
A Community-Based Participatory Framework to Co-Develop Patient Education Materials (PEMs) for Rare Diseases: A Model Transferable across Diseases
 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Background
2. Materials and Methods
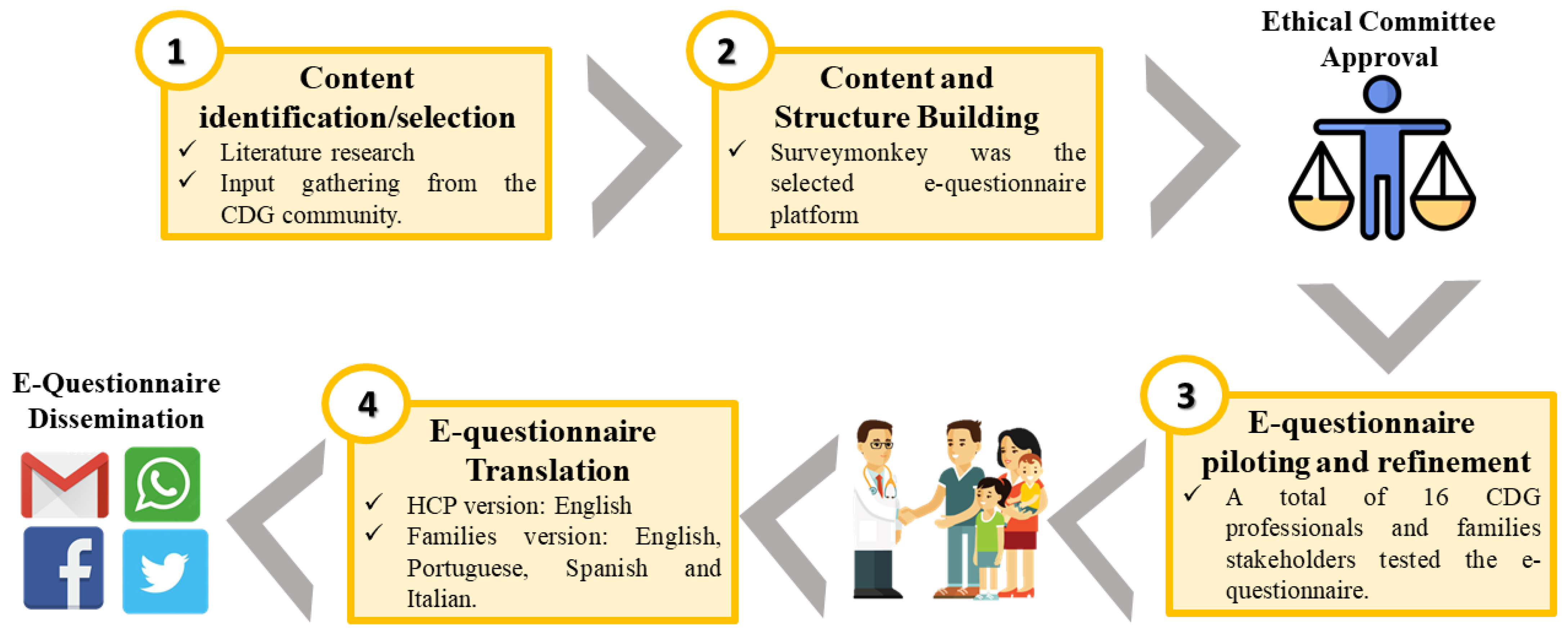
2.1. Assessing Families’ Information Needs: CDG Journey Mapping Questionnaire
