
Long COVID at Different Altitudes: A Countrywide Epidemiological Analysis

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
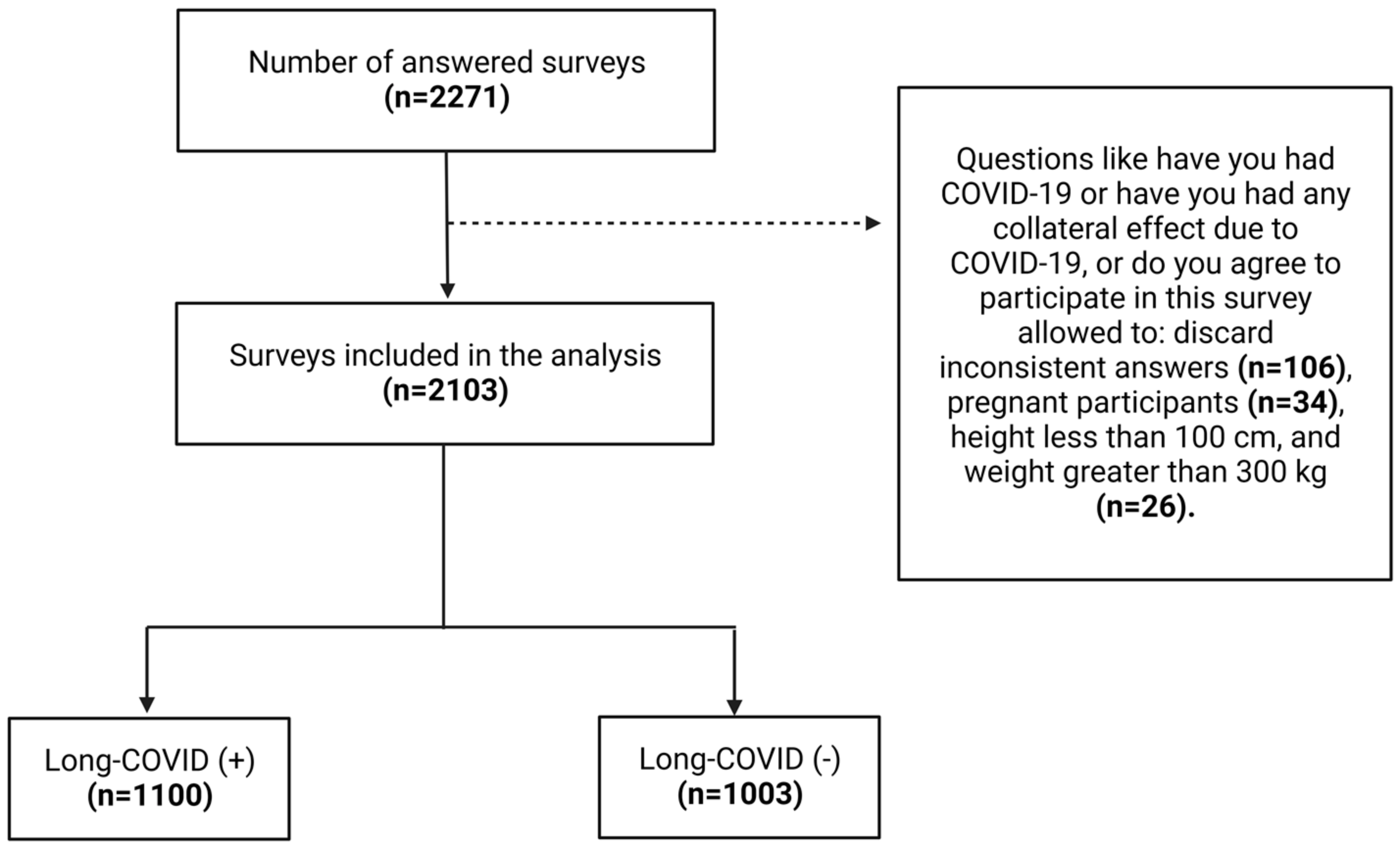
2.1. Study Design and Sample Selection
2.2. Settings
2.3. Population
2.4. Survey Development and Measures
2.5. Data Management
2.6. Statistical Analysis
2.7. Reliability and Validation
2.8. Ethical Approval
3. Results
3.1. General Demographic Information
3.2. Participants with Long-Term COVID19 Symptoms
3.2.1. Demographic and Past Medical History
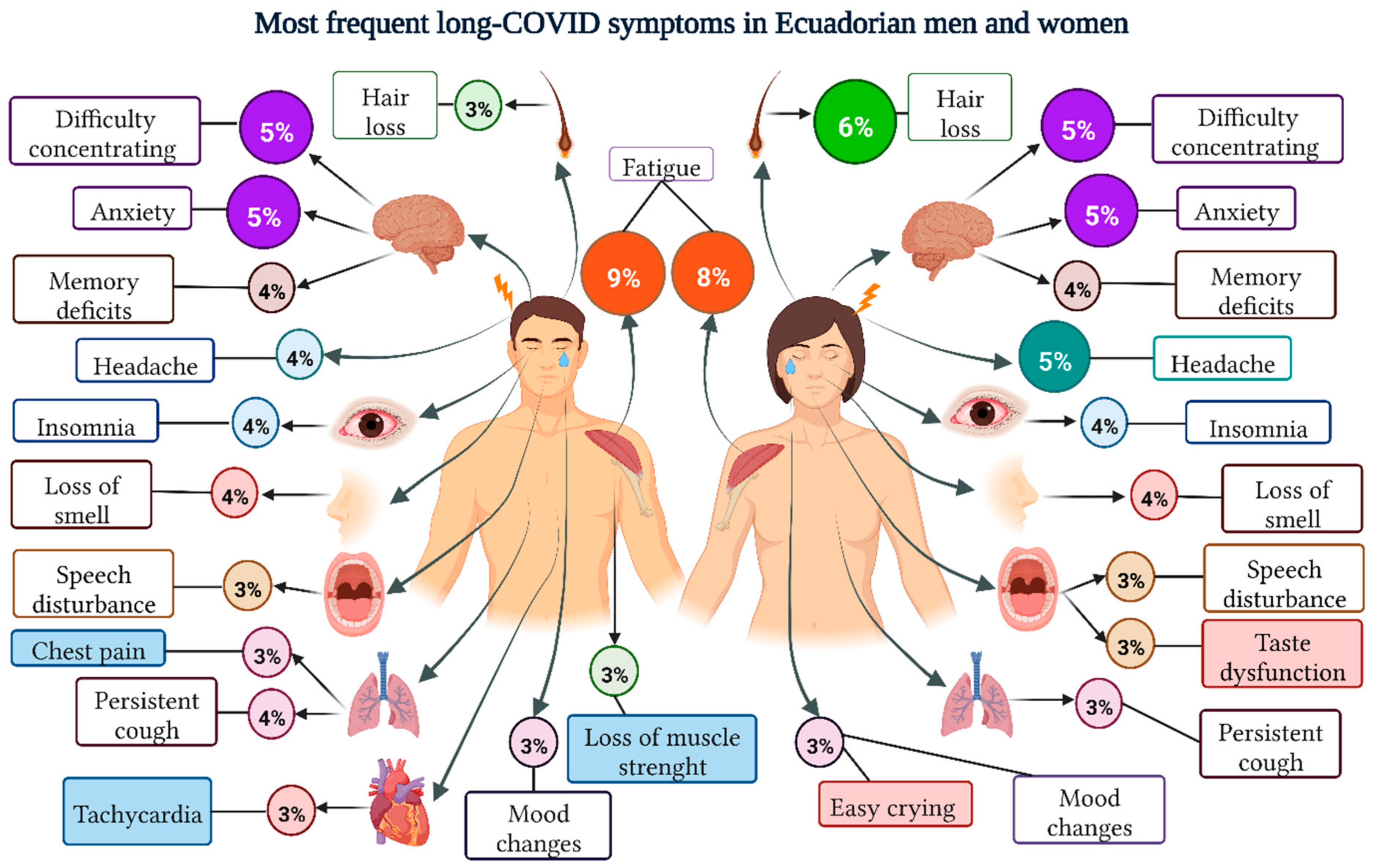
3.2.2. Symptomatologic Analysis
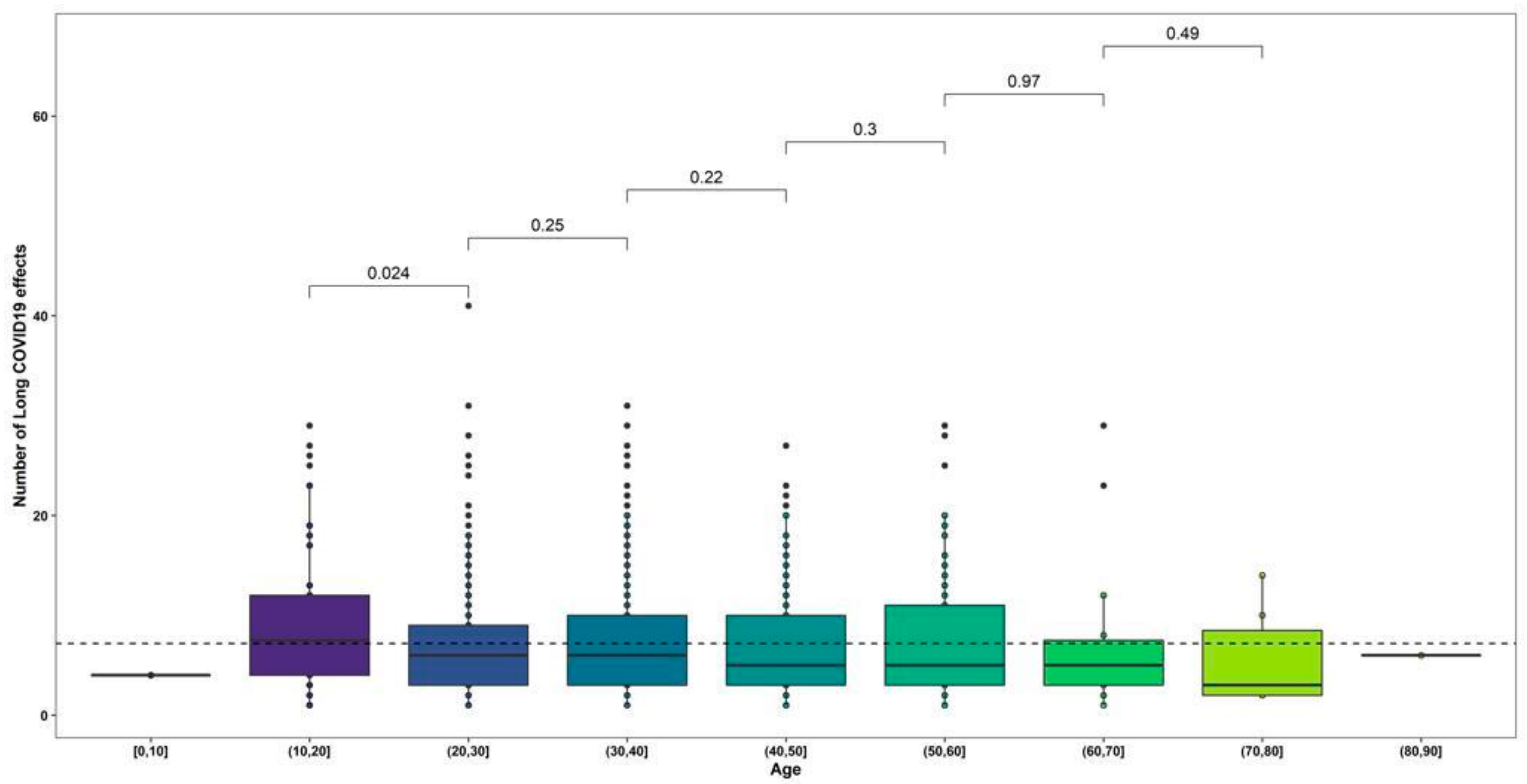
3.2.3. Age Group Analysis
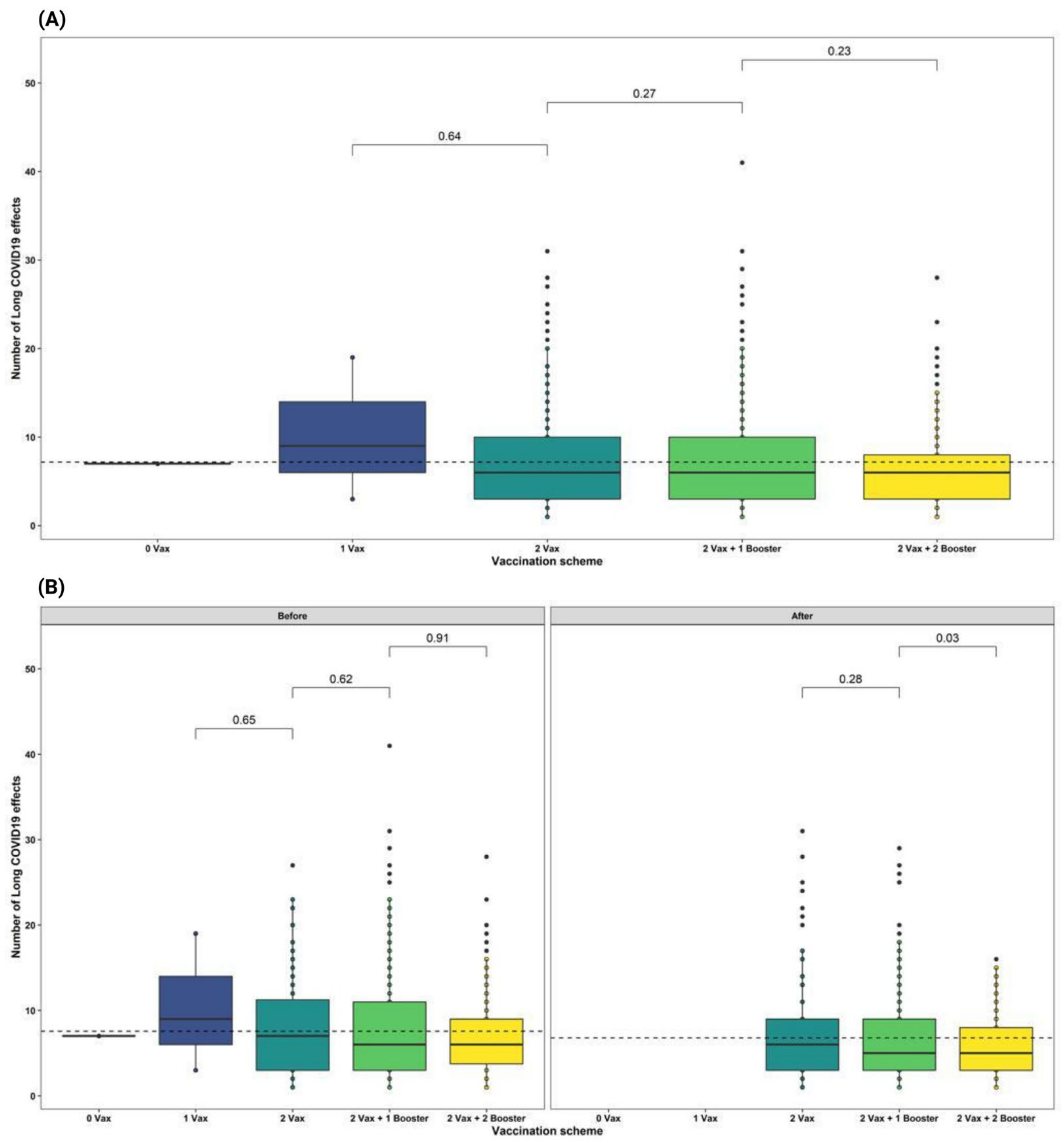
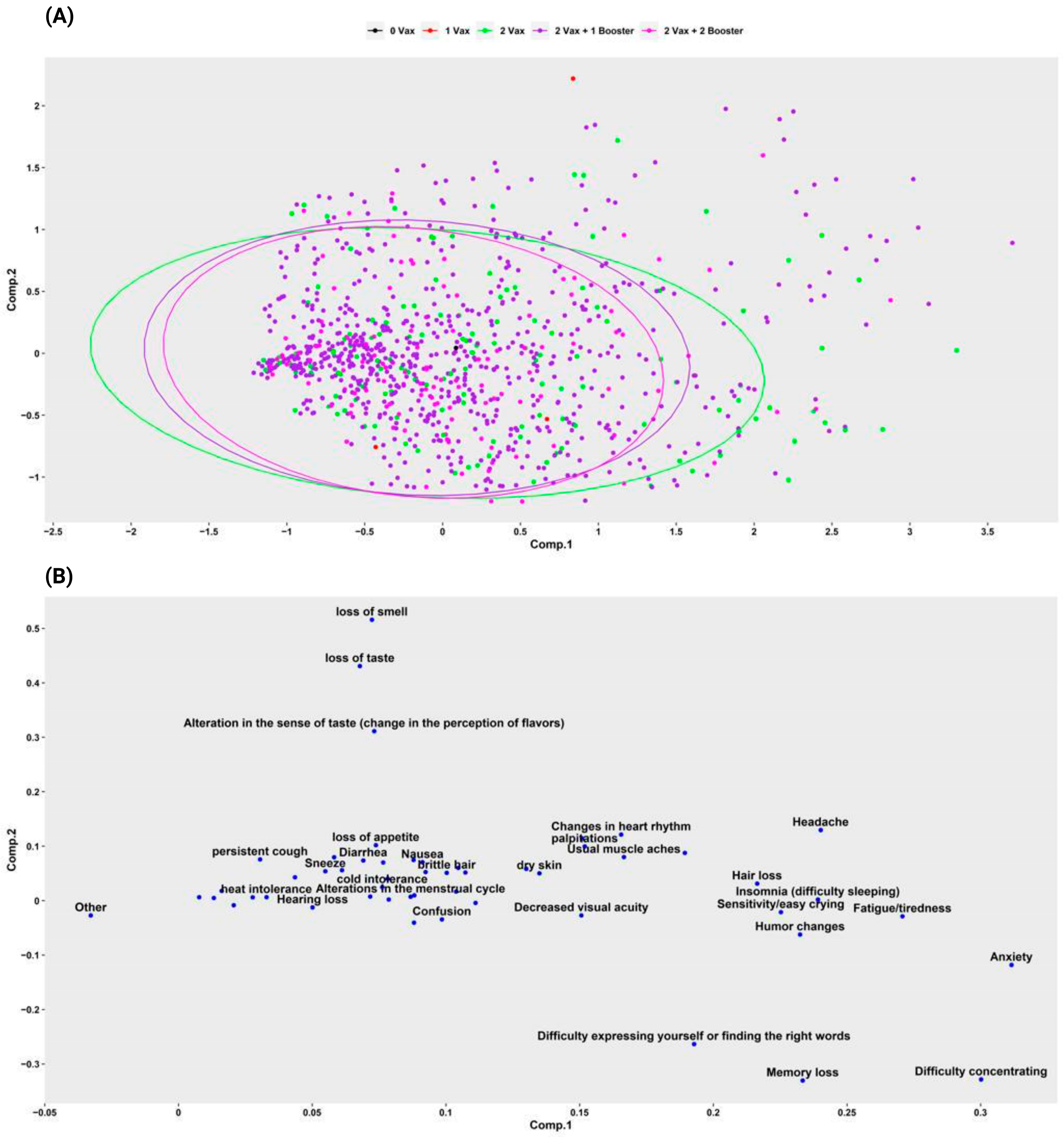
3.2.4. Long-COVID Symptoms by Vaccination Status
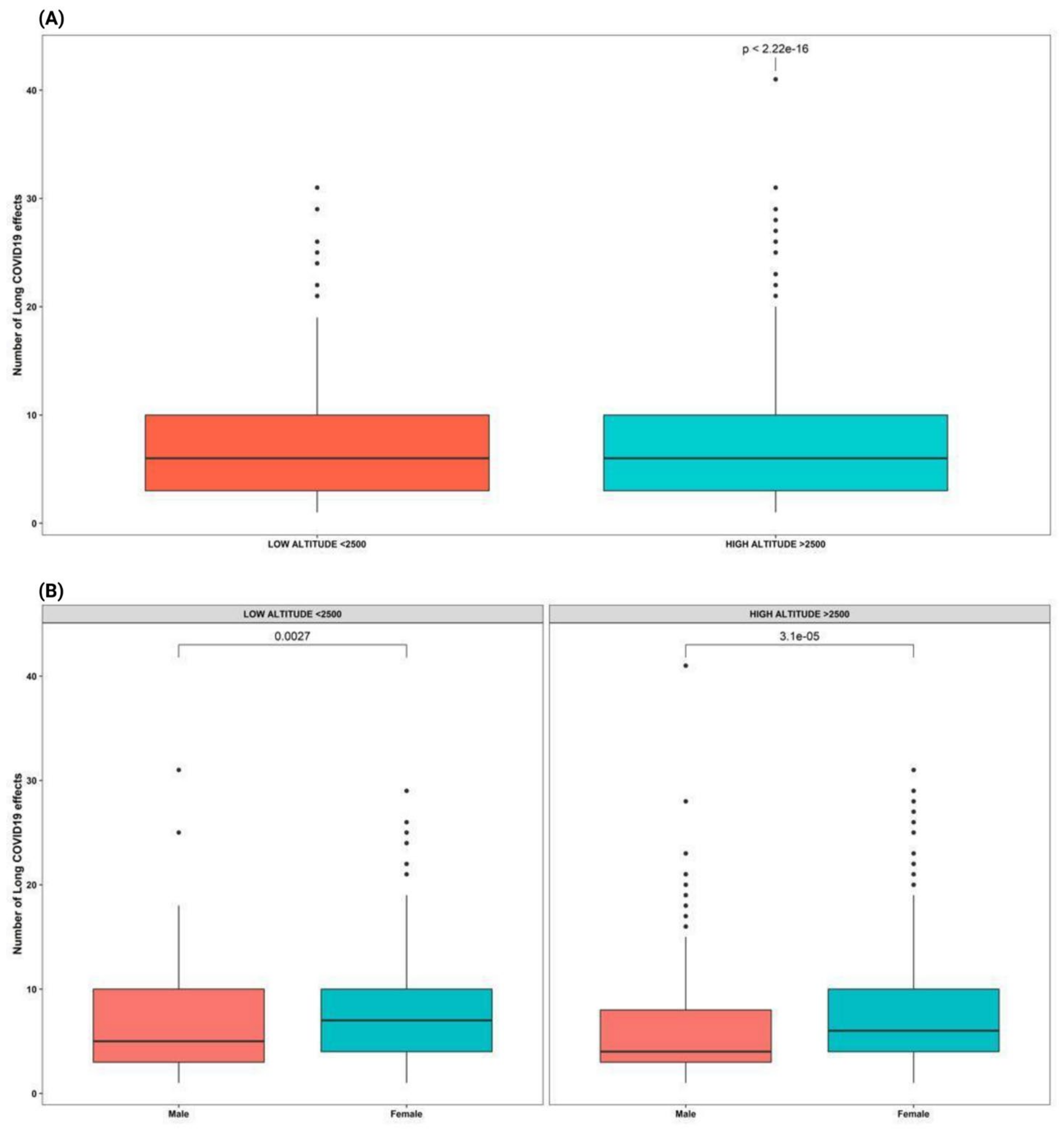
3.3. High Altitude of Residence
3.4. Symptoms Onset, Length, and Duration
3.5. Risk of Long-COVID Symptoms
3.6. Risk by Number of COVID-19 Infections
3.7. Health-Related Quality of Life of Participants with Post-Acute COVID
