1. Introduction
The brains of young children below 6 years old are at the most critical stage of development [
1]. Any prolonged environmental exposure such as exposure to digital screens might influence neural growth leading to a variety of consequences [
2]. Nowadays, children are using screens extensively at an increasingly younger age with some starting as early as infancy [
3,
4]. Population surveys have shown that young children use the screen for more than 1 to 2 h per day [
5,
6].
Excessive screen time in children is associated with many health and psychological consequences such as obesity, language development delays, poorer cognition, behavioural problems, and emotional dysregulations [
7,
8,
9,
10,
11,
12]. More recent studies supported these associations by discovering microstructural changes in the developing brain especially in the tracts involved in language, visual processing, executive functions, and multimodal association [
2,
13,
14]. Because of this, the American Academy of Pediatrics (AAP) recommends young children from the age of 2 to 5 years old should use screens for less than one hour per day; and advises not to expose children less than 18 to 24 months old to any screen media [
9].
Screen dependency is another problem associated with the prolonged use of screens, leading to addiction symptoms similar to substance addiction, such as loss of control and negative emotions (such as irritability and anxiety) when the screen is not available [
13,
15]. To date, the World Health Organization’s (WHO) International Statistical Classification of Diseases and Related Health Problems 11th edition (ICD-11) and the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), have placed Internet Gaming Disorder (IGD) in the section of conditions for further research in the DSM-5 [
16,
17]. Neurologically, IGD has the same brain structure (frontostriatal and frontocingulate) changes similar to other addictions [
18,
19].
Screen dependency is defined as the problematic use of screen media which covers all types of media transmitted through a screen, such as smartphones, tablets, laptops, televisions, portable video games, and so on [
2]. For young children, it is difficult to group them to a specific media since they are generally exposed to all types of screen media [
2,
20,
21]. Because of this, they are continuously exposed to media via the different types of screens that are available to them.
However, research on screen media-related dependencies or addictions has focused primarily on adults, teenagers, and adolescents since most questionnaires were developed for this group. Up to the year 2020, questionnaires for young children were scarce, with a review finding only three questionnaires developed specifically for young children below 10 years old [
20,
22,
23,
24]. Out of this, only one was a parent-report measure suitable for children from the age of 4 to 11 years old [
22]. Parent reports are quick, easy to use, and cost effective. The concurrent validity of the parent report was high for judging language skills identifying language delay. There were no differences in the rating accuracy of mothers with different educational levels. It was also good at reporting behavioural and conduct problems. As of the date of writing, questionnaires for screen media dependency developed and validated specifically for pre-school children are not available. Hence, not much is known about screen media dependency in this age group, from basic information such as its prevalence in the population and its associated factors. Pre-school children are the group of interest since early exposure and prolonged use at the age of the most rapid brain development could cause complications that are substantial if not detected and subject to early intervention. Hence, this study aimed to develop and validate a screen-media dependency questionnaire for pre-school children.
2. Methods
2.1. Participants
Our study population were parents (either the father or mother) with children attending registered pre-school centres in Kuantan, Malaysia, and our target population was the preschool children aged 4 to 6 years old attending registered preschool centres in Kuantan, Malaysia. Inclusion criteria were parents of children aged 4 to 6 years old, who were using any type of digital device; Malaysian citizens; and literate in Bahasa Malaysia. Children with other medical disorders such as ADHD, autistic-like behaviour, or congenital disorders were excluded. The data were obtained from 386 children via stratified random sampling based on the list of registered preschools centres.
