
Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Research Questions
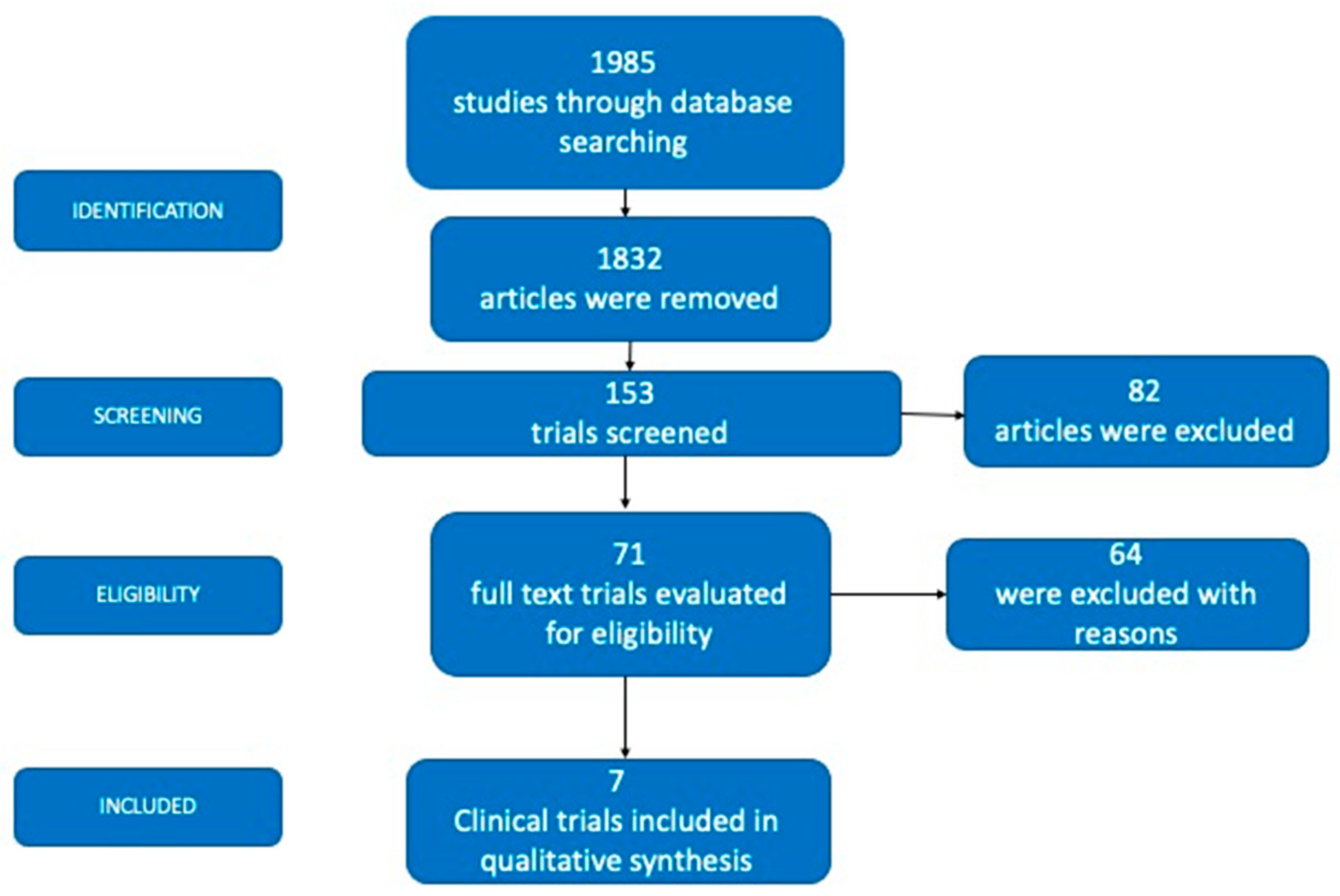
2.4. Data Selection
2.5. Data Extraction
2.6. Outcome Measures
2.7. Risk of Bias
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Razi, M.A.; Mahajan, A.; Qamar, S.; Mehra, S.; Roy, T.R.; Kumari, P. A Comparative Study of Platelet-rich Fibrin (PRF) and Titanium-prepared Platelet-rich Fibrin (T-PRF) in Management of Endo-perio Lesions. J. Contemp. Dent. Pract. 2020, 21, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Retamal-Valdes, B.; Alonso, B.; Feres, M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J. Periodontol. 2018, 89, S85–S102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Tewari, S.; Tewari, S.; Mittal, S. Effect of Time Lapse between Endodontic and Periodontal Therapies on the Healing of Concurrent Endodontic-Periodontal Lesions without Communication: A Prospective Randomized Clinical Trial. J. Endod. 2015, 41, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, X.; Xu, J.; Zhou, X.; Xie, K. Hua Xi Kou Qiang Yi Xue Za Zhi. West China J. Stomatol. 2012, 30, 161–168. [Google Scholar]
- Dembowska, E.; Jaroń, A.; Homik-Rodzińska, A.; Gabrysz-Trybek, E.; Bladowska, J.; Trybek, G. Comparison of the Treatment Efficacy of Endo-Perio Lesions Using a Standard Treatment Protocol and Extended by Using a Diode Laser (940 nm). J. Clin. Med. 2022, 11, 811. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Mao, X.; Hu, F.; Liu, J.; Wang, J. Observation on the effect of periodontal treatment on patients with combined periodontal-pulpal lesions. Am. J. Transl. Res. 2021, 13, 11938–11942. [Google Scholar] [PubMed]
- AlJasser, R.; Bukhary, S.; AlSarhan, M.; Alotaibi, D.; AlOraini, S.; Habib, S.R. Regenerative Therapy Modality for Treatment of True Combined Endodontic-Periodontal Lesions: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 6220. [Google Scholar] [CrossRef] [PubMed]
- Tewari, S.; Sharma, G.; Tewari, S.; Mittal, S.; Bansal, S. Effect of immediate periodontal surgical treatment on periodontal healing in combined endodontic-periodontal lesions with communication—A randomized clinical trial. J. Oral Biol. Craniofac. Res. 2018, 8, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.C.; Walter, C.; Amato, M.; Weiger, R. Treatment of periodontal-endodontic lesions--a systematic review. J. Clin. Periodontol. 2014, 41, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Dakó, T.; Lazăr, A.P.; Bică, C.I.; Lazăr, L. Endo-perio lesions: Diagnosis and interdisciplinary treatment options. Acta Stomatol. Marisiensis 2020, 3, 257–261. [Google Scholar]
- Abbott, P.V.; Salgado, J.C. Strategies for the endodontic management of concurrent endodontic and periodontal diseases. Aust. Dent. J. 2009, 54, S70–S85. [Google Scholar] [CrossRef] [PubMed]
- Citterio, F.; Gualini, G.; Chang, M.; Piccoli, G.M.; Giraudi, M.; Manavella, V.; Baima, G.; Mariani, G.M.; Romano, F.; Aimetti, M. Pocket closure and residual pockets after non-surgical periodontal therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2022, 49, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.M.; Olarte-Sossa, M.; Guzmán, I.C. Association between immunoglobulin G1 against Tannerella forsythia and reduction in the loss of attachment tissue. J. Periodontal Implant Sci. 2014, 44, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Habashneh, R.; Asa’ad, F.A.; Khader, Y. Photodynamic therapy in periodontal and peri-implant diseases. Quintessence Int. 2015, 46, 677–690. [Google Scholar] [CrossRef] [PubMed]
