
Recommender System Based on Collaborative Filtering for Personalized Dietary Advice: A Cross-Sectional Analysis of the ELSA-Brasil Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Dietary Assessment
2.3. Sociodemographic and Clinical Characteristics
2.4. Statistical Analysis
2.5. Recommender System
3. Results
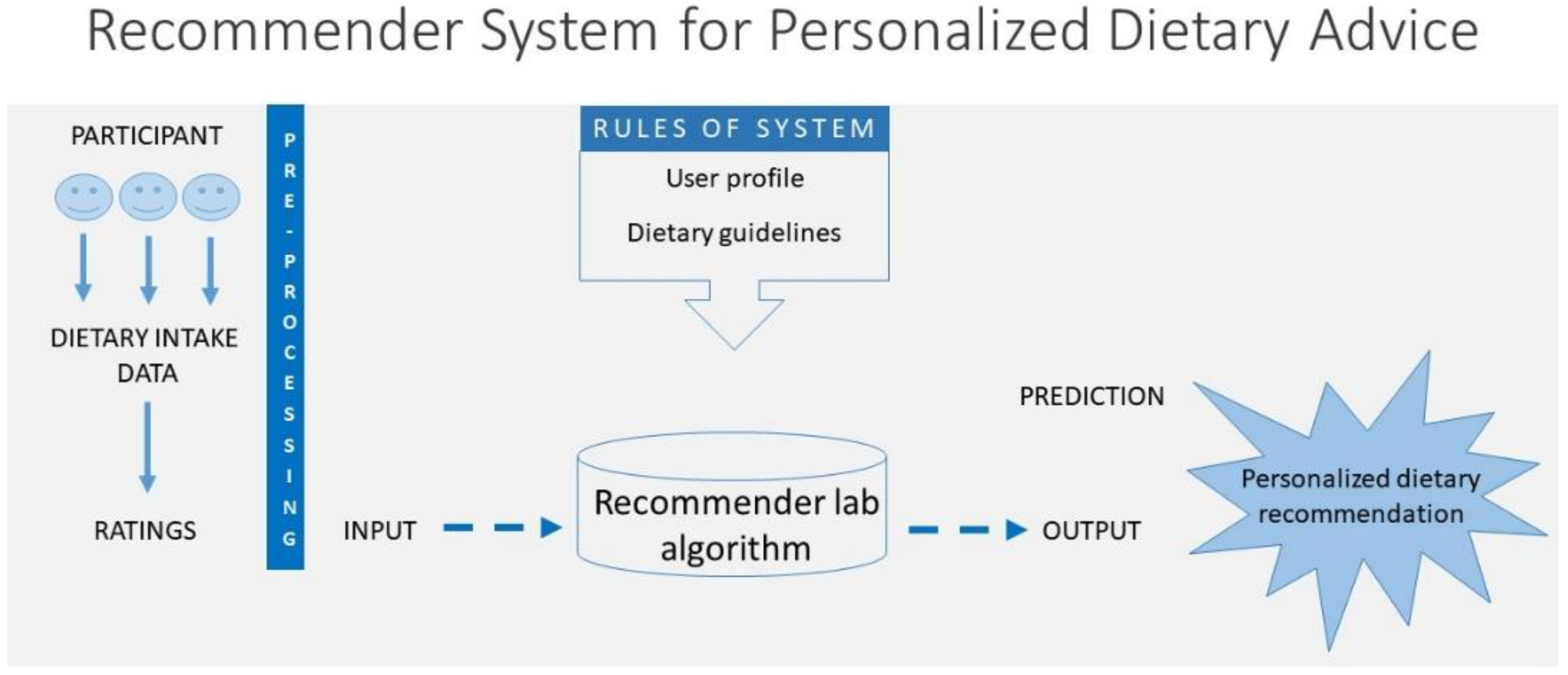
3.1. Architecture of the Recommender System
3.2. Descriptive Analyses
3.3. Food Groups and Items Eligible as Recommendations
3.4. Evaluation of Predictions
3.5. Confusion Matrix
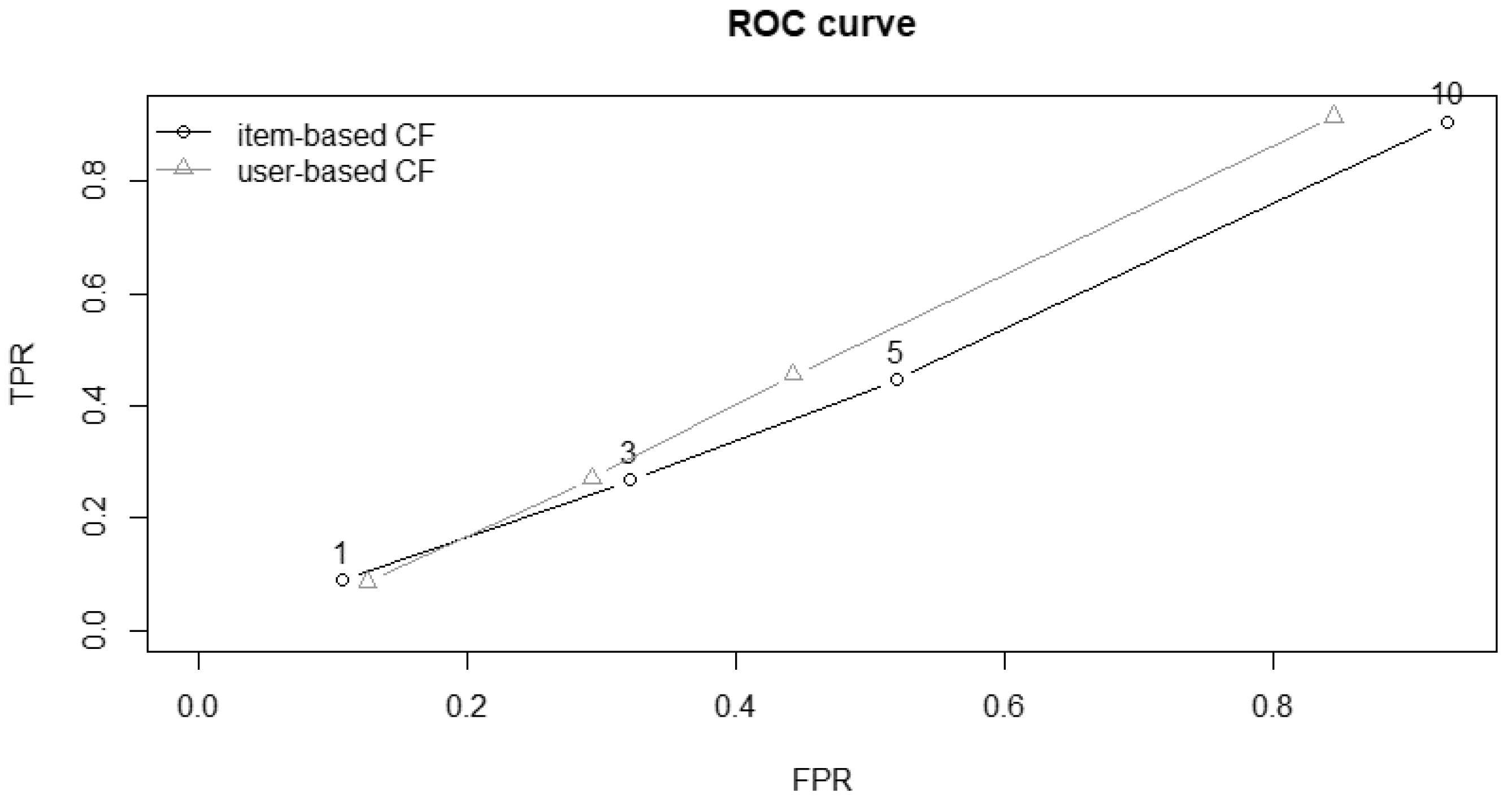
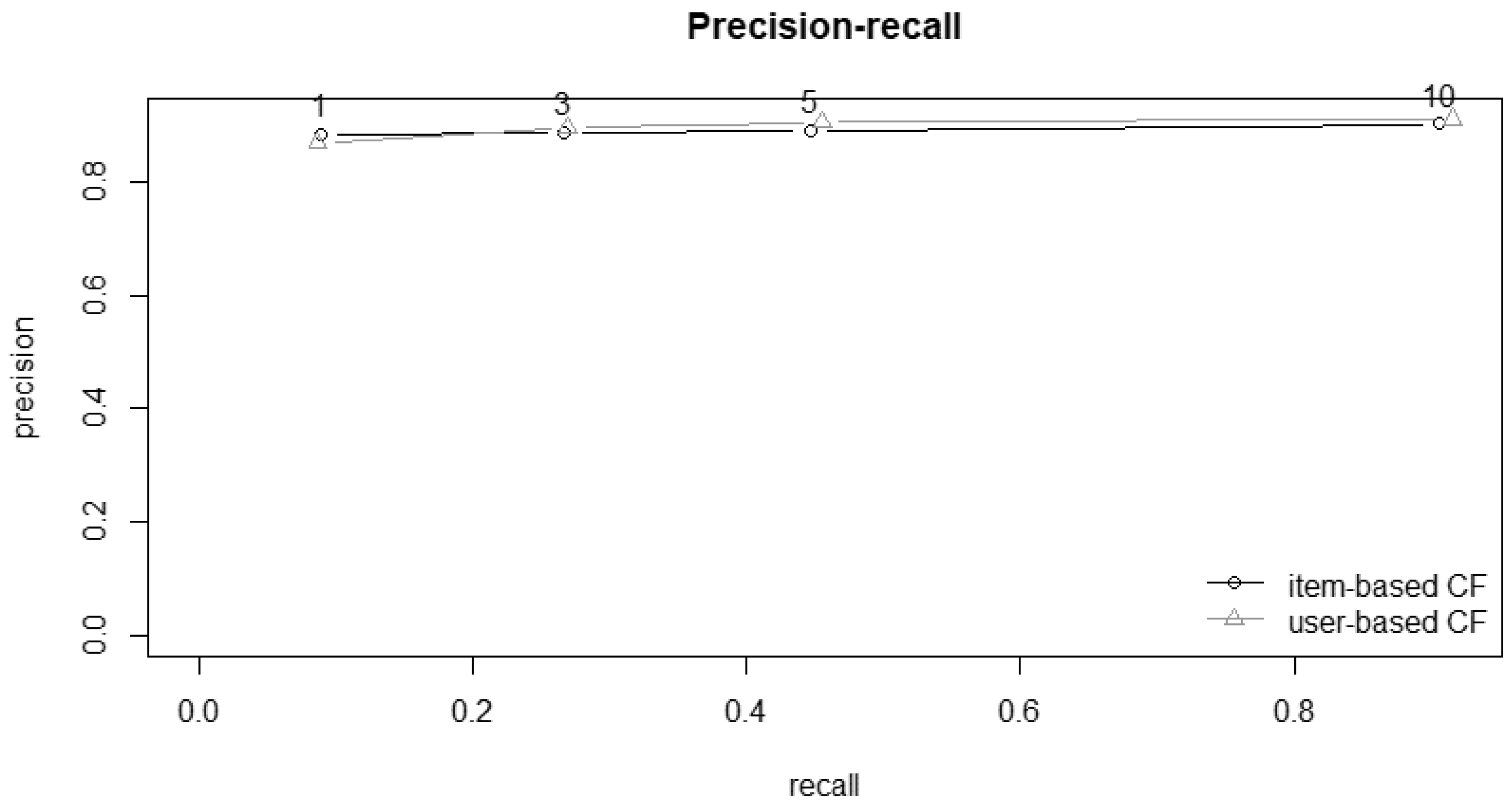
3.6. ROC Curve and Precision–Recall
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desroches, S.; Lapointe, A.; Ratté, S.; Gravel, K.; Légaré, F.; Turcotte, S. Interventions to Enhance Adherence to Dietary Advice for Preventing and Managing Chronic Diseases in Adults. Cochrane Database Syst. Rev. 2013, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Adherence to Long-Term Therapies Evidence for Action; World Health Organization (WHO): Geneva, Switzerland, 2003; ISBN 92 4 154599 2. [Google Scholar]
- Hors-Fraile, S.; Rivera-Romero, O.; Schneider, F.; Fernandez-Luque, L.; Luna-Perejon, F.; Civit-Balcells, A.; de Vries, H. Analyzing Recommender Systems for Health Promotion Using a Multidisciplinary Taxonomy: A Scoping Review. Int. J. Med. Inform. 2018, 114, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Portugal, I.; Alencar, P.; Cowan, D. The Use of Machine Learning Algorithms in Recommender Systems: A Systematic Review. Expert Syst. Appl. 2018, 97, 205–227. [Google Scholar] [CrossRef] [Green Version]
