
Dexmedetomidine Increases MMP-12 and MBP Concentrations after Coronary Artery Bypass Graft Surgery with Extracorporeal Circulation Anaesthesia without Impacting Cognitive Function: A Randomised Control Trial
 , , , , , and
, , , , , and
Abstract
:1. Introduction
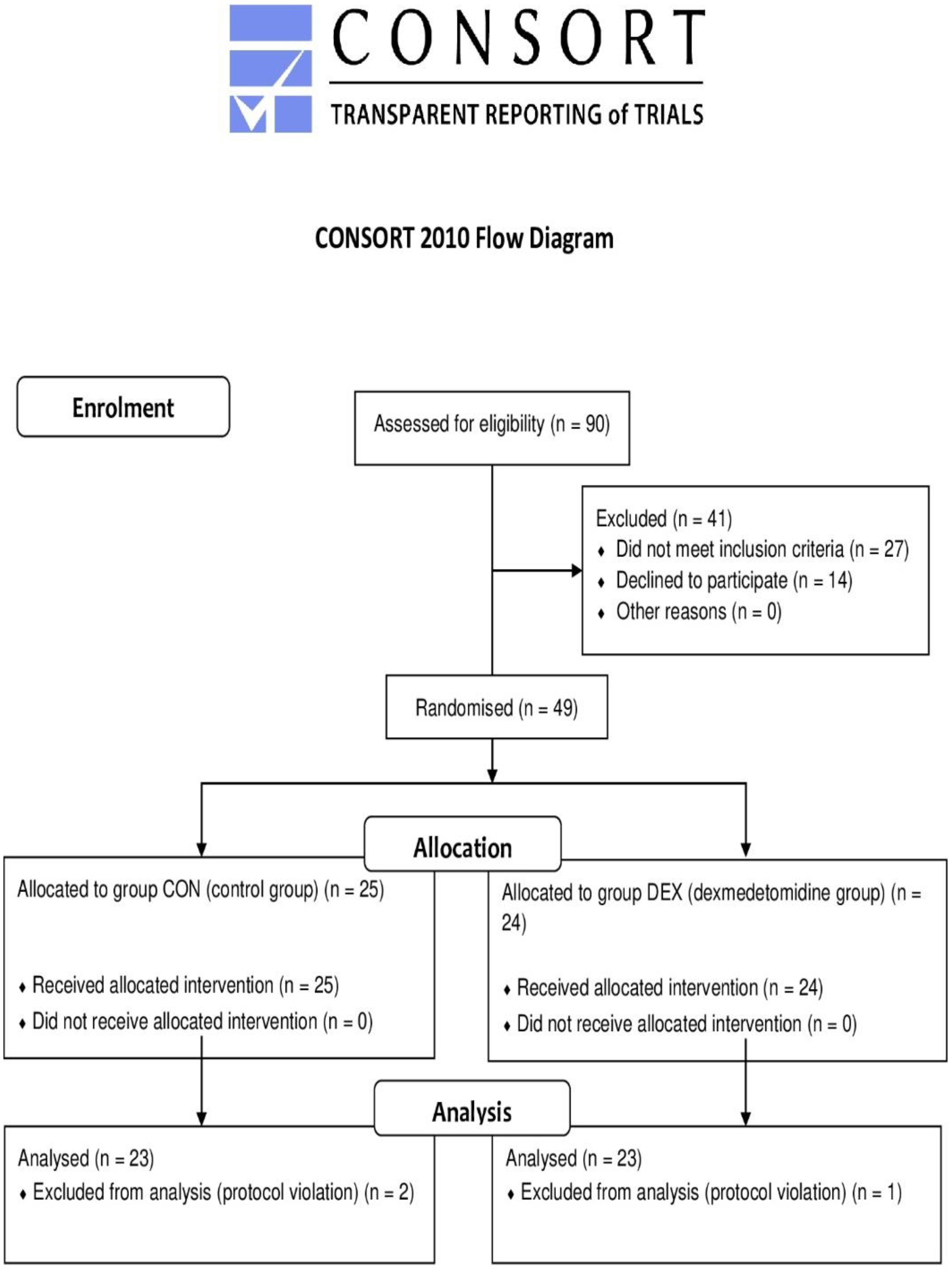
2. Materials and Methods
2.1. Anaesthetic and Surgical Procedures
2.2. Biomarker Measurement
2.3. Cognitive Function Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and Perioperative Data
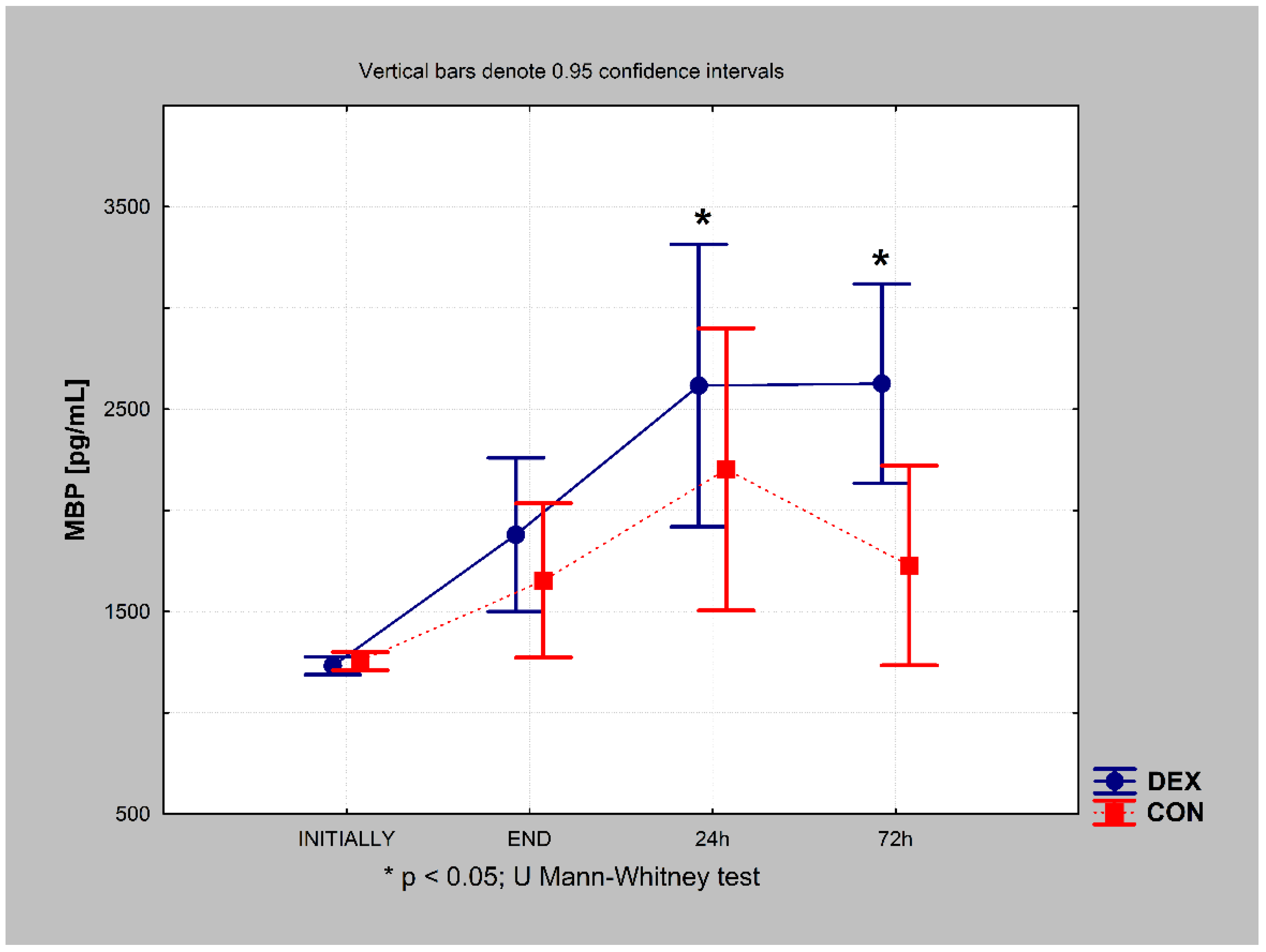
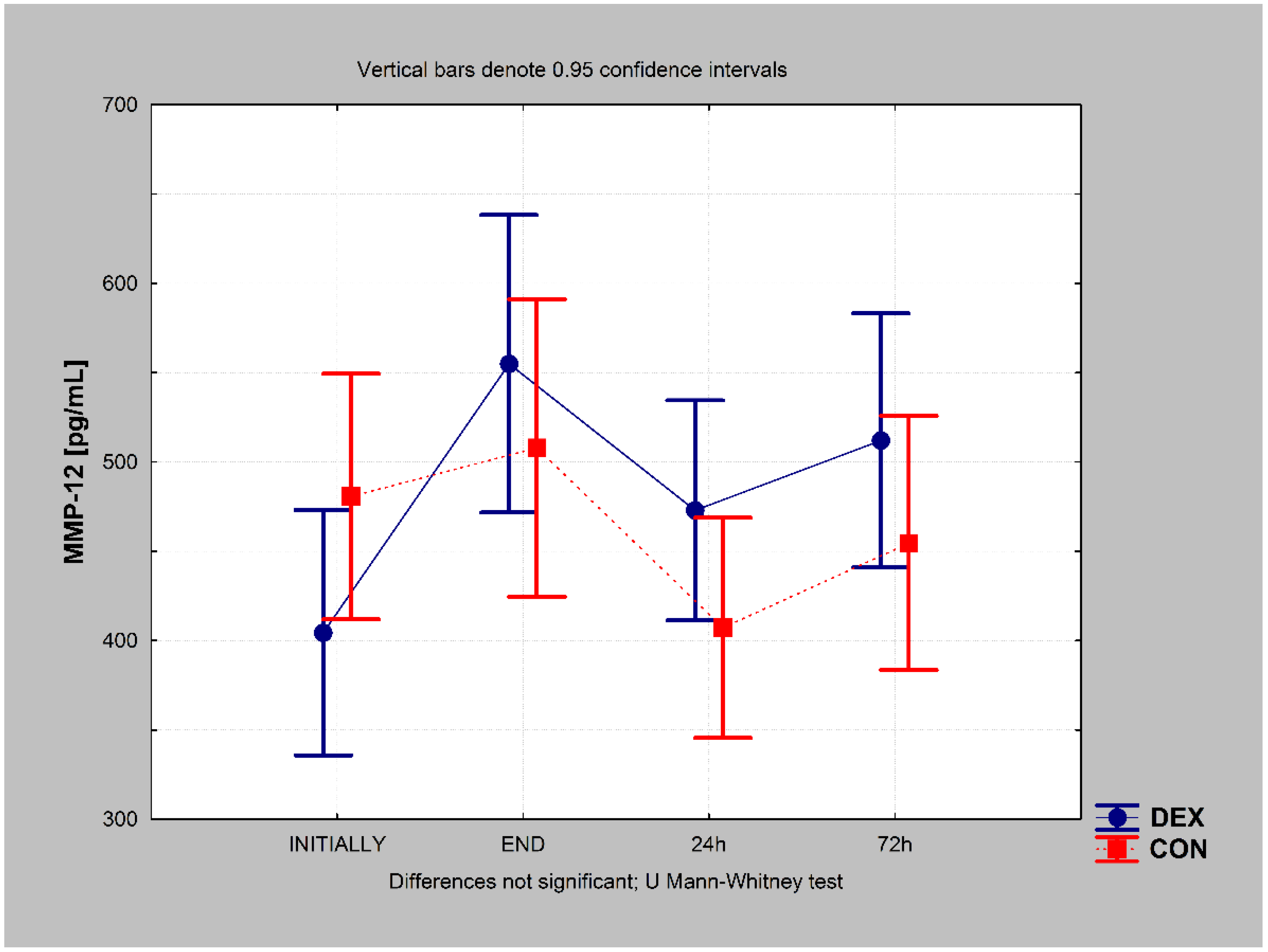
3.2. Biomarker Concentrations
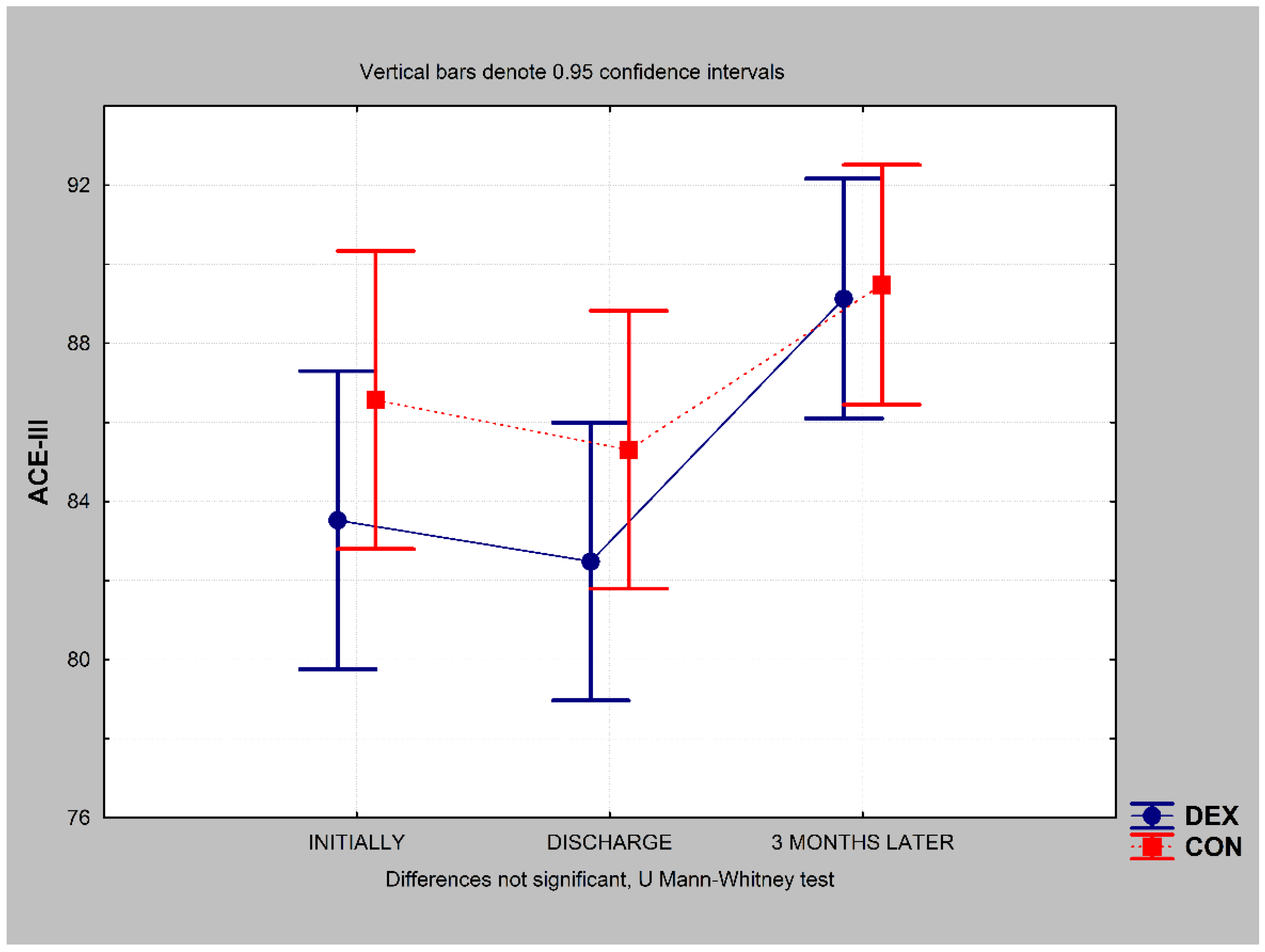
3.3. Cognitive Function
3.4. Domain-Specific Results for Cognitive Function
3.4.1. Attention
3.4.2. Memory
3.4.3. Fluency
3.4.4. Language
3.4.5. Visuospatial Abilities
3.5. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hammon, J.W. Brain Protection during Cardiac Surgery: Circa 2012. J. Extra Corpor. Technol. 2013, 45, 116–121. [Google Scholar] [PubMed]
- Kowalczyk, M. Perioperative Monitoring of Central Nervous System’s Functions. Anestezjologia I Ratownictwo 2017, 11, 336–341. [Google Scholar]
- Funder, K.S.; Steinmetz, J.; Rasmussen, L.S. Cognitive Dysfunction after Cardiovascular Surgery. Minerva Anestesiologica 2009, 75, 4. [Google Scholar]
- Ramlawi, B.; Rudolph, J.L.; Mieno, S.; Khabbaz, K.; Sodha, N.R.; Boodhwani, M.; Levkoff, S.E.; Marcantonio, E.R.; Sellke, F.W. Serologic Markers of Brain Injury and Cognitive Function after Cardiopulmonary Bypass. Ann. Surg. 2006, 244, 593–601. [Google Scholar] [CrossRef]
- Rasmussen, L.S. Postoperative Cognitive Dysfunction: Incidence and Prevention. Best Practice Res. Clin. Anaesthesiol. 2006, 20, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Mathuranath, P.S.; Nestor, P.J.; Berrios, G.E.; Rakowicz, W.; Hodges, J.R. A Brief Cognitive Test Battery to Differentiate Alzheimer’s Disease and Frontotemporal Dementia. Neurology 2000, 55, 1613–1620. [Google Scholar] [CrossRef]
- So, M.; Foxe, D.; Kumfor, F.; Murray, C.; Hsieh, S.; Savage, G.; Ahmed, R.M.; Burrell, J.R.; Hodges, J.R.; Irish, M.; et al. Addenbrooke’s Cognitive Examination III: Psychometric Characteristics and Relations to Functional Ability in Dementia. J. Int. Neuropsychol. Soc. 2018, 24, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.; Clugston, A.; Croucher, M.; Malone, D.; Mau, E.; Sims, A.; Gee, S. Performance of Three Cognitive Screening Tools in a Sample of Older New Zealanders. Int. Psychogeriatr. 