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worobey, M.; Levy, J.I.; Serrano, L.M.; Crits-Christoph, A.; Pekar, J.E.; Goldstein, S.A.; Rasmussen, A.L.; Kraemer, M.U.; Newman, C.; Koopmans, M.P.; et al. The Huanan Seafood Wholesale Market in Wuhan was the early epicenter of the COVID-19 pandemic. Science 2022, 377, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Chippa, V.; Aleem, A.; Anjum, F. Post Acute Coronavirus (COVID-19) Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK570608/ (accessed on 22 July 2022).
- Ortiz-Prado, E.; Simbaña-Rivera, K.; Gómez-Barreno, L.; Rubio-Neira, M.; Guaman, L.P.; Kyriakidis, N.C.; Muslin, C.; Gómez, A.M.; Barba-Ostria, C.; Cevallos-Robalino, D.; et al. Clinical, molecular and epidemiological characterization of the SARS-CoV2 virus and the Coronavirus disease 2019 (COVID-19), a comprehensive literature review. Diagn. Microbiol. Infect. Dis. 2020, 98, 115094. [Google Scholar] [CrossRef] [PubMed]
- PAHO. PAHO Weekly COVID-19 Epidemiological Update-27 September 2022-PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/paho-weekly-covid-19-epidemiological-update-27-september-2022 (accessed on 6 October 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Montenegro, F.; Unigarro, L.; Paredes, G.; Moya, T.; Romero, A.; Torres, L.; López, J.C.; Jara, F.E.; Del, G.; López-Cortés, A.; et al. Acute respiratory distress syndrome (ARDS) caused by the novel coronavirus disease (COVID-19): A practical comprehensive literature review. Expert Rev. Respir. Med. 2021, 15, 183–195. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- WHO. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. World Health Organization. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 22 July 2022).
- Van de Vyver, J.; Leite, A.C.; Alwan, N.A. Navigating the social identity of long covid. BMJ 2021, 375, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Alwan, N.A. The teachings of Long COVID. Commun. Med. 2021, 1, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 74, ciab611. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Iqbal, A.; Iqbal, K.; Ali, S.A.; Azim, D.; Farid, E.; Baig, M.D.; Bin, T.; Raza, M. The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus 2021, 13, e13080. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Yang, L.; Liang, B.; Ye, T.; Li, L.; Li, L.; Liu, D.; Wang, J.; Hesketh, R.L.; Zheng, C. Chest CT Patterns from Diagnosis to 1 Year of Follow-up in Patients with COVID-19. Radiology 2022, 302, 709–719. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xu, H.; Jiang, H.; Wang, L.; Lu, C.; Wei, X.; Liu, J.; Xu, S. The Clinical Features and Outcomes of Discharged Coronavirus Disease 2019 Patients: A Prospective Cohort Study. QJM Int. J. Med. 2020, 113, hcaa178. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, F.; Piva, S.; Stampatori, C.; Righetti, F.; Mega, I.; Peli, E.; Sala, E.; Tomasi, C.; Indelicato, A.M.; Latronico, N.; et al. Neurologic and cognitive sequelae after SARS-CoV2 infection: Different impairment for ICU patients. J. Neurol. Sci. 2022, 432, 120061. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236,379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef]
- Observatorio Social Ecuador. Vacunas|Coronavirus Ecuador. Available online: https://www.covid19ecuador.org/vacunas (accessed on 6 October 2022).
