
Association between Psychological Disorders, Mediterranean Diet, and Chronotype in a Group of Italian Adults

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Assessment of Psychological Profile
2.3. Adherence to MD
2.4. Assessment of Chronotype
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Sample
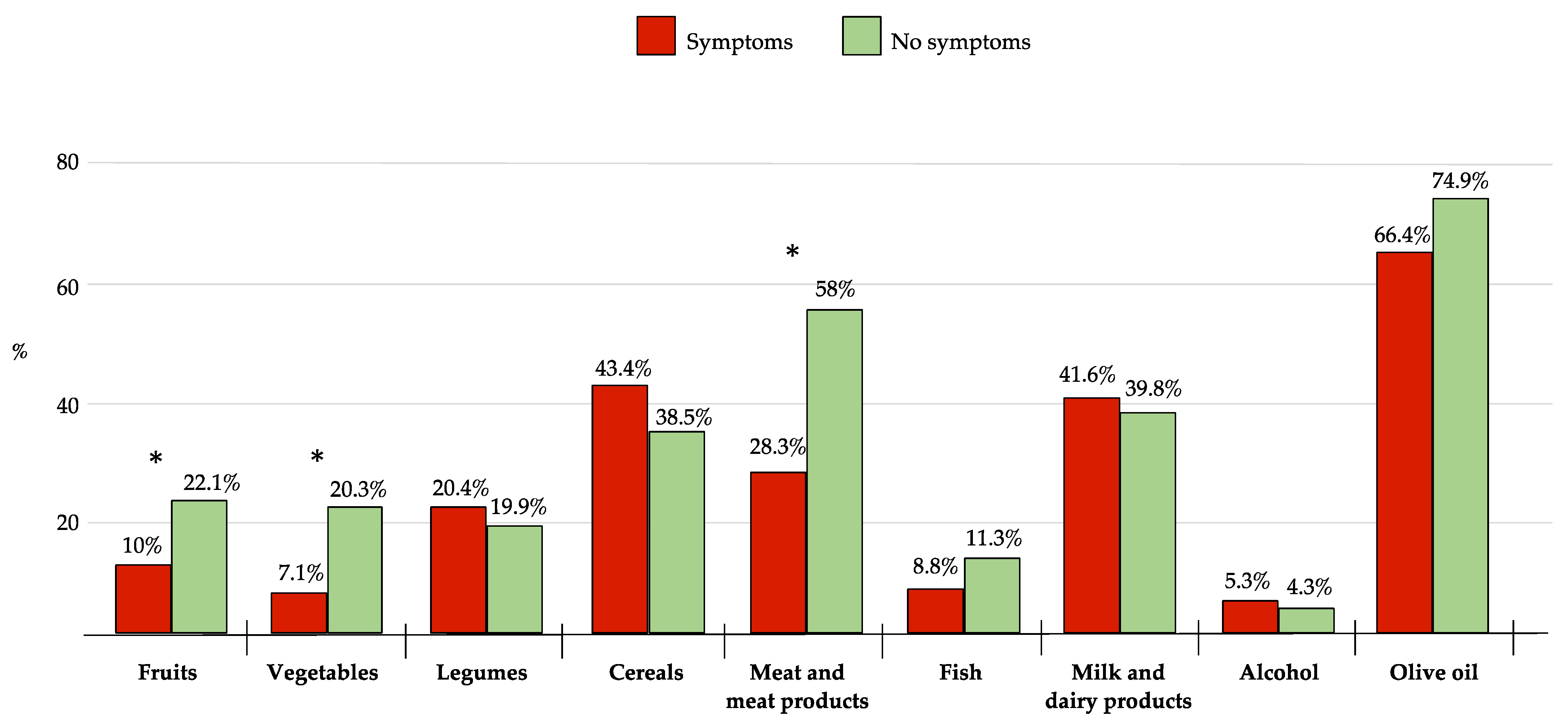
3.2. Psychological Disorders and MD Adherence
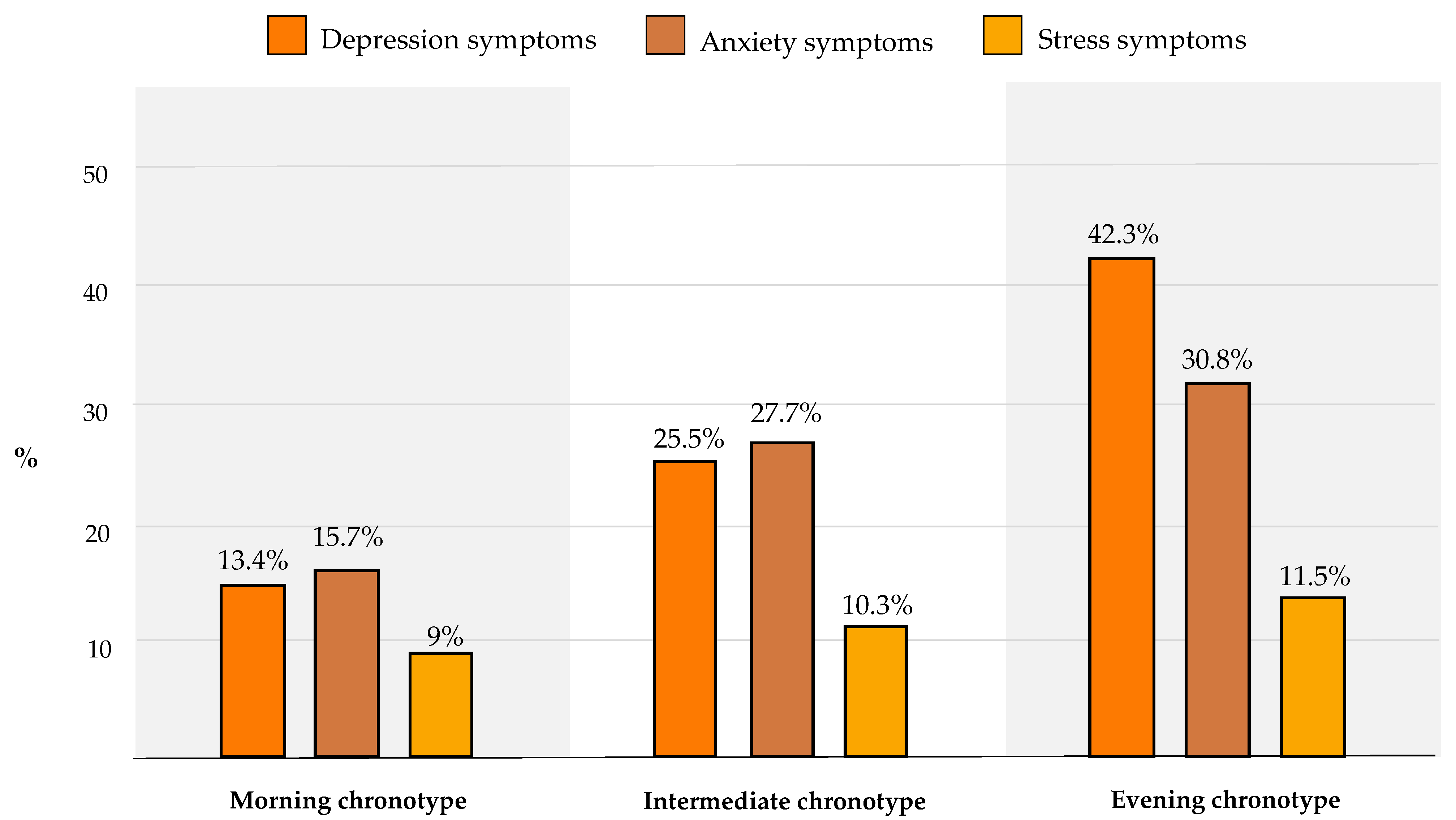
3.3. Psychological Disorders and Chronotype
3.4. Chronotype and MD Adherence
3.5. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coggeshall, M.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiat. 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates; World Health Oganization: Geneva, Switzerland, 2017. [Google Scholar]
- Arias, D.; Saxena, S.; Verguet, S. Quantifying the global burden of mental disorders and their economic value. EClinicalMedicine 2022, 54, 101675. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Rosenblat, J.D.; Brietzke, E.; Pan, Z.; Lee, Y.; Cao, B.; Zuckerman, H.; Kalantarova, A.; McIntyre, R.S. Stress, epigenetics and depression: A systematic review. Neurosci. Biobehav. Rev. 2019, 102, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Zaman, R.; Hankir, A.; Jemni, M. Lifestyle Factors and Mental Health. Psychiatr. Danub. 2019, 31, 217–220. [Google Scholar] [PubMed]
- Nucci, D.; Fatigoni, C.; Amerio, A.; Odone, A.; Gianfredi, V. Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6686. [Google Scholar] [CrossRef]
- Quirk, S.E.; Williams, L.J.; O’Neil, A.; Pasco, J.A.; Jacka, F.N.; Housden, S.; Berk, M.; Brennan, S.L. The association between diet quality, dietary patterns and depression in adults: A systematic review. BMC Psychiatry 2013, 13, 175. [Google Scholar] [CrossRef] [Green Version]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Koster, A.; Odone, A.; Amerio, A.; Signorelli, C.; Schaper, N.C.; Bosma, H.; Köhler, S.; Dagnelie, P.C.; Stehouwer, C.D.A.; et al. Associations of Dietary Patterns with Incident Depression: The Maastricht Study. Nutrients 2021, 13, 1034. [Google Scholar] [CrossRef]
- Singh, B.; Parsaik, A.K.; Mielke, M.M.; Erwin, P.J.; Knopman, D.S.; Petersen, R.C.; Roberts, R.O. Association of Mediterranean diet with mild cognitive impairment and Alzheimer’s disease: A systematic review and meta-analysis. J. Alzheimers Dis. 2014, 2, 271–282. [Google Scholar] [CrossRef]
