
Diets, Dietary Patterns, Single Foods and Pancreatic Cancer Risk: An Umbrella Review of Meta-Analyses
 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Inclusion/Exclusion Criteria
2.3. Selection Process and Data Extraction
2.4. Quality Assessment
2.5. Strengths of Evidence Assessment and Data Analysis
3. Results
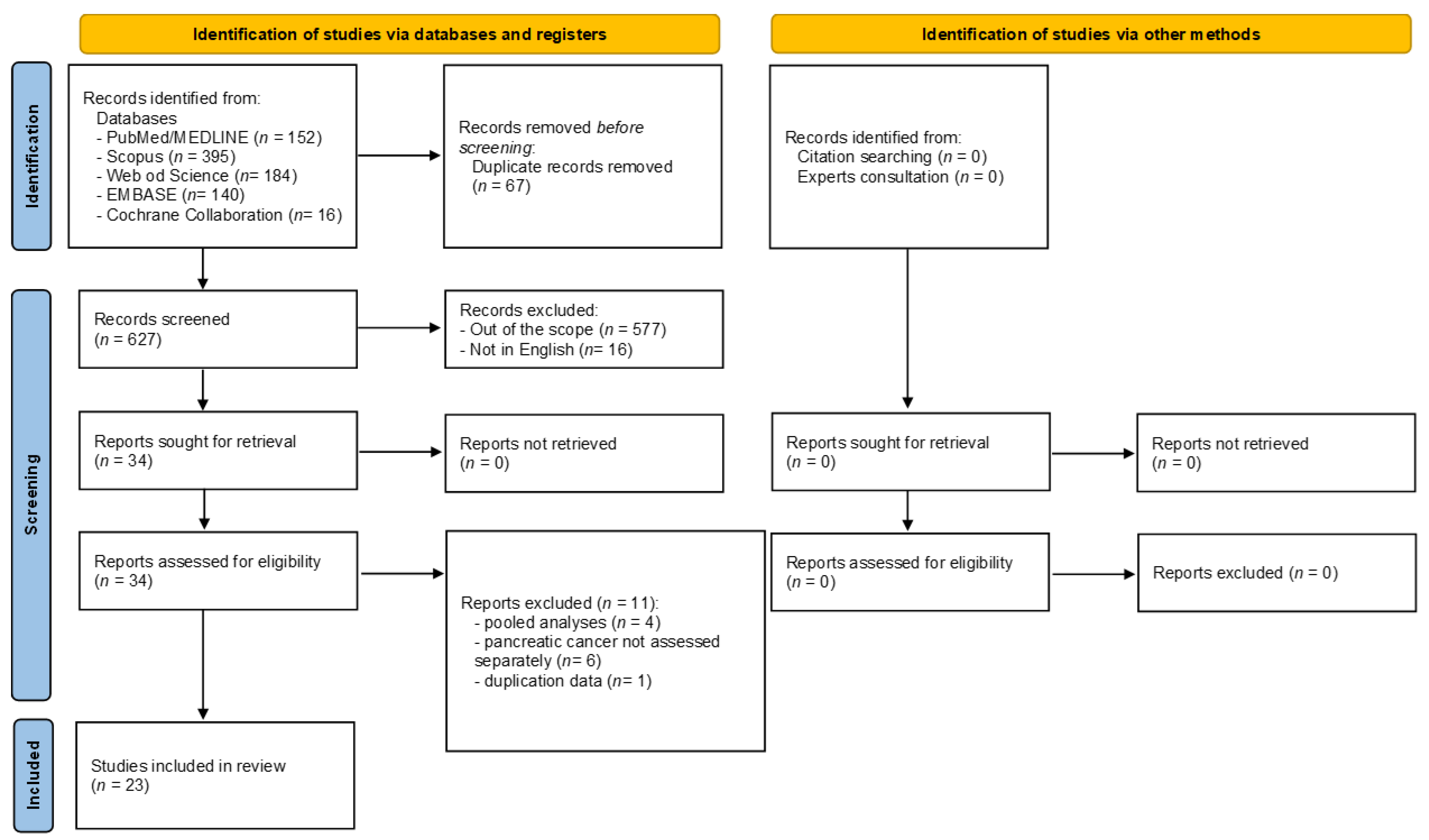
3.1. Search Results
3.2. Characteristics and Methodological Quality of the Meta-Analyses Included
3.3. Strength of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Sanagapalli, S.; Stoita, A. Challenges in diagnosis of pancreatic cancer. World J. Gastroenterol. 2018, 24, 2047–2060. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Childs, E.J.; Mocci, E.; Bracci, P.; Gallinger, S.; Li, D.; Neale, R.E.; Olson, S.H.; Scelo, G.; Bamlet, W.R.; et al. Analysis of Heritability and Genetic Architecture of Pancreatic Cancer: A PanC4 Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1238–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannala, R.; Basu, A.; Petersen, G.M.; Chari, S.T. New-onset diabetes: A potential clue to the early diagnosis of pancreatic cancer. Lancet Oncol. 2009, 10, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Smyrk, T.C.; Levy, M.J.; Topazian, M.A.; Chari, S.T. Fasting Blood Glucose Levels Provide Estimate of Duration and Progression of Pancreatic Cancer Before Diagnosis. Gastroenterology 2018, 155, 490–500.e492. [Google Scholar] [CrossRef]
- Kirkegard, J.; Mortensen, F.V.; Cronin-Fenton, D. Chronic Pancreatitis and Pancreatic Cancer Risk: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2017, 112, 1366–1372. [Google Scholar] [CrossRef] [Green Version]
- Momi, N.; Kaur, S.; Ponnusamy, M.P.; Kumar, S.; Wittel, U.A.; Batra, S.K. Interplay between smoking-induced genotoxicity and altered signaling in pancreatic carcinogenesis. Carcinogenesis 2012, 33, 1617–1628. [Google Scholar] [CrossRef]
- Bracci, P.M. Obesity and pancreatic cancer: Overview of epidemiologic evidence and biologic mechanisms. Mol. Carcinog. 2012, 51, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Pothuraju, R.; Rachagani, S.; Junker, W.M.; Chaudhary, S.; Saraswathi, V.; Kaur, S.; Batra, S.K. Pancreatic cancer associated with obesity and diabetes: An alternative approach for its targeting. J. Exp. Clin. Cancer Res. 2018, 37, 319. [Google Scholar] [CrossRef] [Green Version]
- Nucci, D.; Santangelo, O.E.; Provenzano, S.; Fatigoni, C.; Nardi, M.; Ferrara, P.; Gianfredi, V. Dietary fiber intake and risk of pancreatic cancer: Systematic review and meta-analysis of observational studies. Int. J. Environ. Res. Public Health 2021, 18, 11556. [Google Scholar] [CrossRef]
- Zheng, J.; Guinter, M.A.; Merchant, A.T.; Wirth, M.D.; Zhang, J.; Stolzenberg-Solomon, R.Z.; Steck, S.E. Dietary patterns and risk of pancreatic cancer: A systematic review. Nutr. Rev. 2017, 75, 883–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, Q.Q.; Lin, Y.W.; Chen, H.; Qin, J.; Zheng, X.Y.; Xu, X.; Xie, L.P. Dietary fiber intake is inversely associated with risk of pancreatic cancer: A meta-analysis. Asia Pac. J. Clin. Nutr. 2017, 26, 89–96. [Google Scholar] [CrossRef]