- Ortiz-Prado, E.; Fernandez Naranjo, R.P.; Vasconez, E.; Simbaña-Rivera, K.; Correa-Sancho, T.; Lister, A.; Calvopiña, M.; Viscor, G. Analysis of Excess Mortality Data at Different Altitudes During the COVID-19 Outbreak in Ecuador. High Alt. Med. Biol. 2021, 22, 406–416. [Google Scholar] [CrossRef]
- Pun, M.; Turner, R.; Strapazzon, G.; Brugger, H.; Swenson, E.R. Lower incidence of Covid-19 at high altitude: Facts and confounders. High Alt. Med. Biol. 2020, 21, 217–222. [Google Scholar] [CrossRef]
- Simbaña-Rivera, K.; Jaramillo, P.R.M.; Silva, J.V.V.; Gómez-Barreno, L.; Veintimilla, A.B.; Novillo, J.F.; Almache, W.E.; Cedeño, S.L.; Imba, L.G.; Moran, N.A.; et al. High-altitude is associated with better short-term survival in critically ill COVID-19 patients admitted to the ICU. PLoS ONE 2022, 17, e0262423. [Google Scholar]
- Walsh-Messinger, J.; Manis, H.; Vrabec, A.; Sizemore, j.; Bishof, K.; Debidda, M.; Malaspina, D.; Greenspan, N. The kids are not alright: A preliminary report of Post-COVID syndrome in university students. J. Am. Coll. Health 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef] [PubMed]
- Bonsaksen, T.; Leung, J.; Price, D.; Ruffolo, M.; Lamph, G.; Kebelenga, I.; Thygesen, H.; Geirdal, A.Ø. Self-Reported Long COVID in the General Population: Sociodemographic and Health Correlates in a Cross-National Sample. Life 2022, 12, 901. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 1–15. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Bungenberg, J.; Humkamp, K.; Hohenfeld, C.; Rust, M.I.; Ermis, U.; Dreher, M.; Hartmann, N.-U.K.; Marx, G.; Binkofski, F.; Finke, C.; et al. Long COVID-19: Objectifying most self-reported neurological symptoms. Ann. Clin. Transl. Neurol. 2022, 9, 141–154. [Google Scholar] [CrossRef]
- Jiang, L.; Liu, X.-Y.; Yan, X.-Q.; Liu, Y.-H.; Wang, Y.-J.; Yang, Y.; Wang, L.-R. One-year self-reported neurological sequelae in older COVID-19 survivors. Ageing Neurodegener. Dis. 2022, 2, 10. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, K.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef]
- Wong-Chew, R.M.; Rodríguez Cabrera, E.X.; Rodríguez Valdez, C.A.; Lomelin-Gascon, J.; Morales-Juárez, L.; Cerda, M.L.R.; Villa-Romero, A.R.; Fernández, S.A.; Fernanadez, M.S.; Bello, H.H.; et al. Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City. Ther. Adv. Infect. Dis. 2022, 9, 20499361211069264. [Google Scholar] [CrossRef] [PubMed]
- Smith, G. Does Gender Influence Online Survey Participation? A Record-Linkage Analysis of University Faculty Online Survey Response Behavior; ERIC Document Reproduction Service No. ED 501717; SJSU ScholarWorks: San Jose, CA, USA, 2018; pp. 1–21. [Google Scholar]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Munblit, D.; Pazukhina, E.; Ricchiuto, A.; Sinatti, D.; Zona, M.; Matteis, A.D.; D’Ilario, F.; Gentili, C.; Lanni, R.; et al. Post-COVID Condition in Adults and Children Living in the Same Household in Italy: A Prospective Cohort Study Using the ISARIC Global Follow-Up Protocol. Front. Pediatr. 2022, 10, 834875. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Torres-Macho, J.; Velasco-Arribas, M.; Plaza-Canteli, S.; Arias-Navalón, J.A.; Hernández-Barrera, V.; Guijarro, C. Preexisting hypertension is associated with a greater number of long-term post-COVID symptoms and poor sleep quality: A case–control study. J. Hum. Hypertens. 2022, 36, 582–584. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística y Censos INEC. País atrevido: La nueva cara sociodemográfica del Ecuador. Available online: https://web.archive.org/web/20130918214724/http://www.inec.gob.ec/publicaciones_libros/Nuevacarademograficadeecuador.pdf# (accessed on 29 July 2022).
- Barthélémy, H.; Mougenot, E.; Duracinsky, M.; Salmon-Ceron, D.; Bonini, J.; Péretz, F.; Chassany, O.; Carrieri, P. Smoking increases the risk of post-acute COVID-19 syndrome: Results from a French community-based survey. Tob. Induc. Dis. 2022, 20, 59. [Google Scholar] [CrossRef]
- Kuodi, P.; Gorelik, Y.; Zayyad, H.; Wertheim, O.; Wiegler, K.B.; Jabal, K.A.; Dror, A.A.; Nazzal, S.; Glikman, D.; Edelstein, M. Association between vaccination status and reported incidence of post-acute COVID-19 symptoms in Israel: A cross-sectional study of patients tested between March 2020 and November 2021. medRxiv 2022. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of long covid symptoms after covid-19 vaccination: Community based cohort study. BMJ 2022, 377, e069676. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Gurdasani, D.; O’Hara, M.E.; Hastie, C.; Roderick, P.; Yao, G.; Alwan, N.A. Characteristics and impact of Long Covid: Findings from an online survey. PLoS ONE 2022, 17, e0264331. [Google Scholar] [CrossRef]