2015, 27, 981–989. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Cortés-Martínez, A.; Valles-Salgado, M.; Rognoni, T.; Fernández-Matarrubia, M.; Moreno-Ramos, T.; Matías-Guiu, J. Addenbrooke’s Cognitive Examination III: Diagnostic Utility for Mild Cognitive Impairment and Dementia and Correlation with Standardized Neuropsychological Tests. Int. Psychogeriatr. 2017, 29, 105–113. [Google Scholar] [CrossRef]
- Phillips-Bute, B.; Mathew, J.P.; Blumenthal, J.A.; Grocott, H.P.; Laskowitz, D.T.; Jones, R.H.; Mark, D.B.; Newman, M.F. Association of Neurocognitive Function and Quality of Life 1 Year After Coronary Artery Bypass Graft (CABG) Surgery. Psychosom. Med. 2006, 68, 369–375. [Google Scholar] [CrossRef]
- Kowalczyk, M.; Nestorowicz, A.; Fijałkowska, A.; Kwiatosz-Muc, M. Emotional Sequelae among Survivors of Critical Illness: A Long-Term Retrospective Study. Eur. J. Anaesthesiol. 2013, 30, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, P. Markers of Cerebral Ischemia after Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 1996, 10, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Hernández-García, C.; Rodríguez-Rodríguez, A.; Egea-Guerrero, J.J. Brain Injury Biomarkers in the Setting of Cardiac Surgery: Still a World to Explore. Brain Inj. 2016, 30, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, M.; Guz, M.; Okoń, E.; Jeleniewicz, W.; Grzycka-Kowalczyk, L.; Kiełbus, M.; Dudka, J.; Suseł, W.; Dąbrowski, W.; Stepulak, A. MMP-9 and MMP-2 Regulation in Patients Undergoing Non-Oncological and Non-Vascular Elective Surgery Independent of the Use of Propofol or Sevoflurane. Pharmacol. Rep. 2019, 71, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Chelluboina, B.; Warhekar, A.; Dillard, M.; Klopfenstein, J.D.; Pinson, D.M.; Wang, D.Z.; Veeravalli, K.K. Post-Transcriptional Inactivation of Matrix Metalloproteinase-12 after Focal Cerebral Ischemia Attenuates Brain Damage. Sci. Rep. 2015, 5, 9504. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Lee, S.-R.; Arai, K.; Lee, S.-R.; Tsuji, K.; Rebeck, G.W.; Lo, E.H. Lipoprotein Receptor–Mediated Induction of Matrix Metalloproteinase by Tissue Plasminogen Activator. Nat. Med. 2003, 9, 1313–1317. [Google Scholar] [CrossRef]
- Asahi, M.; Wang, X.; Mori, T.; Sumii, T.; Jung, J.-C.; Moskowitz, M.A.; Fini, M.E.; Lo, E.H. Effects of Matrix Metalloproteinase-9 Gene Knock-Out on the Proteolysis of Blood–Brain Barrier and White Matter Components after Cerebral Ischemia. J. Neurosci. 2001, 21, 7724–7732. [Google Scholar] [CrossRef] [Green Version]