- Gianfredi, V.; Dinu, M.; Nucci, D.; Eussen, S.J.P.M.; Amerio, A.; Schram, M.T.; Schaper, N.; Odone, A. Association between dietary patterns and depression: An umbrella review of meta-analyses of observational studies and intervention trials. Nutr. Rev. 2022, nuac058, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Bayes, J.; Schloss, J.; Sibbritt, D. Effects of Polyphenols in a Mediterranean Diet on Symptoms of Depression: A Systematic Literature Review. Adv. Nutr. 2020, 11, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.J.; Hasler, B.P. Chronotype and Mental Health: Recent Advances. Curr. Psychiatry Rep. 2018, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Roenneberg, T.; Merrow, M. The Circadian Clock and Human Health. Curr. Biol. 2016, 26, R432–R443. [Google Scholar] [CrossRef]
- Merikanto, I.; Partonen, T. Eveningness increases risks for depressive and anxiety symptoms and hospital treatments mediated by insufficient sleep in a population-based study of 18,039 adults. Depress. Anxiety. 2021, 38, 1066–1077. [Google Scholar] [CrossRef]
- Lotti, S.; Pagliai, G.; Colombini, B.; Sofi, F.; Dinu, M. Chronotype Differences in Energy Intake, Cardiometabolic Risk Parameters, Cancer, and Depression: A Systematic Review with Meta-Analysis of Observational Studies. Adv. Nutr. 2022, 13, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Mat Ludin, A.F. The Association between Chronotype and Dietary Pattern among Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 17, 68. [Google Scholar] [CrossRef] [Green Version]
- Lotti, S.; Pagliai, G.; Asensi, M.T.; Giangrandi, I.; Colombini, B.; Sofi, F.; Dinu, M. Morning chronotype is associated with higher adherence to the Mediterranean diet in a sample of Italian adults. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2086–2092. [Google Scholar] [CrossRef]
- SurveyMonkey.com. Available online: https://www.surveymonkey.com/ (accessed on 2 November 2022).
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Sangsefidi, Z.S.; Lorzadeh, E.; Hosseinzadeh, M.; Mirzaei, M. Dietary habits and psychological disorders in a large sample of Iranian adults: A population-based study. Ann. Gen. Psychiatry. 2020, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Petersen, K.S.; Hibbeln, J.R.; Hurley, D.; Kolick, V.; Peoples, S.; Rodriguez, N.; Woodward-Lopez, G. Nutrition and behavioral health disorders: Depression and anxiety. Nutr. Rev. 2021, 79, 247–260. [Google Scholar] [CrossRef]