- Wenzler, J.S.; Falk, W.; Frankenberger, R.; Braun, A. Impact of Adjunctive Laser Irradiation on the Bacterial Load of Dental Root Canals: A Randomized Controlled Clinical Trial. Antibiotics 2021, 10, 1557. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Severino, M.; Gatto, R.; Monaco, A. Effectiveness of diode laser as adjunctive therapy to scaling root planning in the treatment of chronic periodontitis: A meta-analysis. Lasers Med. Sci. 2013, 28, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Girish, K.; Mandava, J.; Chandra, R.R.; Ravikumar, K.; Anwarullah, A.; Athaluri, M. Effect of obturating materials on fracture resistance of simulated immature teeth. J. Conserv. Dent. 2017, 20, 115–119. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Diagnoses | Participants/Number of Affected Teeth | Mean Age | Female/ Male | Endodontic Intervention | Periodontal Intervention | Main Outcomes | Follow-Up |
|---|---|---|---|---|---|---|---|---|
| Dembowska et al. [7] | Periodontitis stage III. Endo-perio lesion. | 12/12 | 47 years | 5/7 | Experimental group: rotary and hand instruments were implemented using the crown-down method. An Epic X Biolase diode laser was used at 940 nm twice a month for three months. Calcium hydroxide paste was applied to the canals between visits. After three months, the canals were filled with GP cones by lateral condensation. Control Group: rotary and hand instruments were applied to the canals between visits without a diode laser. After three months, the canals were filled with GP cones by lateral condensation. | Experimental group: SRP using an ultrasonic scaler and hand curettes plus laser-inactive tip. Three repetitions were performed in each pocket, with intervals of 10 s, twice a month for three months. Control group: SRP using an ultrasonic scaler. | Differences were observed in the decrease in PD between the experimental group and the control group, favoring the experimental group (1.88 ± 0.4 mm versus 0.23 ± 0.09 mm; p < 0.05). Tooth mobility in the experimental group decreased from 1 to 0 (p > 0.05). There was a greater increase in bone level in the experimental group (52.5% versus 27%; p < 0.05). | 6 months |
| AlJasser et al. [9] | An upper anterior non-vital single-rooted tooth with true combined endo-periodontal lesions | 120/120 | 41 years | 95/53 | Apical-coronal techniques were prepared with hand K-files at the established working lengths. Sizes 3, 4, or 5 reamer obturation, injection of the thermo-plasticized GP was performed twice, separately in the control group and experimental group 2. The entire root canal system was filled with MTA for experimental groups 1 and 3. | Control group: SRP Experimental group 1: SRP Experimental group 2: SRP and grafting procedure to fill the bony defect. Experimental group 3: SRP plus grafting procedure to fill the bony defect. | At three months of follow-up, significant differences in mean PD values between groups were observed. PD values of patients in GP plus bone graft (experimental group 2) presented significantly higher PD values than the other three groups (p = 0.025). GP (control group) and MTA (experimental group 1) groups showed significantly higher PD values (4.8 ± 0.89 mm and 3.8 ± 0.75 mm, respectively) compared to groups that received bone grafting (3.1 ± 0.59 mm) (experimental groups 2 and 3). The bone graft groups (experimental groups 2 and 3) improved by 1.8 ± 0.4 mm, whereas the nongrafted groups improved by 0.7 ± 0.1 mm, on average. The MTA + bone graft group (experimental group 3) presented the highest defect fill level (100%), followed by the GP + bone graft group (97%) (experimental group 2). | 12 months |