- Lo, E.H.; Dalkara, T.; Moskowitz, M.A. Mechanisms, Challenges and Opportunities in Stroke. Nat. Rev. Neurosci. 2003, 4, 399–414. [Google Scholar] [CrossRef]
- Lee, S.-R.; Lo, E.H. Induction of Caspase-Mediated Cell Death by Matrix Metalloproteinases in Cerebral Endothelial Cells after Hypoxia—Reoxygenation. J. Cereb. Blood Flow Metab. 2004, 24, 720–727. [Google Scholar] [CrossRef] [Green Version]
- Gu, Z. A Highly Specific Inhibitor of Matrix Metalloproteinase-9 Rescues Laminin from Proteolysis and Neurons from Apoptosis in Transient Focal Cerebral Ischemia. J. Neurosci. 2005, 25, 6401–6408. [Google Scholar] [CrossRef] [Green Version]
- Gasche, Y.; Fujimura, M.; Morita-Fujimura, Y.; Copin, J.-C.; Kawase, M.; Massengale, J.; Chan, P.H. Early Appearance of Activated Matrix Metalloproteinase-9 after Focal Cerebral Ischemia in Mice: A Possible Role in Blood—Brain Barrier Dysfunction. J. Cereb. Blood Flow Metab. 1999, 19, 1020–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heo, J.H.; Lucero, J.; Abumiya, T.; Koziol, J.A.; Copeland, B.R.; del Zoppo, G.J. Matrix Metalloproteinases Increase Very Early during Experimental Focal Cerebral Ischemia. J. Cereb. Blood Flow Metab. 1999, 19, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Mun-Bryce, S.; Rosenberg, G.A. Matrix Metalloproteinases in Cerebrovascular Disease. J. Cereb. Blood Flow Metab. 1998, 18, 1163–1172. [Google Scholar] [CrossRef] [Green Version]
- Chelluboina, B.; Nalamolu, K.R.; Klopfenstein, J.D.; Pinson, D.M.; Wang, D.Z.; Vemuganti, R.; Veeravalli, K.K. MMP-12, a Promising Therapeutic Target for Neurological Diseases. Mol. Neurobiol. 2018, 55, 1405–1409. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Rodriguez, S.; Buxo, X.; Morancho, A.; Riba-Llena, I.; Carrera, A.; Bustamante, A.; Giralt, D.; Montaner, J.; Martinez, C.; et al. Plasma Matrix Metalloproteinases in Patients with Stroke During Intensive Rehabilitation Therapy. Arch. Phys. Med. Rehabil. 2016, 97, 1832–1840. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Kobayashi, T.; Katoh, M.; Saito, S.; Ikeda, Y.; Kobori, M.; Masuho, Y.; Watanabe, T. Expression and Localization of Matrix Metalloproteinase-12 in the Aorta of Cholesterol-Fed Rabbits. Am. J. Pathol. 1998, 153, 109–119. [Google Scholar] [CrossRef]
- Chandler, S.; Cossins, J.; Lury, J.; Wells, G. Macrophage Metalloelastase Degrades Matrix and Myelin Proteins and Processes a Tumour Necrosis Factor-α Fusion Protein. Biochem. Biophys. Res. Comm. 1996, 228, 421–429. [Google Scholar] [CrossRef]
