
Effectiveness of the Online “Dialogue Circles” Nursing Intervention to Increase Positive Mental Health and Reduce the Burden of Caregivers of Patients with Complex Chronic Conditions. Randomized Clinical Trial
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
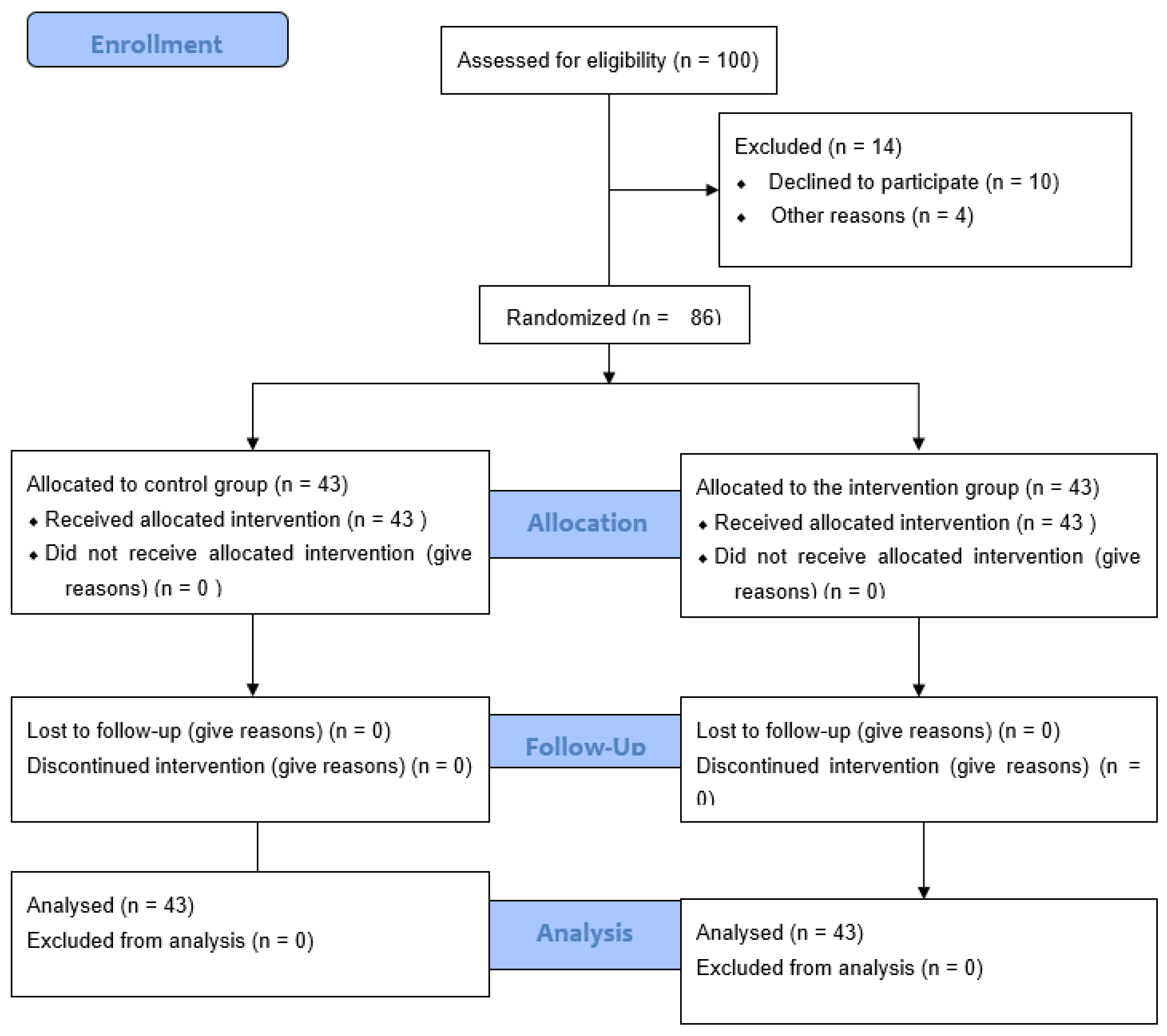
2.2. Setting and Participant Selection
2.3. Randomization and Masking
2.4. Instruments
2.5. Intervention
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic Data
3.2. Levels of Overload and Positive Mental Health at Baseline
3.3. Post-Intervention Levels of Overload and Positive Mental Health
3.4. Post-Intervention Changes
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization-WHO. Noncommunicable Diseases Country Profiles. 2018. Available online: https://apps.who.int/iris/handle/10665/274512 (accessed on 18 October 2022).