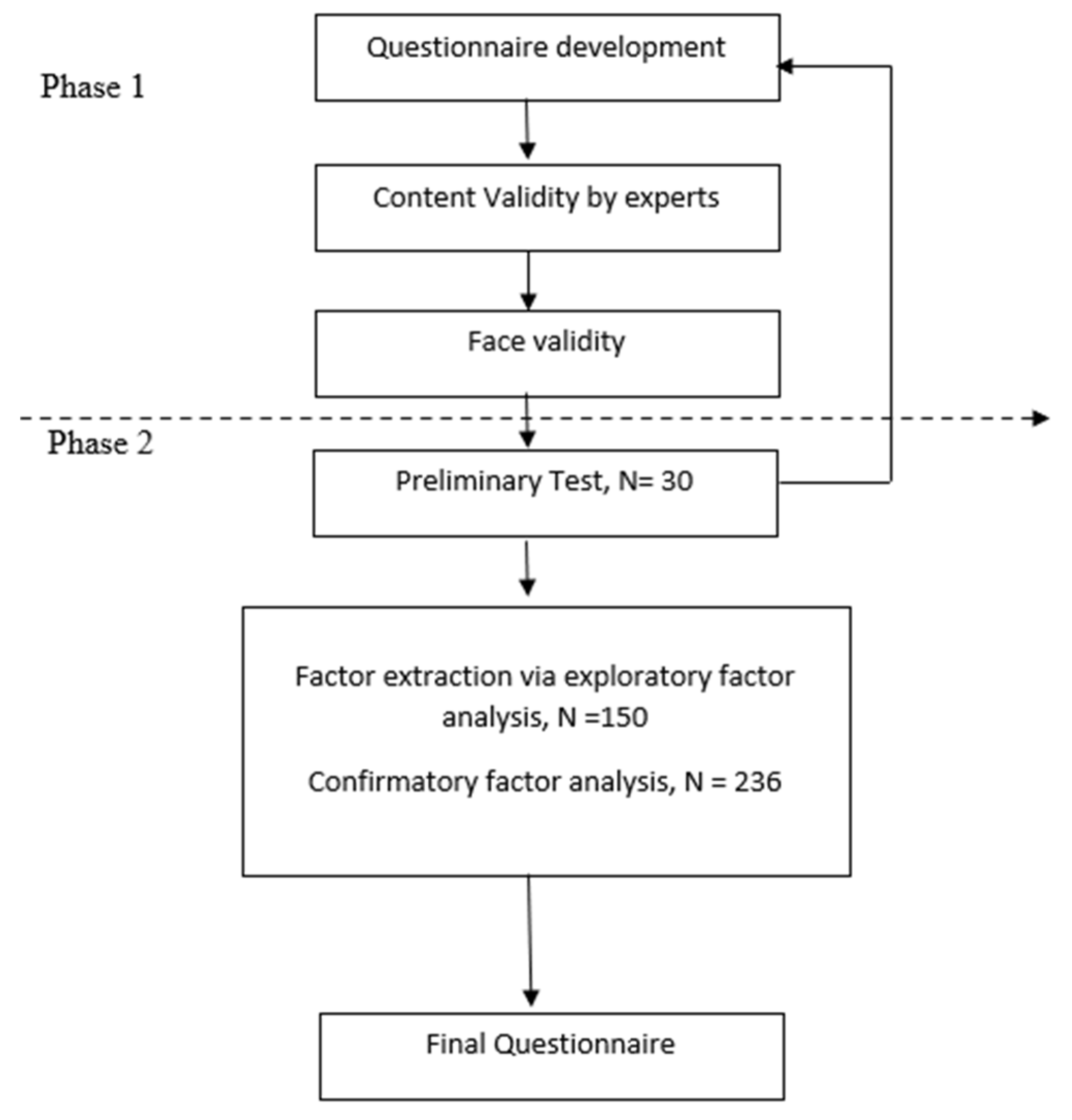
2.2. Procedure
This is a cross sectional validation study, which was divided into 2 phases, and is summarized by the flowchart in
Figure 1.
2.2.1. Phase 1
Phase 1 comprised of screening questionnaire formulation, content validity, and face validity. The team that was involved included two family medicine specialists, two psychiatrists, and one public health specialist. The items of the SDS were created based on the IGD criteria in the DSM-5, content from other literature, and clinical experience. A total of 40 items were produced which covered the domains of the child’s preoccupation with screen media; loss of control over child’s screen media use; child’s withdrawal symptoms; child’s craving; social or lifestyle impairment; the dangerous consequences of screen media use; the child’s increasing tolerance; use of deception associated with screen media and physical complaints due to excessive use. The items were developed in statement forms and parent-report style since the target populations were pre-school children. The initial pool of items was reviewed and revised before proceeding to content and face validity. It was also checked by a language expert to ensure the proper and correct use of language.