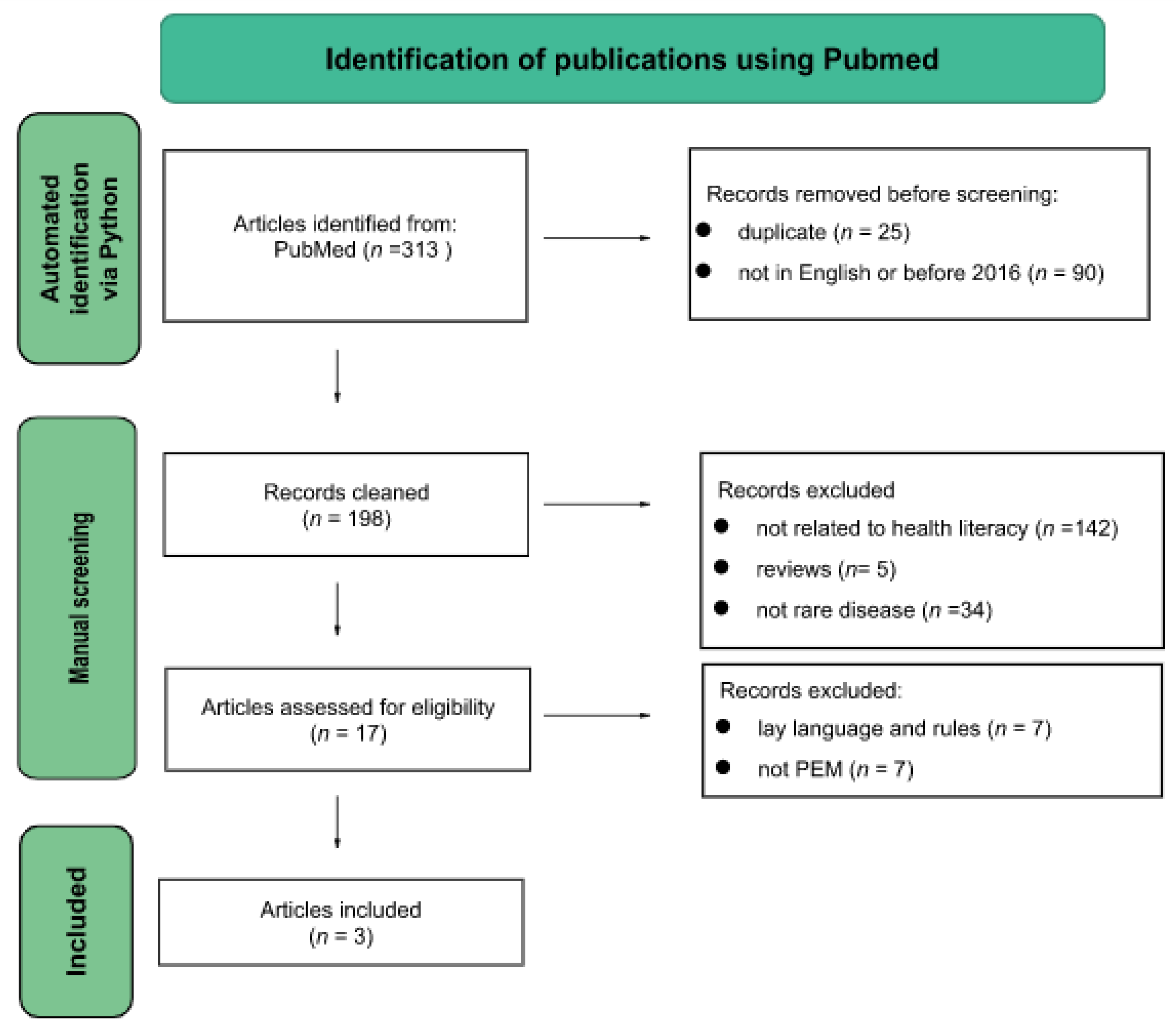
2.2. Literature Search on Frameworks for the Development of PEMs
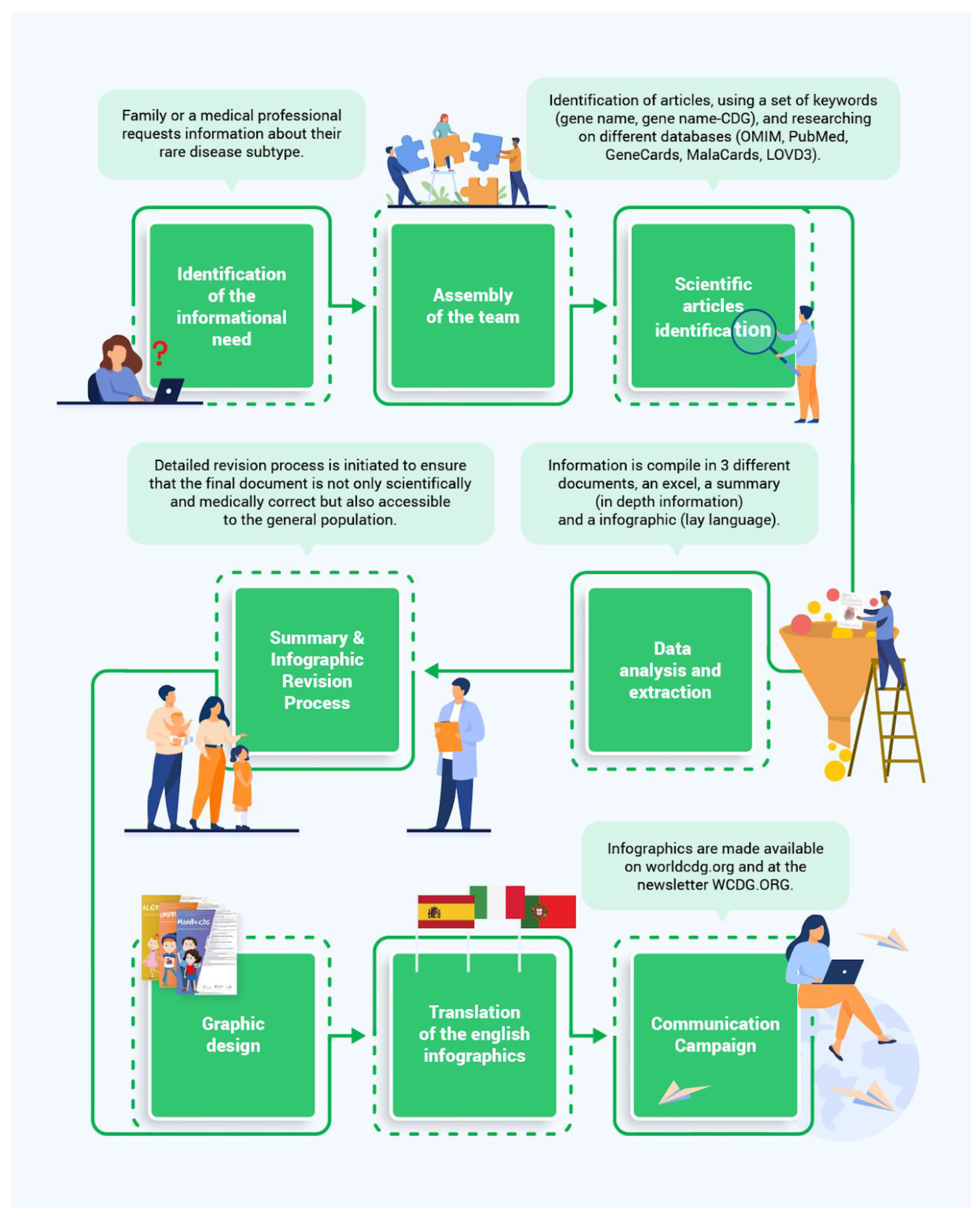
2.3. Community-Based Framework to Develop Patient Education Materials
Set Up of a Community-Based Framework
- Identification of the informational need
- 2.