- Díez-Manglano, J. La Pluripatología, Un Reto Para Los Sistemas Sanitarios. Rev. Clin. Esp. 2017, 217, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gual, N.; Yuste Font, A.; Enfedaque Montes, B.; Blay Pueyo, C.; Martín Álvarez, R.; Inzitari, M. Profile and Evolution of Chronic Complex Patients in a Subacute Unit. Aten. Primaria 2017, 49, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Prat Martínez, M.; Bleda Garcia, S.; Edo Gual, M.; Pineda-Herrero, P. Learning Outcomes of Nursing Skills Related to Decision Making in the Context of Care of the Chronic Patient with Complex Needs. Educ. Med. 2021, 22, 466–472. [Google Scholar] [CrossRef]
- Wright, L.M.; Leahey, M. Nurses and Families A Guide to Family Assessment and Intervention, 6th ed.; References Scientific Research Publishing; FA Davis Company: Philadelphia, PA, USA, 2013; Available online: https://www.scirp.org/(S(lz5mqp453edsnp55rrgjct55))/reference/ReferencesPapers.aspx?ReferenceID=1875806 (accessed on 18 October 2022).
- Tartaglini, M.F.; Feldberg, C.; Hermida, P.D.; Heisecke, S.L.; Dillon, C.; Ofman, S.D.; Nuñez, M.L.; Somale, V. Escala de Sobrecarga Del Cuidador de Zarit: Análisis de Sus Propiedades Psicométricas En Cuidadores Familiares Residentes En Buenos Aires, Argentina. Neurol. Argent. 2020, 12, 27–35. [Google Scholar] [CrossRef]
- Farquhar, M. Assessing Carer Needs in Chronic Obstructive Pulmonary Disease. Chronic. Respir. Dis. 2017, 15, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, C.Y.; Tsai, Y.F. Factors of Caregiver Burden and Family Functioning among Taiwanese Family Caregivers Living with Schizophrenia. J. Clin. Nurs. 2015, 24, 1546–1556. [Google Scholar] [CrossRef]
- Morais Duarte Miranda, G.; da Cruz Gouveia Mendes, A.; Lucia Andrade da Silva, A.; Oswaldo Cruz, F.; Gabriella Morais Duarte Miranda, C. Population Aging in Brazil: Current and Future Social Challenges and Consequences. Rev. Bras. De Geriatr. E Gerontol. 2016, 19, 507–519. [Google Scholar] [CrossRef]
- Roth, D.L.; Fredman, L.; Haley, W.E. Informal Caregiving and Its Impact on Health: A Reappraisal from Population-Based Studies. Gerontologist 2015, 55, 309–319. [Google Scholar] [CrossRef] [Green Version]
- Guerra-Martín, M.D.; Amador-Marín, B.; Martínez-Montilla, J.M. Health Problems of Family Caregivers of People over 65 Suffering from Chronic Renal Failure: A Systematic Review. An. Del Sist. Sanit. De Navar. 2015, 38, 425–438. [Google Scholar] [CrossRef]
- Moriarty, H.; Winter, L.; Short, T.H.; True, G. Exploration of Factors Related to Depressive Symptomatology in Family Members of Military Veterans with Traumatic Brain Injury. J. Fam. Nurs. 2018, 24, 184–216. [Google Scholar] [CrossRef]
- Ngangana, P.C.; Davis, B.L.; Burns, D.P.; McGee, Z.T.; Montgomery, A.J. Intra-Family Stressors among Adult Siblings Sharing Caregiving for Parents. J. Adv. Nurs. 2016, 72, 3169–3181. [Google Scholar] [CrossRef] [PubMed]
- Bove, D.G.; Zakrisson, A.B.; Midtgaard, J.; Lomborg, K.; Overgaard, D. Undefined and Unpredictable Responsibility: A Focus Group Study of the Experiences of Informal Caregiver Spouses of Patients with Severe COPD. J. Clin. Nurs. 2016, 25, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.M.; Ferré-Grau, C.; Ferreira, P.L. Being an Informal Caregiver of a Person with a Pressure Ulcer in the Azores Islands. Adv. Skin. Wound Care 2015, 28, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Deek, H.; Hamilton, S.; Brown, N.; Inglis, S.C.; Digiacomo, M.; Newton, P.J.; Noureddine, S.; Macdonald, P.S.; Davidson, P.M. Family-Centred Approaches to Healthcare Interventions in Chronic Diseases in Adults: A Quantitative Systematic Review. J. Adv. Nurs. 2016, 72, 968–979. [Google Scholar] [CrossRef] [PubMed]
- Pucciarelli, G.; Ausili, D.; Galbussera, A.A.; Rebora, P.; Savini, S.; Simeone, S.; Alvaro, R.; Vellone, E. Quality of Life, Anxiety, Depression and Burden among Stroke Caregivers: A Longitudinal, Observational Multicentre Study. J. Adv. Nurs. 2018, 74, 1875–1887. [Google Scholar] [CrossRef]
- Rossinot, H.; Marquestaut, O.; de Stampa, M. The Experience of Patients and Family Caregivers during Hospital-at-Home in France. BMC Health Serv. Res. 2019, 19, 470. [Google Scholar] [CrossRef]
- Síndrome de Sobrecarga Del Cuidador. Available online: https://www.gerontologica.com/articulo-interes/sindrome-de-sobrecarga-del-cuidador (accessed on 18 October 2022).