- Mossine, V.V.; Mawhinney, T.P.; Giovannucci, E.L. Dried Fruit Intake and Cancer: A Systematic Review of Observational Studies. Adv. Nutr. 2020, 11, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0.; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.J.; Wong, M.C.S. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.1 (Updated September 2020); Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Accardi, G.; Shivappa, N.; Di Maso, M.; Hébert, J.R.; Fratino, L.; Montella, M.; La Vecchia, C.; Caruso, C.; Serraino, D.; Libra, M.; et al. Dietary inflammatory index and cancer risk in the elderly: A pooled-analysis of Italian case-control studies. Nutrition 2019, 63–64, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Wang, M.; Li, R.; Albanes, D.; Anderson, K.E.; Bernstein, L.; van den Brandt, P.A.; English, D.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. Dairy products and pancreatic cancer risk: A pooled analysis of 14 cohort studies. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Koushik, A.; Spiegelman, D.; Albanes, D.; Anderson, K.E.; Bernstein, L.; Van Den Brandt, P.A.; Bergkvist, L.; English, D.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. Intake of fruits and vegetables and risk of pancreatic cancer in a pooled analysis of 14 Cohort studies. Am. J. Epidemiol. 2012, 176, 373–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaud, D.S.; Skinner, H.G.; Wu, K.; Hu, F.; Giovannucci, E.; Willett, W.C.; Colditz, G.A.; Fuchs, C.S. Dietary patterns and pancreatic cancer risk in men and women. J. Natl. Cancer Inst. 2005, 97, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Turati, F.; Rossi, M.; Pelucchi, C.; Levi, F.; La Vecchia, C. Fruit and vegetables and cancer risk: A review of southern European studies. Br. J. Nutr. 2015, 113, S102–S110. [Google Scholar] [CrossRef] [PubMed]
- Elands, R.J.J.; Simons, C.C.J.M.; Van Dongen, M.; Schouten, L.J.; Verhage, B.J.; Van Den Brandt, P.A.; Weijenberg, M.P. A systematic literature review and meta-regression analysis on early-life energy restriction and cancer risk in humans. PLoS ONE 2016, 11, e0158003. [Google Scholar] [CrossRef] [Green Version]
- Fabiani, R.; Minelli, L.; Rosignoli, P. Apple intake and cancer risk: A systematic review and meta-analysis of observational studies. Public Health Nutr. 2016, 19, 2603–2617. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Galvano, F.; Boffetta, P. Health risk factors associated with meat, fruit and vegetable consumption in cohort studies: A comprehensive meta-analysis. PLoS ONE 2017, 12, e0183787. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Kosti, R.I.; Haidopoulos, D.; Dimopoulos, M.; Panagiotakos, D.B. Olive oil intake is inversely related to cancer prevalence: A systematic review and a meta-analysis of 13800 patients and 23340 controls in 19 observational studies. Lipids Health Dis. 2011, 10, 127. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Wang, Z.; Zhu, J.; Murad, A.L.; Prokop, L.J.; Murad, M.H. Nut consumption and risk of cancer and type 2 diabetes: A systematic review and meta-analysis. Nutr. Rev. 2015, 73, 409–425. [Google Scholar] [CrossRef]
- Zahedi, H.; Djalalinia, S.; Asayesh, H.; Mansourian, M.; Abdar, Z.E.; Gorabi, A.M.; Ansari, H.; Noroozi, M.; Qorbani, M. A higher dietary inflammatory index score is associated with a higher risk of incidence and mortality of cancer: A comprehensive systematic review and meta-analysis. Int. J. Prev. Med. 2020, 11, 1358–1367. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, S.; Shab-Bidar, S.; Mohtavinejad, N.; Djafarian, K. A posteriori dietary patterns and risk of pancreatic and renal cancers A systematic review and meta-analysis. Nutr. Food Sci. 2017, 47, 839–868. [Google Scholar] [CrossRef]