- Assembly of the team
- 3.
- Scientific article identification, and data analysis and extraction
- 4.
- Revision process
- 5.
- Graphic design
- 6.
- Translation of the English infographics
- 7.
- Communication campaigns
3. Results
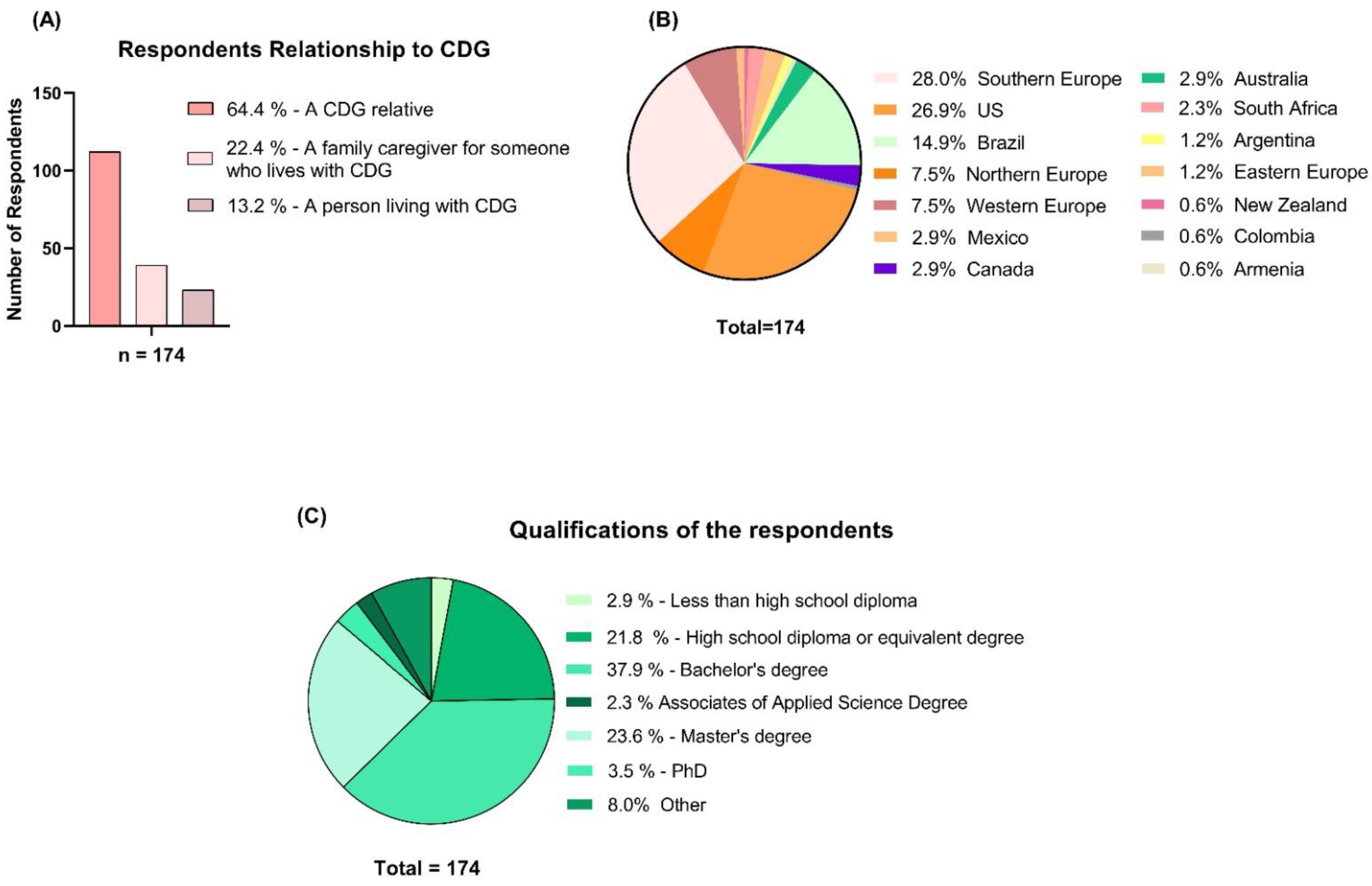
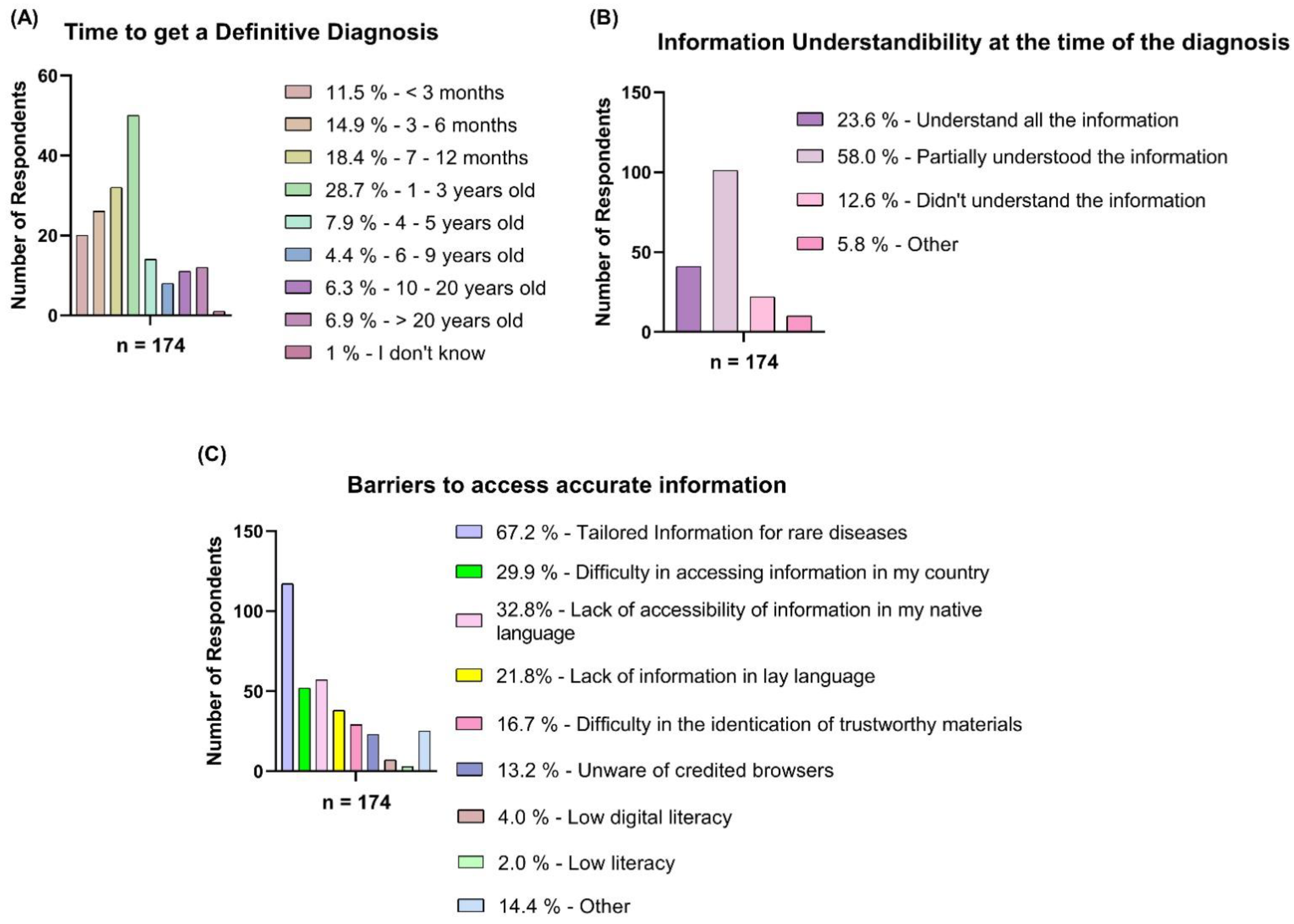
3.1. CDG Community Information Needs
3.2. Existence of Frameworks for PEMs
3.3. Implementation of the Created Community-Centric Framework in CDG
4. Discussion
4.1. Study Strengths and Limitations
4.2. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parnell, T.A. Health Literacy: History, Definitions, and Models. Health Literacy in Nursing; Springer Publishing Company: Berlin, Germany, 2018. [Google Scholar]
- Frisch, A.L.; Camerini, L.; Diviani, N.; Schulz, P.J. Defining and measuring health literacy: How can we profit from other literacy domains? Health Promot Int. 2012, 27, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson-Pant, A. Promoting Health and Literacy for Women’s Empowerment; UNESCO Institute for Lifelong Learning: Hamburg, Germany, 2016. [Google Scholar]
- Speros, C.; Aprn, D. Health literacy: Concept analysis. J. Adv. Nurs. 2005, 50, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Bresolin, L.B. Health literacy: Report of the council on scientific affairs. JAMA 1999, 281, 552–557. [Google Scholar]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2006, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US): Committee