
Persistent Increase of Sympathetic Activity in Post-Acute COVID-19 of Paucisymptomatic Healthcare Workers
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Autonomic Cardiac Balance, HRV Parameters, and Blood Pressure
3. Sample Size Estimation
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 13 June 2022).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Triassi, M.; Pennino, F. Infectious Risk for Healthcare Workers: Evaluation and Prevention. Ann. Di. Ig. Med. Prev. E Comunità. 2018, 30, 48–51. [Google Scholar] [CrossRef]
- Porru, S.; Monaco, M.G.L.; Spiteri, G.; Carta, A.; Pezzani, M.D.; Lippi, G.; Gibellini, D.; Tacconelli, E.; Dalla Vecchia, I.; Sala, E.; et al. SARS-CoV-2 Breakthrough Infections: Incidence and Risk Factors in a Large European Multicentric Cohort of Health Workers. Vaccines 2022, 10, 1193. [Google Scholar] [CrossRef]
- Becker, R.C. Autonomic Dysfunction in SARS-COV-2 Infection Acute and Long-Term Implications COVID-19 Editor’s Page Series. J. Thromb. Thrombolysis. 2021, 52, 692–707. [Google Scholar] [CrossRef]
- Bisaccia, G.; Ricci, F.; Recce, V.; Serio, A.; Iannetti, G.; Chahal, A.A.; Ståhlberg, M.; Khanji, M.Y.; Fedorowski, A.; Gallina, S. Post-Acute Sequelae of COVID-19 and Cardiovascular Autonomic Dysfunction: What Do We Know? J. Cardiovasc. Dev. Dis. 2021, 8, 156. [Google Scholar] [CrossRef]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Lindmark, K.; Connolly, A.-M.F. Risk of Acute Myocardial Infarction and Ischaemic Stroke Following COVID-19 in Sweden: A Self-Controlled Case Series and Matched Cohort Study. Lancet 2021, 398, 599–607. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-Term Cardiovascular Outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Vasudeva, R.; Challa, A.; Al Rifai, M.; Polana, T.; Duran, B.; Vindhyal, M.; Lewis, E.F. Prevalence of Cardiovascular Diseases in COVID-19 Related Mortality in the United States. Prog. Cardiovasc. Dis. 2022, 74, 122–126. [Google Scholar] [CrossRef]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Qusti, S.; Alshammari, E.M.; Gyebi, G.A.; Batiha, G.E.-S. Covid-19-Induced Dysautonomia: A Menace of Sympathetic Storm. ASN Neuro. 2021, 13, 17590914211057636. [Google Scholar] [CrossRef]
- Liviero, F.; Campisi, M.; Mason, P.; Pavanello, S. Transient Receptor Potential Vanilloid Subtype 1: Potential Role in Infection, Susceptibility, Symptoms and Treatment of COVID-19. Front. Med. 2021, 8, 753819. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart Rate Variability: Standards of Measurement, Physiological Interpretation, and Clinical Use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Fang, S.-C.; Wu, Y.-L.; Tsai, P.