- Bae, J.M.; Lee, E.J.; Guyatt, G. Citrus fruit intake and pancreatic cancer risk: A quantitative systematic review. Pancreas 2009, 38, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Darooghegi Mofrad, M.; Mozaffari, H.; Askari, M.R.; Amini, M.R.; Jafari, A.; Surkan, P.J.; Azadbakht, L. Potato Consumption and Risk of Site-Specific Cancers in Adults: A Systematic Review and Dose-Response Meta-Analysis of Observational Studies. Adv. Nutr. 2021, 12, 1705–1722. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Ma, Y.; Yu, M.; Li, G.; Chen, Y.; Li, X.; Chen, X.; Xie, Y.; Wang, X. Poultry and Fish Intake and Pancreatic Cancer Risk: A Systematic Review and Meta-Analysis. Nutr. Cancer 2022, 74, 55–67. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [Green Version]
- Guo, Z.; Hong, Y.; Cheng, Y. Dietary inflammatory index and pancreatic cancer risk: A systematic review and dose-response meta-analysis. Public Health Nutr. 2021, 24, 6427–6435. [Google Scholar] [CrossRef]
- Han, M.A.; Zeraatkar, D.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Zhang, Y.; Algarni, A.; Leung, G.; Storman, D.; Valli, C.; et al. Reduction of red and processed meat intake and cancer mortality and incidence a systematic review and meta-analysis of cohort studies. Ann. Intern. Med. 2019, 171, 711–720. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.R., Jr.; Marquart, L.; Slavin, J.; Kushi, L.H. Whole-grain intake and cancer: An expanded review and meta-analysis. Nutr. Cancer 1998, 30, 85–96. [Google Scholar] [CrossRef]
- Jayedi, A.; Emadi, A.; Shab-Bidar, S. Dietary Inflammatory Index and Site-Specific Cancer Risk: A Systematic Review and Dose-Response Meta-Analysis. Adv. Nutr. 2018, 9, 388–403. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Wang, M.; Jiang, H.Z.; Chen, G.C.; Hua, Y.F. Meta-analysis of fish consumption and risk of pancreatic cancer in 13 prospective studies with 1.8 million participants. PLoS ONE 2019, 14, e0222139. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Wolk, A. Red and processed meat consumption and risk of pancreatic cancer: Meta-analysis of prospective studies. Br. J. Cancer 2012, 106, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Zheng, H.; Bi, J.; Wang, X.; Jiang, T.; Gao, X.; Tian, F.; Xu, M.; Wu, C.; Zhang, L.; et al. Whole Grain Intake Reduces Pancreatic Cancer Risk: A Meta-Analysis of Observational Studies. Medicine 2016, 95, e2747. [Google Scholar] [CrossRef] [PubMed]
- Li, L.Y.; Luo, Y.; Lu, M.D.; Xu, X.W.; Lin, H.D.; Zheng, Z.Q. Cruciferous vegetable consumption and the risk of pancreatic cancer: A meta-analysis. World J. Surg. Oncol. 2015, 13, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, P.Y.; Shu, L.; Shen, S.S.; Chen, X.J.; Zhang, X.Y. Dietary patterns and pancreatic cancer risk: A meta-analysis. Nutrients 2017, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Naghshi, S.; Sadeghian, M.; Nasiri, M.; Mobarak, S.; Asadi, M.; Sadeghi, O. Association of Total Nut, Tree Nut, Peanut, and Peanut Butter Consumption with Cancer Incidence and Mortality: A Comprehensive Systematic Review and Dose-Response Meta-Analysis of Observational Studies. Adv. Nutr. 2021, 12, 793–808. [Google Scholar] [CrossRef]
- Paluszkiewicz, P.; Smolińska, K.; Dębińska, I.; Turski, W.A. Main dietary compounds and pancreatic cancer risk. The quantitative analysis of case-control and cohort studies. Cancer Epidemiol. 2012, 36, 60–67. [Google Scholar] [CrossRef]
- Qin, B.; Xun, P.; He, K. Fish or long-chain (n-3) PUFA intake is not associated with pancreatic cancer risk in a meta-analysis and systematic review. J. Nutr. 2012, 142, 1067–1073. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef]