on Health Literacy. Health Literacy: A Prescription to End Confusion; Nielsen-Bohlman, L., Panzer, A.M., Kindig, D.A., Eds.; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Kickbusch, I.; Wait, S.; Maag, D. Navigating Health: The Role of Health Literacy; Alliance for Health and the Future International Longevity Centre-UK: London, UK, 2006. [Google Scholar]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Elaborating a definition of health literacy: A commentary. J. Health Commun. 2003, 8, 119–120. [Google Scholar] [CrossRef]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Advancing Health Literacy: A Framework for Understanding and Action; John Wiley & Sons: Hoboken, NJ, USA, 2006. [Google Scholar]
- McCabe, J.A. An assignment for building an awareness of the intersection of health literacy and cultural competence skills. J. Med. Libr. Assoc. 2006, 94, 458–461. [Google Scholar] [PubMed]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Together for Health-A Strategic Approach for the EU 2008–2013. 2007. Available online: http://ec.europa.eu/health/ph_overview/strategy/health_strategy_en.htm (accessed on 22 November 2022).
- Bielefeld University. Programmes for Training on Research in Public Health for South Eastern Europe. Available online: https://biecoll.ub.uni-bielefeld.de/index.php/publichealth/article/view/450/545 (accessed on 22 November 2022).