- Corry, M.; While, A.; Neenan, K.; Smith, V. A Systematic Review of Systematic Reviews on Interventions for Caregivers of People with Chronic Conditions. J. Adv. Nurs. 2015, 71, 718–734. [Google Scholar] [CrossRef]
- Thomas, S.; Dalton, J.; Harden, M.; Eastwood, A.; Parker, G. Updated Meta-Review of Evidence on Support for Carers. Health Serv. Deliv. Res. 2017, 5, 1–132. [Google Scholar] [CrossRef] [Green Version]
- Faronbi, J.O.; Faronbi, G.O.; Ayamolowo, S.J.; Olaogun, A.A. Caring for the Seniors with Chronic Illness: The Lived Experience of Caregivers of Older Adults. Arch. Gerontol. Geriatr. 2019, 82, 8–14. [Google Scholar] [CrossRef]
- Ferré-Bergadà, M.; Valls, A.; Raigal-Aran, L.; Lorca-Cabrera, J.; Albacar-Riobóo, N.; Lluch-Canut, T.; Ferré-Grau, C. A Method to Determine a Personalized Set of Online Exercises for Improving the Positive Mental Health of a Caregiver of a Chronically Ill Patient. BMC Med. Inform. Decis. Mak. 2021, 21, 74. [Google Scholar] [CrossRef]
- Bustillo, M.L.; Gómez-Gutiérrez, M.; Guillén, A.I. Informal Caregivers for Dependent Elderly People: A Revision of Psychological Interventions over the Last Ten Years. Clin. Salud. 2018, 29, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Ferré-Grau, C.; Sevilla-Casado, M.; Lleixá-Fortuño, M.; Aparicio-Casals, M.R.; Cid-Buera, D.; Rodero-Sanchez, V.; Vives-Relats, C. Effectiveness of Problem-Solving Technique in Caring for Family Caregivers: A Clinical Trial Study in an Urban Area of Catalonia (Spain). J. Clin. Nurs. 2014, 23, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Parra-Vidales, E.; Soto-Pérez, F.; Perea-Bartolomé, M.; Franco-Martín, M.; Muñoz-Sánchez, J. Intervenciones Online Para Cuidadores de Personas Con Demencia: Revisión Sistemática. Actas. Esp. Psiquiatr. 2017, 45, 116–126. [Google Scholar] [PubMed]
- Corry, M.; Neenan, K.; Brabyn, S.; Sheaf, G.; Smith, V. Telephone Interventions, Delivered by Healthcare Professionals, for Providing Education and Psychosocial Support for Informal Caregivers of Adults with Diagnosed Illnesses. Cochrane Database Syst. Rev. 2019, 2019, CD012533. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Sun, Y.-Y.; Zhong, B. Mindfulness-Based Stress Reduction for Family Carers of People with Dementia. Cochrane Database Syst. Rev. 2018, 2018, CD012791. [Google Scholar] [CrossRef]
- Treanor, C.J.; Santin, O.; Prue, G.; Coleman, H.; Cardwell, C.R.; O’halloran, P.; Donnelly, M. Psychosocial Interventions for Informal Caregivers of People Living with Cancer. Cochrane Database Syst. Rev. 2019, 2019, CD009912. [Google Scholar] [CrossRef]
- Mittelman, M.S.; Roth, D.L.; Coon, D.W.; Haley, W.E. Sustained Benefit of Supportive Intervention for Depressive Symptoms in Caregivers of Patients with Alzheimer’s Disease. Am. J. Psychiatry 2004, 161, 850–856. [Google Scholar] [CrossRef] [Green Version]
- Bakas, T.; Austin, J.K.; Habermann, B.; Jessup, N.M.; McLennon, S.M.; Mitchell, P.H.; Morrison, G.; Yang, Z.; Stump, T.E.; Weaver, M.T. Telephone Assessment and Skill-Building Kit for Stroke Caregivers: A Randomized Controlled Clinical Trial. Stroke 2015, 46, 3478–3487. [Google Scholar] [CrossRef] [Green Version]