-S. Heart Rate Variability and Risk of All-Cause Death and Cardiovascular Events in Patients With Cardiovascular Disease: A Meta-Analysis of Cohort Studies. Biol. Res. Nurs. 2020, 22, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The Relationship of Autonomic Imbalance, Heart Rate Variability and Cardiovascular Disease Risk Factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, H.; Larson, M.G.; Venditti, F.J.; Manders, E.S.; Evans, J.C.; Feldman, C.L.; Levy, D. Impact of Reduced Heart Rate Variability on Risk for Cardiac Events. Circulation 1996, 94, 2850–2855. [Google Scholar] [CrossRef] [Green Version]
- Kaliyaperumal, D.; Rk, K.; Alagesan, M.; Ramalingam, S. Characterization of Cardiac Autonomic Function in COVID-19 Using Heart Rate Variability: A Hospital Based Preliminary Observational Study. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Topal, D.; Uğuz, B.; ZengïN, İ.; Coşar, S.; TïRyakïOğlu, S. Heart Rate Variability in Hospitalized Patients with Suspected or Confirmed Diagnosis of COVID-19: A Retrospective Analysis in Comparison to Healthy Controls and in Relation to Proinflammatory Cytokines. Celal. Bayar. Üniversitesi. Sağlık. Bilim. Enstitüsü. Derg. 2021, 8, 516–523. [Google Scholar] [CrossRef]
- Milovanovic, B.; Djajic, V.; Bajic, D.; Djokovic, A.; Krajnovic, T.; Jovanovic, S.; Verhaz, A.; Kovacevic, P.; Ostojic, M. Assessment of Autonomic Nervous System Dysfunction in the Early Phase of Infection With SARS-CoV-2 Virus. Front. Neurosci. 2021, 15, 640835. [Google Scholar] [CrossRef]
- Kurtoğlu, E.; Afsin, A.; Aktaş, İ.; Aktürk, E.; Kutlusoy, E.; Çağaşar, Ö. Altered Cardiac Autonomic Function after Recovery from COVID-19. Ann. Noninvasive. Electrocardiol. 2022, 27, e12916. [Google Scholar] [CrossRef] [PubMed]
- Asarcikli, L.D.; Hayiroglu, M.İ.; Osken, A.; Keskin, K.; Kolak, Z.; Aksu, T. Heart Rate Variability and Cardiac Autonomic Functions in Post-COVID Period. J. Interv. Card. Electrophysiol. 2022, 63, 715–721. [Google Scholar] [CrossRef]
- Marques, K.C.; Silva, C.C.; Trindade, S.S.; Santos, M.C.S.; Rocha, R.S.B.; Vasconcelos, P.F.C.; Quaresma, J.A.S.; Falcão, L.F.M. Reduction of Cardiac Autonomic Modulation and Increased Sympathetic Activity by Heart Rate Variability in Patients With Long COVID. Front. Cardiovasc. Med. 2022, 9, 862001. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart Rate Variability Analysis Software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Koizumi, K.; Terui, N.; Kollai, M. Effect of Cardiac Vagal and Sympathetic Nerve Activity on Heart Rate in Rhythmic Fluctuations. J. Auton. Nerv. Syst. 1985, 12, 251–259. [Google Scholar] [CrossRef]
- Moak, J.P.; Goldstein, D.S.; Eldadah, B.A.; Saleem, A.; Holmes, C.; Pechnik, S.; Sharabi, Y. Supine Low-Frequency Power of Heart Rate Variability Reflects Baroreflex Function, Not Cardiac Sympathetic Innervation. Heart Rhythm. 2007, 4, 1523–1529. [Google Scholar] [CrossRef]