- Irving, R.; Deborah, G.-E.; Canadian Public Health Association. Expert Panel on Health Literacy, Gibson Library Connections; A vision for a health literate Canada: Report of the Expert Panel on Health Literacy; Canadian Public Health Association: Ottawa, ON, Canada, 2008. [Google Scholar]
- Ishikawa, H.; Yano, E. Patient health literacy and participation in the health-care process. Health Expect. 2008, 11, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, J.M. Health literacy: A concept/dimensional analysis. Nurs. Health Sci. 2008, 10, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Adult Literacy and Life Skills Survey, Summary Results 2006. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4228.0Main+Features12006%20(Reissue) (accessed on 22 November 2022).
- Yost, K.J.; Webster, K.; Baker, D.W.; Choi, S.W.; Bode, R.K.; Hahn, E.A. Bilingual health literacy assessment using the Talking Touchscreen/la Pantalla Parlanchina: Development and pilot testing. Patient Educ. Couns. 2009, 75, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Stocks, N.P.; Hill, C.L.; Gravier, S.; Kickbusch, L.; Beilby, J.J.; Wilson, D.H.; Adams, R.J. Health literacy—A new concept for general practice? Aust. Fam. Physician 2009, 38, 144–147. [Google Scholar]
- Adkins, N.R.; Corus, C. Health Literacy for Improved Health Outcomes: Effective Capital in the Marketplace. J. Consum. Aff. 2009, 43, 199–222. [Google Scholar] [CrossRef]
- Freedman, D.A.; Bess, K.D.; Tucker, H.A.; Boyd, D.L.; Tuchman, A.M.; Wallston, K.A. Public Health Literacy Defined. Am. J. Prev. Med. 2009, 36, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health literacy: What is it? J. Health Commun. 2010, 15, 9–19. [Google Scholar] [CrossRef]
- Rosenbaum, S. The Patient Protection and Affordable Care Act: Implications for Public Health Policy and Practice. Public Health Rep. 2011, 126, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Office of the Assistant Secretary for Health. Available online: https://health.gov/healthypeople/priority-areas/health-literacy-healthy-people-2030 (accessed on 22 November 2022).
- Poureslami, I.; Kopec, J.; Tregobov, N.; Shum, J.; Sawatzky, R.; Hohn, R.; FitzGerald, J.M. An Integrated Framework to Conceptualize and Develop the Vancouver Airways Health Literacy Tool (VAHLT). Int. J. Environ. Res. Public Health 2021, 18, 8646. [Google Scholar] [CrossRef]
- Kickbusch, I.; Pelikan, J.M.; Apfel, F.; Tsouros, A.D. Health Literacy: The Solid Facts; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Hou, W.-H.; Huang, Y.-J.; Lee, Y.; Chen, C.-T.; Lin, G.-H.; Hsieh, C.-L. Validation of the Integrated Model of Health Literacy in Patients with Breast Cancer. Cancer Nurs. 2018, 41, 498–505. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/healthliteracy/shareinteract/TellOthers.html (accessed on 22 November 2022).
- Gazmararian, J.A.; Williams, M.V.; Peel, J.; Baker, D.W. Health literacy and knowledge of chronic disease. Patient Educ. Couns. 2003, 51, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Bennett, I.M.; Chen, J.; Soroui, J.S.; White, S. The Contribution of Health Literacy to Disparities in Self-Rated Health Status and Preventive Health Behaviors in Older Adults. Ann. Fam. Med. 2009, 7, 204–211. [Google Scholar] [CrossRef]
- White, S.; Chen, J.; Atchison, R. Relationship of preventive health practices and health literacy: A national study. Am. J. Health Behav. 2007, 32, 227–242. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; Riekert, K.A.; Bilderback, A.; Chanmugam, A.; Hill, P.; Rand, C.S.; Brancati, F.L.; Krishnan, J.A. Tailored Education May Reduce Health Literacy Disparities in Asthma Self-Management. Am. J. Respir. Crit. Care Med. 2005, 172, 980–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, T.C.; Wolf, M.S.; Bass, P.F.; Thompson, J.A.; Tilson, H.H.; Neuberger, M.; Parker, R. Literacy and Misunderstanding Prescription Drug Labels. Ann. Intern. Med. 2006, 145, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.D.; Tu, W.; Wu, J.; Morrow, D.; Smith, F.; Brater, D.C. Factors Associated With Exacerbation of Heart Failure Include Treatment Adherence and Health Literacy Skills. Clin. Pharmacol. Ther. 2009, 85, 651–658. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Sys-tematic Review. Ann. Intern. Med. 2011, 155, 97. [Google Scholar] [CrossRef]
- King, A. Poor health literacy: A ‘hidden’ risk factor. Nat. Rev. Cardiol. 2010, 7, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Ohio University—College of Health Sciences and Professions. Available online: https://onlinemasters.ohio.edu/blog/how-to-improve-health-literacy/ (accessed on 22 November 2022).
- Fleary, S.A.; Ettienne, R. Social Disparities in Health Literacy in the United States. HLRP Health Lit. Res. Pract. 2019, 3, e47–e52. [Google Scholar] [CrossRef]
- Watson, J.C. Talking the Talk: Enhancing Clinical Ethics with Health Literacy Best Practices. HEC Forum 2019, 31, 177–199. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. Health Literacy Improvement Tools. 2022. Available online: https://www.ahrq.gov/health-literacy/improve/index.html (accessed on 22 November 2022).