- Moskowitz, J.T.; Cheung, E.O.; Snowberg, K.E.; Verstaen, A.; Merrilees, J.; Salsman, J.M.; Dowling, G.A. Randomized Controlled Trial of a Facilitated Online Positive Emotion Regulation Intervention for Dementia Caregivers. Health Psychol. 2019, 38, 391–402. [Google Scholar] [CrossRef]
- Pfeiffer, K.; Beische, D.; Hautzinger, M.; Berry, J.W.; Wengert, J.; Hoffrichter, R.; Becker, C.; van Schayck, R.; Elliott, T.R. Telephone-Based Problem-Solving Intervention for Family Caregivers of Stroke Survivors: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2014, 82, 628–643. [Google Scholar] [CrossRef]
- Cuthbert, C.A.; King-Shier, K.M.; Ruether, J.D.; Tapp, D.M.; Wytsma-Fisher, K.; Fung, T.S.; Nicole Culos-Reed, S. The Effects of Exercise on Physical and Psychological Outcomes in Cancer Caregivers: Results From the RECHARGE Randomized Controlled Trial. Ann. Behav. Med. 2018, 52, 645–661. [Google Scholar] [CrossRef] [PubMed]
- Gómez, Á.M.O. Programa de Intervención Cognoscitivo Conductual En La Calidad de Sueño de Cuidadores Familiares. Rev. Colomb. De Enfermería 2012, 7, 75–85. [Google Scholar] [CrossRef]
- Javier, L.; Instituto de Mayores y Servicios Sociales (Espanya). El Apoyo a Los Cuidadores de Familiares Mayores Dependientes En El Hogar: Desarrollo Del Programa “Cómo Mantener Su Bienestar”. 2007. Available online: https://www.academia.edu/39265058/El_apoyo_a_los_cuidadores_de_familiares_mayores_dependientes_en_el_hogar_desarrollo_del_programa_C%C3%B3mo_mantener_su_bienestar_ (accessed on 17 November 2022).
- Zabalegui Yárnoz, A.; Navarro Díez, M.; Cabrera Torres, E.; Fernández-Puebla, A.G.; Bardallo Porras, D.; Rodríguez Higueras, E.; Gual García, P.; Fernández Capo, M.; Argemí Remon, J. Eficacia de Las Intervenciones Dirigidas a Cuidadores Principales de Personas Dependientes Mayores de 65 Años. Una Revisión Sistemática. Rev. Esp. Geriatr. Gerontol. 2008, 43, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.M.; Bosmans, J.E.; Cuijpers, P.; Zarit, S.H.; Pot, A.M. Effectiveness and Cost-Effectiveness of an Internet Intervention for Family Caregivers of People with Dementia: Design of a Randomized Controlled Trial. BMC Psychiatry 2013, 13, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristancho-Lacroix, V.; Moulin, F.; Wrobel, J.; Batrancourt, B.; Plichart, M.; de Rotrou, J.; Cantegreil-Kallen, I.; Rigaud, A.-S. A Web-Based Program for Informal Caregivers of Persons with Alzheimer’s Disease: An Iterative User-Centered Design. JMIR Res. Protoc. 2014, 3, e46. [Google Scholar] [CrossRef]
- Mar, D.; Fortuño, L.; Montserrat, D.; Martínez, G.; Maria, D.; Canut, T.L.; Merino, J.R.; Cinta, D.; Vidal, E.; Carme, D.; et al. Diseño de Una Web 2.0 Para Cuidadoras de Personas Con Problemas Crónicos de Salud. Pixel-Bit. Rev. De Medios Y Educ. 2015, 47, 149–161. [Google Scholar] [CrossRef]
- Ferré-Grau, C.; Raigal-Aran, L.; Lorca-Cabrera, J.; Ferré-Bergadá, M.; Lleixà-Fortuño, M.; Lluch-Canut, M.T.; Puig-Llobet, M.; Albacar-Riobóo, N. A Multi-Centre, Randomized, 3-Month Study to Evaluate the Efficacy of a Smartphone App to Increase Caregiver’s Positive Mental Health. BMC Public Health 2019, 19, 888. [Google Scholar] [CrossRef]