- azzaq Belaaouaj, A.; Li, A.; Wun, T.-C.; Welgus, H.G.; Shapiro, S.D. Matrix Metalloproteinases Cleave Tissue Factor Pathway Inhibitor. J. Biol. Chem. 2000, 275, 27123–27128. [Google Scholar] [CrossRef]
- Dong, Z.; Kumar, R.; Yang, X.; Fidler, I.J. Macrophage-Derived Metalloelastase Is Responsible for the Generation of Angiostatin in Lewis Lung Carcinoma. Cell 1997, 88, 801–810. [Google Scholar] [CrossRef] [Green Version]
- Cornelius, L.A.; Nehring, L.C.; Harding, E.; Bolanowski, M.; Welgus, H.G.; Kobayashi, D.K.; Pierce, R.A.; Shapiro, S.D. Matrix Metalloproteinases Generate Angiostatin: Effects on Neovascularization. J. Immunol. 1998, 161, 6845–6852. [Google Scholar]
- Challa, S.R.; Nalamolu, K.R.; Fornal, C.A.; Wang, B.C.; Martin, R.C.; Olson, E.A.; Ujjainwala, A.L.; Pinson, D.M.; Klopfenstein, J.D.; Veeravalli, K.K. Therapeutic Efficacy of Matrix Metalloproteinase-12 Suppression on Neurological Recovery after Ischemic Stroke: Optimal Treatment Timing and Duration. Front. Neurosci. 2022, 16, 1012812. [Google Scholar] [CrossRef] [PubMed]
- Anan’ina, T.; Kisel, A.; Kudabaeva, M.; Chernysheva, G.; Smolyakova, V.; Usov, K.; Krutenkova, E.; Plotnikov, M.; Khodanovich, M. Neurodegeneration, Myelin Loss and Glial Response in the Three-Vessel Global Ischemia Model in Rat. Int. J. Mol. Sci. 2020, 21, 6246. [Google Scholar] [CrossRef] [PubMed]
- Brandão, P.G.M.; Lobo, F.R.; Ramin, S.L.; Sakr, Y.; Machado, M.N.; Lobo, S.M. Dexmedetomidine as an Anesthetic Adjuvant in Cardiac Surgery: A Cohort Study. Braz. J. Cardiovasc. Surg. 2016, 31, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Ji, F.; Li, Z.; Young, N.; Moore, P.; Liu, H. Perioperative Dexmedetomidine Improves Mortality in Patients Undergoing Coronary Artery Bypass Surgery. J. Cardiothorac. Vasc. Anesth. 2014, 28, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, F.; Li, Z.; Nguyen, H.; Young, N.; Shi, P.; Fleming, N.; Liu, H. Perioperative Dexmedetomidine Improves Outcomes of Cardiac Surgery. Circulation 2013, 127, 1576–1584. [Google Scholar] [CrossRef] [Green Version]
- Torres, J.; Ishida, K. Neuroprotection After Major Cardiovascular Surgery. Curr. Treat. Options Neurol. 2015, 17, 28. [Google Scholar] [CrossRef]