- Fu, M.; Qu, H.; Yi, Z.; Lu, L.; Liu, Y. A Novel Deep Learning-Based Collaborative Filtering Model for Recommendation System. IEEE Trans. Cybern. 2019, 49, 1084–1096. [Google Scholar] [CrossRef]
- Thomas, A.; Sujatha, A. Comparative Study of Recommender Systems. In Proceedings of the 2016 International Conference on Circuit, Power and Computing Technologies (ICCPCT), Nagercoil, India, 18–19 March 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Mustaqeem, A.; Anwar, S.M.; Majid, M. A Modular Cluster Based Collaborative Recommender System for Cardiac Patients. Artif. Intell. Med. 2020, 102, 101761. [Google Scholar] [CrossRef]
- Wiesner, M.; Pfeifer, D. Health Recommender Systems: Concepts, Requirements, Technical Basics and Challenges. Int. J. Environ. Res. Public Health 2014, 11, 2580–2607. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, S.H.; Etminani, K.; Dehghan, H.; Eslami, S.; Hasibian, M.R.; Arki, H.V.; Saberi, M.R.; Aghabagheri, M.; Namayandeh, S.M. Design and Evaluation of a Smart Medication Recommendation System for the Electronic Prescription. Stud. Health Technol. Inf. 2019, 260, 128–135. [Google Scholar] [CrossRef]
- Hors-Fraile, S.; Malwade, S.; Spachos, D.; Fernandez-Luque, L.; Su, C.; Jeng, W.; Syed-Abdul, S.; Bamidis, P.; Li, Y.-C. A Recommender System to Quit Smoking with Mobile Motivational Messages: Study Protocol for a Randomized Controlled Trial. Trials 2018, 19, 618. [Google Scholar] [CrossRef]