- Nicolaou, M.; Colpo, M.; Vermeulen, E.; Elstgeest, L.E.; Cabout, M.; Gibson-Smith, D.; Knuppel, A.; Sini, G.; Schoenaker, D.A.J.M.; Mishra, G.D.; et al. Association of a priori dietary patterns with depressive symptoms: A harmonised meta-analysis of observational studies. Psychol. Med. 2020, 50, 1872–1883. [Google Scholar] [CrossRef] [Green Version]
- Yin, W.; Löf, M.; Chen, R.; Hultman, C.M.; Fang, F.; Sandin, S. Mediterranean diet and depression: A population-based cohort study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 153. [Google Scholar] [CrossRef]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [Green Version]
- Bayes, J.; Schloss, J.; Sibbritt, D. The effect of a Mediterranean diet on the symptoms of depression in young males (the “AMMEND: A Mediterranean Diet in MEN with Depression” study): A randomized controlled trial. Am. J. Clin. Nutr. 2022, 116, 572–580. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect Disord. 2013, 1, 12–27. [Google Scholar] [CrossRef] [Green Version]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Agirman, G.; Yu, K.B.; Hsiao, E.Y. Signaling inflammation across the gut-brain axis. Science 2021, 374, 1087–1092. [Google Scholar] [CrossRef]
- Adan, R.A.H.; van der Beek, E.M.; Buitelaar, J.K.; Cryan, J.F.; Hebebrand, J.; Higgs, S.; Schellekens, H.; Dickson, S.L. Nutritional psychiatry: Towards improving mental health by what you eat. Eur. Neuropsychopharmacol. 2019, 29, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Młyniec, K.; Davies, C.L.; de Aguero Sanchez, I.G.; Pytka, K.; Budziszewska, B.; Nowak, G. Essential elements in depression and anxiety. Part I. Pharmacol. Rep. 2014, 66, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, O.; Keshteli, A.H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Adherence to Mediterranean dietary pattern is inversely associated with depression, anxiety and psychological distress. Nutr. Neurosci. 2021, 24, 248–259. [Google Scholar] [CrossRef]
- Esgunoglu, L.; Jennings, A.; Connole, E.S.; Murphy, K.J.; Minihane, A.M. Short-term effects of a Mediterranean-style dietary pattern on cognition and mental well-being: A systematic review of clinical trials. Br. J. Nutr. 2022, 128, 1247–1256. [Google Scholar] [CrossRef]
- Au, J.; Reece, J. The relationship between chronotype and depressive symptoms: A meta-analysis. J. Affect Disord. 2017, 218, 93–104. [Google Scholar] [CrossRef]
- Gao, Q.; Sheng, J.; Qin, S.; Zhang, L. Chronotypes and affective disorders: A clock for mood? Brain Sci. Adv. 2019, 5, 145–160. [Google Scholar] [CrossRef]
- Norbury, R. Diurnal preference and depressive symptomatology: A meta-analysis. Sci. Rep. 2021, 11, 12003. [Google Scholar] [CrossRef]