- Wu, Q.J.; Wu, L.; Zheng, L.Q.; Xu, X.; Ji, C.; Gong, T.T. Consumption of fruit and vegetables reduces risk of pancreatic cancer: Evidence from epidemiological studies. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. (ECP) 2016, 25, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.F.; Zou, J.; Dong, J. Fish consumption and risk of gastrointestinal cancers: A meta-analysis of cohort studies. World J. Gastroenterol. 2014, 20, 15398–15412. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Dai, C.; Zhou, L.; Li, Y.; Liu, K.; Deng, Y.J.; Li, N.; Zheng, Y.; Hao, Q.; Yang, S.; et al. Meta-analysis of the association between nut consumption and the risks of cancer incidence and cancer-specific mortality. Aging 2020, 12, 10772–10794. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhan, J.; Wang, Y.; Wang, D. The Relationship Between Plant-Based Diet and Risk of Digestive System Cancers: A Meta-Analysis Based on 3,059,009 Subjects. Front. Public Health 2022, 10, 892153. [Google Scholar] [CrossRef]
- Zhao, Z.; Yin, Z.; Pu, Z.; Zhao, Q. Association Between Consumption of Red and Processed Meat and Pancreatic Cancer Risk: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2017, 15, 486–493.e410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, H.; Mahmud, S.M. Different study designs in the epidemiology of cancer: Case-control vs. cohort studies. Methods Mol. Biol. 2009, 471, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M. Evaluating epidemiologic evidence of the effects of food and nutrient exposures. Am. J. Clin. Nutr. 1999, 69, 1339S–1344S. [Google Scholar] [CrossRef] [Green Version]
- Molina-Montes, E.; Salamanca-Fernandez, E.; Garcia-Villanova, B.; Sanchez, M.J. The Impact of Plant-Based Dietary Patterns on Cancer-Related Outcomes: A Rapid Review and Meta-Analysis. Nutrients 2020, 12, 2010. [Google Scholar] [CrossRef]
- Hever, J.; Cronise, R.J. Plant-based nutrition for healthcare professionals: Implementing diet as a primary modality in the prevention and treatment of chronic disease. J. Geriatr. Cardiol. 2017, 14, 355–368. [Google Scholar] [CrossRef]
- Chan, J.M.; Wang, F.; Holly, E.A. Vegetable and fruit intake and pancreatic cancer in a population-based case-control study in the San Francisco bay area. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2093–2097. [Google Scholar] [CrossRef]
- Chikara, S.; Nagaprashantha, L.D.; Singhal, J.; Horne, D.; Awasthi, S.; Singhal, S.S. Oxidative stress and dietary phytochemicals: Role in cancer chemoprevention and treatment. Cancer Lett. 2018, 413, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Vannini, S.; Moretti, M.; Villarini, M.; Bragazzi, N.L.; Izzotti, A.; Nucci, D. Sulforaphane and Epigallocatechin Gallate Restore Estrogen Receptor Expression by Modulating Epigenetic Events in the Breast Cancer Cell Line MDA-MB-231: A Systematic Review and Meta-Analysis. J. Nutr. Nutr. 2017, 10, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Stefanska, B.; Karlic, H.; Varga, F.; Fabianowska-Majewska, K.; Haslberger, A. Epigenetic mechanisms in anti-cancer actions of bioactive food components--the implications in cancer prevention. Br. J. Pharmacol. 2012, 167, 279–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramaniam, S.; Selvaduray, K.R.; Radhakrishnan, A.K. Bioactive Compounds: Natural Defense Against Cancer? Biomolecules 2019, 9, 758. [Google Scholar] [CrossRef] [Green Version]
- Fowler, M.E.; Akinyemiju, T.F. Meta-analysis of the association between dietary inflammatory index (DII) and cancer outcomes. Int. J. Cancer 2017, 141, 2215–2227. [Google Scholar] [CrossRef] [Green Version]