- Fuller-Tyszkiewicz, M.; Richardson, B.; Little, K.; Teague, S.; Hartley-Clark, L.; Capic, T.; Khor, S.; Cummins, R.A.; Olsson, C.A.; Hutchinson, D. Efficacy of a Smartphone App Intervention for Reducing Caregiver Stress: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e17541. [Google Scholar] [CrossRef]
- Sweet, C.M.C.; Li, E.J.; Sagui-Henson, S.; Chamberlain, C.E.W.; Altman, M. Impact of Online Group Psychoeducation and Support Sessions on Receptivity Towards Digital Mental Health Care During the COVID-19 Pandemic: A Pilot Study. J. Technol. Behav. Sci. 2022, 1–9. [Google Scholar] [CrossRef]
- Ghanbari, E.; Yektatalab, S.; Mehrabi, M. Effects of Psychoeducational Interventions Using Mobile Apps and Mobile-Based Online Group Discussions on Anxiety and Self-Esteem in Women with Breast Cancer: Randomized Controlled Trial. MIR Mhealth Uhealth 2021, 9, e19262. [Google Scholar] [CrossRef]
- Camarena, J.M.T.; Cruzado, J.V.; Llobet, M.P.; Blanco, M.Á.H.; Canut, M.T.L.; Arroyo, M.C.M. Intervención Enfermera “Círculos de Diálogo” Para La Disminución Del Nivel de Sobrecarga de Cuidadores de Pacientes Crónico Complejos y Con Enfermedad Crónica Avanzada. 2021. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=7843709 (accessed on 17 November 2022).
- De Souza, J.B.; Heidemann, I.T.S.B.; Massaroli, A.; Geremia, D.S. Health Promotion in Coping with COVID-19: A Virtual Culture Circle Experience. Rev. Bras. Enferm. 2021, 74, e20200602. [Google Scholar] [CrossRef] [PubMed]
- Regueiro Martínez, A.Á.; Pérez-Vázquez, A.; Gómara Villabona, S.M.; Ferreiro Cruz, M.C. Escala de Zarit Reducida Para La Sobrecarga Del Cuidador En Atención Primaria. Aten. Primaria 2007, 39, 185–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the Impaired Elderly: Correlates of Feelings of Burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’callaghan, C.A. OxMaR: Open Source Free Software for Online Minimization and Randomization for Clinical Trials. PLoS ONE 2014, 9, e110761. [Google Scholar] [CrossRef] [Green Version]
- Lluch, M.T. Construcción de Una Escala Para Evaluar la Salud Mental Positiva. Ph.D. Thesis, Universidad de Barcelona, Barcelona, Spain, 1999. Available online: https://www.tdx.cat/handle/10803/2366 (accessed on 17 November 2022).
- Lluch-Canut, T.; Puig-Llobet, M.; Sánchez-Ortega, A.; Roldán-Merino, J.; Ferré-Grau, C.; Albacar, N.; Broncano, M.; Falcó-Pegueroles, A.; Gelabert, S.; Lleixà, M.M.; et al. Assessing Positive Mental Health in People with Chronic Physical Health Problems: Correlations with Socio-Demographic Variables and Physical Health Status. BMC Public Health 2013, 13, 928. [Google Scholar] [CrossRef] [Green Version]
- Puig Llobet, M.; Sánchez Ortega, M.; Lluch-Canut, M.; Moreno-Arroyo, M.; Hidalgo Blanco, M.À.; Roldán-Merino, J. Positive Mental Health and Self-Care in Patients with Chronic Physical Health Problems: Implications for Evidence-Based Practice. Worldviews Evid. Based Nurs. 2020, 17, 293–300. [Google Scholar] [CrossRef]
- Lluch, M.T. Decálogo de Salud Mental Positiva; Impresión Digital de la Universidad de Barcelona: Barcelona, Spain, 2011; Available online: http://diposit.ub.edu/dspace/handle/2445/20062 (accessed on 17 November 2022).