- Gianfredi, V.; Schaper, N.C.; Odone, A.; Signorelli, C.; Amerio, A.; Eussen, S.J.; Köhler, S.; Savelberg, H.H.C.M.; Stehouwer, C.D.A.; Dagnelie, P.C.; et al. Daily patterns of physical activity, sedentary behavior, and prevalent and incident depression-The Maastricht Study. Scand J. Med. Sci. Sports 2022, 32, 1768–1780. [Google Scholar] [CrossRef]
- McClung, C.A. Circadian genes, rhythms and the biology of mood disorders. Pharmacol. Ther. 2007, 114, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Bunney, W.E.; Bunney, B.G. Molecular clock genes in man and lower animals: Possible implications for circadian abnormalities in depression. Neuropsychopharmacology 2000, 22, 335–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Ferrara, P.; Pennisi, F.; Casu, G.; Amerio, A.; Odone, A.; Nucci, D.; Dinu, M. Association between Daily Pattern of Physical Activity and Depression: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6505. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Blandi, L.; Cacitti, S.; Minelli, M.; Signorelli, C.; Amerio, A.; Odone, A. Depression and Objectively Measured Physical Activity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3738. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 344) | Men (n = 90) | Women (n = 254) | p-Value | |
|---|---|---|---|---|
| Age (years) * | 33.5 ± 13 | 31.5 ± 12.4 | 34.1 ± 12.9 | 0.05 |
| Marital status | ||||
| Unmarried/single, n (%) | 205 (59.6) | 61 (67.8) | 144 (56.7) | 0.06 |
| Education level | ||||
| University, n (%) | 210 (61.1) | 49 (54.4) | 161 (63.4) | 0.13 |
| Body weight (kg) * | 66.1 ± 14.4 | 78.8 ± 14.1 | 61.5 ± 11.4 | <0.001 |
| BMI (kg/m2) * | 23.5 ± 4.3 | 25.1 ± 4 | 22.9 ± 4.2 | <0.001 |
| Ponderal status | ||||
| Overweight or obese, n (%) | 89 (25.9) | 36 (40.0) | 53 (20.9) | <0.001 |
| Smoking habit | ||||
| Yes | 58 (16.9) | 15 (16.7) | 43 (16.9) | 0.95 |
| Physical activity | ||||
| Sedentary lifestyle, n (%) | 112 (32.5) | 17 (18.9) | 95 (37.4) | 0.001 |
| DASS-21 score | ||||
| Depression symptoms, n (%) | 76 (22.1) | 16 (17.8) | 60 (23.6) | 0.25 |
| Anxiety symptoms, n (%) | 80 (23.3) | 4 (4.4) | 30 (11.8) | 0.08 |
| Stress symptoms, n (%) | 34 (9.9) | 15 (16.7) | 65 (25.6) | 0.04 |
| Medi-Lite score | 10.2 ± 2.5 | 10.0 ± 2.5 | 10.2 ± 2.5 | 0.40 |
| MEQ | ||||
| Evening chronotype, n (%) | 25 (7.6) | 6 (6.6) | 20 (7.8) | 0.77 |
| Intermediate chronotype, n (%) | 184 (53.5) | 51 (56.7) | 133 (52.4) | |