- Marx, W.; Veronese, N.; Kelly, J.T.; Smith, L.; Hockey, M.; Collins, S.; Trakman, G.L.; Hoare, E.; Teasdale, S.B.; Wade, A.; et al. The Dietary Inflammatory Index and Human Health: An Umbrella Review of Meta-Analyses of Observational Studies. Adv. Nutr. 2021, 12, 1681–1690. [Google Scholar] [CrossRef]
- Shadhu, K.; Xi, C. Inflammation and pancreatic cancer: An updated review. Saudi J. Gastroenterol. 2019, 25, 3–13. [Google Scholar] [CrossRef]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B. Potato and french fry consumption and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2006, 83, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.S.; Song, M.; Nishihara, R.; Drew, D.A.; Wu, K.; Qian, Z.R.; Fung, T.T.; Hamada, T.; Masugi, Y.; da Silva, A.; et al. Dietary Patterns and Risk of Colorectal Cancer: Analysis by Tumor Location and Molecular Subtypes. Gastroenterology 2017, 152, 1944–1953.e1941. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Xia, J.; Li, L.; Ke, Y.; Cheng, J.; Xie, Y.; Chu, W.; Cheung, P.; Kim, J.H.; Colditz, G.A.; et al. Associations between dietary patterns and the risk of breast cancer: A systematic review and meta-analysis of observational studies. Breast Cancer Res. 2019, 21, 16. [Google Scholar] [CrossRef]
- Bosetti, C.; Turati, F.; Dal Pont, A.; Ferraroni, M.; Polesel, J.; Negri, E.; Serraino, D.; Talamini, R.; La Vecchia, C.; Zeegers, M.P. The role of Mediterranean diet on the risk of pancreatic cancer. Br. J. Cancer 2013, 109, 1360–1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tognon, G.; Nilsson, L.M.; Lissner, L.; Johansson, I.; Hallmans, G.; Lindahl, B.; Winkvist, A. The Mediterranean diet score and mortality are inversely associated in adults living in the subarctic region. J. Nutr. 2012, 142, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and incidence of type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ 2010, 341, c4229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatenoud, L.; Tavani, A.; La Vecchia, C.; Jacobs, D.R., Jr.; Negri, E.; Levi, F.; Franceschi, S. Whole grain food intake and cancer risk. Int. J. Cancer 1998, 77, 24–28. [Google Scholar] [CrossRef]
- International Agency Research on Cancer (IARC). Red Meat and Processed Meat. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2018. [Google Scholar]
- Knuppel, A.; Papier, K.; Fensom, G.K.; Appleby, P.N.; Schmidt, J.A.; Tong, T.Y.N.; Travis, R.C.; Key, T.J.; Perez-Cornago, A. Meat intake and cancer risk: Prospective analyses in UK Biobank. Int. J. Epidemiol. 2020, 49, 1540–1552. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V. Dietary glycemic index, glycemic load and cancer: An overview of the literature. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 18–31. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Angelino, D.; Rosi, A.; Dall’Asta, M.; Bresciani, L.; Ferraris, C.; Guglielmetti, M.; Godos, J.; Del Bo, C.; et al. Effects of Popular Diets on Anthropometric and Cardiometabolic Parameters: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 815–833. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Amerio, A.; Signorelli, C.; Odone, A.; Dinu, M. What Can We Expect from an Umbrella Review? Adv. Nutr. 2022, 13, 684–685. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Description |
|---|---|
| Population | Inclusion: adults (≥18 years) Exclusion: children/adolescents and pregnant women (post-partum depression) |
| Intervention | Inclusion: all diets or dietary patterns/dietary interventions, including single food components Exclusion: study assessing the effect of supplements |