- Cheung, K.; Ling, W.; Karr, C.J.; Weingardt, K.; Schueller, S.M.; Mohr, D.C. Evaluation of a Recommender App for Apps for the Treatment of Depression and Anxiety: An Analysis of Longitudinal User Engagement. J. Am. Med. Inform. Assoc. 2018, 25, 955–962. [Google Scholar] [CrossRef]
- Nouh, R.M.; Lee, H.; Lee, W.-J.; Lee, J.-D. A Smart Recommender Based on Hybrid Learning Methods for Personal Well-Being Services. Sensors 2019, 19, 431. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Karvela, M.; Sohbati, M.; Shinawatra, T.; Toumazou, C. PERSON—Personalized Expert Recommendation System for Optimized Nutrition. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 151–160. [Google Scholar] [CrossRef]
- Lee, C.-S.; Wang, M.-H.; Acampora, G.; Hsu, C.-Y.; Hagras, H. Diet Assessment Based on Type-2 Fuzzy Ontology and Fuzzy Markup Language. Int. J. Intell. Syst. 2010, 25, 1187–1216. [Google Scholar] [CrossRef]
- Oh, Y.; Choi, A.; Woo, W. U-BabSang: A Context-Aware Food Recommendation System. J. Supercomput. 2010, 54, 61–81. [Google Scholar] [CrossRef]
- Lovegrove, J.A.; Gitau, R. Personalized Nutrition for the Prevention of Cardiovascular Disease: A Future Perspective. J. Hum. Nutr. Diet. 2008, 21, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Ge, M.; Ricci, F.; Massimo, D. Health-Aware Food Recommender System. In Proceedings of the 9th ACM Conference on Recommender Systems, Vienna, Austria, 16–20 September 2015; pp. 333–334. [Google Scholar] [CrossRef]