| Morning chronotype, n (%) | 134 (39.0) | 33 (36.7) | 101 (39.8) |
| OR | 95% CI | p-Value | aOR | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Depression symptoms | ||||||
| Age (years) | 0.95 | 0.92-0.99 | 0.01 | 0.94 | 0.92-0.97 | <0.001 |
| Unmarried/single | 2.90 | 1.56-5.38 | 0.22 | - | - | - |
| Sedentary lifestyle | 2.31 | 1.32-4.06 | 0.002 | 2.51 | 1.45-4-37 | 0.001 |
| Lowest adherence to the MD * | 1.35 | 0.79-2.32 | 0.25 | - | - | - |
| Evening chronotype | 2.06 | 0.87-4.88 | 0.15 | - | - | - |
| Anxiety symptoms | ||||||
| Age (years) | 0.98 | 0.95-1.01 | 0.28 | - | - | - |
| Smokers | 1.64 | 0.84-3.17 | 0.14 | - | - | - |
| Unmarried/single | 1.57 | 0.76-3.23 | 0.21 | - | - | - |
| Sedentary lifestyle | 2.35 | 1.34-4.12 | 0.003 | 2.13 | 1.26-3.60 | 0.004 |
| Lowest adherence to the MD * | 1.66 | 0.98-2.81 | 0.05 | 1.69 | 1.01-2.84 | 0.04 |
| Evening chronotype | 0.94 | 0.36-2.44 | 0.91 | - | - | - |
| Stress symptoms | ||||||
| Woman | 3.50 | 1.17-10.43 | 0.02 | 3.25 | 1.10-9.59 | 0.03 |
| Age (years)° | 0.94 | 0.90-0.99 | 0.01 | 0.94 | 0.90-0.98 | 0.01 |
| Unmarried/single | 3.22 | 1.34-7.70 | 0.009 | 3.13 | 1.31-7.46 | 0.01 |
| Body weight (kg) | 0.77 | 0.89-1.00 | 0.07 | - | - | - |
| BMI (kg/m2)° | 1.09 | 0.90-1.32 | 0.37 | - | - | - |
| Lowest adherence to the MD * | 1.79 | 0.86-3.72 | 0.11 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinu, M.; Lotti, S.; Napoletano, A.; Corrao, A.; Pagliai, G.; Tristan Asensi, M.; Gianfredi, V.; Nucci, D.; Colombini, B.; Sofi, F. Association between Psychological Disorders, Mediterranean Diet, and Chronotype in a Group of Italian Adults. Int. J. Environ. Res. Public Health 2023, 20, 335. https://doi.org/10.3390/ijerph20010335
Dinu M, Lotti S, Napoletano A, Corrao A, Pagliai G, Tristan Asensi M, Gianfredi V, Nucci D, Colombini B, Sofi F. Association between Psychological Disorders, Mediterranean Diet, and Chronotype in a Group of Italian Adults. International Journal of Environmental Research and Public Health. 2023; 20(1):335. https://doi.org/10.3390/ijerph20010335
Chicago/Turabian StyleDinu, Monica, Sofia Lotti, Antonia Napoletano, Abigail Corrao, Giuditta Pagliai, Marta Tristan Asensi, Vincenza Gianfredi, Daniele Nucci, Barbara Colombini, and Francesco Sofi. 2023. "Association between Psychological Disorders, Mediterranean Diet, and Chronotype in a Group of Italian Adults" International Journal of Environmental Research and Public Health 20, no. 1: 335. https://doi.org/10.3390/ijerph20010335