| Comparison | No intervention or any diet or dietary patterns/dietary interventions |
| Outcome | Inclusion: pancreatic cancer risk Exclusion: other outcomes or data combined for pancreatic cancer with other gastrointestinal cancers. |
| Study design | Inclusion: systematic reviews with meta-analyses of original studies (both randomized controlled trials and observational studies) Exclusion: meta-analyses not published as peer-reviewed meta-analyses in international scientific journals (book, book chapter, thesis). No full-text papers (abstract, conference paper, letter, commentary, note), systematic review without quantitative analysis, meta-analysis not reporting comprehensive data (e.g., effect size and 95% confidence intervals) |
| Reference | No. of Studies/Study Design | Comparison | ES | Study Population (Age ≥ 18 y) | Quality/Risk of Bias Assessment | No. of Events | Total No. | Summary ES (95% CI) | Fixed p Value | Random p Value | PI (95%) | I2 | Quality of Meta-Analyses ° | Strength of Evidence | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed Effects | Random Effects | ||||||||||||||
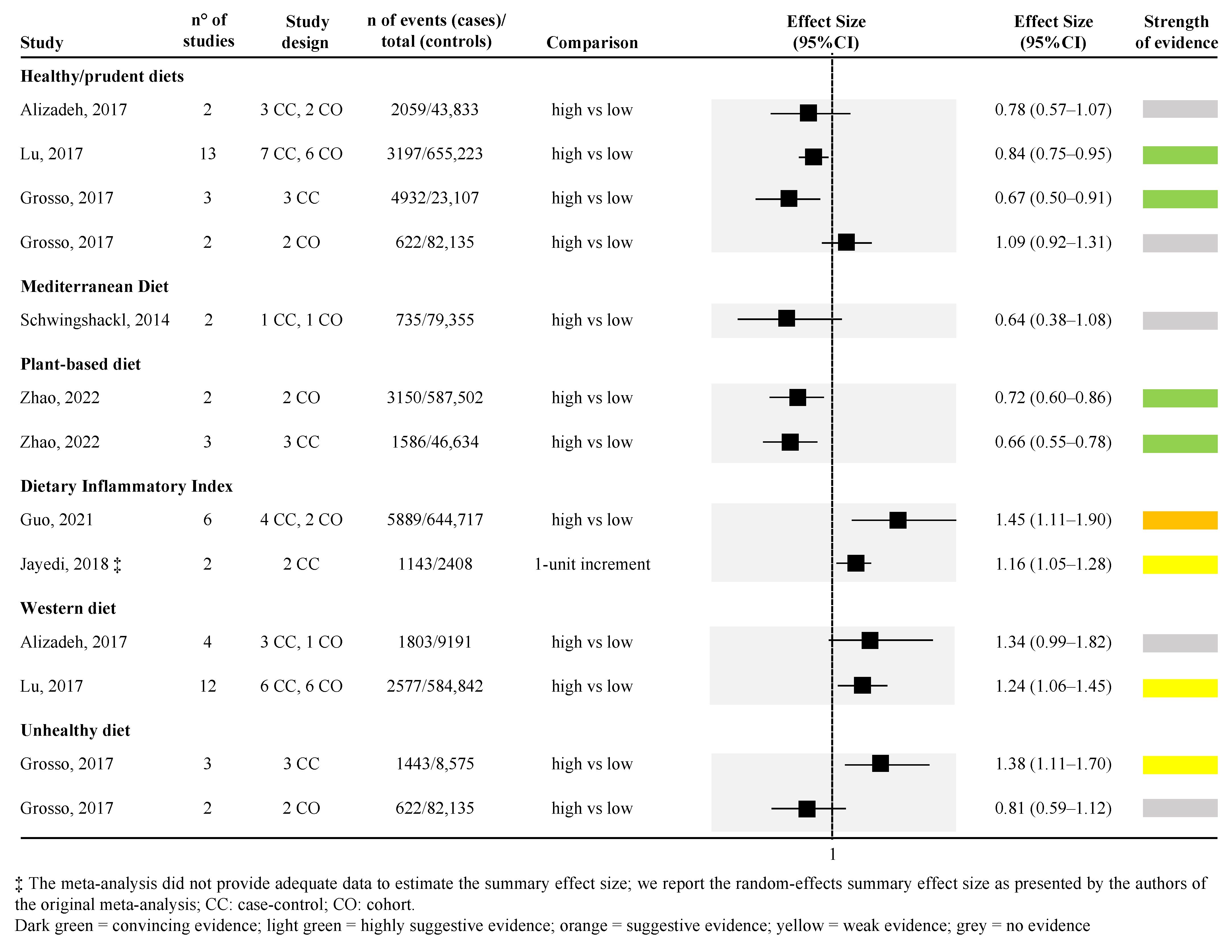
| Healthy */prudent diet | |||||||||||||||
| Alizadeh, 2017 [35] | 5 (3CC, 2CO) | High vs. low | OR | M/F | NOS | 2059 | 43,833 | 0.85 (0.73–0.95) | 0.78 (0.57–1.07) | 0.029 | 0.122 | (0.30–2.04) | 71.68 | Critically low | No evidence |
| Grosso, 2017 [39] | 3CC | High vs. low | RR | M/F | JWHOFAECC | 1443 | 8575 | 0.67 (0.55–0.83) | 0.67 (0.50–0.91) | 0.000 | 0.001 | (0.34–1.33) | 51.73 | Low | Highly suggestive |
| Grosso, 2017 [39] | 2CO | High vs. low | RR | M/F | JWHOFAECC | 622 | 82,135 | 1.09 (0.92–1.29) | 1.09 (0.92–1.31) | 0.300 | 0.322 | (−0.24–0.42) | 11.72 | Low | Highly suggestive |
| Lu, 2017 [48] | 13 (7CC, 6CO) | High vs. low | OR | M/F | NOS | 3197 | 655,223 | 0.84 (0.78–0.90) | 0.84 (0.75–0.95) | 0.000 | 0.004 | (0.61–1.17) | 46.82 | Critically low | No evidence |
| Plant-based diet | |||||||||||||||
| Zhao, 2022 [56] | 2 CO | High vs. low | RR | M/F | ROBINS-I | 3150 | 587,502 | 0.82 (0.75–0.89) | 0.72 (0.60–0.86) | 0.000 | 0.000 | (0.46–1.13) | 54.14 | Low | Highly suggestive |
| Zhao, 2022 [56] | 3 CC | High vs. low | OR | M/F | ROBINS-I | 1586 | 46,634 | 0.67 (0.60–0.76) | 0.66 (0.55–0.78) | 0.000 | 0.000 | (0.40–1.07) | 44.80 | Low | Highly suggestive |
| Dietary Inflammatory Index (DII) | |||||||||||||||
| Guo, 2021 [40] | 6 (4CC, 2CO) | High vs. low | RR | M/F | NOS | 5889 | 644,717 | 1.19 (1.11–1.28) | 1.45 (1.11–1.90) | 0.000 | 0.006 | (0.70–3.00) | 88.8 | Low | Suggestive |
| Jayedi, 2018 [43] | 2CC | 1-unit increment in the DII | RR | M/F | NOS | 1143 | 2408 | N.E. | 1.16 (1.05–1.28) | N.E. | n.s. | N.E. | 61.6 | Moderate | Weak evidence |
| Western diet | |||||||||||||||
| Alizadeh, 2017 [35] | 4 (3CC, 1CO) | High vs. low | OR | M/F | NOS | 1803 | 9191 | 1.39 (1.11–1.73) | 1.34 (0.99–1.82) | 0.004 | 0.060 | (0.66–2.92) | 46.92 | Critically low | No evidence |
| Lu, 2017 [48] | 12 (6CC, 6CO) | High vs. low | OR | M/F | NOS | 2577 | 584,842 | 1.24 (1.14–1.35) | 1.24 (1.06–1.45) | 0.000 | 0.008 | (0.69–2.22) | 69.55 | Critically low | Weak evidence |
| Unhealthy diet * | |||||||||||||||
| Grosso, 2017 [39] | 3CC | High vs. low | RR | M/F | JWHOFAECC | 1443 | 8575 | 1.41 (1.18–1.68) | 1.38 (1.11–1.70) | 0.000 | 0.003 | (0.85–2.24) | 29.12 | Low | Weak evidence |
| Grosso, 2017 [39] | 2CO | High vs. low | RR | M/F | JWHOFAECC | 622 | 82,135 | 0.81 (0.59–1.12) | 0.81 (0.59–1.12) | 0.206 | 0.206 | (0.41–1.61) | 0.00 | Low | No evidence |