- Rahman, F.; Pechnik, S.; Gross, D.; Sewell, L.; Goldstein, D.S. Low Frequency Power of Heart Rate Variability Reflects Baroreflex Function, Not Cardiac Sympathetic Innervation. Clin. Auton. Res. 2011, 21, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carod-Artal, F.J. Infectious Diseases Causing Autonomic Dysfunction. Clin. Auton. Res. 2018, 28, 67–81. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.-H.; Wood, J.; O’Dea, M.R.; Dutton, S.; Shamardani, K.; Nwangwu, K.; et al. Mild Respiratory COVID Can Cause Multi-Lineage Neural Cell and Myelin Dysregulation. Cell 2022, 185, 2452–2468.e16. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Montiel, A.; Fernández-Carvajal, A.; Planells-Cases, R.; Fernández-Ballester, G.; González-Ros, J.M.; Messeguer, À.; González-Muñiz, R. Advances in Modulating Thermosensory TRP Channels. Expert Opin. Ther. Pat. 2012, 22, 999–1017. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Zhang, Y.; Wang, M.; Zhang, H.; Chen, Y.; Adcock, I.M.; Chung, K.F.; Mo, J.; Zhang, Y.; Li, F. TRPV1 and TRPA1 in Lung Inflammation and Airway Hyperresponsiveness Induced by Fine Particulate Matter (PM2.5). Oxid. Med. Cell Longev. 2019, 2019, 7450151. [Google Scholar] [CrossRef] [Green Version]
- Liviero, F.; Campisi, M.; Scarpa, M.C.; Mason, P.; Guarnieri, G.; Maestrelli, P.; Pavanello, S. Multiple Single Nucleotide Polymorphisms of the Transient Receptor Potential Vanilloid 1 (TRPV1) Genes Associate with Cough Sensitivity to Capsaicin in Healthy Subjects. Pulm. Pharm. 2020, 61, 101889. [Google Scholar] [CrossRef]
- Liviero, F.; Scarpa, M.C.; De Stefani, D.; Folino, F.; Campisi, M.; Mason, P.; Iliceto, S.; Pavanello, S.; Maestrelli, P. Modulation of TRPV-1 by Prostaglandin-E 2 and Bradykinin Changes Cough Sensitivity and Autonomic Regulation of Cardiac Rhythm in Healthy Subjects. Sci. Rep. 2020, 10, 15163. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, Y.; Yang, H.; Capó-Aponte, J.E.; Tachado, S.D.; Wolosin, J.M.; Reinach, P.S. NF-ΚB Feedback Control of JNK1 Activation Modulates TRPV1-Induced Increases in IL-6 and IL-8 Release by Human Corneal Epithelial Cells. Mol. Vis. 2011, 17, 3137–3146. [Google Scholar] [PubMed]
- Williams, D.P.; Koenig, J.; Carnevali, L.; Sgoifo, A.; Jarczok, M.N.; Sternberg, E.M.; Thayer, J.F. Heart Rate Variability and Inflammation: A Meta-Analysis of Human Studies. Brain. Behav. Immun. 2019, 80, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ask, T.F.; Lugo, R.G.; Sütterlin, S. The Neuro-Immuno-Senescence Integrative Model (NISIM) on the Negative Association Between Parasympathetic Activity and Cellular Senescence. Front. Neurosci. 2018, 12, 726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tracey, K.J. The Inflammatory Reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef]