- Raimann, F.; Adam, E.; Strouhal, U.; Zacharowski, K.; Seifert, V.; Forster, M.-T. Dexmedetomidine as Adjunct in Awake Craniotomy–Improvement or Not? Anaesthesiol. Intensive Ther. 2020, 52, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Kaczmarek, B.; Ilkowska, Z.; Kropinska, S.; Tobis, S.; Krzyminska-Siemaszko, R.; Kaluzniak-Szymanowska, A.; Wieczorowska-Tobis, K. Applying ACE-III, M-ACE and MMSE to Diagnostic Screening Assessment of Cognitive Functions within the Polish Population. Int. J. Environ. Res. Public Health 2022, 19, 12257. [Google Scholar] [CrossRef]
- Noordzij, M.; Tripepi, G.; Dekker, F.W.; Zoccali, C.; Tanck, M.W.; Jager, K.J. Sample Size Calculations: Basic Principles and Common Pitfalls. Nephrol. Dial. Transplant. 2010, 25, 1388–1393. [Google Scholar] [CrossRef] [Green Version]
- Svedin, P.; Hagberg, H.; Mallard, C. Expression of MMP-12 after Neonatal Hypoxic-Ischemic Brain Injury in Mice. Dev. Neurosci. 2009, 31, 427–436. [Google Scholar] [CrossRef]
- Nalamolu, K.R.; Chelluboina, B.; Magruder, I.B.; Fru, D.N.; Mohandass, A.; Venkatesh, I.; Klopfenstein, J.D.; Pinson, D.M.; Boini, K.M.; Veeravalli, K.K. Post-Stroke MRNA Expression Profile of MMPs: Effect of Genetic Deletion of MMP-12. Stroke Vasc. Neurol. 2018, 3, 153–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chelluboina, B.; Klopfenstein, J.D.; Pinson, D.M.; Wang, D.Z.; Vemuganti, R.; Veeravalli, K.K. Matrix Metalloproteinase-12 Induces Blood–Brain Barrier Damage After Focal Cerebral Ischemia. Stroke 2015, 46, 3523–3531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cassai, A.; Boscolo, A.; Geraldini, F.; Zarantonello, F.; Pettenuzzo, T.; Pasin, L.; Iuzzolino, M.; Rossini, N.; Pesenti, E.; Zecchino, G.; et al. Effect of Dexmedetomidine on Hemodynamic Responses to Tracheal Intubation: A Meta-Analysis with Meta-Regression and Trial Sequential Analysis. J. Clin. Anesth. 2021, 72, 110287. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, M.; Ahmadinejad, M.; Mohajerani, S.; Mirkheshti, A. Impact of Dexmedetomidine on Hemodynamic Changes during and after Coronary Artery Bypass Grafting. Ann. Card. Anaesth. 2017, 20, 152. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Qian, J.; Cheng, H.; Ji, F.; Liu, H. The Influence of Perioperative Dexmedetomidine on Patients Undergoing Cardiac Surgery: A Meta-Analysis. PLoS ONE 2016, 11, e0152829. [Google Scholar] [CrossRef]