| Mediterranean diet (MD) | |||||||||||||||
| Schwingshackl, 2014 [52] | 2 (1CC, 1CO) | High vs. low | RR | M/F | NOS | 735 | 79,355 | 0.76 (0.68–0.86) | 0.64 (0.38–1.08) | 0.000 | 0.095 | (0.00–195.42) | 89.38 | Moderate | No evidence |
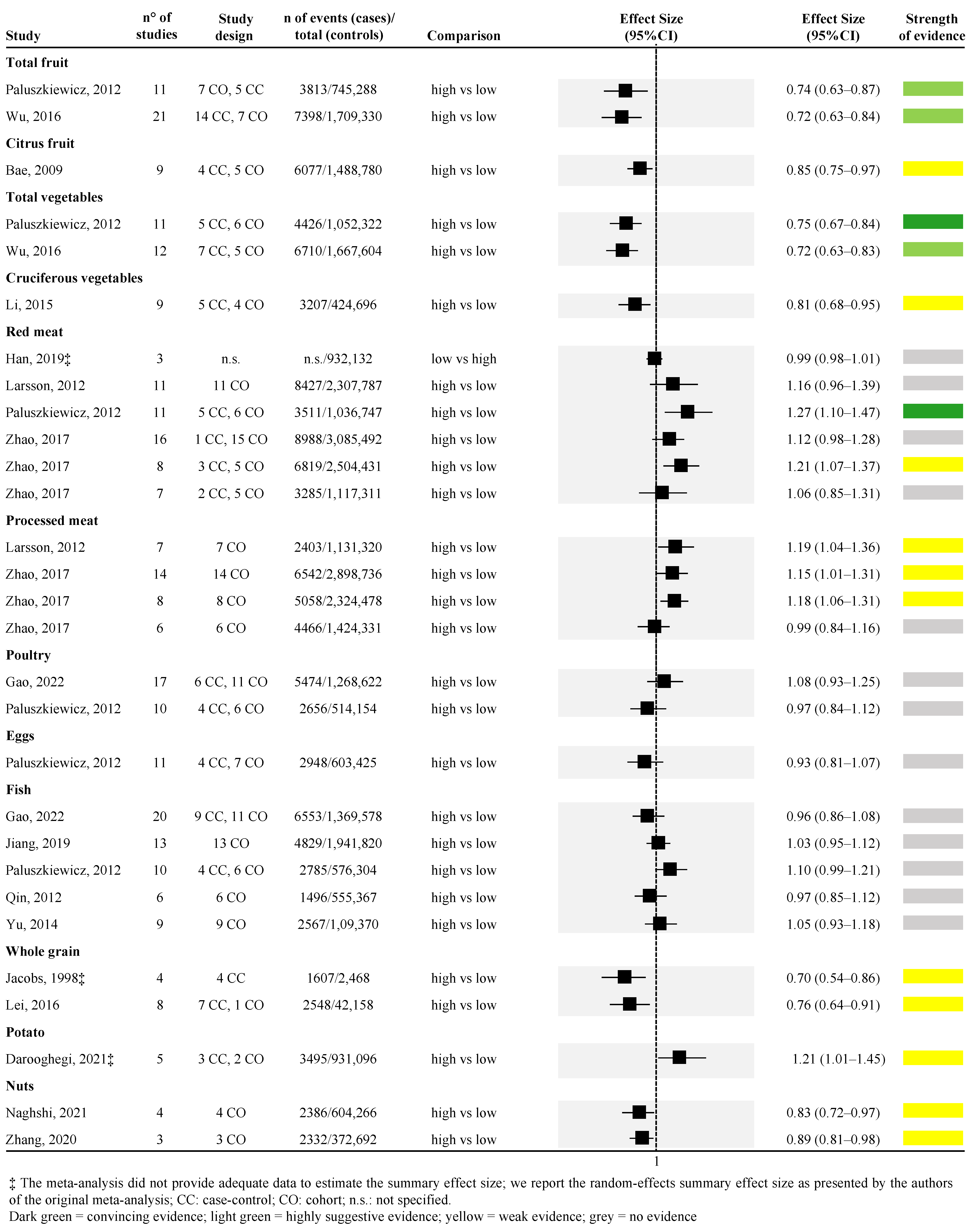
| Total fruit | |||||||||||||||
| Paluszkiewicz, 2012 [50] | 12 (7CO, 5CC) | High vs. low | RR | M/F | QRA for HOS | 3813 | 745,288 | 0.76 (0.67–0.87) | 0.74 (0.63–0.87) | 0.000 | 0.000 | (0.52–1.06) | 29.01 | Critically low | Highly suggestive |
| Wu, 2016 [53] | 21 (14CC, 7CO) | High vs. low | RR | M/F | NOS | 7398 | 1,709,330 | 0.79 (0.73–0.86) | 0.72 (0.63–0.84) | 0.000 | 0.000 | (0.43–1.23) | 57.67 | Low | Highly suggestive |
| Citrus fruit | |||||||||||||||
| Bae, 2009 [36] | 9 (4CC, 5CO) | High vs. low | RR | M/F | GRADE | 6077 | 1,488,780 | 0.88 (0.79–0.97) | 0.85 (0.75–0.97) | 0.011 | 0.016 | (0.65–1.11) | 28.99 | Low | Weak evidence |
| Total vegetables | |||||||||||||||
| Paluszkiewicz, 2012 [50] | 11 (5CC, 6CO) | High vs. low | RR | M/F | QRA for HOS | 4426 | 1,052,322 | 0.77 (0.70–0.84) | 0.75 (0.67–0.84) | 0.000 | 0.000 | (0.58–0.96) | 24.95 | Critically low | Convincing |
| Wu, 2016 [53] | 17 (12CC, 5CO) | High vs. low | RR | M/F | NOS | 6710 | 1,667,604 | 0.76 (0.69–0.83) | 0.72 (0.63–0.83) | 0.000 | 0.000 | (0.46–1.12) | 45.35 | Low | Highly suggestive |
| Cruciferous vegetables | |||||||||||||||
| Li, 2015 [47] | 9 (5CC, 4CO) | High vs. low | OR | M/F | NOS | 3207 | 424,696 | 0.83 (0.75–0.92) | 0.81 (0.68–0.95) | 0.000 | 0.010 | (0.52–1.25) | 53.13 | Moderate | Weak evidence |
| Whole grain | |||||||||||||||
| Jacobs, 1998 ‡ [42] | 4CC | High vs. low | OR | M/F | none | 1067 | 2468 | n.a. | 0.70 (0.54–0.86) | n.a. | n.a. | N.E. | n.a. | Critically low | Weak evidence |
| Lei, 2016 ‡ [46] | 8 (7CC, 1CO) | High vs. low | OR | M/F | NOS | 2548 | 42,158 | n.a. | 0.76 (0.64–0.91) | n.a. | 0.002 | N.E. | 11.70 | Critically low | Weak evidence |
| Red meat | |||||||||||||||
| Han, 2019 ‡ [41] | 3 | Low vs. High | RR | M/F | CATRITRB | n.s. | 932,132 | n.a. | 0.99 (0.98–1.01) | n.a. | n.a. | N.E. | n.a. | Moderate | N.E. |
| Larsson, 2012 [45] | 11CO | High vs. low | RR | M/F | none | 8427 | 2,307,787 | 1.10 (1.00–1.21) | 1.16 (0.96–1.39) | 0.051 | 0.117 | (0.60–2.18) | 67.91 | Critically low | No evidence |
| Paluszkiewicz, 2012 [50] | 11 (5CC, 6CO) | High vs. low | RR | M/F | QRA for HOS | 3511 | 1,036,747 | 1.25 (1.14–1.37) | 1.27 (1.10–1.47) | 0.000 | 0.001 | (0.89–1.81) | 46.43 | Critically low | Convincing |
| Zhao, 2017 [57] | 16 (1CC, 15CO) | High vs. low | RR | M/F | NOS | 8988 | 3,085,492 | 1.15 (1.07–1.25) | 1.12 (0.98–1.28) | 0.000 | 0.090 | (0.75–1.66) | 51.98 | Critically low | No evidence |
| Zhao, 2017 [57] | 8 (3CC, 5CO) | High vs. low | RR | M | NOS | 6819 | 2,504,431 | 1.21 (1.08–1.35) | 1.21 (1.07–1.37) | 0.001 | 0.002 | (1.05–1.39) | 12.99 | Critically low | Weak evidence |
| Zhao, 2017 [57] | 7 (2CC, 5CO) | High vs. low | RR | F | NOS | 3285 | 1,117,311 | 1.05 (0.89–1.23) | 1.06 (0.85–1.31) | 0.579 | 0.610 | (0.64–1.75) | 35.45 | Critically low | No evidence |
| Processed meat | |||||||||||||||
| Larsson, 2012 [45] | 7CO | High vs. low | RR | M/F | none | 2403 | 1,131,320 | 1.19 (1.04–1.36) | 1.19 (1.04–1.36) | 0.011 | 0.011 | (1.01–1.39) | 0.00 | Critically low | Weak evidence |
| Zhao, 2017 [57] | 14 CO | High vs. low | RR | M/F | NOS | 6542 | 2,898,736 | 1.17 (1.08–1.28) | 1.15 (1.01–1.31) | 0.000 | 0.004 | (0.82–1.62) | 45.67 | Critically low | Weak evidence |