- Mol, M.B.A.; Strous, M.T.A.; van Osch, F.H.M.; Vogelaar, F.J.; Barten, D.G.; Farchi, M.; Foudraine, N.A.; Gidron, Y. Heart-Rate-Variability (HRV), Predicts Outcomes in COVID-19. PLoS ONE 2021, 16, e0258841. [Google Scholar] [CrossRef]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Long, X.; Zhang, Q.; Fang, X.; Li, N.; Lin, Z.; Li, J.; Xiong, N. Mild Manifestations of COVID-19 in Healthcare Workers. PLoS Negl. Trop. Dis. 2020, 14, e0008950. [Google Scholar] [CrossRef]
- Maraschini, A.; Corsi, E.; Salvatore, M.A.; Donati, S.; ItOSS COVID-19 working group. Coronavirus and Birth in Italy: Results of a National Population-Based Cohort Study. Ann. Ist. Super. Sanita. 2020, 56, 378–389. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Recovered COVID-19 HCWs | Control HCWs | p-Value |
|---|---|---|---|
| N, people | 44 | 44 | n.a. |
| Age, years | 44.7 ± 9.98 | 45.2 ± 10.3 | 0.80 |
| Male gender | 12 (27.3%) | 12 (27.3%) | n.d. |
| Systolic blood pressure, mmHg | 131.7 ± 15.5 | 126.6 ± 11.2 | 0.08 |
| Diastolic blood pressure, mmHg | 82.9 ± 8.23 | 81.5 ± 6.70 | 0.35 |
| Body mass index, kg/m2 | 24.5 ± 4.19 | 23.8 ± 3.98 | 0.47 |
| Night shift workers | 20 (45.4%) | 14 (31.8%) | 0.20 * |
| Vaccinated HCWs | 21 (47.7%) | 40 (90.9%) | 0.00032 * |
| Disease duration, days | 15.5 (10.2–20.0) | n.a. | n.a. |
| Duration from COVID-19 to ECG, days | 30 (5.2–55.7) | n.a. | n.a. |
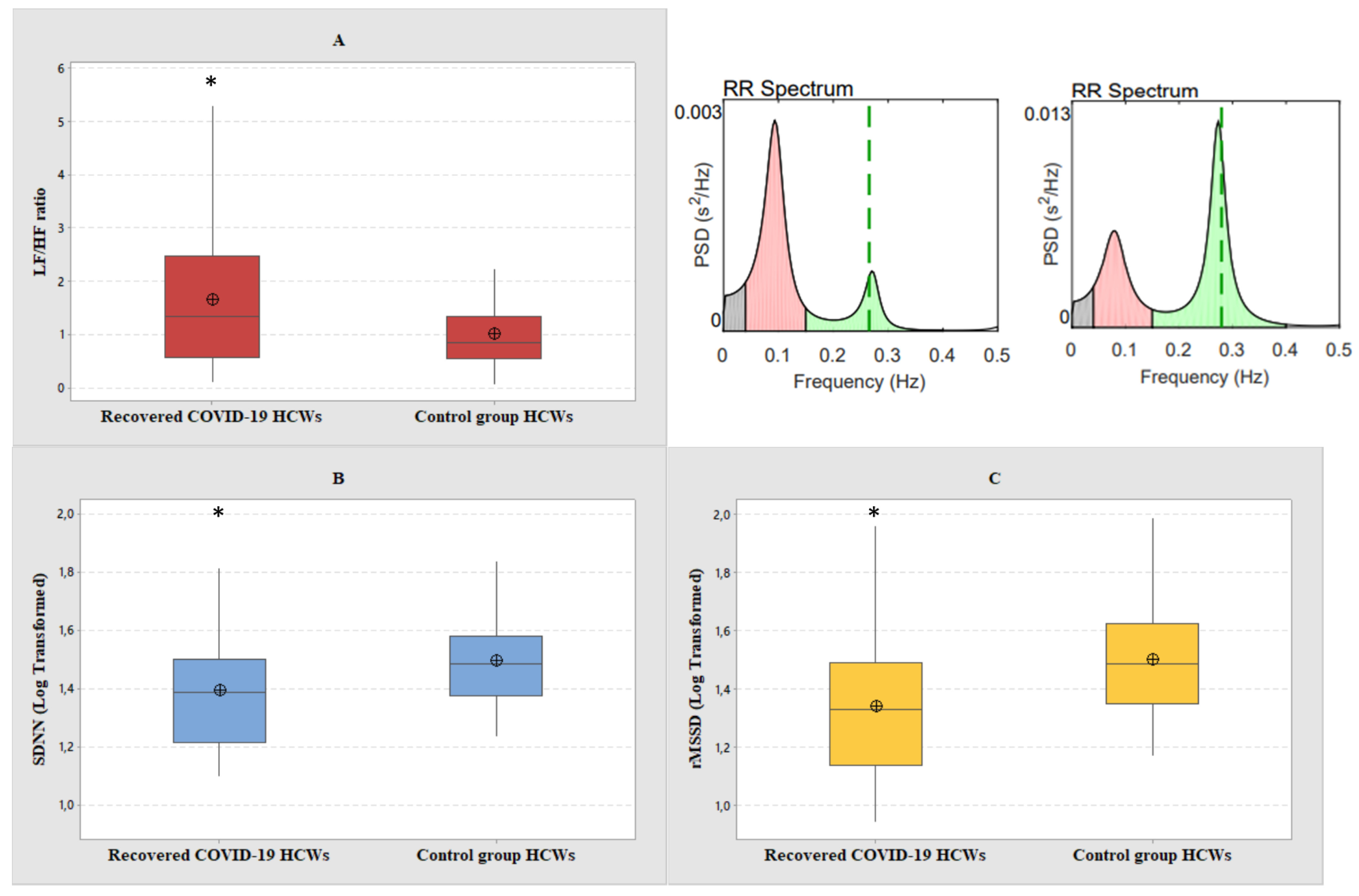
| Variables | Recovered COVID-19 HCWs | Control Group HCWs | p-Value | Effect Size Value |
|---|---|---|---|---|
| nLF | 53.6 ± 19.8 | 45.4 ± 16.2 | 0.03 * | 0.45 |
| nHF | 46.4 ± 19.8 | 54.6 ± 16.2 | 0.03 * | 0.45 |
| LF/HF | 1.66 ± 1.37 | 1.00 ± 0.66 | 0.006 * | 0.61 |
| SDNN a | 1.39 (1.21–1.50) | 1.49 (1.37–1.58) | 0.01 * | 0.58 |
| RMSSD a | 1.33 (1.14–1.49) | 1.49 (1.35–1.62) | 0.002 * | 0.70 |
| Mean HR, bpm | 73.9 ± 8.67 | 69 ± 10.4 | 0.01 * | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liviero, F.; Scapellato, M.L.; Folino, F.; Moretto, A.; Mason, P.; Pavanello, S. Persistent Increase of Sympathetic Activity in Post-Acute COVID-19 of Paucisymptomatic Healthcare Workers. Int. J. Environ. Res. Public Health 2023, 20, 830. https://doi.org/10.3390/ijerph20010830
Liviero F, Scapellato ML, Folino F, Moretto A, Mason P, Pavanello S. Persistent Increase of Sympathetic Activity in Post-Acute COVID-19 of Paucisymptomatic Healthcare Workers. International Journal of Environmental Research and Public Health. 2023; 20(1):830. https://doi.org/10.3390/ijerph20010830
Chicago/Turabian StyleLiviero, Filippo, Maria Luisa Scapellato, Franco Folino, Angelo Moretto, Paola Mason, and Sofia Pavanello. 2023. "Persistent Increase of Sympathetic Activity in Post-Acute COVID-19 of Paucisymptomatic Healthcare Workers" International Journal of Environmental Research and Public Health 20, no. 1: 830. https://doi.org/10.3390/ijerph20010830