Four experts were involved in the content validity which were: a child and adolescent psychiatrist; an addiction medicine psychiatrist; a family medicine specialist; and a child psychologist. Expert opinion was given based on the content of the questionnaire, whether it adequately captured screen dependency among pre-schoolers. This included the domain used and the items within each domain. Other than that, whether each item represented the domain or a different domain, whether the item(s) should be included or excluded in the questionnaire, the percentage for each item should be included in the questionnaire based on its significance, and any suggestions for improvement of the questionnaire. Revisions were made based on the feedback given. The preliminary version of the questionnaire after content validity comprised of 30 items distributed over 7 domains.
Face validity was completed next to check whether the item produced was comprehensible for the population and did not contain any medical jargon. This was achieved by sending the questionnaire to five parents/guardians who fulfilled the inclusion criteria and were not involved in the full-scale study later.
2.2.2. Phase 2
Phase 2 included a pre-test, the actual field study (larger population), data collection, and analysis.
A pre-test on 30 participants was carried out to detect any confusion on items, and whether respondents had suggestions for possible improvements of the items. It also gave a rough idea of the response distribution to each item, which was important in determining whether there was enough variation in the response to justify moving forward with a larger-scale test. This also provided feedback on the data collection flow before proceeding with the larger field study.
The larger field study consisted of two samples for factor extraction analysis using exploratory factor analysis and dimensionality via confirmatory factor analysis, respectively [
25]. It was recommended that EFA should have a sample size of at least 50 respondents or a respondents-to-items ratio of 5:1 and that CFA should have a sample size of at least 200 respondents [
26]. In this study, the first sample consisted of 150 participants and the second sample consisted of 236 participants, which was higher than the recommendations, and which had the advantage, among others, of better item ratio and lower measurement errors [
27].
2.3. Data Collection Procedure
A list of selected pre-schools was obtained from the State Education Department. The selected pre-schools were approached individually by the researcher. The teacher was briefed regarding the research. Any questions regarding the research were answered before the distribution of the questionnaire. After adequate explanation and consent was given by the pre-school centre, the teacher then shared with the parents the summary of the research and patient information sheet via a WhatsApp® group. Any questions regarding the research were replied by the researcher. Only then, with the help of the teacher, was the link to the questionnaire distributed via the WhatsApp® group. The questionnaire was in Google® forms given the pandemic situation to help minimize visits to pre-school centres. This method also helped parents to interact directly with the researcher as well as ensuring appropriate time for the parent to give their responses. The parent needed to fill in the consent form before they could proceed with the questionnaire. All the responses were automatically sent to the researcher after completion. The data collection was executed from 1 October 2020 to 28 February 2021.
2.4. Assessment Materials
This study instrument comprised of 2 sections. Section A was the sociodemographic data of the population. This was to provide additional information regarding the subject of the study regarding the parent, children, environment as well as the media viewing habits of the children in this study.
Section B consisted of the newly developed SDS questionnaire to detect screen dependency disorder. The questionnaire was in Bahasa Malaysia, suitable for the Bahasa Malaysia-speaking population, which is the majority in this country. A Likert scale was used for item scoring. This study used a 4-point Likert scale, ‘Strongly disagree’, ‘Disagree’, ‘Agree’, and ‘Strongly Agree’ with a score of ‘1’, ‘2’, ‘3’, and ‘4’, respectively.
6. Discussion
Increased screen time is associated with many negative consequences on children’s physical and mental health. Because of this, the APA recommends that young children from the age of 2 to5 years old only be exposed to good quality media content for less than 1 h per day [
9]. The sociodemographic data in this study showed that during weekdays, only a minority of children followed this recommendation, and this number was even less during the weekends. Clearly, the children in this study use the screen more than the current recommendations, which is similar to other local and international population studies [
5,
6].