- Traill, W.B.; Chambers, S.A.; Butler, L. Attitudinal and Demographic Determinants of Diet Quality and Implications for Policy Targeting. J. Hum. Nutr. Diet. 2012, 25, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Aquino, E.M.L.; Barreto, S.M.; Bensenor, I.M.; Carvalho, M.S.; Chor, D.; Duncan, B.B.; Lotufo, P.A.; Mill, J.G.; Molina, M.D.C.; Mota, E.L.A.; et al. Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Objectives and Design. Am. J. Epidemiol. 2012, 175, 315–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bensenor, I.M.; Griep, R.H.; Pinto, K.A.; de Faria, C.P.; Felisbino-Mendes, M.; Caetano, E.I.; Albuquerque, L.d.S.; Schmidt, M.I. Routines of Organization of Clinical Tests and Interviews in the ELSA-Brasil Investigation Center. Rev Saúde Pública 2013, 47, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Willet, W. Correction for the Effects of Measurement Error. In Nutritional Epidemiology; Willet, W., Ed.; Oxford University Press: New York, NY, USA, 1998; pp. 74–147. ISBN 13 978019512297. [Google Scholar]
- Molina, M.D.C.B.; Faria, C.P.D.; Cardoso, L.D.O.; Drehmer, M.; Velasquez-Meléndez, J.G.; Gomes, A.L.C.; Melere, C.; Diniz, M.D.F.H.S.; Sichieri, R.; Benseñor, I.J.M. Diet Assessment in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Development of a Food Frequency Questionnaire. Rev. De Nutr. 2013, 26, 167–176. [Google Scholar] [CrossRef]