- Turan, A.; Bashour, C.A.; You, J.; Kirkova, Y.; Kurz, A.; Sessler, D.I.; Saager, L. Dexmedetomidine Sedation after Cardiac Surgery Decreases Atrial Arrhythmias. J. Clin. Anesth. 2014, 26, 634–642. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, K.; Wang, W.; Xie, G.; Fang, X. Dexmedetomidine Sedation Reduces Atrial Fibrillation after Cardiac Surgery Compared to Propofol: A Randomized Controlled Trial. Crit. Care 2016, 20, 298. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.; Zhang, H.; Huang, L.; Liu, Y.; Liu, F.; Dong, Z. Protective Effect of Dexmedetomidine in Coronary Artery Bypass Grafting Surgery. Exp. Ther. Med. 2013, 6, 497–502. [Google Scholar] [CrossRef] [Green Version]
- The Effect of Dexmedetomidine on Myocardial Ischemia/Reperfusion Injury in Patients Undergoing Cardiac Surgery with Cardiopulmonary Bypass: A Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7409–7417. [CrossRef]
- Cheng, H.; Li, Z.; Young, N.; Boyd, D.; Atkins, Z.; Ji, F.; Liu, H. The Effect of Dexmedetomidine on Outcomes of Cardiac Surgery in Elderly Patients. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1502–1508. [Google Scholar] [CrossRef] [Green Version]
- Govêia, C.S.; de Miranda, D.B.; Oliveira, L.V.d.B.; Praxedes, F.B.; Moreira, L.G.; Guimarães, G.M.N. Dexmedetomidine Reduces Postoperative Cognitive and Behavioral Dysfunction in Adults Submitted to General Anesthesia for Non-Cardiac Surgery: Meta-Analysis of Randomized Clinical Trials. Braz. J. Anesth. (Engl. Ed.) 2021, 71, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; He, R.; Chen, S.; Qu, Y. Effect of Dexmedetomidine on Early Postoperative Cognitive Dysfunction and Peri-Operative Inflammation in Elderly Patients Undergoing Laparoscopic Cholecystectomy. Exp. Ther. Med. 2015, 10, 1635–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Du, X.; Wu, F.; Hu, Y.; Xv, Z.; Mi, W. Dexmedetomidine Improves Early Postoperative Neurocognitive Disorder in Elderly Male Patients Undergoing Thoracoscopic Lobectomy. Exp. Ther. Med. 2020, 20, 3868–3877. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Li, J.; Zhong, Y.; Guan, X.; Huang, A.; Ma, L. Effects of Dexmedetomidine on Postoperative Cognitive Function in Patients Undergoing Coronary Artery Bypass Grafting. Exp. Ther. Med. 2018, 16, 4685–4689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, M.F.; Kirchner, J.L.; Phillips-Bute, B.; Gaver, V.; Grocott, H.; Jones, R.H.; Mark, D.B.; Reves, J.G.; Blumenthal, J.A. Neurological Outcome Research Group and the Cardiothoracic Anesthesiology Research Endeavors Investigators Longitudinal Assessment of Neurocognitive Function after Coronary-Artery Bypass Surgery. N. Engl. J. Med. 2001, 344, 395–402. [Google Scholar] [CrossRef]