In recent times, the advancement of the internet has allowed for media content to be streamed at any time, making this a preferred choice of media delivery as compared to traditional media (television broadcast, cable, and satellite). Hence the popularity of digital-ready devices such as mobile phones which can access digital media at any time and place. However, modern television is now equipped with internet capabilities that can be used to watch online media. Therefore, despite the increasing utilization of smartphones among young children, the television continues to also be utilized by young children [
3]. This is consistent with the finding that most of the children in this study used the smartphone and the television as opposed to other screen devices. This is also in line with the finding that the main on-screen activity for pre-school children in this study is watching online videos, playing video games, and using educational apps. The combination of the availability of both continuous media content and digital-ready devices, which are available both on the go and at home, contributes to the prolonged and excessive use of the screen which could lead to screen dependency.
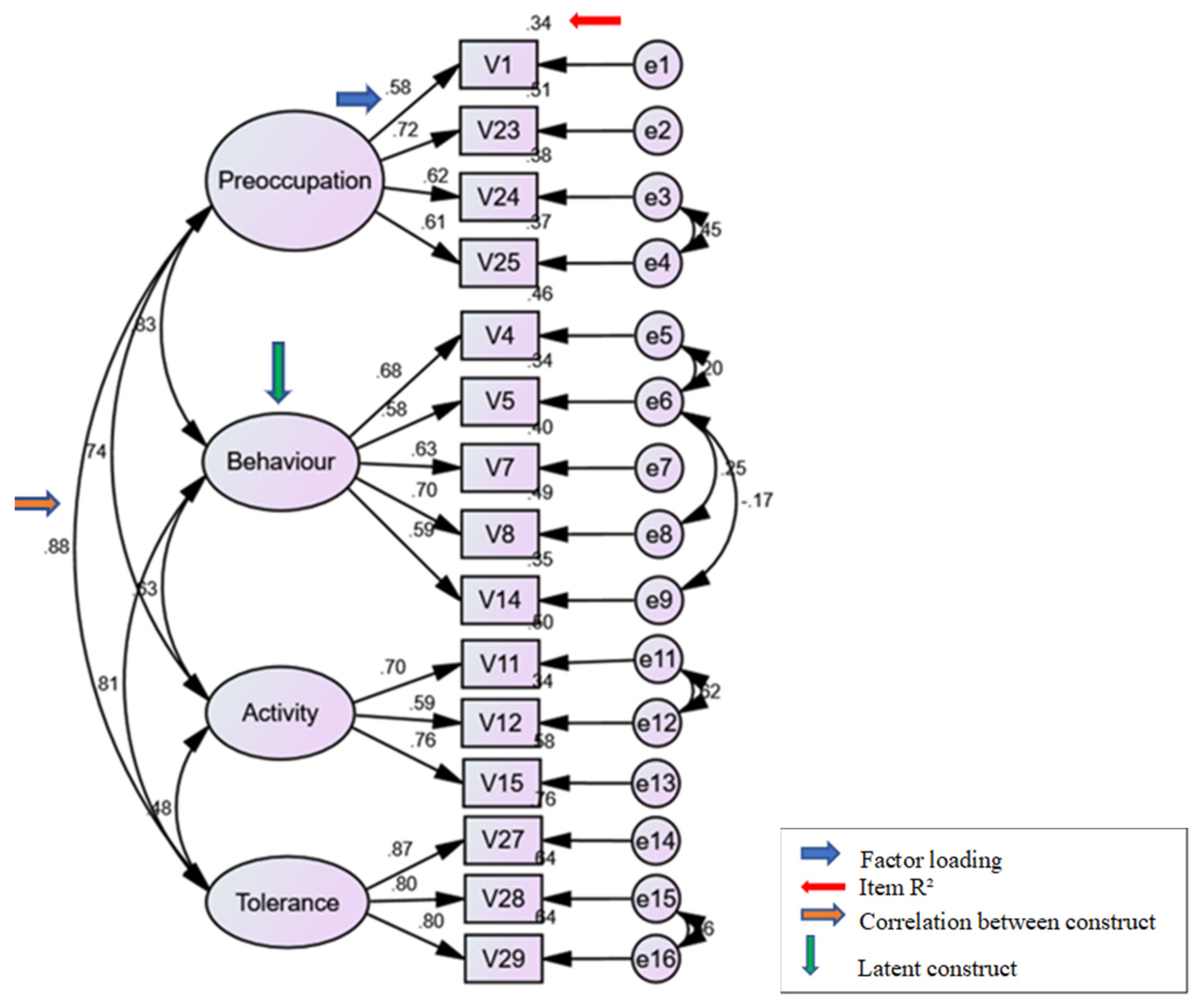
The main purpose of this study was to develop a sound and reliable psychometric screening questionnaire to assess screen dependency among pre-school children. As elaborated above, the SDS underwent a robust psychometric analysis and demonstrated adequate results on the construct validity and excellent internal consistency, proving that the SDS is a valid and reliable tool to be used.