| Zhao, 2017 [57] | 8 CO | High vs. low | RR | M | NOS | 5058 | 2,324,478 | 1.18 (1.06–1.31) | 1.18 (1.06–1.31) | 0.003 | 0.003 | (1.03–1.37) | 0.00 | Critically low | Weak evidence |
| Zhao, 2017 [57] | 6 CO | High vs. low | RR | F | NOS | 4466 | 1,424,331 | 0.99 (0.84–1.16) | 0.99 (0.84–1.16) | 0.884 | 0.884 | (0.83–1.19) | 0.00 | Critically low | No evidence |
| Poultry | |||||||||||||||
| Gao, 2022 [38] | 17 (6CC, 11CO) | High vs. low | RR | M/F | NOS | 5474 | 1,268,622 | 1.10 (1.0–1.21) | 1.08 (0.93–1.25) | 0.06 | 0.334 | (1.44–3.24) | 45.40 | Critically low | No evidence |
| Paluszkiewicz, 2012 [50] | 10 (4CC, 6CO) | High vs. low | RR | M/F | QRA for HOS | 2656 | 514,154 | 1.00 (0.92–1.09) | 0.97 (0.84–1.12) | 0.966 | 0.662 | (0.68–1.39) | 34.62 | Critically low | No evidence |
| Eggs | |||||||||||||||
| Paluszkiewicz, 2012 [50] | 11 (4CC, 7CO) | High vs. low | RR | M/F | QRA for HOS | 2948 | 603,425 | 0.95 (0.89–1.01) | 0.93 (0.81–1.07) | 0.081 | 0.322 | (0.66–1.33) | 48.59 | Critically low | No evidence |
| Fish | |||||||||||||||
| Gao, 2022 [38] | 20 (9CC, 11CO) | High vs. low | RR | M/F | NOS | 6553 | 1,369,578 | 0.94 (0.88–1.00) | 0.96 (0.86–1.08) | 0.061 | 0.480 | (0.44–0.95) | 54.57 | Critically low | No evidence |
| Jiang, 2019 [44] | 13CO | High vs. low | RR | M/F | NOS | 4829 | 1,941,820 | 1.03 (0.95–1.12) | 1.03 (0.95–1.12) | 0.471 | 0.471 | (0.95–1.12) | 0.00 | Low | No evidence |
| Paluszkiewicz, 2012 [38] | 10 (4CC, 6CO) | High vs. low | RR | M/F | QRA for HOS | 2785 | 576,304 | 1.10 (1.02–1.18) | 1.10 (0.99–1.21) | 0.008 | 0.070 | (0.98–1.23) | 22.58 | Critically low | No evidence |
| Qin, 2012 [51] | 6CO | High vs. low | HR | M/F | Based on 4 criteria defined by the authors | 1496 | 555,367 | 0.97 (0.85–1.12) | 0.97 (0.85–1.12) | 0.692 | 0.692 | (0.83–1.14) | 0.00 | Low | No evidence |
| Yu, 2014 [54] | 9CO | High vs. low | RR | M/F | NOS | 2567 | 1,094,370 | 1.05 (0.93–1.18) | 1.05 (0.93–1.18) | 0.464 | 0.464 | (0.90–1.20) | 0.00 | Low | No evidence |
| Potato | |||||||||||||||
| Darooghegi Mofrad, 2021 ‡ [37] | 5 (3CC, 2CO) | High vs. low | n.s. | M/F | ROBINS-E | 3495 | 931,096 | n.a. | 1.21 (1.01–1.45) | n.a. | 0.008 | N.E. | n.a. | Low | Weak evidence |
| Nuts | |||||||||||||||
| Naghshi, 2021 [49] | 4CO | High vs. low | HR | M/F | NOS | 2386 | 604,266 | 0.83 (0.72–0.97) | 0.83 (0.72–0.97) | 0.017 | 0.017 | (0.67–1.04) | 0.00 | Moderate | Weak evidence |
| Zhang, 2020 [55] | 3CO | High vs. low | RR | M/F | NOS | 2332 | 372,692 | 0.90 (0.83–0.97) | 0.89 (0.81–0.98) | 0.004 | 0.015 | (0.72–1.10) | 31.46 | Low | Weak evidence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianfredi, V.; Ferrara, P.; Dinu, M.; Nardi, M.; Nucci, D. Diets, Dietary Patterns, Single Foods and Pancreatic Cancer Risk: An Umbrella Review of Meta-Analyses. Int. J. Environ. Res. Public Health 2022, 19, 14787. https://doi.org/10.3390/ijerph192214787
Gianfredi V, Ferrara P, Dinu M, Nardi M, Nucci D. Diets, Dietary Patterns, Single Foods and Pancreatic Cancer Risk: An Umbrella Review of Meta-Analyses. International Journal of Environmental Research and Public Health. 2022; 19(22):14787. https://doi.org/10.3390/ijerph192214787
Chicago/Turabian StyleGianfredi, Vincenza, Pietro Ferrara, Monica Dinu, Mariateresa Nardi, and Daniele Nucci. 2022. "Diets, Dietary Patterns, Single Foods and Pancreatic Cancer Risk: An Umbrella Review of Meta-Analyses" International Journal of Environmental Research and Public Health 19, no. 22: 14787. https://doi.org/10.3390/ijerph192214787