| Yan et al. [8] | Combined periodontal-pulpal lesions. Presence of endo-perio lesions without root damage. | 327/360 | 48 years | 171/156 | Experimental group: ET Control group: ET | Experimental group: periodontal basic treatment for 2 weeks after ET. Six weeks later, if there were still more than 5 mm periodontal pockets and bleeding after detection, flap treatment was performed. Control group: supragingival scaling | The mean PD in the experimental group decreased by 1.8 ± 0.05 mm compared with the control group (p < 0.05). Two years after treatment, tooth mobility in the experimental group was significantly lower than that in the control group (p < 0.05). Alveolar bone absorption 2 years after operation was not significantly different from that before surgery (p > 0.05) in the experimental group. Alveolar bone absorption 2 years after treatment was significantly reduced compared with that before treatment (p < 0.05) in the control group. | 24 months |
| Razi et al. [1] | Primary endo and secondary perio. | 140/140 | 18–58 years | 60/80 | Experimental and control groups: ET was finalized for all the teeth studied prior to the periodontal treatment. | Control group: PRF in infrabony defect Experimental group: Titanium-prepared PRF in infrabony defect | Mean PD and CAL were improved after 3 and 6 months in both groups (p > 0.05). The mean change in PD after 6 months was 2.56 mm (42.59%) in the control group and 2.51 mm (43.90%) in the experimental group (p > 0.05). The mean change in CAL after 6 months was 2.52 mm (40.82%) in the control group and 2.41 mm (42.12%) in the experimental group (p > 0.05). | 6 months |
| Tewari et al. [10] | Concurrent endo-perio lesion with apical radiolucency, along with communication through the periodontal pocket | 40/40 | 42 years | 8/32 | Experimental and control groups: ET and intracanal medicament (calcium hydroxide) were placed for 7–10 days. | SRP with an ultrasonic scaler and hand instruments and ET were simultaneously performed. Control group (immediate periodontal surgery): OFD was performed 21 days after initiation of ET and SRP. Experimental group (delayed periodontal surgery): OFD was performed 3 months after initiation of ET and SRP. | Mean PD, CAL, and tooth mobility were improved after 3 and 6 months in both groups (p > 0.05). The mean change in PD after 6 months was 3.3 ± 0.54 mm in the control group and 3.4 ± 0.52 mm in the experimental group. The mean change in CAL after 6 months was 2.7 ± 0.12 mm in the control group and 2.69 ± 0.03 mm in the experimental group. | 9 months |