- Molina, M.D.C.B.; Benseñor, I.M.; Cardoso, L.D.O.; Velasquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S.; De Faria, C.P.; Melere, C.; Manato, L.; Gomes, A.L.C.; et al. Reprodutibilidade e Validade Relativa Do Questionário de Frequência Alimentar Do ELSA-Brasil. Cad. De Saúde Pública 2013, 29, 379–389. [Google Scholar] [CrossRef]
- MS. Ministério Da Saúde. Ministério Da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia Alimentar Para a População Brasileira; Ministério da Saúde: Brasília, Brazil, 2014; pp. 1–156.
- Zenun Franco, R. Online Recommender System for Personalized Nutrition Advice. In Proceedings of the Eleventh ACM Conference on Recommender Systems, Como, Italy, 27–31 August 2017; pp. 411–415. [Google Scholar] [CrossRef] [Green Version]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical Review: Vegetables and Fruit in the Prevention of Chronic Diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [Green Version]
- Reddy, K.S.; Katan, M.B. Diet, Nutrition and the Prevention of Hypertension and Cardiovascular Diseases. Public Health Nutr. 2004, 7, 167–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahsler, M. Recommenderlab: A Framework for Developing and Testing Recommendation Algorithms; R Package Version 0.2-2; Southern Methodist University: Dallas, TX, USA, 2017; Available online: http://lyle.smu.edu/IDA/recommenderlab/ (accessed on 8 October 2022).