- Rodríguez-González, A.M.; Rodríguez-Míguez, E.; Duarte-Pérez, A.; Díaz-Sanisidro, E.; Barbosa-Álvarez, Á.; Clavería, A. Estudio Observacional Transversal de La Sobrecarga En Cuidadoras Informales y Los Determinantes Relacionados Con La Atención a Las Personas Dependientes. Aten. Primaria 2017, 49, 156–165. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the Sensitivity of the Barthel Index for Stroke Rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Tulia Sánchez Martínez, R.; Milena, E.; Cardona, M.; Rocío Gómez-Ortega, O. Intervenciones de Enfermería Para Disminuir La Sobrecarga En Cuidadores: Un Estudio Piloto. Rev. Cuid. 2016, 7, 1171–1184. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Tello, M.; Casado-Mejía, R.; Ortega-Calvo, M.; Ruiz-Arias, E. Sobrecarga Sentida En Personas Cuidadoras Informales de Pacientes Pluripatológicos En Una Zona Urbana. Enferm. Clin. 2012, 22, 286–292. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.C.; Nicholls, E.; Cabrera, T.V.; Drew, A.; Jimenez-Maldonado, M.; Martinez-Cortes, M.L. Health-Related Quality of Life in Caregivers of Individuals with Traumatic Brain Injury from Guadalajara, Mexico. J. Rehabil. Med. 2011, 43, 983–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arechabala, M.C.; Catoni, M.I.; Palma, E.; Barrios, S. Depresión y Autopercepción de La Carga Del Cuidado En Pacientes En Hemodiálisis y Sus Cuidadores. Rev. Panam. De Salud Pública 2011, 30, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Minué-Lorenzo, S.; Fernández-Aguilar, C. Visión Crítica y Argumentación Sobre Los Programas de Atención de La Cronicidad En Atención Primaria y Comunitaria. Aten. Primaria 2018, 50, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Ramón-Arbués, E.; Martínez-Abadía, B.; Martín-Gómez, S. Factores Determinantes de La Sobrecarga Del Cuidador. Estudio de Las Diferencias de Género. Aten. Primaria 2017, 49, 308–309. [Google Scholar] [CrossRef] [PubMed]
- Rubio Fernández, E.; Martínez Momblan, M.A.; Rosino Bosch, A.; Manresa Domínguez, J.M.; Ramos Fernández, A.; Torres Quintana, A. Carga del cuidador principal informal del paciente crónico complejo y paciente crónico avanzado en dos centros de urgencia de atención primaria de la provincia de Barcelona. Rev. Rol. Enferm. 2020, 43, 290–296. [Google Scholar]
- Toffoletto, M.C.; Reynaldos-Grandón, K.L. Determinantes Sociales de Salud, Sobrecarga Familiar y Calidad de Vida de Cuidadores Familiares de Pacientes Oncológicos En Cuidados Paliativos. Rev. De Salud Pública 2019, 21, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Elizabeth Flores, G.; Edith Rivas, R.; Fredy Seguel, P. burden level in performing the role of family caregivers of elderly with severe dependence. Cienc. Y Enfermería 2012, 18, 29–41. [Google Scholar] [CrossRef]
- Ferré-Grau, C.; Raigal-Aran, L.; Lorca-Cabrera, J.; Lluch-Canut, T.; Ferré-Bergadà, M.; Lleixá-Fortuño, M.; Puig-Llobet, M.; Miguel-Ruiz, M.D.; Albacar-Riobóo, N. A Mobile App–Based Intervention Program for Nonprofessional Caregivers to Promote Positive Mental Health: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e21708. [Google Scholar] [CrossRef]
- Lopes Da Silva, M.C.; De, R.; Almeida, O.; Lopes Da, M.C.; Rosemary, S. Círculos de Diálogo: A Perspectiva Das Emoções Com Os Professores. Perspectiva 2021, 39, 1–19. [Google Scholar] [CrossRef]
- Freire, P. Pedagogia da Esperança: Um Reencontro com a Pedagogia do Oprimido. Editora Paz e Terra. 1987. Available online: https://books.google.com.au/books?hl=en&lr=&id=I73NAgAAQBAJ&oi=fnd&pg=PT4&dq=%3DFreire,+P.+Pedagogia+da+esperan%C3%A7a:+um+reencontro+com+a+pedagogia+do+oprimido.+Editora+Paz+e+Terra,+1987.&ots=q0b2z0S6nw&sig=VeMEcSWpp86nNyHOntFzm9fZShw&redir_esc=y#v=onepage&q&f=false (accessed on 17 November 2022).