- Shoemaker, S.J.; Wolf, M.S.; Brach, C. Development of the Patient Education Materials Assessment Tool (PEMAT): A new measure of understandability and actionability for print and audiovisual patient information. Patient Educ. Couns. 2014, 96, 395–403. [Google Scholar] [CrossRef] [Green Version]
- WHO Regional Office for Europe. Regional Committee for Europe Draft WHO European Roadmap for Implementation of Health Literacy Initiatives through the Life Course; WHO Regional Office for Europe: Brussels, Belgium, 2019. [Google Scholar]
- Centers for Disease Control and Prevention. Simply Put A Guide for Creating Easy-to-Understand Materials; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010.
- CDG World Organization. Available online: https://worldcdg.org/advocacy/empowerment-all (accessed on 22 November 2022).
- Sorensen, K. Health Literacy: A Neglected European Public Health Disparity. Ph.D. Thesis, Maastricht University, Maastricht, The Netherlands, November 2013. [Google Scholar] [CrossRef]
- Betschart, P.; Staubli, S.E.; Zumstein, V.; Babst, C.; Sauter, R.; Schmid, H.-P.; Abt, D. Improving Patient Education Materials: A Practical Algorithm from Development to Validation. Curr. Urol. 2019, 13, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Badiu, C.; Bonomi, M.; Borshchevsky, I.; Cools, M.; Craen, M.; Ghervan, C.; Hauschild, M.; Hershkovitz, E.; Hrabovszky, E.; Juul, A.; et al. Developing and evaluating rare disease educational materials co-created by expert clinicians and patients: The paradigm of congenital hypogonadotropic hypogonadism. Orphanet J. Rare Dis. 2017, 12, 57. [Google Scholar] [CrossRef] [Green Version]
- Cardão, C.; Barros, L.; Francisco, R.; Silva, D.; Ferreira, V.R. Experiences of parents with children with congenital disorders of gly-cosylation: What can we learn from them? Disabil. Health J. 2021, 14, 101065. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, C.; dos Reis, V.; Silva, S.; Videira, P.A.; Morava, E.; Jaeken, J. Public and patient involvement in needs assessment and social innovation: A people-centred approach to care and research for congenital disorders of glycosylation. BMC Health Serv. Res. 2017, 17, 682. [Google Scholar] [CrossRef] [Green Version]
- Marques-Da-Silva, D.; Ferreira, V.D.R.; Monticelli, M.; Janeiro, P.; Videira, P.A.; Witters, P.; Jaeken, J.; Cassiman, D. Liver involvement in congenital disorders of glycosylation (CDG). A systematic review of the literature. J. Inherit. Metab. Dis. 2017, 40, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Francisco, R.; Pascoal, C.; Marques-da-Silva, D.; Morava, E.; Gole, G.A.; Coman, D.; Jaeken, J.; dos Reis Ferreira, V. Keeping an eye on congenital disorders of O-glycosylation: A systematic literature review. J. Inherit Metab. Dis. 2019, 42, 29–48. [Google Scholar] [CrossRef]
- Dorough, A.; Narendra, J.H.; Wilkie, C.; Hegde, A.; Swain, K.; Chang, E.H.; Oliver, T.; Flythe, J.E. Stakeholder-Guided Development of Dialysis Vascular Access Education Materials. Kidney360 2021, 2, 1115–1123. [Google Scholar] [CrossRef]
- Giguère, A.; Zomahoun, H.T.V.; Carmichael, P.-H.; Uwizeye, C.B.; Légaré, F.; Grimshaw, J.M.; Gagnon, M.-P.; Auguste, D.U.; Massougbodji, J. Printed educational materials: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Grudniewicz, A.; Kealy, R.; Rodseth, R.N.; Hamid, J.; Rudoler, D.; Straus, S.E. What is the effectiveness of printed educational materials on primary care physician knowledge, behaviour, and patient outcomes: A systematic review and meta-analyses. Implement. Sci. 2015, 10, 164. [Google Scholar] [CrossRef] [Green Version]
- Francisco, R.; Alves, S.; Gomes, C.; Granjo, P.; Pascoal, C.; Brasil, S.; Neves, A.; Santos, I.; Miller, A.; Krasnewich, D.; et al. A Participatory Framework for Plain Language Clinical Management Guideline Development. Int. J. Environ. Res. Public Health 2022, 19, 13506. [Google Scholar] [CrossRef] [PubMed]
- Brasil, S.; Pascoal, C.; Francisco, R.; Ferreira, V.D.R.; Videira, P.A.; Valadão, G. Artificial intelligence (AI) in rare diseases: Is the future brighter? Genes 2019, 10, 978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walkowiak, D.; Domaradzki, J. Are rare diseases overlooked by medical education? Awareness of rare diseases among physicians in Poland: An explanatory study. Orphanet J. Rare Dis. 2021, 16, 400. [Google Scholar] [CrossRef] [PubMed]
- Zurynski, Y.; Gonzalez, A.; Deverell, M.; Phu, A.; Leonard, H.; Christodoulou, J.; Elliott, E. Rare disease: A national survey of paediatricians’ experiences and needs. BMJ Paediatr. Open 2017, 1, e000172. [Google Scholar] [CrossRef]
- Rare 2030. The Development and Market Launch of Orphan Drugs from 1980–2019: A Quantitative Analysis. Available online: https://download2.eurordis.org/rare2030/deliverables/D5.3%20R%26D%20and%20market%20launch%20of%20orphan%20drugs.pdf (accessed on 22 November 2022).