- da Silva, E.Q.; Camilo-Junior, C.G.; Pascoal, L.M.L.; Rosa, T.C. An Evolutionary Approach for Combining Results of Recommender Systems Techniques Based on Collaborative Filtering. Expert Syst. Appl. 2016, 53, 204–218. [Google Scholar] [CrossRef]
- Cheung, K.L.; Durusu, D.; Sui, X.; de Vries, H. How Recommender Systems Could Support and Enhance Computer-Tailored Digital Health Programs: A Scoping Review. Digit. Health 2019, 5, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Norouzi, S.; Ghalibaf, A.K.; Sistani, S.; Banazadeh, V.; Keykhaei, F.; Zareishargh, P.; Amiri, F.; Nematy, M.; Etminani, K. A Mobile Application for Managing Diabetic Patients’ Nutrition: A Food Recommender System. Arch. Iran. Med. 2018, 21, 466–472. [Google Scholar]
- Han, J.; Kamber, M.; Pei, J. Data Mining: Concepts and Techniques, 3rd ed.; Morgan Kaufmann: Burlington, MA, USA, 2011; ISBN 9780123814791. [Google Scholar]
- Celis-Morales, C.; Livingstone, K.M.; Marsaux, C.F.M.; Macready, A.L.; Fallaize, R.; O’Donovan, C.B.; Woolhead, C.; Forster, H.; Walsh, M.C.; Navas-Carretero, S.; et al. Effect of Personalized Nutrition on Health-Related Behaviour Change: Evidence from the Food4me European Randomized Controlled Trial. Int. J. Epidemiol. 2017, 46, 578–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helander, E.; Kaipainen, K.; Korhonen, I.; Wansink, B. Factors Related to Sustained Use of a Free Mobile App for Dietary Self-Monitoring With Photography and Peer Feedback: Retrospective Cohort Study. J. Med. Internet Res. 2014, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Rokach, L.; Shapira, B.; Kantor, P.B. (Eds.) Recommender Systems Handbook; Springer: Boston, MA, USA, 2011; ISBN 978-0-387-85819-7. [Google Scholar]
- Norouzi, S.; Nematy, M.; Zabolinezhad, H.; Sistani, S.; Etminani, K. Food Recommender Systems for Diabetic Patients: A Narrative Review. Rev. Clin. Med. 2017, 4, 128–130. [Google Scholar] [CrossRef]
- Abhari, S.; Safdari, R.; Azadbakht, L.; Lankarani, K.B.; Kalhori, S.R.N.; Honarvar, B.; Abhari, K.; Ayyoubzadeh, S.M.; Karbasi, Z.; Zakerabasali, S.; et al. A Systematic Review of Nutrition Recommendation Systems: With Focus on Technical Aspects. J. Biomed. Phys. Eng. 2019, 9, 591–602. [Google Scholar] [CrossRef]
- Hill, J.O. Can a Small-Changes Approach Help Address the Obesity Epidemic? A Report of the Joint Task Force of the American Society for Nutrition, Institute of Food Technologists, and International Food Information Council. Am. J. Clin. Nutr. 2009, 89, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.T.; Reidlinger, D.P.; Hoffmann, T.C.; Campbell, K.L. Telehealth Methods to Deliver Dietary Interventions in Adults with Chronic Disease: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2016, 104, 1693–1702. [Google Scholar] [CrossRef] [Green Version]
