.56 | 30.11 ± 8.03 | 0.23 |
| PF_attempts (Average) | 45.10 ± 20.71 | 66.32 ± 20.36 | 1.03 * | 27.38 ± 12.00 | 38.35 ± 12.65 | 0.89 * |
| MVC @80% | 18.33 ± 5.00 | 17.33 ± 5.39 | 0.19 | 14.00 ± 6.78 | 16.93 ± 5.38 | 0.48 |
| BMI kg/m2 | 28.31 ± 4.64 | 28.62 ± 4.67 | 0.07 | 25.28 ± 4.88 | 25.74 ± 5.18 | 0.09 |
| Fat Mass kg | 31.79 ± 11.47 | 30.20 ± 10.45 | 0.14 | 23.47 ± 8.95 | 22.23 ± 9.18 | 0.14 |
| Muscle Mass kg | 43.79 ± 4.16 | 46.19 ± 3.19 | 0.65 * | 41.69 ± 3.65 | 44.00 ± 4.08 | 0.60 * |
| df | Mean Square | F | Sig. | Partial ETA Squared | ||
|---|---|---|---|---|---|---|
| URINARY INCONTINENCE FACTORS | ||||||
| UI: Frequency | Interaction | 1, 22 | 0.4 | 1.8 | 1.94 | 0.76 |
| Condition | 1, 22 | 0.07 | 0.05 | 0.82 | 0 | |
| Time effect | 1, 22 | 13.07 | 58.54 | 0.00 * | 0.73 | |
| UI: Severity | Interaction | 1, 22 | 0.31 | 1.47 | 0.24 | 0.06 |
| Condition | 1, 22 | 0.31 | 0.79 | 0.38 | 0.03 | |
| Time effect | 1, 22 | 2.81 | 13.26 | 0.00 * | 0.38 | |
| Total ISI Score (frequency*severity) | Interaction | 1, 22 | 6.24 | 3 | 0.1 | 0.12 |
| Condition | 1,22 | 9.11 | 1.33 | 0.26 | 0.57 | |
| Time effect | 1, 22 | 53.9 | 26.02 | 0.00 * | 0.54 | |
| Average PF muscle strength | Interaction | 1, 22 | 295.89 | 2.84 | 0.11 | 0.11 |
| Condition | 1, 22 | 5871.71 | 14.83 | 0.00 * | 0.4 | |
| Time effect | 1, 22 | 2913.86 | 27.99 | 0.00 * | 0.56 | |
| PF resting pressure | Interaction | 1, 22 | 243.54 | 4.54 | 0.04 * | 0.14 |
| Condition | 1, 22 | 0.62 | 0 | 0.96 | 0 | |
| Time effect | 1, 22 | 37.04 | 0.69 | 0.41 | 0.02 | |
| MVC of PF at 80% | Interaction | 1, 22 | 43.51 | 2.06 | 0.17 | 0.85 |
| Condition | 1, 22 | 63.01 | 1.36 | 0.26 | 0.06 | |
| Time effect | 1, 22 | 10.51 | 0.5 | 0.49 | 0.02 | |
| PHYSICAL HEALTH | ||||||
| Weight | Interaction | 1, 22 | 0.24 | 0.1 | 0.76 | 0.01 |
| Condition | 1, 22 | 1220.7 | 3.69 | 0.07 | 0.14 | |
| Time effect | 1, 22 | 13.64 | 5.72 | 0.03 * | 0.21 | |
| BMI | Interaction | 1, 22 | 0.02 | 0.18 | 0.68 | 0.01 |
| Condition | 1, 22 | 98.35 | 2.06 | 0.17 | 0.09 | |
| Time effect | 1, 22 | 1.67 | 4.73 | 0.04 * | 0.18 | |
| Muscle Mass (kg) | Interaction | 1, 22 | 0.03 | 0.01 | 0.91 | 0 |
| Condition | 1, 22 | 51.63 | 1.89 | 0.18 | 0.08 | |
| Time effect | 1, 22 | 62.31 | 36.14 | 0.00 * | 0.62 | |
| Fat Mass (kg) | Interaction | 1, 22 | 0.34 | 0.09 | 0.77 | 0 |
| Condition | 1, 22 | 746.85 | 3.97 | 0.06 | 0.15 | |
| Time effect | 1, 22 | 22.51 | 5.86 | 0.02 * | 0.21 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cross, D.; Kirshbaum, M.N.; Wikander, L.; Tan, J.-Y.; Moss, S.; Gahreman, D. Does a Kegel Exercise Program Prior to Resistance Training Reduce the Risk of Stress Urinary Incontinence? Int. J. Environ. Res. Public Health 2023, 20, 1481. https://doi.org/10.3390/ijerph20021481
Cross D, Kirshbaum MN, Wikander L, Tan J-Y, Moss S, Gahreman D. Does a Kegel Exercise Program Prior to Resistance Training Reduce the Risk of Stress Urinary Incontinence? International Journal of Environmental Research and Public Health. 2023; 20(2):1481. https://doi.org/10.3390/ijerph20021481
Chicago/Turabian StyleCross, Donelle, Marilynne N. Kirshbaum, Lolita Wikander, Jing-Yu (Benjamin) Tan, Simon Moss, and Daniel Gahreman. 2023. "Does a Kegel Exercise Program Prior to Resistance Training Reduce the Risk of Stress Urinary Incontinence?" International Journal of Environmental Research and Public Health 20, no. 2: 1481. https://doi.org/10.3390/ijerph20021481