- Bruce, I.A.; Ezgü, F.S.; Kampmann, C.; Kenis, V.; Mackenzie, W.; Stevens, B.; Walker, R.; Hendriksz, C. Addressing the need for patient-friendly medical communications: Adaptation of the 2019 recommendations for the management of MPS VI and MPS IVA. Orphanet J. Rare Dis. 2022, 17, 91. [Google Scholar] [CrossRef]
- Zeltner, N.A.; Welsink-Karssies, M.M.; Landolt, M.A.; Bosshard-Bullinger, D.; Keller, F.; Bosch, A.M.; Groenendijk, M.; Grünert, S.C.; Karall, D.; Rettenbacher, B.; et al. Reducing complexity: Explaining inborn errors of metabolism and their treatment to children and adolescents. Orphanet J. Rare Dis. 2019, 14, 248. [Google Scholar] [CrossRef] [Green Version]
- Patient Innovation-Sharing Solutions, Improving Life. Available online: https://patient-innovation.com/post/4957?language=en (accessed on 22 November 2022).
- Francisco, R.; Pascoal, C.; Marques-Da-Silva, D.; Brasil, S.; Pimentel-Santos, F.M.; Altassan, R.; Jaeken, J.; Grosso, A.R.; Ferreira, V.D.R.; Videira, P.A. New Insights into Immunological Involvement in Congenital Disorders of Glycosylation (CDG) from a People-Centric Approach. J. Clin. Med. 2020, 9, 2092. [Google Scholar] [CrossRef]
- Arriaga, M.; Francisco, R.; Nogueira, P.; Oliveira, J.; Silva, C.; Câmara, G.; Sørensen, K.; Dietscher, C.; Costa, A. Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. Int. J. Environ. Res. Public Health 2022, 19, 4225. [Google Scholar] [CrossRef]
- Marques-Da-Silva, D.; Francisco, R.; Ferreira, V.D.R.; Forbat, L.; Lagoa, R.; Videira, P.A.; Witters, P.; Jaeken, J.; Cassiman, D. An Electronic Questionnaire for Liver Assessment in Congenital Disorders of Glycosylation (LeQCDG): A Patient-Centered Study. JIMD Rep. 2019, 44, 55–64. [Google Scholar] [CrossRef]
- Garcia-Codina, O.; Juvinyà-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; Gonzàlez, S.J.S.; Masachs-Fatjo, E.; Santaeugènia, S.J.; Magrinyà-Rull, P.; Saltó-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1112. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Published after 2016 | Health literacy papers mainly focusing on patient clinical management |
| Written in English | Reviews, open articles and similar articles, with the exception of those used for contextualization |
| Orphanet classification is used, and only rare diseases with orphacodes are accepted | |
| PEMs specific to a disease | |
| Frameworks related to the creation of the content from PEMs |
| Nationalities | Translators | Developers of the PEMs | Revisors and Validators | |
|---|---|---|---|---|
| Medical Professionals | Families | |||
| Portuguese | 2 | 8 | 1 | |
| Spanish | 3 | 2 | 1 | 2 |
| Italian | 2 | 1 | ||
| Italian/Swiss | 1 | |||
| Belgian | 1 | |||
| American | 4 | 6 | ||
| Brazilian | 2 | |||
| Canadian | 3 | |||
| Australian | 1 | |||
| Mexican | 1 | |||
| Turkish | 1 | |||
| British | 1 | |||
| German | 1 | |||