- Kelders, S.M.; Bohlmeijer, E.T.; Pots, W.T.M.; Gemert-Pijnen, J.E.W.C. Van Comparing Human and Automated Support for Depression: Fractional Factorial Randomized Controlled Trial. Behav. Res. Ther. 2015, 72, 72–80. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | General | Train | Test | p Value 9 | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Study population | 12,667 | 100.0 | 8866 | 100 | 3801 | 100 | |
| Sex | |||||||
| Male | 5217 | 41.2 | 3665 | 41.3 | 1552 | 40.8 | |
| Female | 7450 | 58.8 | 5201 | 58.7 | 2249 | 59.2 | 0.596 |
| Age (years) 1 | 52 | 45–59 | 52 | 45–59 | 52 | 45–59 | 0.850 |
| Education level | |||||||
| Elementary (or less) | 1423 | 11.2 | 1022 | 11.5 | 401 | 10.5 | |
| High school | 4072 | 32.2 | 2829 | 31.9 | 1243 | 32.7 | |
| College | 7172 | 56.6 | 5015 | 56.6 | 2157 | 56.8 | 0.247 |
| Retirement | |||||||
| No | 10,046 | 79.3 | 7012 | 79.1 | 3034 | 79.8 | |
| Yes | 2621 | 20.7 | 1854 | 20.9 | 767 | 20.2 | 0.351 |
| Race/ethnicity | |||||||
| White | 6994 | 55.2 | 4887 | 55.1 | 2107 | 55.4 | |
| Mixed | 3379 | 26.7 | 2373 | 26.8 | 1006 | 26.5 | |
| Black | 1831 | 14.4 | 1281 | 14.4 | 550 | 14.5 | |
| Others 2 | 463 | 3.7 | 325 | 3.7 | 138 | 3.6 | 0.986 |
| Marital status | |||||||
| Not single | 8181 | 64.6 | 5700 | 64.3 | 2481 | 65.3 | |
| Single | 4486 | 35.4 | 3166 | 35.7 | 1320 | 34.7 | 0.290 |
| Per capita income 3 | |||||||
| 1° tercile | 4225 | 33.4 | 2994 | 33.8 | 1231 | 32.4 | |
| 2° tercile | 4492 | 35.5 | 3093 | 34.9 | 1399 | 36.8 | |
| 3° tercile | 3950 | 31.2 | 2779 | 31.3 | 1171 | 30.8 | 0.103 |
| Living alone | |||||||
| No | 11,043 | 87.2 | 1157 | 13.1 | 467 | 12.3 | |
| Yes | 1624 | 12.8 | 7709 | 86.9 | 3334 | 87.7 | 0.239 |
| Smoking habit | |||||||
| Never | 7306 | 57.7 | 5137 | 57.9 | 2169 | 57.0 | |
| Ex-smoker | 3780 | 29.8 | 2643 | 29.8 | 1137 | 29.9 | |
| Current smoker | 1581 | 12.5 | 1086 | 12.3 | 495 | 13.0 | 0.440 |
| Physical activity 4 | |||||||
| Sedentary | 5798 | 45.8 | 4022 | 45.4 | 1776 | 46.7 | |
| Insufficiently active | 3354 | 26.5 | 2371 | 26.7 | 983 | 25.8 | |
| Active | 3515 | 27.7 | 2473 | 27.8 | 1042 | 27.4 | 0.354 |
| Health self-assessment | |||||||
| Good | 10,266 | 81.1 | 7191 | 81.1 | 3075 | 80.9 | |
| Regular | 2167 | 17.1 | 1510 | 17.0 | 657 | 17.3 | |
| Bad | 234 | 1.8 | 165 | 1.9 | 69 | 1.8 | 0.930 |
| BMI (kg/m2) 1 | 26.3 | 23.7–29.5 | 26.3 | 23.7–29.6 | 26.2 | 23.7–29.4 | 0.939 |
| Waist-to-hip ratio 1 | 0.9 | 0.8-1.0 | 0.9 | 0.8–1.0 | 0.9 | 0.8–1.0 | 0.473 |
| Dyslipidemia 5 | |||||||