- Paital, B.; Agrawal, P.K. Air pollution by NO2 and PM2.5 explains COVID-19 infection severity by overexpression of angiotensin-converting enzyme 2 in respiratory cells: A review. Environ. Chem. Lett. 2021, 19, 25–42. [Google Scholar] [CrossRef]
- Berger, M.M.; Hackett, P.H.; Bärtsch, P. No Relevant Analogy Between COVID-19 and Acute Mountain Sickness. High Alt. Med. Biol. 2020. [Google Scholar] [CrossRef]
- Imray, C.; Wright, A.; Subudhi, A.; Roach, R. Acute Mountain sickness: Pathophysiology, prevention, and treatment. Prog. Cardiovasc. Dis. 2010, 52, 467–484. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Sareban, M.; Bärtsch, P. Acute mountain sickness: Do different time courses point to different pathophysiological mechanisms? J. Appl. Physiol. 2020, 128, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Prado, E.; Simbaña-Rivera, K.; Duta, D.; Ochoa, I.; Izquierdo-Condoy, J.S.; Vasconez, E.; Carrasco, K.; Calvopiña, M.; Viscor, G.; Paz, C. Optimism and Health Self-Perception-Related Differences in Indigenous Kiwchas of Ecuador at Low and High Altitude: A Cross-Sectional Analysis. High Alt. Med. Biol. 2022, 23, 26–36. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Long COVID n (%) | Not Long COVID n (%) | Total n | p-Value | |
|---|---|---|---|---|---|
| Respondents | 1100 (52.3) | 1003 (47.7) | 2103 | ||
| Demographics | |||||
| Sex | Male | 396 (48.2) | 425 (51.8) | 821 | 0.003 |
| Female | 704 (54.9) | 578 (45.1) | 1282 | ||
| Age (years) | 0 to 10 | 1 (33.3) | 2 (66.7) | 3 | <0.001 |
| 10 to 20 | 60 (33.5) | 119 (66.5) | 179 | ||
| 21 to 30 | 382 (50.1) | 381 (49.9) | 763 | ||
| 31 to 40 | 372 (56.8) | 283 (43.2) | 655 | ||
| 41 to 50 | 191 (55.7) | 152 (44.3) | 343 | ||
| 51 to 60 | 72 (57.1) | 54 (42.9) | 126 | ||
| 61 to 70 | 15 (60.0) | 10 (40.0) | 25 | ||
| 71 to 80 | 6 (75.0) | 2 (25.0) | 8 | ||
| 81 to 90 | 1 (100.0) | 1 | |||
| Residence altitude | Out of the country | 5 (55.6) | 4 (44.4) | 9 | 0.368 |
| >2500 m | 789 (53.3) | 692 (46.7) | 1481 | ||
| <2500 m | 306 (49.9) | 307 (50.1) | 613 | ||
| Comorbidities | No | 853 (49.4) | 873 (50.6) | 1726 | <0.001 |
| Yes | 247 (65.5) | 130 (34.5) | 377 | ||
| Smoke | No | 993 (52.4) | 901 (47.6) | 1894 | 0.79 |
| Yes | 107 (51.2) | 102 (48.8) | 209 | ||
| Alcohol | No | 298 (53.0) | 264 (47.0) | 562 | 0.726 |
| Yes | 802 (52.0) | 739 (48.0) | 1541 | ||
| Severity of infection | Mild | 1056 (51.7) | 987 (48.3) | 2043 | <0.001 |
| Moderate | 19 (59.4) | 13 (40.6) | 32 | ||
| Severe | 25 (89.3) | 3 (10.7) | 28 |
| Symptom | Vaccine n (%) | Time of Infection n (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total n | No Vax. | 1 Dose | 2 Doses | 2 Doses + 1 Boosters | 2 Doses + 2 Boosters | p-Value | Before Vaccine | After Vaccine | p-Value | |
| Alopecia | 32 | -- | -- | 7 (21.9) | 23 (71.9) | 2 (6.2) | 0.383 | 16 (50.0) | 16 (50.0) | 0.999 |
| Taste dysfunction | 199 | -- | 1 (0.5) | 32 (16.1) | 138 (69.3) | 28 (14.1) | 0.841 | 121 (60.8) | 78 (39.2) | 0.002 |
| Alterations in glucose | 16 | -- | -- | 5 (31.3) | 10 (62.5) | 1 (6.2) | 0.202 | 9 (56.2) | 7 (43.8) | 0.864 |
| Menstrual cycle alterations | 118 | -- | -- | 16 (13.6) | 81 (68.6) | 21 (17.8) | 0.231 | 56 (47.5) | 62 (52.5) | 0.473 |
| Hallucinations | 20 | 1 (5.0) | -- | 6 (30.0) | 13 (65.0) | -- | <0.001 | 13 (65.0) | 7 (35.0) | 0.299 |
| Anxiety | 379 | 1 (0.3) | 1 (0.3) | 68 (17.9) | 271 (71.5) | 38 (10.0) | 0.114 | 205 (54.1) | 174 (45.9) | 0.154 |
| Brittle hair | 111 | -- | -- | 16 (14.4) | 81 (73.0) | 14 (12.6) | 0.901 | 65 (58.6) | 46 (41.4) | 0.114 |
| Mood changes | 234 | -- | -- | 40 (17.1) | 173 (73.9) | 21 (9.0) | 0.119 | 123 (52.6) | 111 (47.4) | 0.641 |
| Tachycardia | 184 | 1 (0.5) | 1 (0.5) | 32 (17.4) | 131 (71.3) | 19 (10.3) | 0.13 | 99 (53.8) | 85 (46.2) | 0.451 |
| Blood pressure changes | 74 | -- | 1 (1.3) | 13 (17.6) | 51 (68.9) | 9 (12.2) | 0.303 | 42 (56.8) | 32 (43.2) | 0.365 |
| Confusion | 61 | 1 (1.6) | -- | 18 (29.5) | 39 (64.0) | 3 (4.9) | <0.001 | 39 (63.9) | 22 (36.1) | 0.051 |
| Diarrhea | 56 | -- | -- | 10 (17.9) | 36 (64.2) | 10 (17.9) | 0.436 | 32 (57.1) | 24 (42.9) | 0.419 |
| Difficulty concentrating | 387 | -- | 2 (0.5) | 59 (15.2) | 270 (69.8) | 56 (14.5) | 0.449 | 214 (55.3) | 173 (44.7) | 0.042 |
| Speech disturbance | 241 | -- | 1 (0.4) | 45 (18.7) | 159 (66.0) | 36 (14.9) | 0.26 | 126 (52.3) | 115 (47.7) | 0.705 |
| Decreased visual acuity | 147 | -- | 1 (0.7) | 29 (19.7) | 100 (68.0) | 17 (11.6) | 0.361 | 92 (62.6) | 55 (37.4) | 0.003 |
| Loss of muscle strength | 170 | -- | -- | 32 (18.8) | 128 (75.3) | 10 (5.9) | 0.009 | 91 (53.5) | 79 (46.5) | 0.526 |