{kind=link}
| Items | Overall | Control | Intervention | p-Value | |
|---|---|---|---|---|---|
| Age | 56.00 [49.25, 63.00] | 60.00 [54.50, 65.00] | 53.00 [46.50, 59.00] | 0.002 | |
| Caregiver months | 26.50 [16.25, 48.00] | 30.00 [18.00, 48.00] | 24.00 [14.00, 48.00] | 0.267 | |
| Gender | 0.102 | ||||
| Men | 17 (19.77%) | 12 (27.91%) | 5 (11.63%) | ||
| Women | 69 (80.23%) | 31 (72.09%) | 38 (88.37%) | ||
| Educational level | <0.001 | ||||
| No studies | 1 (1.16%) | 1 (2.33%) | 0 (0.00%) | ||
| Primary education | 21 (24.42%) | 17 (39.53%) | 4 (9.30%) | ||
| Intermediate level training cycle | 14 (16.28%) | 2 (4.65%) | 12 (27.91%) | ||
| Baccalaureate or higher education | 23 (26.74%) | 11 (25.58%) | 12 (27.91%) | ||
| University education | 27 (31.40%) | 12 (27.91%) | 15 (34.88%) | ||
| Marital status | 0.030 | ||||
| Single | 12 (13.95%) | 3 (6.98%) | 9 (20.93%) | ||
| Domestic partner | 6 (6.98%) | 1 (2.33%) | 5 (11.63%) | ||
| Married | 56 (65.12%) | 34 (79.07%) | 22 (51.16%) | ||
| Divorced | 12 (13.95%) | 5 (11.63%) | 7 (16.28%) | ||
| Number of children | 0.171 | ||||
| 0 | 23 (26.74%) | 10 (23.26%) | 13 (30.23%) | ||
| 1 | 19 (22.09%) | 7 (16.28%) | 12 (27.91%) | ||
| 2 | 38 (44.19%) | 24 (55.81%) | 14 (32.56%) | ||
| 3 | 6 (6.98%) | 2 (4.65%) | 4 (9.30%) | ||
| Employment status | 0.244 | ||||
| Unemployed | 15 (17.44%) | 8 (18.60%) | 7 (16.28%) | ||
| Part-time work | 5 (5.81%) | 2 (4.65%) | 3 (6.98%) | ||
| Employed | 44 (51.16%) | 18 (41.86%) | 26 (60.47%) | ||
| Self-employed | 6 (6.98%) | 5 (11.63%) | 1 (2.33%) | ||
| Retired | 16 (18.60%) | 10 (23.26%) | 6 (13.95%) | ||
| Family relationship | 0.277 | ||||
| Spouse | 17 (19.77%) | 11 (25.58%) | 6 (13.95%) | ||
| Son/daugher | 67 (77.91%) | 32 (74.42%) | 35 (81.40%) | ||
| Son-in-law/daugher-in-law | 1 (1.16%) | 0 (0.00%) | 1 (2.33%) | ||
| Others | 1 (1.16%) | 0 (0.00%) | 1 (2.33%) | ||
| Living together | 0.459 | ||||
| No | 22 (25.58%) | 13 (30.23%) | 9 (20.93%) | ||
| Yes | 64 (74.42%) | 30 (69.77%) | 34 (79.07%) | ||
| Receives financial benefits | 1.000 | ||||
| No | 65 (75.58%) | 33 (76.74%) | 32 (74.42%) | ||
| Yes | 21 (24.42%) | 10 (23.26%) | 11 (25.58%) |
| Items | Overall | Control | Intervention | p-Value |
|---|---|---|---|---|
| ZBI-7 Total score | 24.00 [21.00, 27.00] | 22.00 [20.00, 25.00] | 26.00 [24.00, 28.00] | <0.001 |
| Burden | 86 (100.00%) | 43 (100.00%) | 43 (100.00%) | 1.000 |
| PMH total score | 93.00 [89.25, 96.00] | 93.00 [90.50, 96.50] | 91.00 [89.00, 95.50] | 0.467 |
| F1: Personal satisfaction | 15.00 [13.00, 18.00] | 15.00 [13.00, 18.00] | 16.00 [14.00, 19.00] | 0.252 |
| F2: Prosocial attitude | 14.00 [13.00, 15.00] | 14.00 [13.00, 14.50] | 14.00 [13.00, 15.00] | 0.446 |
| F3: Self-control | 13.00 [11.00, 14.00] | 14.00 [12.00, 14.50] | 11.00 [10.00, 13.00] | <0.001 |
| F4: Autonomy | 8.50 [7.00, 11.00] | 8.00 [7.00, 10.00] | 9.00 [7.00, 11.00] | 0.238 |
| F5: Problem solving and self-actualization | 26.50 [23.00, 30.00] | 28.00 [23.50, 31.00] | 26.00 [22.00, 28.50] | 0.029 |
| F6: Interpersonal relationship skills | 15.00 [13.00, 16.00] | 14.00 [13.00, 15.00] | 15.00 [14.00, 17.00] | 0.005 |
| Items | Overall | Control | Intervention | p-Value |