- Moller, J.T.; Cluitmans, P.; Rasmussen, L.S.; Houx, P.; Rasmussen, H.; Canet, J.; Rabbitt, P.; Jolles, J.; Larsen, K.; Hanning, C.D.; et al. Long-Term Postoperative Cognitive Dysfunction in the Elderly: ISPOCD1 Study. Lancet 1998, 351, 857–861. [Google Scholar] [CrossRef]
- de Vugt, M.E.; Verhey, F.R.J. The Impact of Early Dementia Diagnosis and Intervention on Informal Caregivers. Prog. Neurobiol. 2013, 110, 54–62. [Google Scholar] [CrossRef]
- DeKosky, S.T.; Marek, K. Looking Backward to Move Forward: Early Detection of Neurodegenerative Disorders. Science 2003, 302, 830–834. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.F.; Grocott, H.P.; Mathew, J.P.; White, W.D.; Landolfo, K.; Reves, J.G.; Laskowitz, D.T.; Mark, D.B.; Blumenthal, J.A. Report of the Substudy Assessing the Impact of Neurocognitive Function on Quality of Life 5 Years After Cardiac Surgery. Stroke 2001, 32, 2874–2881. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group DEX (n = 23) | Group CON (n = 23) | p-Value | |
|---|---|---|---|
| Age (years) | 67 (10) | 66 (5) | 0.854 |
| Weight (kg) | 76 (19) | 83 (16) | 0.151 |
| Height (cm) | 167 (10) | 170 (9) | 0.282 |
| EF (%) | 52 (45–60) | 60 (50–61) | 0.035 |
| Surgical time (min) | 193 (47) | 168 (31) | 0.038 |
| Anaesthetic time (min) | 248 (49) | 218 (32) | 0.017 |
| Clamping time (min) | 49 (9) | 42 (12) | 0.166 |
| ECC time (min) | 79 (29) | 67 (18) | 0.078 |
| MMP-12 initial value (pg/mL) | 388 (303–474) | 433 (352–563) | 0.267 |
| MBP initial value (pg/mL) | 1223 (1179–1302) | 1243 (1173–1339) | 0.637 |
| ACE-III initially (score 0–100) | 83 (74–92) | 88 (81–92) | 0.323 |
| CI initial value | 1.9 (1.6–2.1) | 1.9 (1.7–2.1) | 0.482 |
| CI after surgery | 2.2 (2.0–2.4) | 2.4 (2.2–2.7) | 0.057 |
| CI 24 h after surgery | 3.1 (2.8–3.3) | 3.2 (2.8–3.4) | 0.792 |
| Group DEX (n = 23) | Group CON (n = 23) | p-Value | |
|---|---|---|---|
| Comorbidities, n (%) | |||
| Myocardial infarction history | 15 (65) | 10 (43) | 0.141 |
| Heart muscle contractility disorders | 11 (48) | 14 (61) | 0.381 |
| Atrial fibrillation | 4 (17) | 3 (13) | 0.706 |
| Congestive heart failure | 2 (9) | 1 (4) | 0.495 |
| Hypertension | 21 (91) | 18 (78) | 0.230 |
| Thyroid disease | 3 (13) | 4 (17) | 0.706 |
| Preoperative medications, n (%) | |||
| β-Blockers | 19 (83) | 20 (87) | 0.706 |
| Calcium channel blockers | 12 (52) | 8 (35) | 0.251 |
| ACE inhibitors | 15 (65) | 9 (39) | 0.085 |
| Angiotensin II receptor blocker | 5 (22) | 8 (35) | 0.334 |
| Diuretics | 12 (52) | 5 (22) | 0.041 |
| Statins | 23 (100) | 22 (96) | 0.338 |
| Alcohol intake, n (%) | |||