| No | 5237 | 41.3 | 3666 | 41.4 | 1571 | 41.3 | |
| Yes | 7430 | 58.7 | 5200 | 58.6 | 2230 | 58.7 | 0.985 |
| Hypertension 6 | |||||||
| No | 8159 | 64.4 | 5708 | 64.4 | 2451 | 64.5 | |
| Yes | 4508 | 35.6 | 3158 | 35.6 | 1350 | 35.5 | 0.912 |
| Diabetes 7 | |||||||
| No | 10,634 | 83.9 | 7450 | 84.0 | 3184 | 83.8 | |
| Yes | 2033 | 16.1 | 1416 | 16.0 | 617 | 16.2 | 0.713 |
| Cardiovascular disease 8 | |||||||
| No | 12,188 | 96.2 | 8529 | 96.2 | 3659 | 96.2 | |
| Yes | 479 | 3.8 | 337 | 3.8 | 142 | 3.7 | 0.860 |
| RMSE 1 | MSE 2 | MAE 3 | |
|---|---|---|---|
| User-Based CF | 1.49 | 2.21 | 1.26 |
| Item-Based CF | 1.67 | 2.78 | 1.40 |
| User-Based Collaborative Filtering (UBCF) | ||||||||
| K | TP | FP | FN | TN | Precision | Recall | TPR | FRP |
| 1 | 0.88 | 0.12 | 9.08 | 0.92 | 0.88 | 0.09 | 0.09 | 0.11 |
| 3 | 2.70 | 0.30 | 7.25 | 0.75 | 0.90 | 0.27 | 0.27 | 0.27 |
| 5 | 4.54 | 0.46 | 5.41 | 0.59 | 0.91 | 0.46 | 0.46 | 0.43 |
| 10 | 9.11 | 0.89 | 0.85 | 0.15 | 0.91 | 0.91 | 0.91 | 0.84 |
| Item-Based Collaborative Filtering (IBCF) | ||||||||
| K | TP | FP | FN | TN | Precision | Recall | TPR | FRP |
| 1 | 0.88 | 0.12 | 9.08 | 0.92 | 0.88 | 0.09 | 0.09 | 0.12 |
| 3 | 2.66 | 0.34 | 7.30 | 0.70 | 0.89 | 0.27 | 0.27 | 0.33 |
| 5 | 4.45 | 0.55 | 5.51 | 0.49 | 0.89 | 0.45 | 0.45 | 0.53 |
| 10 | 9.03 | 0.97 | 0.93 | 0.07 | 0.90 | 0.91 | 0.91 | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, V.C.; Gorgulho, B.; Marchioni, D.M.; Alvim, S.M.; Giatti, L.; de Araujo, T.A.; Alonso, A.C.; Santos, I.d.S.; Lotufo, P.A.; Benseñor, I.M. Recommender System Based on Collaborative Filtering for Personalized Dietary Advice: A Cross-Sectional Analysis of the ELSA-Brasil Study. Int. J. Environ. Res. Public Health 2022, 19, 14934. https://doi.org/10.3390/ijerph192214934
Silva VC, Gorgulho B, Marchioni DM, Alvim SM, Giatti L, de Araujo TA, Alonso AC, Santos IdS, Lotufo PA, Benseñor IM. Recommender System Based on Collaborative Filtering for Personalized Dietary Advice: A Cross-Sectional Analysis of the ELSA-Brasil Study. International Journal of Environmental Research and Public Health. 2022; 19(22):14934. https://doi.org/10.3390/ijerph192214934
Chicago/Turabian StyleSilva, Vanderlei Carneiro, Bartira Gorgulho, Dirce Maria Marchioni, Sheila Maria Alvim, Luana Giatti, Tânia Aparecida de Araujo, Angelica Castilho Alonso, Itamar de Souza Santos, Paulo Andrade Lotufo, and Isabela Martins Benseñor. 2022. "Recommender System Based on Collaborative Filtering for Personalized Dietary Advice: A Cross-Sectional Analysis of the ELSA-Brasil Study" International Journal of Environmental Research and Public Health 19, no. 22: 14934. https://doi.org/10.3390/ijerph192214934