The SDS was developed based on the DSM-5’s IGD criteria and other literature on addiction [
16,
36,
37]. The final 15 items under 4 domains covered important areas in the DSM-5’s IGD. The four domains are “Preoccupation with screen media”, “Behavioural issues related to screen media use”, “Effect on daily life activities”, and “Parent’s perception on child’s screen media tolerance”. The “Preoccupation with screen media” domain reflects the child’s obsession with the screen to the extent that he/she asks for the screen at every possible moment. The “Behavioural issues related to screen media use” domain reflects the withdrawal criteria in DSM-5’s IGD. In behavioural addiction, withdrawal manifests primarily as symptoms, with lesser physical signs as seen in pharmacological withdrawal [
38]. Symptoms such as irritability or anxiety from a young child, either from the use of the screen or from the effect of stopping the screen itself, can be obtained from the parent’s observations of the child’s behaviour. The questions in this domain also capture the negative behaviour that occurs from the difficulty in controlling the child’s screen use. The “effect on daily life” domain covers one of the most important areas in screen dependency: excessive use to the extent of affecting the normal functioning of daily living [
2,
21]. The DSM-5 notes the severity of dependency depends on the degree of daily activities that are affected [
16]. The final domain covers tolerance which is the need to use the screen longer or more frequently to obtain the same satisfying effect [
38]. The sentence structure in this domain was constructed based on the parents’ perception since tolerance is difficult to determine from a third person. However, in a young child who is still dependent on their parents, the parents’ observation of their child’s activities is legitimate, as seen in other studies on the accuracy of parental observations [
39,
40]. The SDS covers important domains that capture screen dependency in children, within the scope of 15 items, which can be answered within 5 min, making it a suitable tool to be used for busy parents and in combination with other questionnaires in future epidemiological studies.
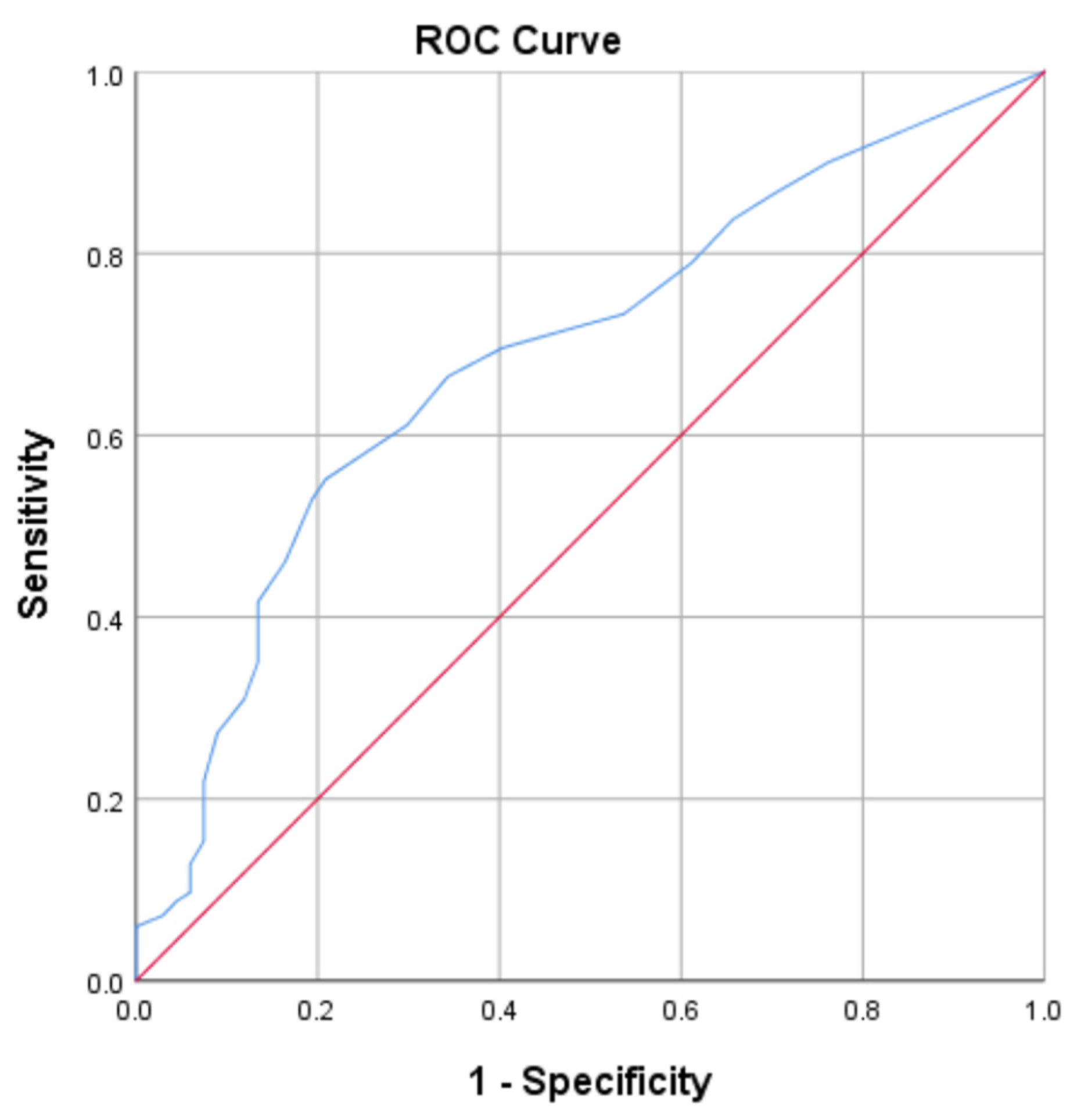