| Swedish | 1 | |||
| Total | 8 | 11 | 6 | 19 |
| Types of Glycosylation | Disease Designation(s) | Final Infographics per Language | |||
|---|---|---|---|---|---|
| English | Portuguese | Italian | Spanish | ||
| N-linked CDG | ALG1-CDG |  | - | ||
| ALG2-CDG | | - | | ||
| ALG3-CDG | | ||||
| ALG6-CDG | | ||||
| ALG8-CDG | | - | |||
| ALG9-CDG | | ||||
| ALG11-CDG | | ||||
| ALG12-CDG | | ||||
| FUT8-CDG | | ||||
| MAN1B1-CDG (Mental retardation 15) | | ||||
| RFT1-CDG | | ||||
| MOGS-CDG | | ||||
| MPI-CDG * | | ||||
| PMM2-CDG | | ||||
| SSR3-CDG | | ||||
| SSR4-CDG | | - | | ||
| GPI-biosynthesis defects | PIGA-CDG (Multiple congenital anomalies-hypotonia-seizures syndrome 2) | | - | | |
| PIGG-CDG (Mental retardation 53) | | ||||
| PIGN-CDG (Multiple congenital anomalies-hypotonia-seizures syndrome 1 (milder phenotype) | | ||||
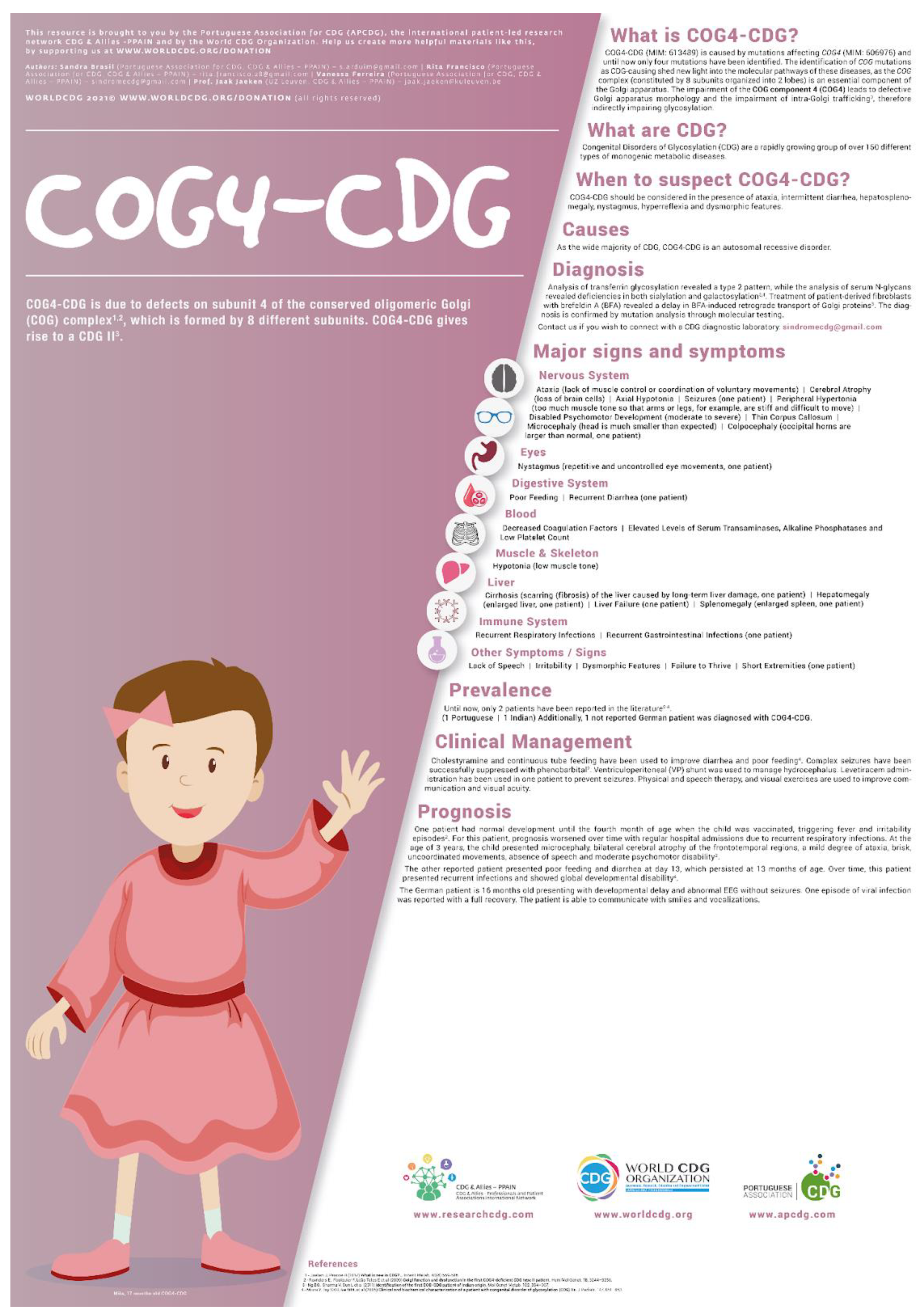
| Disorders of multiple glycosylation pathways | COG4-CDG | | |||
| COG5-CDG | | - | | | |
| COG6-CDG | | ||||
| DOLK-CDG | | ||||
| DPM1-CDG | | - | | ||
| DPM2-CDG | | - | | ||
| GMPPA-CDG (Alacrima, achalasia, and mental retardation syndrome) | | ||||
| MPDU1-CDG | | - | | ||
| NANS-CDG (Spondyloepimetaphyseal dysplasia, Camera-Genevieve type) | | ||||
| PGM1-CDG | | ||||
| SLC35A2-CDG (epileptic encephalopathy) (high incidence of de novo variants) | | ||||
| SLC39A8-CDG | | - | | ||
| O-linked CDG | B4GALT7-CDG (Ehlers–Danlos syndrome, spondylodysplastic type, 1) | | - | | |
| Total | 32 | 23 | 30 | 29 | |
: Finished infographics.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falcão, M.; Allocca, M.; Rodrigues, A.S.; Granjo, P.; Francisco, R.; Pascoal, C.; Rossi, M.G.; Marques-da-Silva, D.; Magrinho, S.C.M.; Jaeken, J.; et al. A Community-Based Participatory Framework to Co-Develop Patient Education Materials (PEMs) for Rare Diseases: A Model Transferable across Diseases. Int. J. Environ. Res. Public Health 2023, 20, 968. https://doi.org/10.3390/ijerph20020968
Falcão M, Allocca M, Rodrigues AS, Granjo P, Francisco R, Pascoal C, Rossi MG, Marques-da-Silva D, Magrinho SCM, Jaeken J, et al. A Community-Based Participatory Framework to Co-Develop Patient Education Materials (PEMs) for Rare Diseases: A Model Transferable across Diseases. International Journal of Environmental Research and Public Health. 2023; 20(2):968. https://doi.org/10.3390/ijerph20020968
Chicago/Turabian StyleFalcão, Marta, Mariateresa Allocca, Ana Sofia Rodrigues, Pedro Granjo, Rita Francisco, Carlota Pascoal, Maria Grazia Rossi, Dorinda Marques-da-Silva, Salvador C. M. Magrinho, Jaak Jaeken, and et al. 2023. "A Community-Based Participatory Framework to Co-Develop Patient Education Materials (PEMs) for Rare Diseases: A Model Transferable across Diseases" International Journal of Environmental Research and Public Health 20, no. 2: 968. https://doi.org/10.3390/ijerph20020968