| Decreased libido/sexual desire | 115 | -- | -- | 18 (15.7) | 81 (70.4) | 16 (13.9) | 0.949 | 60 (52.2) | 55 (47.8) | 0.866 |
| Abdominal pain | 70 | -- | -- | 11 (15.7) | 47 (67.2) | 12 (17.1) | 0.551 | 32 (45.7) | 38 (54.3) | 0.429 |
| Headache | 354 | 1 (0.3) | 1 (0.3) | 56 (15.8) | 246 (69.5) | 50 (14.1) | 0.578 | 184 (52.0) | 170 (48.0) | 0.702 |
| Chest pain | 187 | -- | 1 (0.5) | 31 (16.6) | 136 (72.7) | 19 (10.2) | 0.555 | 92 (49.2) | 95 (50.8) | 0.644 |
| Burning sensation in any part of the body | 75 | -- | -- | 15 (20.0) | 57 (76.0) | 3 (4.0) | 0.046 | 40 (53.3) | 35 (46.7) | 0.764 |
| Unusual muscle aches | 109 | -- | 1 (0.9) | 18 (16.5) | 77 (70.7) | 13 (11.9) | 0.576 | 56 (51.4) | 53 (48.6) | 0.999 |
| Usual muscle aches | 164 | -- | 1 (0.6) | 33 (20.1) | 112 (68.3) | 18 (11.0) | 0.269 | 88 (53.7) | 76 (46.3) | 0.513 |
| Shaking chills | 45 | -- | 1 (2.2) | 8 (17.8) | 33 (73.3) | 3 (6.7) | 0.043 | 22 (48.9) | 23 (51.1) | 0.891 |
| Sneezing | 92 | -- | 1 (1.0) | 11 (12.0) | 71 (77.2) | 9 (9.8) | 0.199 | 41 (44.6) | 51 (55.4) | 0.237 |
| Fatigue or tiredness | 652 | 1 (0.2) | 2 (0.3) | 101 (15.5) | 460 (70.5) | 88 (13.5) | 0.863 | 331 (50.8) | 321 (49.2) | 0.9 |
| Tingling in extremities | 137 | -- | -- | 25 (18.3) | 101 (73.7) | 11 (8.0) | 0.159 | 76 (55.5) | 61 (44.5) | 0.303 |
| Insomnia | 342 | -- | -- | 54 (15.8) | 252 (73.7) | 36 (10.5) | 0.262 | 175 (51.2) | 167 (48.8) | 0.991 |
| Heat intolerance | 20 | -- | -- | 6 (30.0) | 12 (60.0) | 2 (10.0) | 0.211 | 10 (50.0) | 10 (50.0) | 0.999 |
| Cold intolerance | 92 | -- | -- | 16 (17.4) | 65 (70.6) | 11 (12.0) | 0.883 | 54 (58.7) | 38 (41.3) | 0.151 |
| Nausea | 68 | -- | 1 (1.5) | 13 (19.1) | 47 (69.1) | 7 (10.3) | 0.19 | 31 (45.6) | 37 (54.4) | 0.425 |
| Neuritis | 96 | -- | -- | 20 (20.8) | 65 (67.7) | 11 (11.5) | 0.355 | 48 (50.0) | 48 (50.0) | 0.921 |
| Palpitations | 182 | 1 (0.6) | 1 (0.5) | 30 (16.5) | 125 (68.7) | 25 (13.7) | 0.197 | 96 (52.8) | 86 (47.2) | 0.663 |
| Facial paralysis | 7 | -- | -- | 1 (14.3) | 5 (71.4) | 1 (14.3) | 0.99 | 5 (71.4) | 2 (28.6) | 0.48 |
| Loss of appetite | 55 | -- | 1 (1.8) | 9 (16.4) | 39 (70.9) | 6 (10.9) | 0.153 | 23 (41.8) | 32 (58.2) | 0.207 |
| Hearing loss | 49 | -- | -- | 7 (14.3) | 36 (73.5) | 6 (12.2) | 0.937 | 33 (67.3) | 16 (32.7) | 0.028 |
| Hair loss | 391 | -- | 2 (0.5) | 62 (15.9) | 274 (70.0) | 53 (13.6) | 0.672 | 227 (58.1) | 164 (41.9) | <0.001 |
| Loss of taste | 172 | -- | 1 (0.6) | 27 (15.7) | 125 (72.7) | 19 (11.0) | 0.719 | 114 (66.3) | 58 (33.7) | <0.001 |
| Memory deficits | 287 | -- | 2 (0.7) | 54 (18.8) | 196 (68.3) | 35 (12.2) | 0.14 | 155 (54.0) | 132 (46.0) | 0.264 |
| Muscle loss | 97 | -- | 1 (1.0) | 12 (12.4) | 69 (71.1) | 15 (15.5) | 0.315 | 59 (60.8) | 38 (39.2) | 0.054 |
| Loss of smell | 263 | -- | 2 (0.8) | 37 (14.1) | 190 (72.2) | 34 (12.9) | 0.296 | 170 (64.6) | 93 (35.4) | <0.001 |
| Body hair loss | 14 | -- | -- | 2 (14.3) | 12 (85.7) | -- | 0.978 | 7 (50.0) | 7 (50.0) | 0.999 |
| Pruritus (itching) | 114 | -- | -- | 22 (19.3) | 76 (66.7) | 16 (14.0) | 0.475 | 66 (57.9) | 48 (42.1) | 0.145 |
| Gastroesophageal reflux | 87 | -- | -- | 16 (18.4) | 62 (71.3) | 9 (10.3) | 0.636 | 51 (58.6) | 36 (41.4) | 0.17 |
| Skin dryness | 139 | -- | -- | 28 (20.1) | 98 (70.5) | 13 (9.4) | 0.171 | 71 (51.1) | 68 (48.9) | 0.999 |
| Thirst | 77 | -- | 1 (1.3) | 11 (14.3) | 61 (79.2) | 4 (5.2) | 0.048 | 30 (39.0) | 47 (61.0) | 0.038 |
| Easy crying | 202 | -- | -- | 40 (19.8) | 138 (68.3) | 24 (11.9) | 0.217 | 114 (56.4) | 88 (43.6) | 0.102 |
| Excessive sweating | 90 | -- | 1 (1.1) | 16 (17.8) | 59 (65.5) | 14 (15.6) | 0.292 | 51 (56.7) | 39 (43.3) | 0.311 |
| Tremor of the extremities | 90 | -- | -- | 20 (22.2) | 59 (65.6) | 11 (12.2) | 0.216 | 48 (53.3) | 42 (46.7) | 0.724 |
| Persistent cough | 245 | -- | 1 (0.4) | 28 (11.4) | 185 (75.5) | 31 (12.7) | 0.184 | 93 (38.0) | 152 (62.0) | <0.001 |
| Brittle nails | 113 | -- | -- | 20 (17.7) | 80 (70.8) | 13 (11.5) | 0.778 | 58 (51.3) | 55 (48.7) | 0.999 |
| Vomit | 25 | -- | 1 (4.0) | 4 (16.0) | 17 (68.0) | 3 (12.0) | 0.004 | 10 (40.0) | 15 (60.0) | 0.362 |
| Total | 7746 | 7 | 31 | 1310 | 5472 | 926 | 4164 | 3582 | ||
| Altitude n (%) | ||||||
|---|---|---|---|---|---|---|
| Out of the Country | <2500 m | >2500 m | p-Value | Total n | ||
| Symptoms | Taste dysfunction | -- | 46 (23.1) | 153 (76.9) | 0.111 | 199 |
| Menstrual cycle alterations | 1 (0.9) | 26 (22.0) | 91 (77.1) | 0.276 | 118 | |
| Anxiety | 1 (0.3) | 114 (30.0) | 264 (69.7) | 0.392 | 379 | |
| Brittle hair | -- | 33 (29.7) | 78 (70.3) | 0.741 | 111 | |
| Mood changes | -- | 79 (33.8) | 155 (66.2) | 0.031 | 234 | |