| Occasional | 12 (52) | 14 (63) | 0.455 |
| None | 11 (48) | 9 (39) | 0.541 |
| Years of education, median (IQR) | 10 (8–11) | 12 (10–14) | 0.029 |
| Intraoperative opioids (remifentanil) | |||
| Total dose (µg), mean (SD) | 4892 (1665) | 5230 (2018) | 0.886 |
| Total dose/kg (µg/kg), mean (SD) | 63.8 (17.4) | 62.1 (19.2) | 0.748 |
| ICU length of stay (days), median (IQR) | 2 (2–3) | 3 (2–3) | 0.138 |
| Intubation time (hours), median (IQR) | 6.1 (4.9–7.0) | 7.0 (5.0–7.8) | 0.195 |
| Re-exploration for bleeding, n (%) | 2 (9) | 1 (4) | 0.495 |
| Inotrope (dobutamine) dosage | |||
| Total (mg), median (IQR) | 305 (208–450) | 133 (30–390) | 0.013 |
| Total/kg (mg/kg), median (IQR) | 4.3 (2.8–7.6) | 2.0 (0.4–3.9) | 0.005 |
| Vasoconstrictor (norepinephrine) use, n (%) | 4 (17) | 2 (9) | 0.424 |
| Delirium, n (%) | 2 (9) | 5 (22) | 0.230 |
| Group DEX (n = 23) | Group CON (n = 23) | p-Value | |
|---|---|---|---|
| Initially | 12 (52) | 8 (35) | 0.251 |
| Discharge time | 10 (44) | 9 (39) | 0.732 |
| 3 months after discharge | 6 (26) | 5 (22) | 0.752 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalczyk, M.; Panasiuk-Kowalczyk, A.; Stadnik, A.; Guz, M.; Cybulski, M.; Jeleniewicz, W.; Stepulak, A.; Kwiatosz-Muc, M. Dexmedetomidine Increases MMP-12 and MBP Concentrations after Coronary Artery Bypass Graft Surgery with Extracorporeal Circulation Anaesthesia without Impacting Cognitive Function: A Randomised Control Trial. Int. J. Environ. Res. Public Health 2022, 19, 16512. https://doi.org/10.3390/ijerph192416512
Kowalczyk M, Panasiuk-Kowalczyk A, Stadnik A, Guz M, Cybulski M, Jeleniewicz W, Stepulak A, Kwiatosz-Muc M. Dexmedetomidine Increases MMP-12 and MBP Concentrations after Coronary Artery Bypass Graft Surgery with Extracorporeal Circulation Anaesthesia without Impacting Cognitive Function: A Randomised Control Trial. International Journal of Environmental Research and Public Health. 2022; 19(24):16512. https://doi.org/10.3390/ijerph192416512
Chicago/Turabian StyleKowalczyk, Michał, Anna Panasiuk-Kowalczyk, Adam Stadnik, Małgorzata Guz, Marek Cybulski, Witold Jeleniewicz, Andrzej Stepulak, and Magdalena Kwiatosz-Muc. 2022. "Dexmedetomidine Increases MMP-12 and MBP Concentrations after Coronary Artery Bypass Graft Surgery with Extracorporeal Circulation Anaesthesia without Impacting Cognitive Function: A Randomised Control Trial" International Journal of Environmental Research and Public Health 19, no. 24: 16512. https://doi.org/10.3390/ijerph192416512