The SDS can be scored from the lowest to the highest possible scores of 15 to 60, with the higher score meaning higher dependency to the screen. The mean score for the participants of this study is 25.58, which is above the cut-off score of 24.5. Slightly more participants (50.8%) fall into the non-dependent group, and 49.2% are in the dependant group.
This study has its limitations. The SDS was developed in Bahasa Malaysia and is a good questionnaire to be used among Malaysians that are well-versed in this language. Therefore, it is recommended that this questionnaire be validated in other languages and cultures. This study also suffers from recall and social desirability bias, which is a common limitation of self- or parent-report measures. Apart from that, this study did not undergo further validation to assess its relationship with other variables/measures, such as against a gold standard (criterion validity) or other similar measures (convergent validity). This is due to the fact that there is no gold standard for screen dependency diagnoses at this moment. However, future research can include further validation against clinical diagnosis once a standardized diagnostic criterion is established.
There is heated debate among researchers on whether categories are acceptable in psychological research since some psychological disorders such as personality disorders or pathological worry degree of severity exist as a unidimensional spectrum and categorizing may mask its underlying reality, while other psychological disorders such as addiction, depression, or eating disorders have a clear latent construct to differentiate normal and abnormal [
41,
42]. Statistically, it is also recommended that scores of psychological illnesses be best interpreted in continuous data rather than in categories to minimize errors [
43,
44]. However, it is also argued that it is practical to have cut-off scores to facilitate the clinical assessment and for comparison in future epidemiological studies [
41]. The cut-off in this study, again, is suitable for this population and it is recommended to compare with cut-off scores elicited in clinical samples or with other similar questionnaires for further validation.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}