|---|---|---|---|---|
| ZBI-7 Total score | 23.00 [20.00, 26.00] | 25.00 [22.00, 27.00] | 20.00 [18.00, 24.00] | <0.001 |
| Burden | 80 (93.02%) | 43 (100.00%) | 37 (86.05%) | 0.034 |
| PMH total score | 98.00 [89.25, 112.00] | 89.00 [83.00, 93.00] | 112.00 [105.50, 118.00] | <0.001 |
| F1: Personal satisfaction | 17.50 [14.00, 21.00] | 14.00 [12.00, 18.00] | 20.00 [17.00, 22.50] | <0.001 |
| F2: Prosocial attitude | 15.00 [13.00, 16.00] | 13.00 [12.00, 14.00] | 16.00 [16.00, 17.00] | <0.001 |
| F3: Self-Control | 13.00 [12.00, 15.00] | 13.00 [11.00, 14.00] | 15.00 [13.00, 16.00] | <0.001 |
| F4: Autonomy | 10.00 [8.00, 12.00] | 8.00 [6.00, 10.00] | 12.00 [9.00, 14.00] | <0.001 |
| F5: Problem solving and self-actualization | 28.50 [24.00, 32.00] | 25.00 [19.50, 29.00] | 32.00 [28.00, 33.50] | <0.001 |
| F6: Interpersonal relationship skills | 16.00 [14.00, 19.00] | 14.00 [13.00, 15.00] | 19.00 [18.00, 21.00] | <0.001 |
| Items | Control | Intervention | p-Value |
|---|---|---|---|
| ZBI-7 total score | 2.00 [1.00, 3.00] | −5.00 [−6.00, −4.00] | <0.001 |
| PMH total score | −4.00 [−8.50, −1.50] | 18.00 [14.00, 25.50] | <0.001 |
| F1: Personal satisfaction | 0.00 [−1.00, 0.50] | 3.00 [2.00, 4.50] | <0.001 |
| F2: Prosocial attitude | −1.00 [−1.00, 0.00] | 2.00 [1.00, 3.00] | <0.001 |
| F3: Self-control | −1.00 [−2.00, 0.00] | 2.00 [1.50, 4.00] | <0.001 |
| F4: Autonomy | 0.00 [−0.50, 1.00] | 2.00 [1.00, 3.00] | <0.001 |
| F5: Problem solving and self-actualization | −2.00 [−4.50, 0.00] | 5.00 [3.00, 8.00] | <0.001 |
| F6: Interpersonal relationship skills | 0.00 [−1.00, 1.00] | 4.00 [3.00, 5.00] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinoco-Camarena, J.M.; Puig-Llobet, M.; Lluch-Canut, M.T.; Roldan-Merino, J.; Moreno-Arroyo, M.C.; Moreno-Poyato, A.; Balaguer-Sancho, J.; Agüera, Z.; Sánchez-Ortega, M.A.; Hidalgo-Blanco, M.Á. Effectiveness of the Online “Dialogue Circles” Nursing Intervention to Increase Positive Mental Health and Reduce the Burden of Caregivers of Patients with Complex Chronic Conditions. Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2023, 20, 644. https://doi.org/10.3390/ijerph20010644
Tinoco-Camarena JM, Puig-Llobet M, Lluch-Canut MT, Roldan-Merino J, Moreno-Arroyo MC, Moreno-Poyato A, Balaguer-Sancho J, Agüera Z, Sánchez-Ortega MA, Hidalgo-Blanco MÁ. Effectiveness of the Online “Dialogue Circles” Nursing Intervention to Increase Positive Mental Health and Reduce the Burden of Caregivers of Patients with Complex Chronic Conditions. Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2023; 20(1):644. https://doi.org/10.3390/ijerph20010644
Chicago/Turabian StyleTinoco-Camarena, Jose Manuel, Montserrat Puig-Llobet, María Teresa Lluch-Canut, Juan Roldan-Merino, Mari Carmen Moreno-Arroyo, Antonio Moreno-Poyato, Judith Balaguer-Sancho, Zaida Agüera, Maria Aurelia Sánchez-Ortega, and Miguel Ángel Hidalgo-Blanco. 2023. "Effectiveness of the Online “Dialogue Circles” Nursing Intervention to Increase Positive Mental Health and Reduce the Burden of Caregivers of Patients with Complex Chronic Conditions. Randomized Clinical Trial" International Journal of Environmental Research and Public Health 20, no. 1: 644. https://doi.org/10.3390/ijerph20010644