| Gupta et al. [3] | Teeth with a clinical/radiographic diagnosis of a concurrent endo-perio lesion without communication | 31/37 | 45 years | 17/14 | Experimental and control groups: step-back technique. Canals were obturated with GP with the lateral condensation technique. | Control group: SRP with an ultrasonic scaler and hand instruments. ET and SRP were performed simultaneously. Experimental group: SRP was performed 3 months after completing ET. | Both groups presented a significant improvement in all clinical parameters evaluated after the completion of endodontic and periodontal treatment (p < 0.05). However, there was more improvement in periodontal parameters in the control group at the 3-month follow-up compared with the experimental group (PD 1.35 ± 0.72 mm versus 0.21 ± 0.27 mm; p < 0.05; CAL 1.36 ± 0.72 mm versus 0.14 ± 0.32 mm; p < 0.05). At 3 and 6 months after SRP (3- and 6-month follow-up in the control group, and 6- and 9-month follow- up in the experimental group), both groups presented a similar reduction in PD and gain in CAL (p > 0.05). Improvements in periodontal parameters that were reached in 6 months in the experimental group were achieved only in 3 months in the control group (p > 0.05). An improvement in the periapical index score was observed in 100% of cases in both groups (experimental group =1.39 mm versus control group = 1.37 mm; p > 0.05). | 6 months |
| Li et al. [6] | Endo-perio combined lesions | 30/30 | 44 years | 18/12 | Control and experimental groups: ET | ET and SRP were performed simultaneously. Control group: SRP Experimental group: SRP plus diode laser irradiation | Mean PD and CAL were improved after 6 months in both groups. The mean change in PD after 6 months was 0.4 ± 0.04 mm in the control group and 1.67 ± 0.19 mm in the experimental group (p < 0.05). The mean change in CAL after 6 months was 0.59 ± 0.06 mm in the control group and 0.9 ± 0.08 mm in the experimental group (p < 0,05). An improvement in the periapical index score was observed in both groups (control group = 0.27 mm versus experimental group = 0.73 mm; p > 0.05). | 6 months |
| Study | a | b | c | d | e | f | g | h | i | j | k | l | m | n | o | p | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dembowska et al. [7] | 3 | 3 | 3 | 0 | 0 | 3 | 3 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 75% |
| Aljasser et al. [9] | 3 | 3 | 3 | 3 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 87.5% |
| Yan et al. [8] | 3 | 3 | 3 | 3 | 0 | 3 | 0 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 75% |
| Razi et al. [1] | 3 | 3 | 3 | 3 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 87.5% |
| Tewari et al. [10] | 3 | 3 | 3 | 3 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 87.5% |
| Gupta et al. [3] | 3 | 3 | 3 | 3 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 87.5% |
| Li et al. [6] | 3 | 3 | 3 | 0 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 81.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardila, C.M.; Vivares-Builes, A.M. Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies. Int. J. Environ. Res. Public Health 2022, 19, 13649. https://doi.org/10.3390/ijerph192013649
Ardila CM, Vivares-Builes AM. Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies. International Journal of Environmental Research and Public Health. 2022; 19(20):13649. https://doi.org/10.3390/ijerph192013649
Chicago/Turabian StyleArdila, Carlos M., and Annie Marcela Vivares-Builes. 2022. "Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies" International Journal of Environmental Research and Public Health 19, no. 20: 13649. https://doi.org/10.3390/ijerph192013649