| Tachycardia | -- | 67 (36.4) | 117 (63.6) | 0.006 | 184 | |
| Difficulty concentrating | 1 (0.3) | 101 (26.1) | 285 (73.6) | 0.485 | 387 | |
| Speech disturbance | -- | 59 (24.5) | 182 (75.5) | 0.202 | 241 | |
| Decreased visual acuity | 1 (0.7) | 44 (29.9) | 102 (69.4) | 0.743 | 147 | |
| Loss of muscle strength | 1 (0.6) | 54 (31.8) | 115 (67.6) | 0.433 | 170 | |
| Decreased libido/sexual desire | 1 (0.9) | 43 (37.4) | 71 (61.7) | 0.038 | 115 | |
| Headache | -- | 98 (27.7) | 256 (72.3) | 0.951 | 354 | |
| Chest pain | -- | 59 (31.6) | 128 (68.4) | 0.263 | 187 | |
| Unusual muscle aches | -- | 27 (24.8) | 82 (75.2) | 0.505 | 109 | |
| Usual muscle aches | -- | 46 (28.0) | 118 (72.0) | 0.999 | 164 | |
| Fatigue or tiredness | 3 (0.5) | 188 (28.8) | 461 (70.7) | 0.66 | 652 | |
| Tingling in extremities | -- | 43 (31.4) | 94 (68.6) | 0.39 | 137 | |
| Insomnia | 2 (0.6) | 114 (33.3) | 226 (66.1) | 0.02 | 342 | |
| Palpitations | -- | 66 (36.3) | 116 (63.7) | 0.008 | 182 | |
| Hair loss | 2 (0.5) | 113 (28.9) | 276 (70.6) | 0.815 | 391 | |
| Loss of taste | -- | 47 (27.3) | 125 (72.7) | 0.916 | 172 | |
| Memory deficits | 1 (0.4) | 73 (25.4) | 213 (74.2) | 0.542 | 287 | |
| Loss of smell | -- | 67 (25.5) | 196 (74.5) | 0.344 | 263 | |
| Pruritus (itching) | -- | 35 (30.7) | 79 (69.3) | 0.56 | 114 | |
| Skin dryness | -- | 32 (23.0) | 107 (77.0) | 0.199 | 139 | |
| Easy crying | -- | 59 (29.2) | 143 (70.8) | 0.721 | 202 | |
| Persistent cough | 1 (0.4) | 75 (30.6) | 169 (69.0) | 0.54 | 245 | |
| Brittle nails | -- | 30 (26.6) | 83 (73.4) | 0.811 | 113 | |
| Total | 6338 | |||||
| Symptom characteristics | ||||||
| Onset time | Initiated with infection | 4 (0.9) | 104 (23.2) | 341 (76.0) | 0.004 | |
| 3 to 5 weeks after infection | 1 (0.2) | 126 (30.4) | 287 (69.3) | 0.243 | ||
| 5 to 7 weeks after infection | . | 28 (27.2) | 75 (72.8) | 0.948 | ||
| 7 to 9 weeks after infection | . | 15 (30.0) | 35 (70.0) | 0.865 | ||
| After 9 weeks of infection | . | 33 (39.3) | 51 (60.7) | 0.022 | ||
| Symptoms duration | Between 1 to 4 weeks | . | 53 (23.7) | 171 (76.3) | 0.129 | |
| Between 4 to 8 weeks | . | 47 (25.8) | 135 (74.2) | 0.543 | ||
| Between 8 to 12 weeks | 3 (2.6) | 28 (24.4) | 84 (73.0) | 0.001 | ||
| Between 3 to 6 months | . | 60 (28.6) | 150 (71.4) | 0.889 | ||
| Between 6 to 12 months | . | 34 (26.0) | 97 (74.1) | 0.662 | ||
| More than 12 months | 2 (0.8) | 84 (35.3) | 152 (63.9) | 0.007 | ||
| Frequency of presentation | Once a month | . | 23 (23.7) | 74 (76.3) | 0.393 | |
| Once every two weeks | . | 20 (23.8) | 64 (76.2) | 0.452 | ||
| Once a week | . | 75 (34.7) | 141 (65.3) | 0.016 | ||
| Over 3 days a week | 2 (0.7) | 82 (27.6) | 213 (71.7) | 0.804 | ||
| Daily | 3 (0.9) | 94 (28.4) | 234 (70.7) | 0.324 | ||
| Total | 15 | 918 | 2367 | |||
| Characteristics | Long COVID n = 1100 | Not long COVID n = 1003 | OR (95% CI) | |
|---|---|---|---|---|
| (n) | (n) | |||
| Sex | Men (ref.) | 396 | 425 | 1.31 (1.10–1.56) |
| Women | 704 | 578 | ||
| Altitude | Low (ref.) | 306 | 307 | 1.14 (0.95–1.38) |
| High | 789 | 692 | ||
| Comorbidities | No (ref.) | 853 | 873 | 1.95 (1.541–2.453) |
| Yes | 247 | 130 | ||
| Smoke | No (ref.) | 993 | 901 | 0.95 (0.72–1.27) |
| Yes | 107 | 102 | ||
| Alcohol | No (ref.) | 298 | 264 | 0.96 (0.79–1.17) |
| Yes | 802 | 739 | ||
| Severity of infection | Mild (ref.) | 1056 | 987 | |
| Moderate | 19 | 13 | 1.37 (0.67–2.78) | |
| Severe | 25 | 3 | 7.79 (2.34–25.88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izquierdo-Condoy, J.S.; Fernandez-Naranjo, R.; Vasconez-González, E.; Cordovez, S.; Tello-De-la-Torre, A.; Paz, C.; Delgado-Moreira, K.; Carrington, S.; Viscor, G.; Ortiz-Prado, E. Long COVID at Different Altitudes: A Countrywide Epidemiological Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14673. https://doi.org/10.3390/ijerph192214673
Izquierdo-Condoy JS, Fernandez-Naranjo R, Vasconez-González E, Cordovez S, Tello-De-la-Torre A, Paz C, Delgado-Moreira K, Carrington S, Viscor G, Ortiz-Prado E. Long COVID at Different Altitudes: A Countrywide Epidemiological Analysis. International Journal of Environmental Research and Public Health. 2022; 19(22):14673. https://doi.org/10.3390/ijerph192214673
Chicago/Turabian StyleIzquierdo-Condoy, Juan S., Raul Fernandez-Naranjo, Eduardo Vasconez-González, Simone Cordovez, Andrea Tello-De-la-Torre, Clara Paz, Karen Delgado-Moreira, Sarah Carrington, Ginés Viscor, and Esteban Ortiz-Prado. 2022. "Long COVID at Different Altitudes: A Countrywide Epidemiological Analysis" International Journal of Environmental Research and Public Health 19, no. 22: 14673. https://doi.org/10.3390/ijerph192214673